
Abstract
The right to liberty and security of the person is protected by Article 5 of the European Convention on Human Rights which has been incorporated into the Human Rights Act 1998. The 2014 Supreme Court judgment in the case commonly known as Cheshire West provided for an ‘acid test’ to be employed in establishing a deprivation of liberty. This ‘acid test’ of ‘continuous supervision and not free to leave’ led to concerns that patients lacking capacity being treated on an Intensive Care Unit could be at risk of a ‘deprivation of liberty’, if this authority was applicable to this setting. This article revisits the aftermath of Cheshire West before describing the recent legal developments around deprivation of liberty pertaining to intensive care by summarising the recent Ferreira judgments which appear for now to answer the question as to the applicability of Cheshire West in life-saving treatment.
Keywords
Article 5(1) of the ECHR.
Post Cheshire West
The acid test appeared prima facie universal with potentially limitless scope. Unsurprisingly, a default position evolved amongst some legal and medical professionals that assumed Cheshire West required a ‘context insensitive’ interpretation, with the potential to apply equally in the arena of clinical care as it did in the context of long-term social care. This resulted in great uncertainty for intensive care professionals and hospital trusts.
The paucity of subsequent case law did little to dispel this assumption. Consequently, guidance issued to clinicians by numerous stakeholders including the Department of Health (DOH) and the Law Society seemed to reaffirm this position of wider interpretation in the absence of any judicial decision to the contrary.3,4 In assisting clinicians and hospital trusts to maintain fidelity with the law, the Law Society indicated that an extension of the principles of Cheshire West into the hospital setting, including conveyance to and from hospital by ambulance, in emergency departments and the ICU should actively be considered, giving examples to illustrate accordingly. 4 Guidance from the DOH acknowledged the operation of DOLS in emergency or intensive care settings was ‘causing some concern’ but reminded providers of the ability to self-authorise a DOL for up to seven days by following the ‘urgent authorisation’ process. 3 This status quo was further “legitimised” by an acceptance from government of the need to reform the entire law underpinning DOLS, and the subsequent work by the Law Commission in this regard proceeded on the basis that deprivation of liberty was a concept that could apply equally in the intensive care setting. 5
