
Abstract
A patient suffered significant bleeding during an attempt at percutaneous dilatational tracheostomy due to an aberrant anterior jugular vein. Bleeding was controlled with pressure temporarily, but quickly returned necessitating conversion to an open technique. We present an algorithm for the management of significant peri-procedural bleeding during this procedure.
Case report
A 56-year-old male was admitted to the ICU from the Emergency Department following a road traffic accident. His injuries included a left sided pneumothorax, T2-T7 flail segment, pulmonary contusions, open humeral fracture and a depressed conscious level. After initial resuscitation, the patient was transferred to the operating theatre for management of his open fracture. An initial CT of the cervical spine showed no injury and there was spontaneous movement in all limbs prior to intubation, so the cervical spine was cleared.
On arrival in theatre, approximately 1 L fresh blood drained in to the intercostal drain and a Video-Assisted Thoracoscopy (VATS) was performed. To facilitate this, an attempt was made to replace the endotracheal tube (ETT) with a double-lumen tube. This was difficult to place due to glottis swelling and eventually a size 7 standard ETT was sited. No active bleeding was found during the VATS procedure and the patient returned to the ICU.
During the next day, it became impossible to pass endotracheal (ET) suction catheters down the tube, and with the known upper airway problems, the patient was prepared for percutaneous dilatational tracheostomy (PDT) in the operating theatre. In accordance with local unit policy, the risks and benefits of PDT were discussed with the next of kin and the procedure carried out under the Adults with Incapacity (Scotland) Act 2000. The decision to perform the procedure in theatre was made due to the known upper airway difficulties, to have anaesthetic assistance available in case of airway loss.
The patient was positioned supine with slight neck extension. Under bronchoscopic guidance the ETT was withdrawn to the level of the glottis. The surgical site was prepared with chlorhexidine skin prep and Lignocaine 2% with 1:80,000 adrenaline infiltrated in the subcutaneous plane. A 1 cm transverse skin incision was made in the midline of the neck at the level of the second and third tracheal rings. Using an artery forcep, blunt dissection was carried out down to the pre-tracheal fascia with good haemostasis.
The trachea was then punctured on first attempt with the introducing needle and guidewire passed without difficulty. Needle and wire position were confirmed on bronchoscopy and there was no external or internal bleeding evident at this point.
The initial small dilator was inserted smoothly and confirmed on bronchoscopy. On removing the dilator, there was brisk bleeding into the surgical field. Immediate pressure was applied; however, after 1 min of continuous pressure, bleeding continued on removal of the swabs.
Pressure was reapplied and assistance requested from the senior head and neck surgeon on call. The guidewire was left in situ and the ETT advanced under bronchoscopic guidance, to the normal position and the cuff inflated. Haemodynamic stability was maintained throughout.
On arrival of the surgical team, the transverse incision was extended. The left anterior jugular vein was identified first in the expected lateral position, within the subcutaneous plane. The right anterior jugular vein was noted to be more medial, over-lying the trachea in the subcutaneous plane. There was a small oval puncture in the side wall of this vessel causing the haemorrhage. This was ligated and haemostasis achieved. An open tracheostomy was completed uneventfully.
The patient returned to the unit with no long-term sequelae or requirement for blood transfusion. Blood loss was estimated at 100–200 ml.
Discussion
PDT is a safe and very common procedure in ICUs across the UK. Significant bleeding, airway loss and death are well described, but are thankfully rare sequelae of this relatively common procedure. Studies have produced varying rates of complication, mainly due to inconsistencies in definition, but is usually quoted as being 11–18.2%1,2 with the majority of these being minor complications, such as peristomal oozing.
