
Abstract
Catecholamines are entrenched in the management of shock states. A paradigm shift has pervaded the critical care arena in recent years acknowledging their propensity to cause harm and fuel a ‘death-spiral’. We present the case of a 21-year-old male following a witnessed out-of-hospital cardiac arrest who received high-quality cardiopulmonary resuscitation and standard advanced life support for refractory ventricular fibrillation until return of spontaneous circulation after 70 min. Early post-admission echocardiography revealed severe diffuse sub-basal left ventricular hypertrophy with dynamic mid-cavity obstruction and akinetic apical pouching. Within this context, a decatecholaminised strategy comprising a beta-blocker was used to augment the left ventricular end-diastolic volume and attain cardiovascular stability.
Keywords
Introduction
Endogenous catecholamines and their synthetic counterparts are mainstay in the stabilisation of the haemodynamically impaired, including cardiac arrest (CA) patients. 1 Until recently, their role has been undisputed for both pragmatic and ethical reasons despite the weak evidence-based practice.2,3 A recent study confirms that adrenaline augments mortality in cardiogenic shock. 4 Hence, the omission of catecholamines in such situations has been put forward by several authors.5,6
A case of hypertrophic cardiomyopathy (HCM) with mid-cavity obstruction is described to serve as a case in point that cardiovascular collapse managed by a blind, non-ultrasound (US) guided and catecholamine-based strategy could be detrimental. Potential haemodynamic interventions are discussed with reference to those which are catecholamine-sparing.
Case presentation
A 21-year-old man, without prior medical history or cardiac symptoms and a keen judoka, was referred to our intensive care unit (ICU) following resuscitation after sudden out-of-hospital cardiac arrest (OOHCA) with an initial shockable rhythm – ventricular fibrillation (VF). Return of spontaneous circulation (ROSC) was achieved 70 min after collapse. Intra-arrest management was consistent with current guidelines and total cumulative adrenaline dose was 14 mg. Advanced airway management at the scene was undertaken in face of overt pulmonary aspiration.
Early bloods were indicative of severe and protracted low output syndrome despite apparent high-quality intra-arrest cardiopulmonary resuscitation (CPR): disseminated intravascular coagulation (DIC), severe rhabdomyolysis, a cardio-hepatic syndrome and acute kidney injury (AKI).
Initial management included timely bronchoscopy for particulate aspiration, protective ventilation, continuous renal replacement therapy, metabolic control and targeted temperature management at 35℃–36℃ for the first 48 h with concordant sedation.
Admission electrocardiogram (ECG) was suggestive of apical HCM: a strain pattern with giant T-wave inversions (10–15 mm) in the precordial leads bearing time-honoured diagnostic significance, 7 voltage criteria of left ventricular (LV) hypertrophy, diffuse absence of septal Q-waves 8 and a discretely notched depolarization (QRS) complex in the inferior leads and V4–V6. The latter, although far from achieving established standards, could signal an increased risk for malignant arrhythmia. 9
Post–ROSC emergent coronary angiography revealed no significant lesions. Whole body computed tomography (CT) at admission showed normal grey-white matter differentiation, dependent lung segments atelectasis/consolidation, a characteristic hour-glass or dumbbell LV configuration (see Figure 1) indicative of sub-basal HCM with mid-ventricular obstruction (MVO) and a thinned apex.
10
Maximal wall thickness and systolic muscular apposition length were twice as large as the mean of a cohort of 28 patients with LV apical aneurysm and HCM.