Mental Health Act 1983 (as amended by the Mental Health Act 2007).
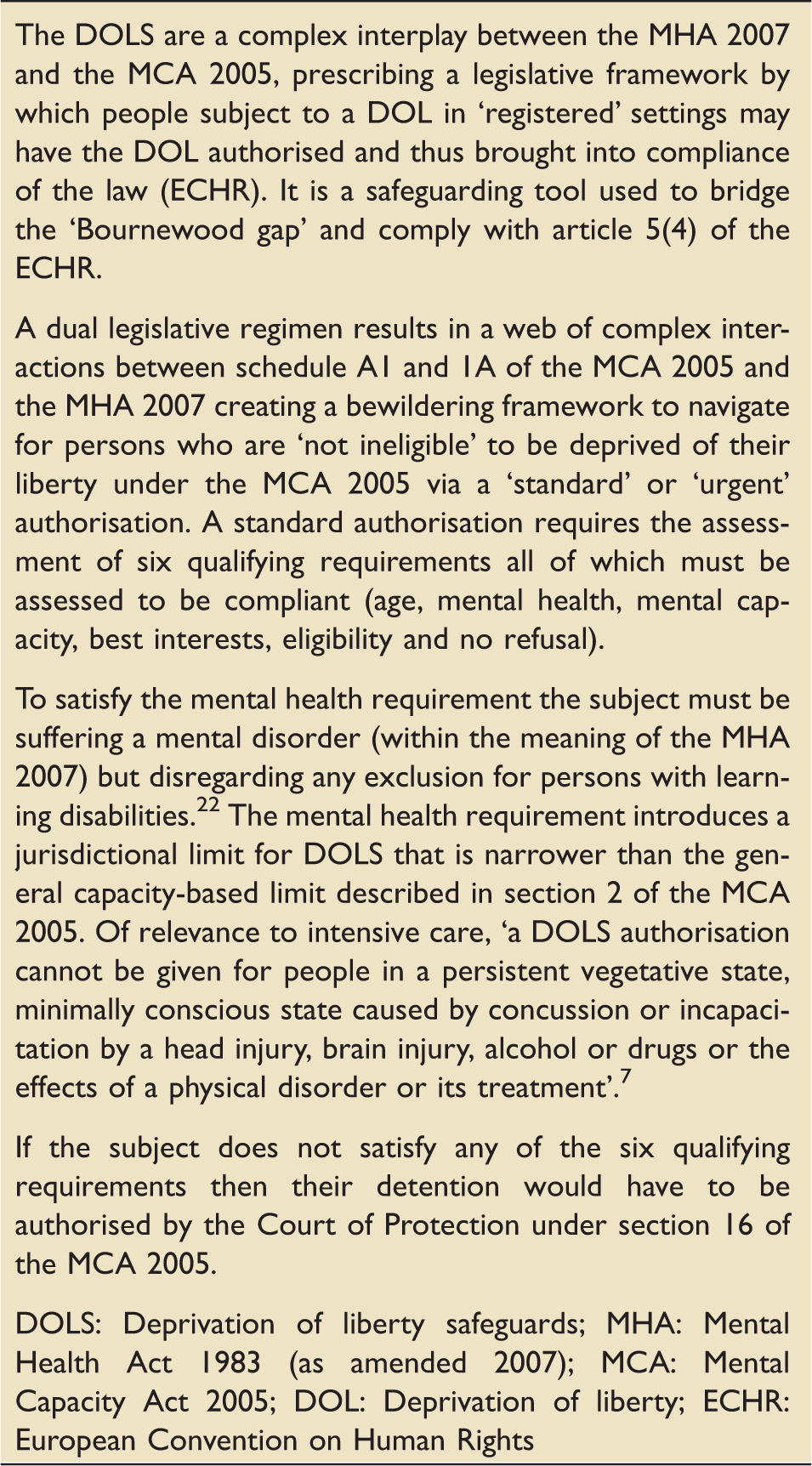
Deprivation of liberty safeguards.
In the absence of law reform, the question however remained, whether the ‘acid test’ which appeared to work so elegantly in addressing the mischief that arose in Cheshire West was applicable in the provision of life-sustaining treatment on an ICU, accepting any wider resource implications as the price for safeguarding the individual right to liberty.
The opportunity to answer this question came, albeit indirectly, via an application for a judicial review of the decision by Her Majesty’s (HM) Coroner for Inner London South not to hold an inquest by jury into the death of a patient on an ICU in R(on the application of Ferreira) v HM Senior Coroner for Inner London South. 7 This application was dismissed by the High Court in October 2015, leading to appeal in which the Intensive Care Society (ICS) and the Faculty of Intensive Care Medicine (FICM) through the Legal and Ethical Policy Unit acted as joint interveners.
On the 26th January 2017, the Court of Appeal handed down its judgment, holding that Cheshire West is not the precedent authority in establishing a deprivation of liberty in the ICU and consequently a wholesale extension of that authority into urgent medical care as unwarranted.
This article summarises this landmark judgment and its implication for intensive care practice going forward.
R(on the application of Ferreira) v HM Senior Coroner for Inner London South
High Court ([2015] EWHC 2990 (Admin), MHLO 76)
The initial case before Gross LJ and Charles J was the first occasion a lower court had been asked to define the scope of Cheshire West in the context of intensive care treatment. The case centred on Maria Ferreira, a 45-year old with Down’s syndrome, who suffered learning difficulties and limited mobility needing 24-hour care (which was principally given by her sister). Maria died in the ICU of Kings College Hospital after an acute illness. Her sister, Luisa, as the claimant, brought judicial review proceedings against HM Senior Coroner for Inner London South for his decision not to summon a jury to hear the inquest into Maria’s death. At its core was the Coroners and Justice Act (CJA) 2009 and if, under its relevant sections, the coroner was duty bound to call a jury because Maria was in ‘state detention’. 8 The question asked of the court was whether Maria’s treatment in ICU amounted to ‘state detention’ with the basis of the claimant’s case being that Maria was deprived of her liberty in terms of Article 5 of the ECHR and therefore this amounted to ‘state detention’ for the purposes of the CJA 2009.
