
Abstract
Chronic lymphocytic inflammation with pontine perivascular enhancement responsive to steroids (CLIPPERS) has been described in multiple case reports since it was first described in the literature in 2010. The patient described is a 54-year-old man with no significant medical history who presented with ataxia, diplopia and hearing and taste disturbances. His GCS reduced to the point at which he required intubation and he was treated for 50 days on an intensive care unit. The patient’s course also includes seizures, first described in 2014, and central pyrexia, which has not been previously described in case reports of CLIPPERS. Intravenous methylprednisolone resulted in a rapid and significant recovery; neurological rehabilitation is ongoing 10 months from diagnosis. The importance of recognition of unusual radiological findings and rapid treatment cannot be overemphasised in improving patient’s long-term outcomes.
Introduction
Chronic lymphocytic inflammation with pontine perivascular enhancement responsive to steroids (CLIPPERS) was first described as a syndrome made up of clinical and radiological findings by Pittock et al. 1 CLIPPERS is a neurological syndrome of uncertain aetiology; symptoms include diplopia and gait ataxia, and pontine lesions are a common feature seen on magnetic resonance imaging. Patients display a favourable response to glucocorticosteroid therapy. 1 CLIPPERS tends to be a diagnosis of exclusion, with patients often initially treated for stroke, encephalitis, multiple sclerosis or Wernicke’s encephalopathy. 2 There is evidence to suggest that prompt treatment may reduce the need for long-term immunosuppressant therapy, although others argue that CLIPPERS is by its nature relapsing–remitting and therefore lifelong treatment is required.3–5 There have also been multiple cases of CLIPPERS which have been fatal. 6 It appears to have a relationship with patients proceeding to develop B-cell lymphoma, although there is debate as to whether this can be attributed to misdiagnosis of the initial presentation. 7 This new case of CLIPPERS is presented to increase awareness of the condition so that future patients may receive appropriate, effective treatment in a timely manner. The patient also had features such as seizure activity and central pyrexia which are less commonly described in the literature.
Case
A 54-year-old male presented to the emergency department with a 10-day history of vomiting and feeling generally unwell. During this time, he had also developed dizziness, ataxia and diplopia. He also described taste and hearing disturbances. On examination, he had bilateral nystagmus and marked gait ataxia. Within 24 h of admission, he had developed right-sided weakness. He became less responsive and GCS decreased to 8 (E1, V2, M5), at which point the patient was transferred to the intensive care unit, where intermittent apnoea and airway compromise resulted in tracheal intubation. Downgoing plantar reflexes and myoclonic jerks were noted on examination.
A CT head from day 1 showed no evidence of intracranial pathology. Bloods on admission were largely normal except for a white cell count of 17 × 109/L, neutrophils of 15.6 × 109/L and an elevated C-reactive protein (256 mg/L). Lactate dehydrogenase was 345 U/L. Serum immunoglobulin (Ig) G was slightly decreased at 4.3. IgA and IgM were normal. Cerebrospinal fluid taken on day 2 showed a white cell count of 96 (40% polymorphs and 60% lymphocytes). No organisms were found and viral PCR and cryptococcal antigens were negative. All blood, urine, sputum and cerebrospinal fluid cultures and viral screens were negative. Angiotensin converting enzyme, anti-gangliosides, beta-human chorionic gonadotropin, prostate specific antigen, antinuclear antibody (ANA), extractable nuclear antigen, perinuclear antineutrophil cytoplasmic antibodies, cytoplasmic antineutrophil cytoplasmic antibodies, anti-glomerular basement membrane antibody, liver kidney microsome type 1, antimitochondrial antibody, smooth muscle antibody, nuclear ANA, lupus anticoagulant, complements, anti-cardiolipin, Bence-Jones protein and beta-2 microglobulin were negative. A bone marrow biopsy to rule out intravascular lymphoma was negative. The patient was treated as a potential encephalitis and commenced amoxicillin, ceftriaxone and acyclovir.
Seizure activity was observed such as dilatation and constriction of pupils, tonic-clonic movements of lower limbs and spasticity of both upper and lower limbs. Seizures occurred on a daily basis and were terminated with intravenous administration of lorazepam as required. EEG confirmed seizure activity. Intravenous phenytoin was successfully used to prevent further seizures.
Although the initial CT head had been inconclusive, an MR head was performed on day 5, showing potential inflammatory or infective changes to the dorsal part of the pons, the cerebellar peduncles and the region of the nucleus dentatus. A stroke was once again excluded. Following the patient developing a pyrexia 42℃ on day 14, a second MR was done on day 15. The findings were largely unchanged, and reported as likely due to inflammation or a paraneoplastic syndrome (Figure 1). No new source of infection was found, and the patient required internal and external cooling for seven days.