11
CT (from left to right – filling of the LV). Slit-like LV cavity with mid-ventricular obstruction and apical pouch; maximum thickness: 30 mm; overall length: 70–80 mm; apposition length: 25–30 mm. CT: computed tomography; LV: left ventricle.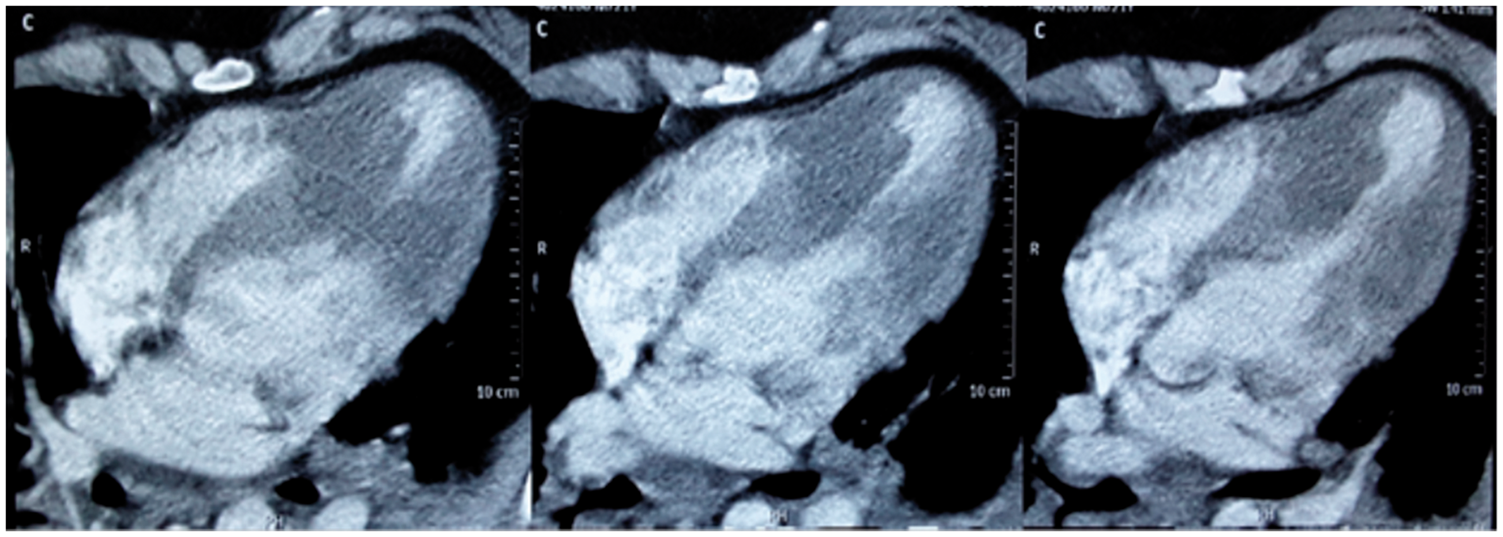
Echo parameters: Diastolic dysfunction grade III. 12
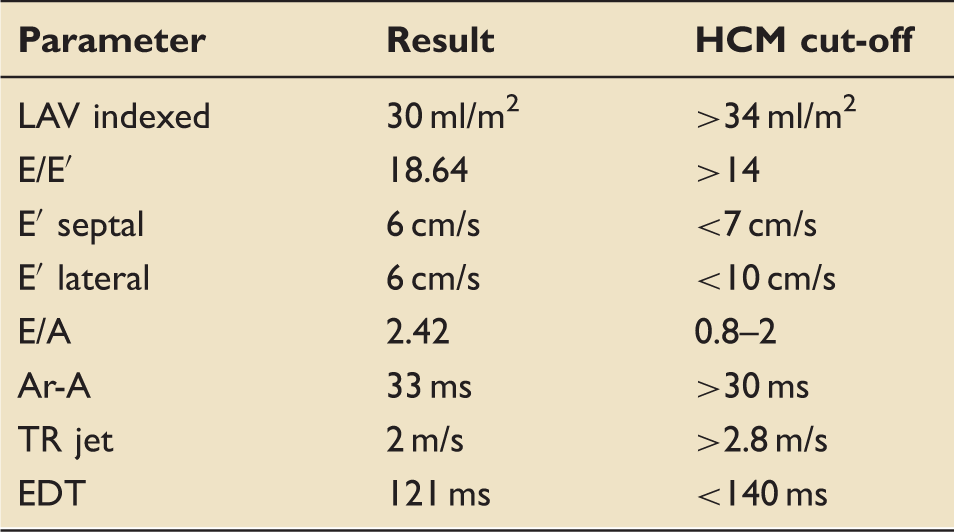
HCM: hypertrophic cardiomyopathy; LAV: left atrial volume; E and A: early and late atrial blood filling (peak velocities); E/A: the ratio between the peak modal velocities of early (passive) and late (active due to atrial contraction) diastolic filling, respectively; E′: peak mitral annular velocity during early filling (measured at septal and lateral mitral annulus); Ar-A: time difference between duration of pulmonary venous flow and mitral inflow during atrial contraction; TR jet: peak velocity of tricuspid regurgitation jet; EDT: E wave (early atrial filling) deceleration time.