Gross LJ and Charles J dismissed the claim for varied and conflicting reasons. Gross LJ utilised the concept of ‘context’ to reason that a DOL had not occurred, before concluding the coroner’s decision was not unreasonable, accepting that another coroner may have concluded differently. On the other hand, Charles J grappled with the language employed in the CJA 2009 concluding that because Maria was not compulsorily detained, she was not in state custody and thus was not deprived of her liberty. 7
Subsequently, the case was reviewed in the Court of Appeal.
Court of Appeal [2017] EWCA Civ 31
The Court of Appeal judgment was delivered by a single judge, Arden LJ, with whom Mcfarlane LJ and Cranston J agreed. It simplified the reasoning upon which the appeal was dismissed and in doing so provided clarity in respect to Article 5 within the intensive care setting. The central question remained whether the decision of HM Coroner not to convene an inquest by jury was lawful under the CJA 2009.
The appellant’s principal argument was that the coroner and the divisional court ‘failed to recognise the acid test was applicable and should have been applied’. It was argued that Maria Ferreira was under continuous supervision and control of the hospital, unable to leave due to sedation and ventilation, with any acquiescence to treatment on Maria’s part being an irrelevance to establishing a potential infringement of her Article 5 rights. Pertinent to this argument was that the ‘hypothetical question’ regarding the response to attempts by family members to remove a patient, rebuffed as ‘fanciful’ by Gross LJ in the divisional court, should have been asked.4,7
Counsel for HM Coroner argued that concluding an Article 5 infringement in this case does not promote the original purpose of that article. The essence of this case was that the doctors did not want to keep Maria Ferreira confined or to impose a regime of deprivation but were intending for her to leave as soon as it was safe for her to do so.
The court granted a joint intervention by the ICS and FICM describing the realities of administering and receiving care on an ICU and the impact of DOLS, without comment or prejudice to the specifics of this case. In describing the typical patient journey through a critical care episode, the evidence drew the Court’s attention to the difficulties of establishing capacity and consent for ICU treatment in both the admission and continuing care for the 80% of emergency/unplanned admissions.9,10 The intervention also drew attention to the ongoing difficulties of predicting the need for additional treatment, making it extremely difficult if not impossible to advise the patient and or relatives of the degree of organ support or the likely experiences and outcome anticipated for an individual. 9 Notwithstanding the potential for DOLS proceedings to harm the relationship between the patient’s family and clinical teams and the fact most patients would be physically unable to leave, the court accepted the submission that retrospective actions to identify, and subsequently refer for authorisation, a potential DOL in what would be a ‘normal’ ICU case would result in a heavy burden to front-line senior medical and nursing staff resulting in a distraction from delivering effective clinical care.9,11 Though such arguments around resource implications alone do not (and should not) generally influence legal obligations, the court did take comfort from avoiding such costs where no policy justification is apparent, accepting that Cheshire West should not apply as it was directed towards long-term care, with the policy justifications cited being absent in urgent life-saving care.
A joint intervention by the Secretaries of State (SOS) for Health and Justice adopted a number of the arguments presented by the ICS and FICM but also argued that Article 5(1)(e) of the ECHR only applies to persons of unsound mind. 12 Thus, in a normal ICU case, a person with a disorder of consciousness, a person with a brain injury or a person temporarily unconscious (with no accompanying mental disorder) are not persons of unsound mind within the meaning of Article 5(1)(e). Citing the inability to prescribe in law a ‘deprivation’ in such cases other than by an application to the Court of Protection (recall the qualifying requirements for DOLS ‘standard authorisation’, see Box 3), they argued that the absence of such lawful remedy is indicative that no such deprivation of liberty exists.
