
Abstract
We report the case of a 69-year-old man admitted to the emergency department of a UK district general hospital with an extradural haematoma following closed head injury. He deteriorated rapidly before transfer to the regional neurosurgical centre and was treated with decompression of the extradural haematoma through an EZ-IO™ intraosseous needle in our department, with telephone guidance from the neurosurgeon. We believe this to be the first reported use of this technique in a district general hospital.
Background
Extradural haematoma is a neurosurgical emergency, for which craniotomy and evacuation of haematoma are the definitive management. However, many patients will present to the district general hospital, with no neurosurgical department, thus mandating a secondary transfer to the regional neurosurgical unit. Neuroprotective measures including optimising of the patients’ neurophysiology, use of hypertonic fluids and urgent transfer to a tertiary centre for definitive treatment in the form of craniotomy and evacuation of haematoma remains the mainstay of initial management. 1
We report the decompression of a computerised tomography (CT) – confirmed extradural haematoma using an EZ-IO™ intraosseous (IO) needle in an unconscious patient, whilst the patient was prepared for transfer to the regional neurosurgical centre. We were directed by telephone on needle placement with respect to key landmarks by advice from a neurosurgeon who had reviewed the CT imaging remotely. We believe this to be the first reported application of this novel procedure in a district general hospital.
Case report
A 69-year-old man presented to our emergency department (ED) following closed-head injury. He had lost consciousness at scene, but quickly recovered and on arrival to ED had a Glasgow Coma Score (GCS) of 14: E4, V4, M6. He was previously fit and well and on no regular medication. He deteriorated quickly in ED to a GCS of 3 with a dilated right pupil. Despite intubation, ventilation and 1-mg/kg intravenous mannitol, his right pupil remained fixed and dilated to 5 mm. The left pupil was 3 mm and still reactive. Standard neuroprotective measures were continued while an urgent CT scan was performed of his head and spine (Figure 1). This showed a fracture of the temporal and parietal bones with a large, right extradural haematoma up to 18 mm in depth, significant midline shift and right uncal herniation. No clear evidence of acute cervical spine injury was identified.