Dynamic echo parameters – before and after treatment.
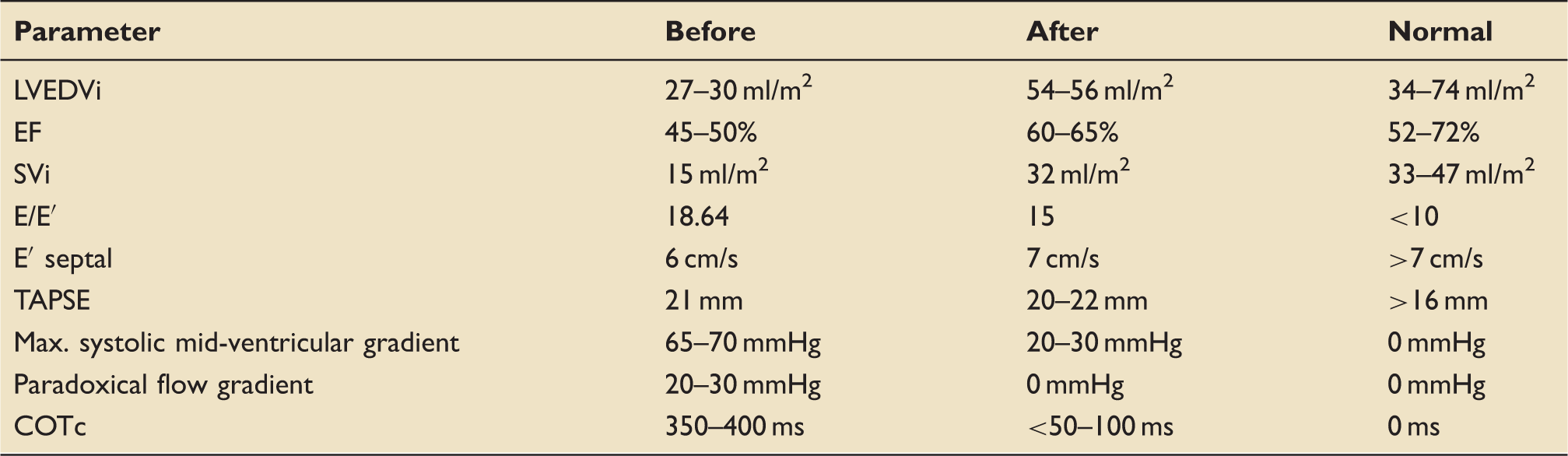
TAPSE: tricuspid annular plane systolic excursion; COTc: corrected (to heart rate) cavity obstruction time (severe if > 350 ms) 13 ; LVEDVi: indexed left ventricle end-diastolic volume; EF: ejection fraction; SVi: indexed stroke volume; E and A: early and late atrial blood filling (peak velocities); E′: peak mitral annular velocity during early filling (measured at septal and lateral mitral annulus).