Assessing the merits of the appellant’s principal argument Arden LJ based the primary reasoning for her dismissal of the appeal directly on European Court of Human Rights (ECtHR) jurisprudence and Cheshire West (in contrast to the High Court) and its application to urgent care.
Restriction versus deprivation?
ECtHR case law relating to restriction versus deprivation.
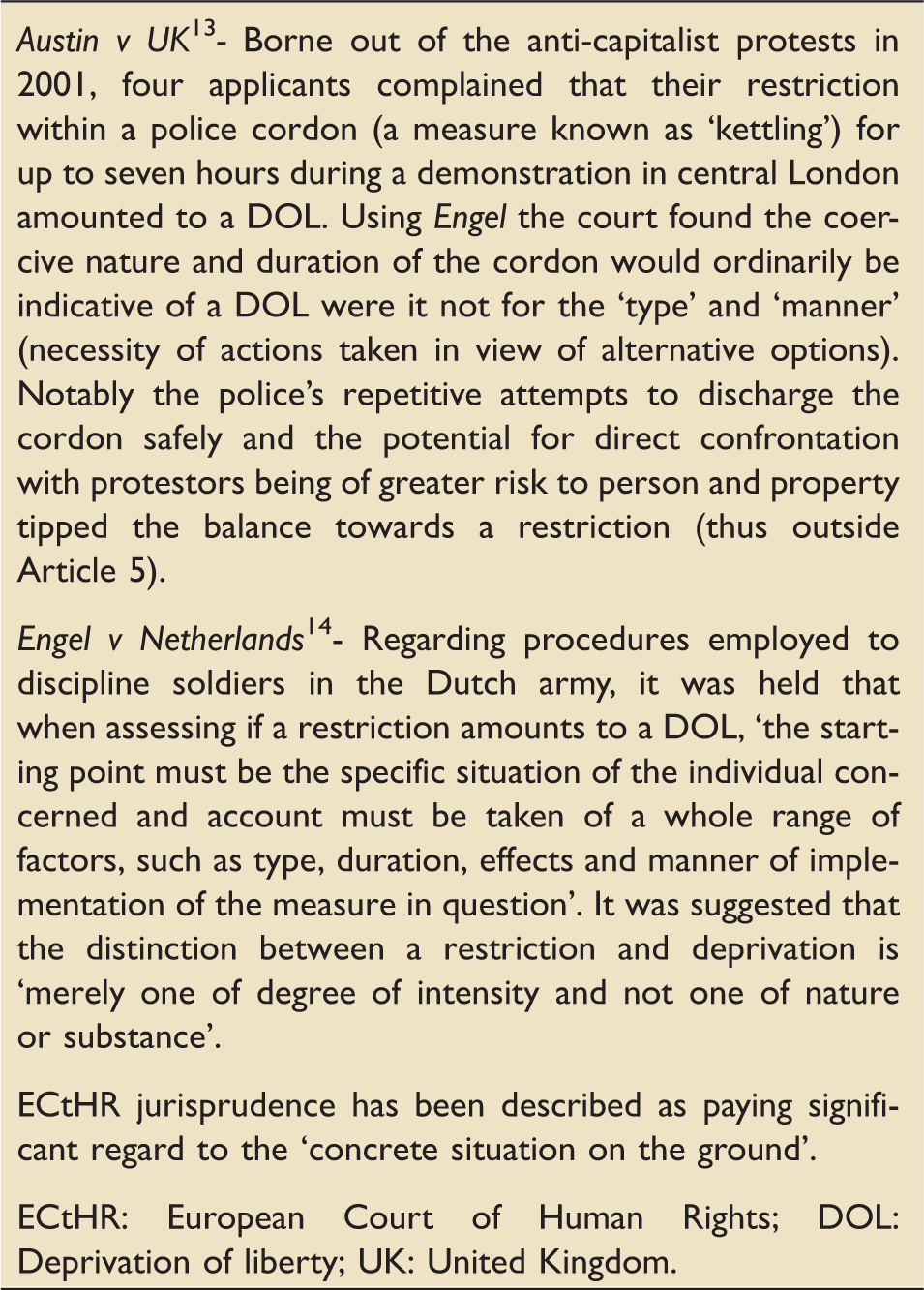
Austin allowed the court to hold that if the interference is outside of the Article 5(1) exceptions, for example provision of intensive care, and the ECtHR reaches the conclusion the interference was justified, then it can conclude that no deprivation of liberty occurred.