Although the majority of bleeding is minimal, there is the potential for more severe and catastrophic bleeding. In one study of 497 cases, bleeding complicated the procedure in 24 cases (4.8%), with six of these requiring conversion to an open tracheostomy. 3 Furthermore, PDT was found to be associated with a 0.17% incidence of lethal complications, most of which were due to bleeding (38%), with 31% of haemorrhagic deaths occurring at the time of insertion. 4
Despite this being the most common complication of tracheostomies, teaching focusses on the management of the displaced or blocked tracheostomy and any guidance on the management of haemorrhage discusses the late haemorrhage, rather than peri-procedural bleeding.5,6 There is little in the literature regarding the management of bleeding during PDT. We have produced a simple algorithm to assist the intensivist encountering significant bleeding during PDT (Figure 1).
Algorithm for bleeding during PDT.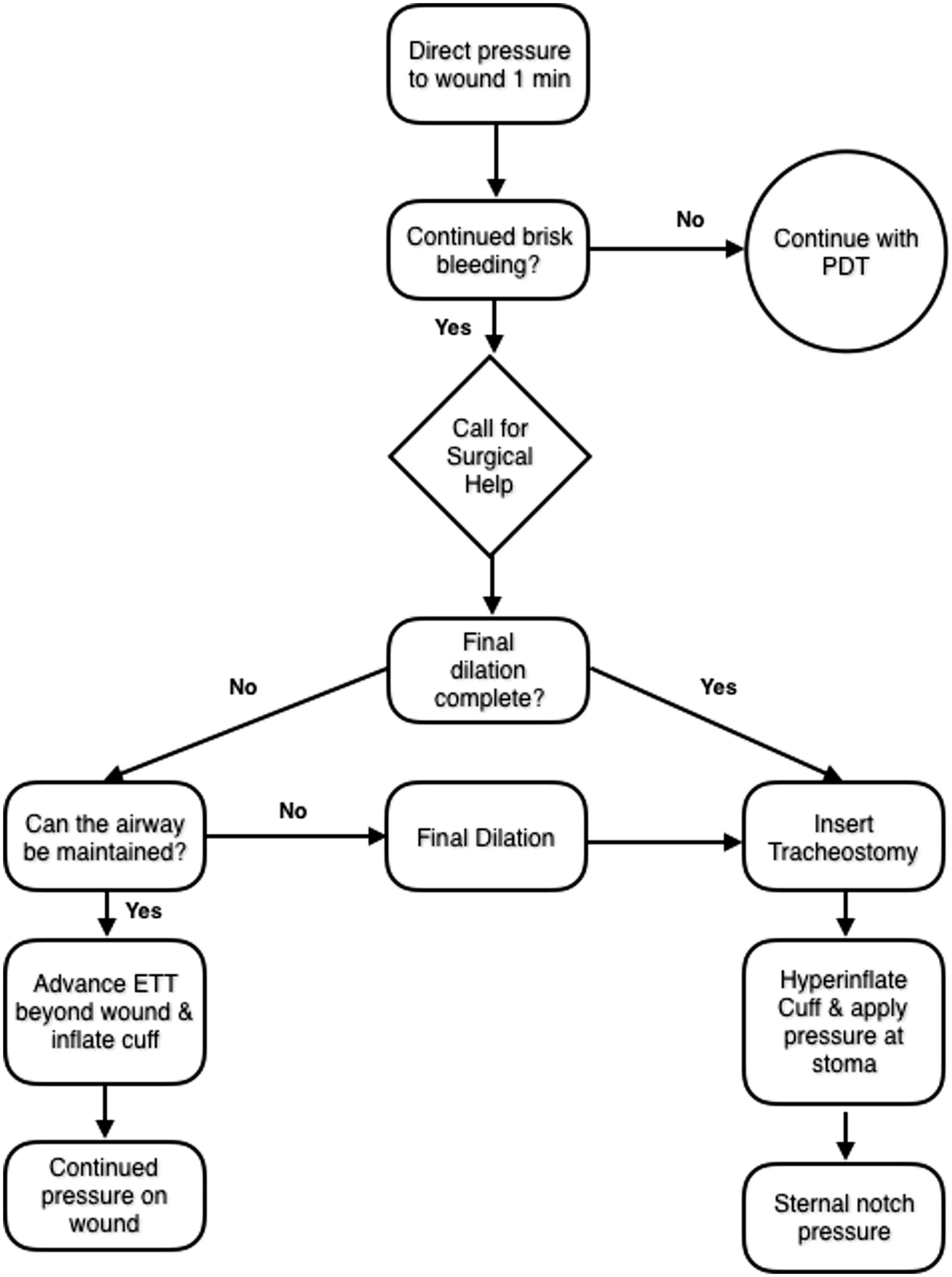
Planning for complications
Although not usually performed by surgeons, PDT remains a surgical procedure and should be treated with the same precautions to one performed in the operating theatre. Use of the World Health Organisation (WHO) surgical checklist can assist teams in preparing for rare but significant complications, such as airway loss and major bleeding.