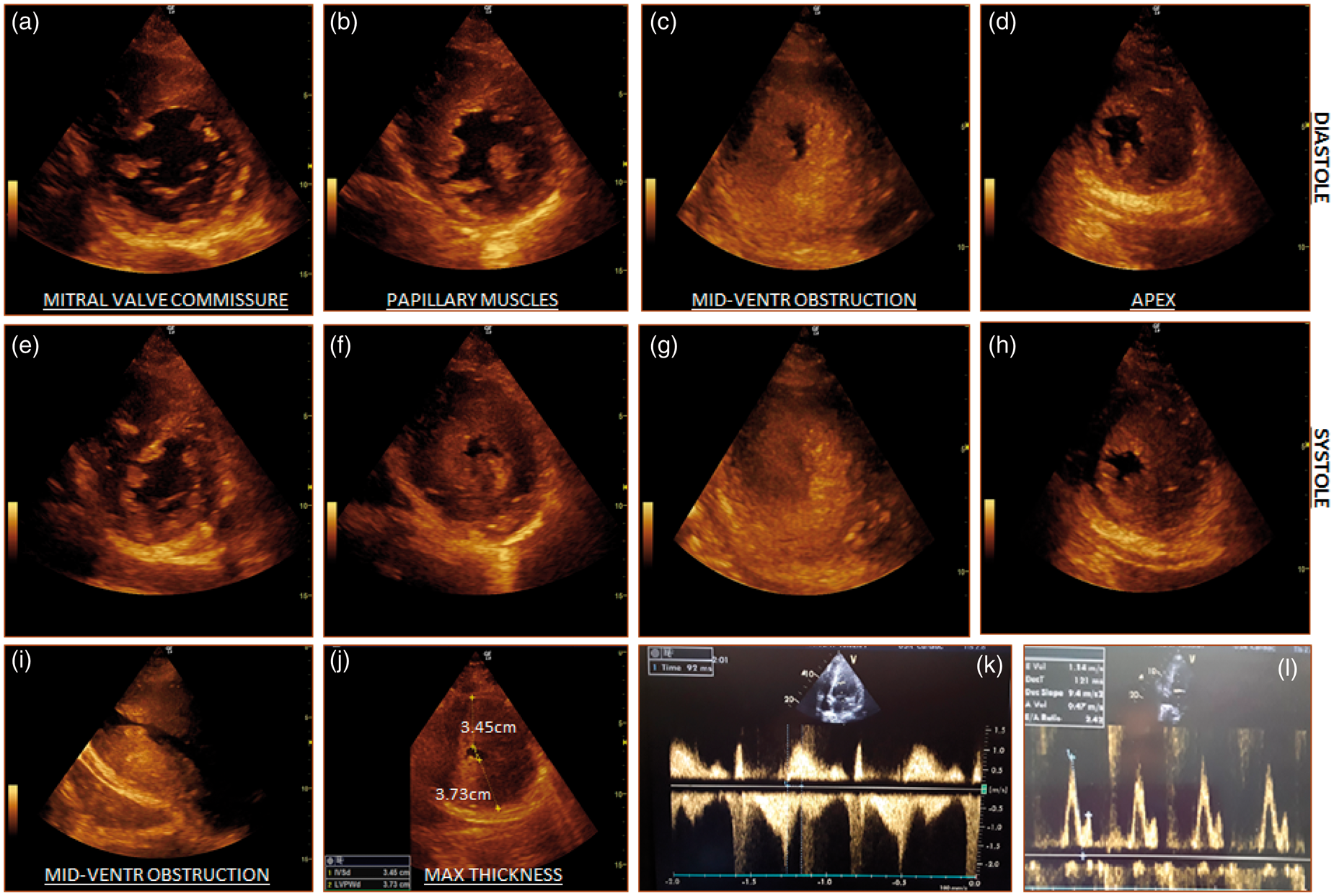
Echo parameters – 2D and Doppler studies (early, before treatment). (1) (a–e), (b–f), (c–g), (d–h) systolic–diastolic pairs of parasternal short-axis views at different LV levels showing mid-cavity obstruction and apical asynergy; (i) LV focused apical two-chamber view, reflecting slit-like LV cavity; (j) above papillary muscles, parasternal short axis view showing maximum thickness. (2) (k) apical four-chamber view, continuous Doppler shows mitral inflow and overlapping diastolic jet of opposite direction, which is consistent with paradoxical jet flow (diastolic flow from systolically sequestered apex towards LV outflow, peak velocity = 2.5 m/s); l – pulsed-wave Doppler between mitral leaflet tips showing E/A = 2.42, which is consistent with grade 3 diastolic dysfunction. 12 LV: left ventricle.
Haemodynamic and metabolic parameters – before and after treatment.