Quoting Arden LJ,
‘The Strasbourg Court (ECtHR) looks to the realities of the situation. It accepts that not every interference with a person’s liberty of movement involves a potential violation of Article 5. In Austin [it] has specifically excepted from Article 5(1) the category of interference described as “commonly occurring restrictions on movement”. In my judgment, any deprivation of liberty resulting from the administration of life-saving treatment to a person falls within this category’. 15
Treatment on an ICU is a (relatively) commonly occurring event which can occur to persons of sound or unsound mind without discrimination. So long as the treatment is kept to a minimum required for that purpose and is broadly similar for patients being treated for a physical disorder between those of sound and unsound mind, there is no interference with Article 5.
The Court of Appeal held that Cheshire West is not the governing authority in cases of acute or urgent care, accepting the submissions that it was directed at an entirely different situation providing no guidance in regard to Article 5 in urgent or intensive care treatment. 15
Arden LJ presented a further avenue to reaching the same verdict, if it was established she erred in law. Even if the ‘acid test’ in Cheshire West were to be applied, she concluded the deceased was always free to leave, if there had been a ‘lawful decision to do so’ (for example, the decision of a patient with capacity or that of a court in the case of a patient lacking capacity). 15
Furthermore, Arden LJ dismissed the idea that treatments given on an ICU are generally attributable to the state,
‘… .In the case of a patient in intensive care, the true cause of their not being free to leave is their underlying illness, which was the reason why they were taken into intensive care. The person may have been rendered unresponsive by reason of treatment they have received, such as sedation, but, while that treatment is an immediate cause, it is not the real cause. The real cause is their illness, a matter for which (in the absence of special circumstances) the state is not responsible’. 15
In summary, Ferreira held that urgent life-saving physical treatment can be given to patients lacking capacity in the absence of an underlying mental disorder, or to a patient with an underlying mental disorder as long as the treatment is ‘materially’ analogous to that given to a patient without an underlying mental disorder when the physical illness is not attributable to the state, without a violation of their Article 5 rights.
Discussion
The Court of Appeal’s judgment in Ferreira provides much-needed clarity and a more certain legal basis for regular intensive care practice involving incapacitated patients.
Article 5 and intensive care: post Ferreira.