Several patient-related risk factors are associated with increased risk of peri-procedural bleeding. Inability to palpate the tracheal rings, previous neck/mediastinal surgery or irradiation, goitre or the presence of any obvious overlying vessels should be considered red flags and the patient should be discussed with ENT/Maxillofacial Surgery regarding potential for surgical tracheostomy.
Consideration should also be given to the availability of surgical support. For this reason, PDT should not routinely be performed out of hours and local plans should be in place for appropriate surgical referral in hospitals without ENT or Maxillofacial cover.
Management of bleeding during PDT
With the use of vasoconstrictor/local anaesthesia mixes prior to commencing, there should be minimal blood loss during the insertion. A brisk bleed obscuring visibility should raise the possibility of vessel injury.
Potentially injured structures during PDT.
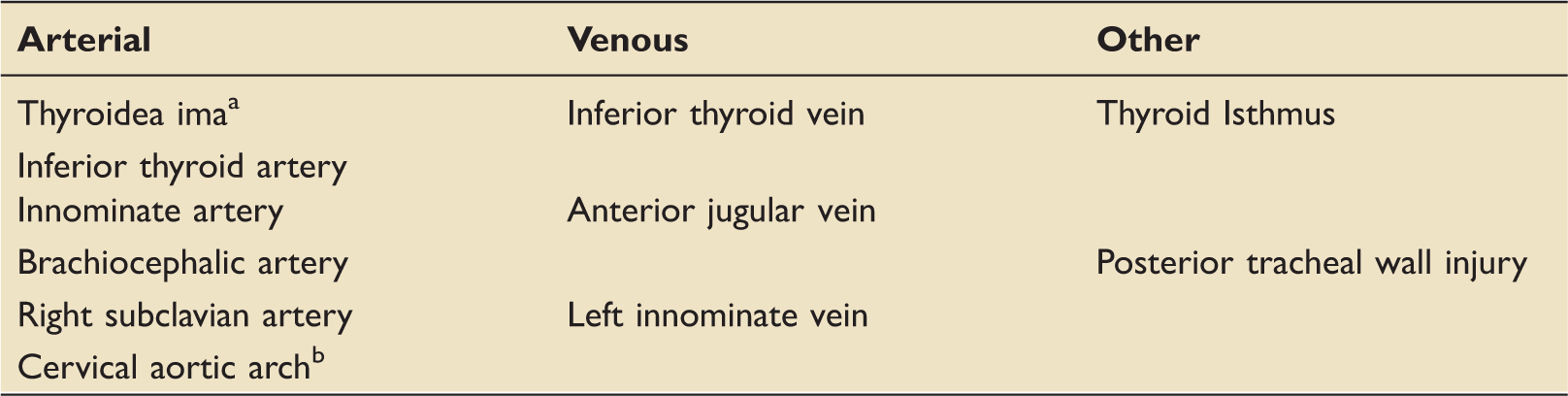
PDT: percutaneous dilatational tracheostomy.
Present in 3% of patients.
Rare congenital anomaly with arch extending outside mediastinum.
Once significant bleeding is identified, the initial response should be a period of direct digital pressure over the tracheostomy site and this is usually sufficient in the case of small vessel injury. 3 If the guide wire has already been placed, this should be left in situ to allow insertion of a dilator to tamponade any bleeding and assist with rescue airway access.