CT head showing large right extradural haematoma.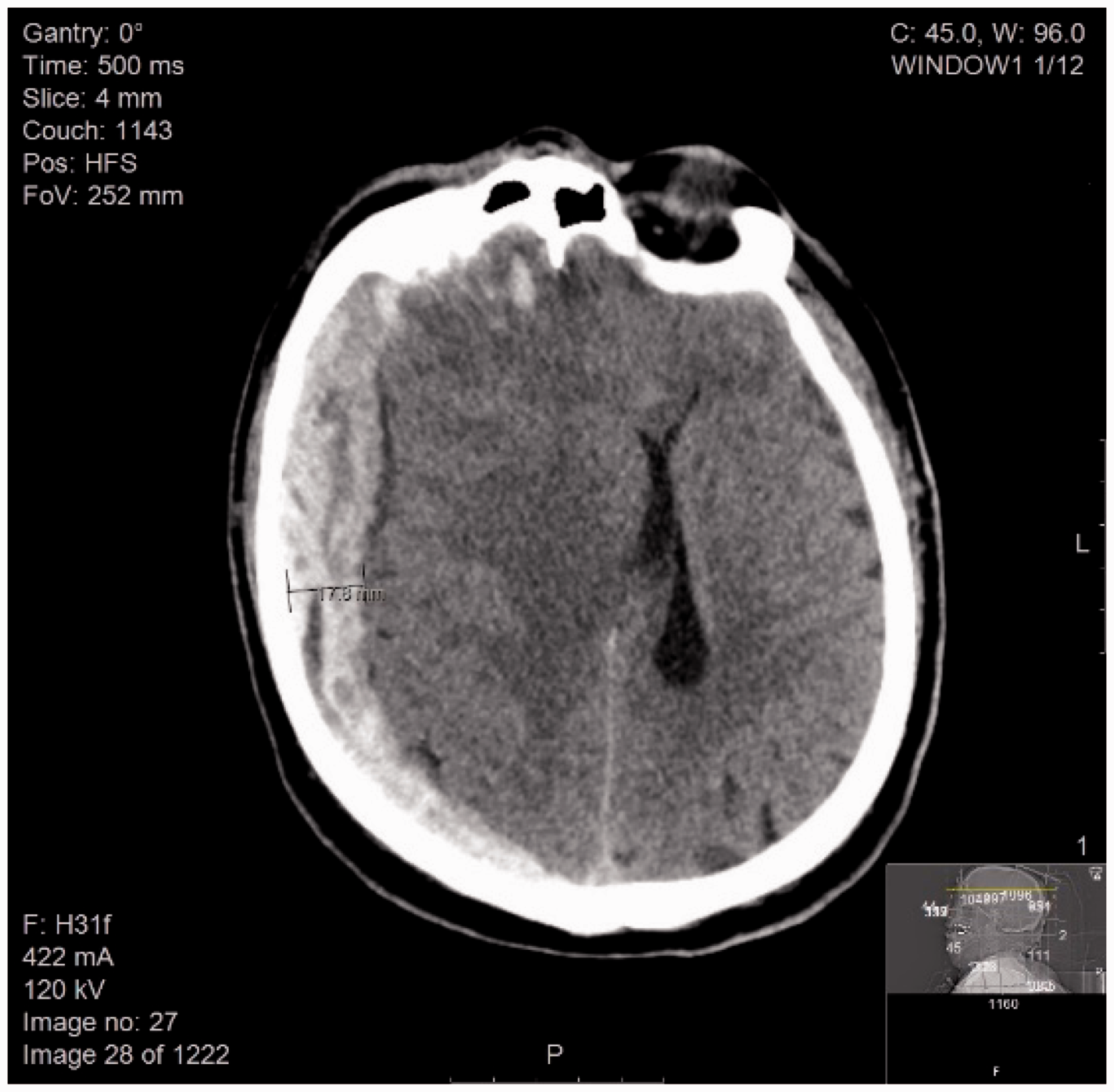
By the time of completion of the CT scan, the left pupil also became dilated to 5 mm and both pupils were now unreactive to light. The case was discussed immediately with our regional neurosurgical centre, with review of the CT images. Considering the patient’s severe clinical condition and that it was likely to be 40–50 min before neurosurgery would be possible, we were advised to attempt to decompress the haematoma immediately in ED using a 25-mm long EZ-IO™ IO needle. The needle was to be inserted to its full depth, on the right side of the skull, 2 cm superior and just anterior to the upper border of the ear, aspirating as much blood as possible using a syringe whilst checking for any return of pupillary response. Although there were no staff on-site with experience in craniostomy, there were personnel competent in the use of the EZ-IO device and it was considered better to attempt the procedure under these circumstances than to wait until transfer to the neurosurgical centre for decompression. The next of kin were informed of the severe nature of his injury and also of the novel but life-saving intention of the intervention.
The procedure was performed in an aseptic manner using a 25-mm EZ-IO™ IO needle and electric driver. There was an immediate release of blood and a total of 70 ml of blood over 10 min was aspirated using a 50-ml Luer lock syringe, while the patient was simultaneously prepared for transfer (Figure 2). By the end of the aspiration, the right pupil remained unchanged, but the left pupil reduced in size to 3 mm whilst remaining non-reactive to light. In view of the apparent improvement, our regional neurosurgical centre recommended a further dose of mannitol. Unfortunately the patient’s left pupil began to increase in size and remained fixed and he remained GCS 3/15. In view of the absence of brain function, the transient response to both mannitol and aspiration of haematoma and the time it would take to transfer him to the neurosurgical unit; we were advised by the neurosurgical team that transfer for neurosurgery no longer seemed to be in his best interests and it was agreed with the family and local critical care team that he would remain in our hospital for end-of-life care. The patient was not rescanned, albeit this would have been useful to assess any change in the size of the haematoma.