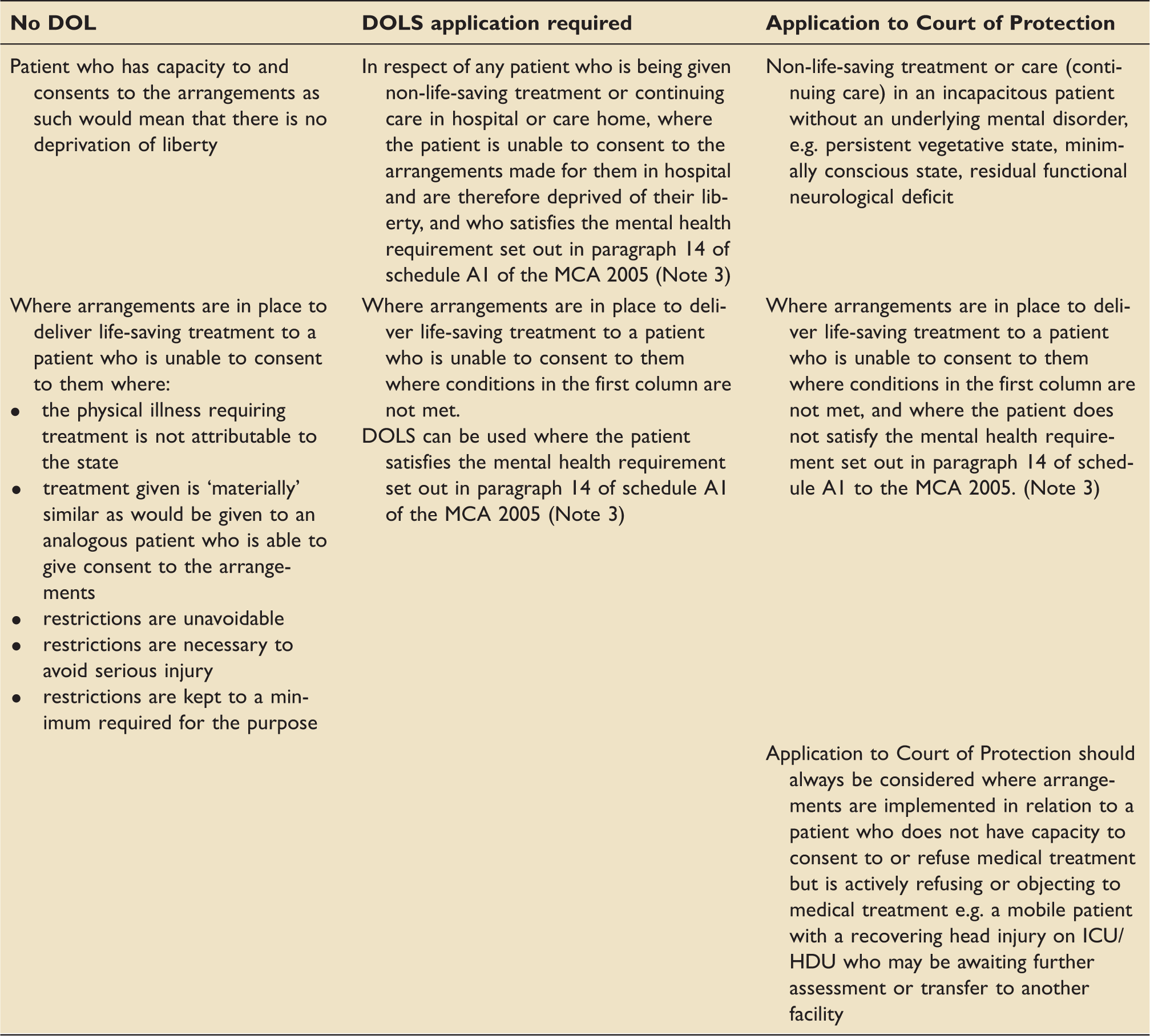
DOL: Deprivation of liberty; DOLS: Deprivation of liberty safeguards; MCA: Mental Capacity Act 2005.
Note (1): this table concerns the circumstances of those who are subject to arrangements which satisfy the “acid test” set down by the Supreme Court in the Cheshire West case, i.e. being under continuous supervision and control and not free to leave.
Note (2): DOLS does not provide authority to treat a patient. Treatment is carried out in the case of those who lack the capacity to consent to it on the basis of the defence contained in s.5 of the Mental Capacity Act 2005 (which also applies to restraint where the additional conditions set down in s.6 are met).
Note (3): Paragraph 14 of schedule A1 of the MCA 2005 22 states:
14 (1) The relevant person meets the mental health requirement if he is suffering from a mental disorder (within the meaning of the Mental Health Act, but disregarding any exclusion for persons with learning disability).