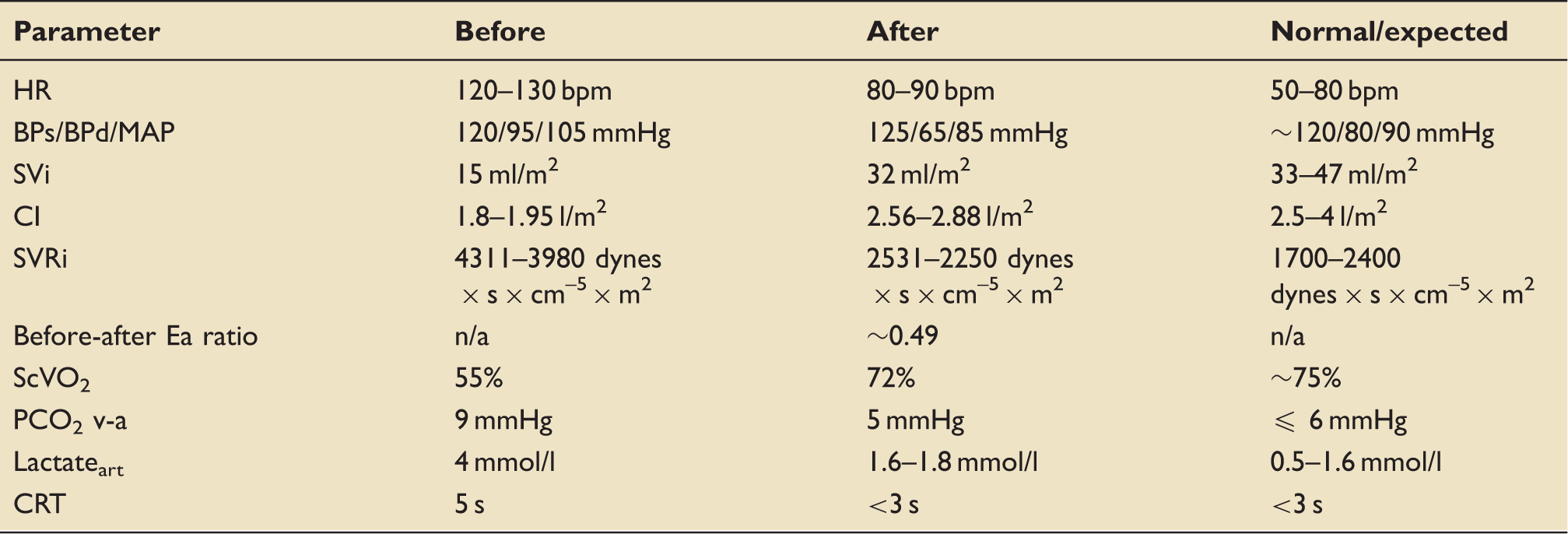
Decatecholaminisation improved the VO2/DO2 relationship (SVi, PCO2 v-a, ScVO2, lactate) and the vasomotor tone (before-after Ea ratio, SVRi), which ultimately led to improved microcirculatory (CRT) dynamics (observation window – first 6 to 12 h). HR: heart rate; BPs: systolic blood pressure; BPd: diastolic blood pressure; MAP: mean arterial pressure; CI: cardiac index; SVRi: indexed systemic vascular resistance; Ea: arterial elastance defined as 0.9 × BPs/SV; ScVO2: central venous oxygen saturation; PCO2 v-a: venous-to-arterial carbon dioxide (CO2) tension difference; lactateart: arterial lactate concentration; CRT: capillary refill time.
Post-cardiac arrest organ dysfunction stabilised in the next few days. Neuro-prognostication was performed 72 hours later. Long-term outcome was poor: early myoclonus less than 24 hours after ICU admission, electroencephalogram showing diffuse low voltage/burst-suppression pattern after the first three days and no obvious neurological improvement over a three-week period (best motor score was 2). A ‘non escalation of care’ policy was agreed upon after discussion with the family.
A clinical diagnosis of HCM, known to be an autosomal trait in close to 60% of cases, is always called for in first-degree relatives of the proband. Echocardiographic examination of the young man’s father revealed moderate (LV wall thickness 15–16 mm), diffuse LV hypertrophy. Free from other known loading conditions, this was considered diagnostic for HCM. 17
Discussion
HCM is the most common genetic heart disease and cause of sudden death in young athletes, affecting 1 in every 500 individuals. It displays a highly heterogeneous phenotypic and genotypic spectrum. 18
Indicators of need for advanced imaging (e.g. echocardiography).