MR head day 15.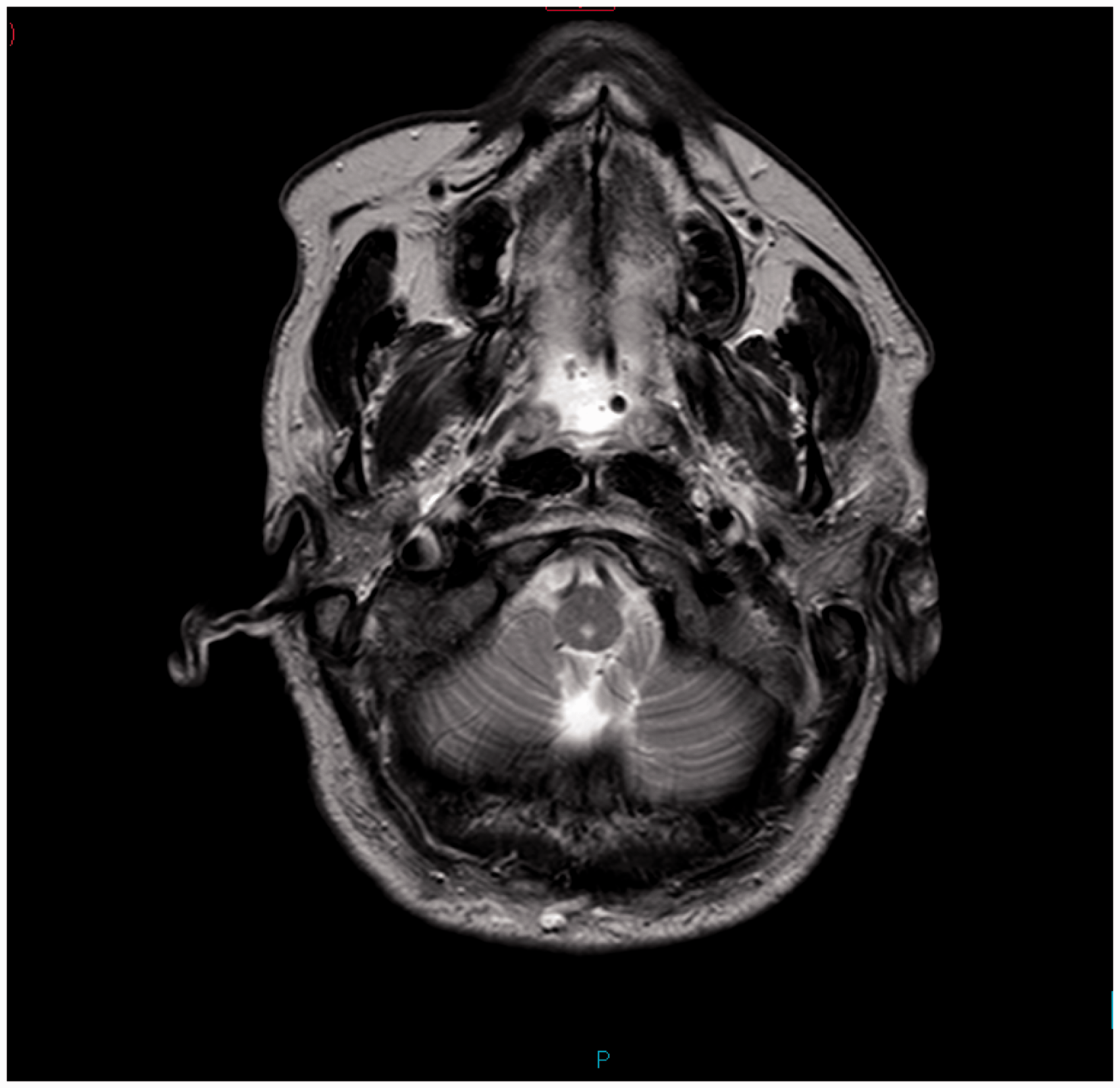
The patient remained intubated and ventilated until day 30, when a third MR was done and reviewed by a regional neuroradiology team. Unlike the previous scans, this was done with contrast, and was compared to the previous imaging. Several irregular regions of enhancement within the midbrain and pons were identified, and for the first time, CLIPPERS was suggested as a differential diagnosis (Figure 2).