Aspiration of extradural blood using an IO needle.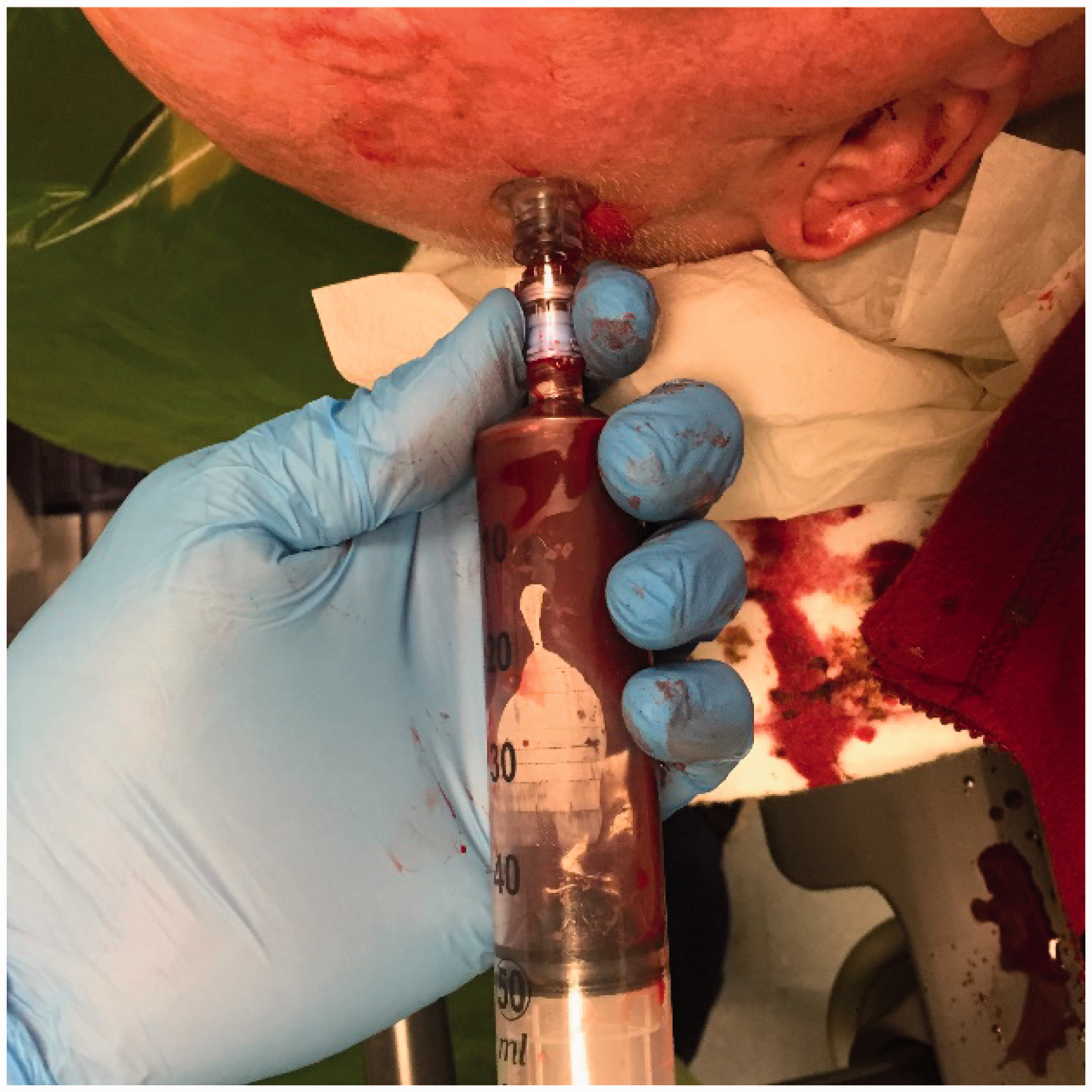
The patient was admitted to our intensive care unit where his care was prioritised towards maintenance of comfort and dignity. He passed away two days later, having failed to regain consciousness, and after the cessation of advanced organ support.