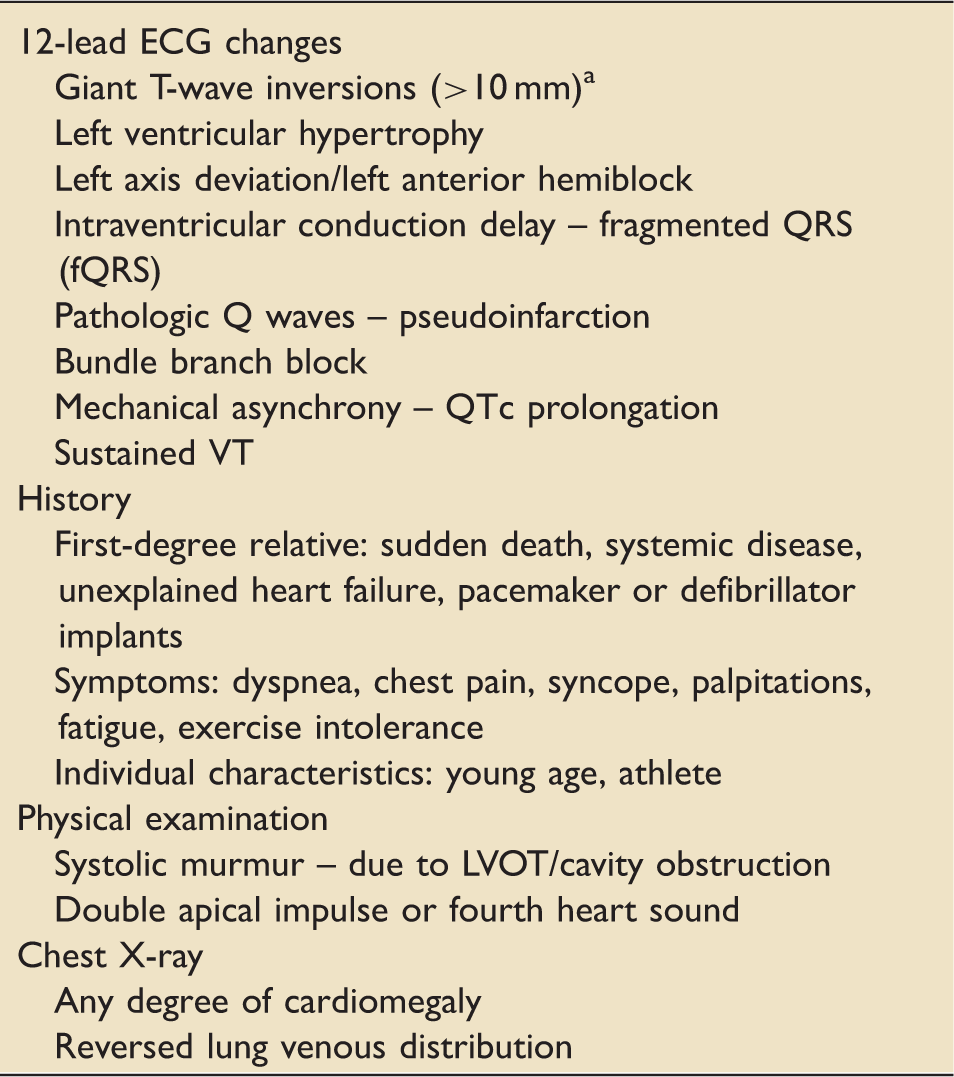
Highly suggestive of apical HCM; the other indicators lack specificity and call for a combined interpretation. Threshold for requesting echocardiography should be low, especially when confronted with shock states. ECG: electrocardiogram; VT: ventricular tachycardia; LVOT: left ventricular outflow tract.
Regardless of its longitudinal evolution, this rare MVO phenotype (8–9.4% of all HCM21,22) elicits unique haemodynamic consequences. Depending on the duration and length of the muscular apposition, it results in abnormally small end-diastolic LV volumes and corresponding stroke volumes with or without preserved ejection fraction. 14 MVO disrupts normal intraventricular coupling by imposing a mid-cavity afterload, which can extend well beyond systole. This then results in a high-pressure apical chamber, which brings about two interrelated phenomena: (a) apical dysfunction culminating with aneurysm formation and (b) asynchronous diastolic filling with a paradoxical jet flow moving away from the intrasystolic pressurized apex towards the LV base. 23
Lusitropic impairment of some degree is common to all HCM subtypes, but the MVO phenotype is known to exhibit high-grade diastolic dysfunction. 24 This aggravates preload sensitivity and places the heart at mechanical disadvantage. 25
MVO predisposes to sudden death and malignant arrhythmias.21,22 Moreover, apical aneurysms 11 as well as diastolic paradoxical jet flows, 26 independently, add further cardiovascular morbidity and mortality. Our patient fulfilled all these indicators.