(2) An exclusion for persons with learning disability is any provision of the Mental Health Act which provides for a person with learning disability not to be regarded as suffering from mental disorder for one or more purposes of that Act.
However, Ferreira yields questions that undoubtedly will be the subject of further debate.
The judgment makes no attempt to define what amounts to immediate life-saving treatment. Whilst the onset of life-saving treatment may be straightforward to identify, the inevitable question arises, at what point does immediate life-saving treatment end and continuing care begin, especially in the initial stages post critical illness? Thus, in the absence of recovery of capacity, at what point does Ferreira end and the ceding of Article 5 rights give way to the requirements of Cheshire West for an individual’s treatment?
On the analysis of Arden LJ, a DOL does not occur in a critically ill patient of unsound mind so long as the following caveats are satisfied; that the treatment is not ‘materially’ different to that which would be bestowed on a patient of sound mind and is ‘unavoidable as a result of circumstances beyond the control of the authorities’. Currently, a ‘material’ difference and ‘beyond state control’ have yet to be defined in this context. For example, what if a treatment regimen was specifically tailored to a person of unsound mind that differs from that given to an analogous patient of sound mind, e.g. the timing of tracheostomy to aid weaning from a ventilator? It is unlikely that such a situation, with clinical justification, would be viewed as a ‘material’ difference, especially in the context of life-saving treatment.
In the Court’s judgment, the example given by Arden LJ, which clearly falls outside of the criteria described, was that of NHS Trust I v G. 16 Here, a pregnant woman who lacked the capacity to make decisions about her peri-natal care due to an underlying psychiatric illness was actively objecting to obstetric care and intervention. She was the subject of a judgment that rendered lawful the potential provision of obstetric care to include a Caesarean section and restraint amounting to a DOL which would clearly be ‘materially’ different to that of a woman of sound mind.
A further example might be that of a patient with Schizophrenia who is the victim of self harm or trauma (which may or may not be due to the underlying mental disorder) and requiring life-saving treatment. During the course of treatment there may arise a time when a divergence in the management of such sequelae of critical illness like agitation or delirium occurs. The absence of a competent refusal to continuing ICU treatment may necessitate the use of treatments that are materially different to that employed in a person without a mental disorder in a similar situation, for example physical restraints in addition to pharmacotherapy to control extreme agitation and delirium. Furthermore, the employment of a registered mental health nurse (RMN) in addition to ICU staff to attend a patient being treated outside of the provisions of the Mental Health Act could conceivably be seen by some as coercive in nature and materially different, potentially giving rise to a DOL that would require authorisation. Readers are encouraged to remain vigilant to factors that would be considered ‘atypical’ that arguably take the patient outside of the conditions outlined in Ferreira and thus vulnerable to an Article 5 violation.
Arden’s LJ judgment refrained from establishing a temporal definition as to what amounts to a DOL in part due to the judgment suggesting that in the course of providing life-saving treatment the situation is removed from engaging Article 5 in its entirety. Subsequently, the potential for engaging Article 5 must be realised at the conclusion of the life-saving treatment. This is important in the case of patients who do not regain capacity at the conclusion of their critical illness, e.g. after a cardiac arrest. Such a patient would fall outside of Article 5 at least initially, however there must come a time when a potential DOL borne out of the need to deliver continuing treatment needs to be prescribed by law. Would an ongoing requirement for artificial hydration and nutrition be considered life-saving, thus allowing it to continue indefinitely? This seems somewhat divorced from the spirit of Arden’s LJ judgment, so potential for a DOL may materialise requiring authorisation in due course.