Discussion
We believe this to be the first reported IO needle craniostomy, used to partially drain an extradural collection in a unit where neurosurgery is not performed on site, with guidance from a neurosurgeon. The use of IO needle craniostomy by neurosurgeons in a tertiary centre to temporise an extradural haematoma whilst simultaneously preparing for craniotomy has recently been reported. 2
Treatment of extradural haematoma is a time critical intervention, with significantly worse outcomes with increasing time to evacuation from onset of anisocoria 3 or coma. 4 The Monro–Kellie Doctrine (Kellie 1824; Monro, 1783) established the critical dependence of intracranial pressure on small changes in the volume of the cranial contents.5,6 Hence, the aim of this technique is not to drain the entire haematoma, but to decompress. Even a small reduction in volume may have significant effect on intracranial pressure, therefore improving cerebral perfusion and preventing secondary brain injury and herniation.
IO needles are available in most EDs in the UK and are easy to use, requiring minimal prior training. This report demonstrates that an IO needle can be used to drain an intracranial haematoma when there are no other options available to save life under the guidance of the neurosurgical team.
As in this case, Bulstrode et al. have advocated that the site of insertion should be the point of maximal clot depth and therefore localisation of the insertion point would be on a case by case basis. Failing to contact the target haematoma with the needle is a potential complication, but it has been suggested that most extradural haematomas requiring emergency craniotomy are sufficiently large that this seems unlikely. 2 The needle length should be based on the age of the patient, degree of subcutaneous swelling and scan appearances and must also be of sufficient depth to penetrate both the scalp and the cranium. Whilst a 25-mm needle was used in this case, the presence of significant scalp swelling might necessitate the use of a longer needle and should be agreed as part of the dialogue and planning between the remote neurosurgical team and local clinicians performing the craniostomy.
Potential complications of this procedure include misplacement, infection, haemorrhage and neurological injury. The closest parallel in routine neurosurgical practice is probably intracranial pressure monitor insertion for which the reported rates of clinically significant infection and haemorrhage in large case series are <5% and 1–3%, respectively.7–9 With this technique being performed by a non-neurosurgeon in conditions where sterility is difficult to maintain, rates of infection or significant haemorrhage could be higher than this. However, these risks need to be considered in the context of the procedure being used as an emergency temporising measure aimed at preventing death and secondary brain injury.
It took approximately 10 min to insert the IO needle and aspirate the blood. This was performed whilst awaiting the ambulance and did not delay transfer to our regional neurosurgical centre. This is critical as it is known that local treatment must be undertaken in parallel with facilitating time critical transfer. A prospective study has shown patients at district general hospitals with life-threatening extradural (or subdural) haematomas have prolonged times to decompression above a suggested 4-h window. 10
One alternative to decompression using an IO needle is emergency burr hole formation. A number of small case reports or series have described ED burrhole drainage to temporise compression from extradural haematomas with reported survival, 11 but unfamiliarity and complexity of performing this procedure locally and the potential for delay in transfer and complications mean this is not routinely advocated or practised.
Although burr hole formation is more familiar to neurosurgeons and a minority of trauma or rural surgeons, and may provide more reliable decompression, we suggest that it is unlikely that the skills and equipment will be available immediately for this technique in most district general hospitals. Conversely, the use of IO needles is now accepted as part of Resuscitation Council (UK) Guidelines,12,13 meaning equipment and expertise is often available in the ED.
Although there was unfamiliarity in using an EZ-IO needle for this particular purpose, we were proficient in the use of EZ-IO needles and therefore found it easy to perform without prior training. Although the patient did not ultimately survive, the procedure was technically straightforward and could be expected to be performed in a similar manner, benefiting other patients when there are no other options available. Extradural blood also clots relatively easily, so this method may be better for liquefactive clots, although removal of even a small volume of blood may temporise ICP before definitive management.
In conclusion, we suggest that the use of an IO needle to decompress a life-threatening extradural haematoma should be considered in the district general hospital. If attempted, this should be under the guidance of the on-call neurosurgeon, without causing delay to definitive neurosurgery, and with proper consideration of the potential risks and benefits of the procedure. Further study of times to transfer and outcome following life-threatening extradural is warranted.
Consent
Consent was obtained on a best interest basis in the first instance, and publication of the report was discussed and approved by the relatives.
Footnotes
Acknowledgement
This procedure was conceived by Jonathan Hempenstall and Aabir Chakraborty.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.