Beta-blockade minimized the MVO mediated restrictive filling of the LV as suggested by the COT profile (see Table 2). On the contrary, catecholamines would perpetuate low LV dimensions and low flow, which would conventionally lead to escalation of the adrenergic support.
Shock-induced endotheliopathy (SHINE) has recently been depicted as a common denominator for states, which are driven by excessive sympatho-adrenal hyperactivation. 27 Sepsis, trauma (especially traumatic brain injury), burns, post-cardiac arrest syndrome, subarachnoid haemorrhage, pheochromocytoma or immoderate beta-2 stimulation are all classic examples of such states and each one of them has already been ascribed an adrenergic storm epitome such as the more specific Takotsubo cardiomyopathy (TCM) or the all-inclusive term stress-cardiomyopathy (SCM).28,29 TCM is not a mere epiphenomenon but portends a poor risk by itself as shown by Templin et al. 30 Within this context, beta-blockade has been advocated in several scenarios: CA resuscitation, 31 traumatic brain injury,32,33 sepsis 34 and burns. 35
Decatecholaminisation is an ‘umbrella’ term, 36 encircling much more than beta-blockers. Other agents may also have a role. Clonidine has been shown in animal models to rectify pressor responsiveness, hence minimizing adrenergic support. 37 Vasopressin has a role in the vasoplegic syndrome arising in post-cardiac surgery patients. 38 Angiotensin, alongside vasopressin, could be another useful adjunct in septic vasoplegia allowing catecholamine dose reductions. 39 SEPSIS-ACT, a phase 2 b/3 adaptive clinical trial (NCT02508649), will investigate selepressin use in septic shock. Levosimendan is yet another inotropic agent but one recent study in septic patients 40 and two in cardiac surgery patients41,42 have been disappointing with no mortality benefit.
Myocardial metabolic resuscitation with high-dose glucose-insulin-potassium (HDI) regimes looks promising according to a recent audit from a London teaching hospital but prospective evaluation is yet to be undertaken. 43
Lastly, mechanical support has received unprecedented attention. Not only a catecholamine-sparing strategy, veno-arterial extracorporeal membrane oxygenation could provide the optimum ventriculo-arterial coupling through its amplifying effect on LV afterload, 44 hence opposing the MVO.
The overall outcome of this case reflects a drawn-out resuscitation. A high cumulative dose of epinephrine, as also used in our case, has been found to negatively impact on morbidity and mortality in OOHCA. 45 Within the current mechanical milieu (severe MVO), it is conceivable to see it as a chief additive cause of intractable CA. ALS-compliant echocardiography 46 and intra-arrest beta-blockade 47 may be better delineated in the future and may have changed the course in this case. Until then, the goal of good functional outcome post CA and CPR remains a challenge, in particular with cases such as that described here.
Our case underlines the fact that echocardiography has a potential yet to be explored in the acute care setting as already described by a recent consensus document. 48 Mixed systolic–diastolic indices such as the Tei index of myocardial performance may serve to optimize the pacing rate with consequent reduction of catecholaminergic support. 49 Translating such findings to non-paced critically ill patients could be envisaged in the future through pharmacological control of heart rate. Funny channel (If) blockers 50 and beta blockers could be options to consider. Acute mechanical support will most likely prove to be another high-yield territory for future trials investigating a role for echocardiography. Right-LV interdependence has been foregrounded as a predictor of successful weaning after cardiac mechanical assistance. 51 Relatedly, a reversed order of ventricular filling has been found to predict a positive fluid balance. 52 Such measurements could be potential targets for predictive enrichment strategies of trials to come.
Conclusion
An association of refractory VF/ventricular tachycardia (VT) arrest and young age should be assessed carefully with consideration for the possibility of HCM. Treatment and outcomes of cardiac arrest in such cases highlights the limits and the inadequacies of current resuscitation strategies. Timely quantitative haemodynamic assessment, ideally including echocardiography, and an individualized, pathophysiologically oriented care should become more widespread until much awaited randomised controlled prospective clinical trials rise to our expectations.
Footnotes
Authors’ contributions
Both authors contributed equally to this manuscript. Cosmin Balan was the treating physician.
Consent
This case report is published with the written consent of the next of kin.
Declaration of conflicting interests
The authors declare no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.