Finally, what of the patient who has a residual disorder of the mind secondary to a physical illness which is reversible, for example delirium? Again, the patient would fall outside of Article 5(1)(e). With respect to ICU delirium, it might be argued that as the presence of delirium is associated with a significant risk of mortality, its diagnosis would indicate that life-threatening illness remains and its treatment would be consistent with Arden’s LJ judgment. The situation clearly changes if such disorder of the mind is deemed to be irreversible or is functional in nature when previous considerations would surface. For example, the patient with a head injury awaiting placement at a rehabilitation facility would be subject to supervision and prevented from leaving (and on occasion submitted to restraint) on an ICU but their treatment would not be considered as life-saving. In effect, if the ICU is to be utilised as a ‘place of safety’ for a person within the hospital because of its ability to provide continuous supervision and control then a DOL is likely to materialise.
Consequently, Ferreira is not a ‘fait accompli’, and it is imperative for the ICS, FICM and other professional stakeholders to remain engaged with the Law Commission and government in their review of legislation in this area. Illustrating the pace of recent developments, the Law Commission recently published draft legislation which would see the scrapping of the DOLS system and its replacement with a new scheme called the ‘Liberty Protection Safeguards’. 17 Whilst still at an embryonic stage and some way from a final Act of Parliament, it would legislate for the temporary authorisation of a DOL in ‘urgent cases’ by an Approved Mental Capacity Professional for a period of up to 14 days, though it steers clear of defining a DOL.
The draft legislation also proposes an amendment to section 4B of the Mental Capacity Act (MCA) 2005 allowing for acts, such as restraint, that amount to a DOL in an emergency situation to prevent serious harm to the patient. Readers are reminded that the MCA 2005 does not currently provide any defence for acts that might amount to a DOL (section 5 and 6), thus clinicians have voiced concerns regarding the deployment of such restraints due to the risk of fluxing from a lawful restriction to a potentially unlawful deprivation. 18 However, whether or not the Liberty Protection Safeguards in their envisaged form will ever reach the statute book and what form this might entail remains uncertain as government legislative priorities may lay elsewhere after the general election. The Conservative’s manifesto commitment to a new Mental Health Bill may also be a complicating factor if they are returned to government. 19
Notably Arden LJ does not suggest that a DOL can never occur in respect of hospital treatment and it is likely that this judgment does little for our colleagues involved in the longer term treatment of incapacitated patients. It also does not give a defence to potential Article 5 infringements borne out of prolonged hospital admissions for non-medical reasons (for example social care placement issues).
The Supreme Court judgment in Cheshire West opened a Pandora’s box of extraordinary legal argument and analysis, some of which at times appeared divorced from the real world. The Court of Appeal has, for now at least, emphatically offered some common sense by providing a simple and eloquent analysis as to why Cheshire West does not as a matter of course extend into urgent medical care, without negating the very essence of the right in question.
However, significant questions remain. The Austin case somewhat relied upon in this judgment was highly controversial in itself, with some legal observers describing it as an ‘anomaly’. 20 It could also be argued that the position of a patient lacking capacity on the ICU is not easily reconcilable with the judgment in HL v UK, 2 where it was concluded that the long-held doctrine of ‘necessity’ did not provide a voluntary patient with sufficient protection against an ‘arbitrary’ DOL. Furthermore, there remains a significant issue around the concept of ‘freedom to leave’ with the Court of Appeal having previously (in the context of social care) ruled that a person’s physical disability does not take them outside the scope of Article 5. 21 The appellant has been refused permission to appeal by the Supreme Court (the same court that gave us Cheshire West), therefore it appears that Ferreira is the authoritative interpretation of DOL and the ICU – for now at least.
Footnotes
Acknowledgements
The authors would like to thank Alex Ruck Keene and Ben Troke for their invaluable contribution in proof reading and suggesting amendments to this manuscript. Any errors of legal fact are entirely the responsibility of the authors.
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: D Bryden provided the clinical submission to the Court of Appeal in Ferreira on behalf of the ICS and FICM; at the time SJ Brett was President of the ICS.
Disclaimer
Whilst the authors have endeavoured to ensure the content herewith is correct, the information contained is intended for information only, are the views of the authors and is not intended to construe or replace formal legal advice.