Images from day 30 MR head with annotation from neuroradiology MDT, showing enhancement within the midbrain and pons.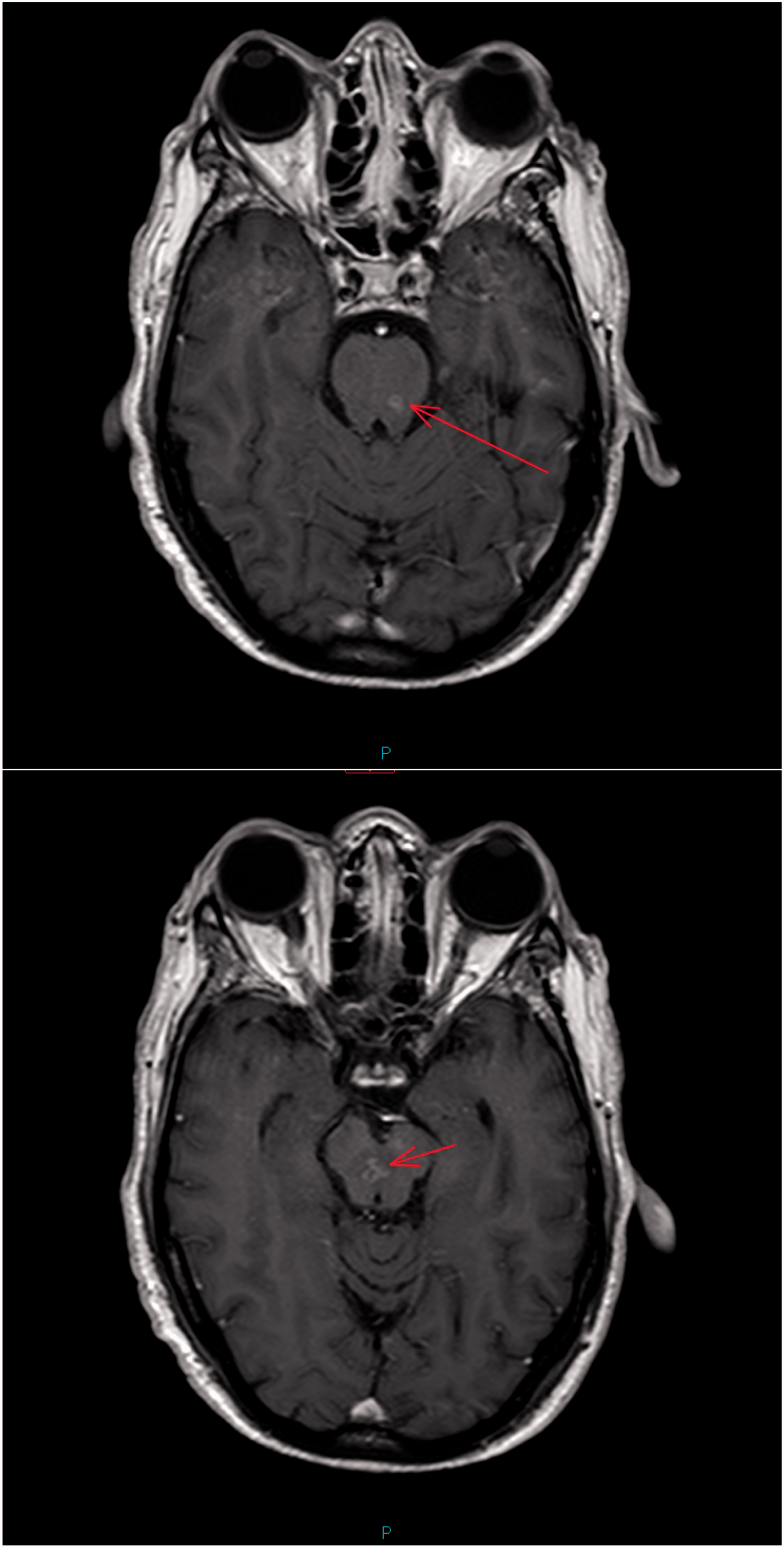
Following this, treatment was commenced with methylprednisolone 1 g intravenously. An almost immediate improvement was seen in the patient’s clinical condition. He was alert and able to follow commands within several days, although unable to speak due to a tracheostomy. Nystagmus persisted but he had no further spasticity. His motor function was further impaired by the significant muscle wasting that had occurred during his long stay on intensive care. Intravenous Ig had also been started (0.4 g/kg/day) at the same time as steroids but were stopped following the correlation with the patient’s clinical improvement on steroids.