In case of failure for digital pressure to achieve haemostasis, reapplication of pressure should be performed and immediate referral for Ear, Nose & Throat (ENT) or Maxillofacial assistance made. While awaiting the surgical team's arrival, priorities should be to ensure a protected, patent airway while maintaining pressure on the wound. Blood should be immediately cross-matched and large bore venous access secured, with staff identified to manage any resuscitation, allowing the operators to focus on securing the airway and haemorrhage control.
To assist the surgical team, emergency theatres should be notified and tracheostomy equipment made available with a selection of tracheostomy and endotracheal tubes. If the patient cannot be transferred to theatre due to clinical reasons or lack of theatre availability, then tracheostomy equipment, diathermy, suction and appropriate lighting must be available in the ICU.
If the airway is able to be secured and the final dilation has not been performed, the ETT should be advanced under bronchoscopic guidance past the puncture site and the cuff inflated. During this time, the airway should be inspected for significant soiling with blood, and should be suctioned as needed to maintain airway patency whilst simultaneously maintaining external pressure on the bleeding point.
If the airway is unable to be secured, or the ability to oxygenate or ventilate is impaired, securing the airway should take priority and the wound dilated up normally.
This dilation may confer a degree of tamponade to the bleeding point; however, there is the risk that dilating may cause further vascular injury, resulting in more significant haemorrhage. If this does not improve the bleeding, the tracheostomy should be inserted and the cuff hyperinflated to protect the airway and provide a degree of tamponade. On insertion of the tracheostomy, the operator should immediately apply pressure around the stoma. If bleeding is not controllable, then pressure should be applied at the sternal notch to compress the innominate artery.
Pressure is likely to temporarily arrest a bleeding point for most venous or small arterial bleeds until the surgical team arrives. Of concern is large arterial or major vessel injury, where the increased pressure may result in haematoma formation and airway soiling. Securing the airway early allows the operating team to focus on management of the haemorrhage and appropriate fluid resuscitation, while awaiting expert surgical assistance.
Once the airway is secured and the bleeding arrested, fibreoptic bronchoscopy should be performed to evaluate the degree of airway soiling and perform respiratory toilet, preventing later complications such as lower airway obstruction secondary to clots. Bronchoscopy also allows for confirmation of appropriate tracheostomy placement and confirmation that haemorrhage has been controlled.
Can this be prevented in the future?
A thorough assessment should be performed in all patients undergoing PDT, including an examination of the neck for identifiable landmarks or obvious vessels. This should be done in the position that the procedure will be performed in to allow for movement from the neutral position.
Previous imaging, especially CT scans, should be reviewed for the presence of any problematic vessels, but it should be remembered that the scan will be performed in the neutral position and not reflect the anatomy at the time of PDT.
There has been much debate in the intensive care literature regarding pre-procedural ultrasound (US) to identify problematic neck vessels in patients undergoing PDT.7–9 Despite the technique being described in 1998, there is no data to guide on how widespread the use of procedural US is in UK practice.
Although the use of US has been shown to be safe and useful at identifying aberrant vessels, 7 no studies have shown a reduction in peri-procedural bleeding compared to landmark technique.8,10 This is acknowledged by a joint statement from the Royal College of Anaesthetists (RCoA) and Faculty of Intensive Care Medicine (FICM) after the death of a patient due to bleeding after Minitrach placement. 11
Conclusion
PDT is a safe and reliable technique and although significant bleeding during PDT is rare, having a plan on how to arrest bleeding while specialist assistance is sought is essential for when the situation occurs. We believe the above plan of prioritising the airway, while applying direct pressure provides a safe and effective method of arresting bleeding in the hands of non-surgical operators. Ultrasound remains a potential option for the operator to be fully aware of any vulnerable structures; however, studies are yet to prove that its use is associated with a lower incidence of bleeding complications.
Footnotes
Patient Consent
Written consent has been obtained from the patient for publication.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.