A second lumbar puncture was done on day 38, seven days after methylprednisolone was started. This had a white cell count of 72 (5% polymorphs and 95% lymphocytes). Again, no organisms were found.
When the patient no longer required mechanical ventilation, he was transferred from the intensive care unit to the high-dependency unit, where his condition continued to improve. He had required a tracheostomy during the respiratory wean but this was removed on day 70, and the patient was able to breathe and talk normally. Intravenous methylprednisolone was changed to oral prednisolone at 60 mg daily. This was reduced to 50 mg daily and the patient continued to improve. Over the course of several months, oral steroids have been weaned down and discontinued. Intravenous Ig were given periodically over several months, but this did not appear to make a marked difference to the patient’s recovery, in line with other literature. 8
Intensive neurological rehabilitation was required and is ongoing, 10 months from presentation. Swallowing difficulties have persisted and the patient has had recurrent aspiration pneumoniae. However, he continues to make progress, and it is thought that this will improve with ongoing rehab.
Discussion
The tentative diagnosis of CLIPPERS was made following the patient’s second MR scan on day 30, after the exclusion of other pathologies and a failure to respond to other therapies. Other case reports do not appear to describe the length of time between onset and diagnosis, but in this patient’s case it was 30 days before steroid therapy was commenced.
The patient in this case report had a significantly reduced GCS and required airway support for several weeks. Other cases describe a relapsing–remitting course of ataxia, diplopia, dysarthria and paraesthesia. No case reports have been found where symptoms were severe enough for organ support to be required, and for the patient to then go on to recover from the disease.
Pyrexia has not previously been reported in cases of CLIPPERS. Central pyrexia has been well described in patients requiring neurological intensive care, particularly those with subarachnoid haemorrhage and vasospasm. 9 It is possible that an infective source was not found; however, in the absence of cultures and a failure to respond to antimicrobials, central pyrexia appears more likely. The significance of this remains to be seen but may indicate another aspect of CLIPPERS syndrome which becomes more evident as further research is undertaken.
Seizures in CLIPPERS were only reported for the first time in 2014. 10 Seizure activity in this patient was occurring on a daily basis, with episodes lasting up to 10 min. Intravenous phenytoin successfully controlled seizures in this patient. Oral phenytoin was continued for several months and eventually discontinued. The patient has had no further seizures since stopping anticonvulsant therapy.
Other case reports describe patients with histories of allergies, 11 pre-existing neurological conditions such as multiple sclerosis, 12 or lymphoma 13 ; however, this patient’s only previous complaint was lichen planus of the scalp.
Remission was successfully induced by intravenous steroid therapy and this has been described in the majority of the literature available. In evidence drawn from the management of vasculitis, immunosuppression is recommended to continue for 2–5 years14,15; however, this patient is not currently on immunosuppressive therapy. He remains under the care of a physician and is undergoing regular review.
Conclusion
Despite the growing number of case reports about CLIPPERS, new and less common features are still being described. However, all successful treatment of CLIPPERS involves intravenous steroid use followed by maintenance therapy. It would be helpful if other case reports would include the length of time between onset and therapy so that the potential effect of delays on long-term outcomes can be evaluated in future. However, due to the rarity of CLIPPERS and the importance of excluding other causes, delays are inevitable. This case also suggests that MR scans in patients with unusual clinical features or less-common radiological findings involving the pons should be reviewed by a specialist neuroradiologist and that the use of contrast in scans may facilitate image interpretation. It could be argued that the threshold for trialling IV steroids in similar patients could be lower. As many patients with CLIPPERS respond positively within five days, it may be worth trialling in patients with atypical neurological symptoms and radiological appearances, particularly if they are as unwell as the patient described above. It remains to be seen whether seizures and central pyrexia appear in future case reports of this complex and unusual neurological condition.
The pathophysiology of CLIPPERS is poorly understood. Increased cerebrospinal fluid protein levels, the absence of pleocytosis, contrast-enhancing MR lesions and good response to steroid suggest an immune-mediated disease. Pathologic studies (brain biopsy and a limited number of post-mortem examinations) have shown T-cell infiltration of the brainstem, with the pons being the area most affected. On post-mortem, lesions were seen at different stages of evolution, suggesting a relapsing–remitting disease. 8 Epstein-Barr virus has been seen in several cases, including one which progressed to intracranial lymphoma. Other authors have hypothesised that CLIPPERS may be a pre-lymphoma condition and have emphasised the importance of continued follow-up to monitor long-term outcomes. 16
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Consent
Consent for the case report was obtained verbally from the patient and in writing from the next-of-kin.