
Abstract
Background
Hospital admissions with decompensated chronic alcoholic liver disease have been increasing, leading to increased pressure on intensive care unit services.
We aimed to determine the outcome and prognostic factors for patients with alcoholic liver disease requiring admission to intensive care unit.
Methods
This was a retrospective study over 5 years (January 2006–December 2010) of all intensive care unit admissions with alcoholic liver disease to either of the two Leeds Teaching Hospitals NHS Trust general intensive care units. A detailed case note review was conducted based on a pre-established proforma. Eighty-two patients included. Primary outcome was hospital mortality.
Results
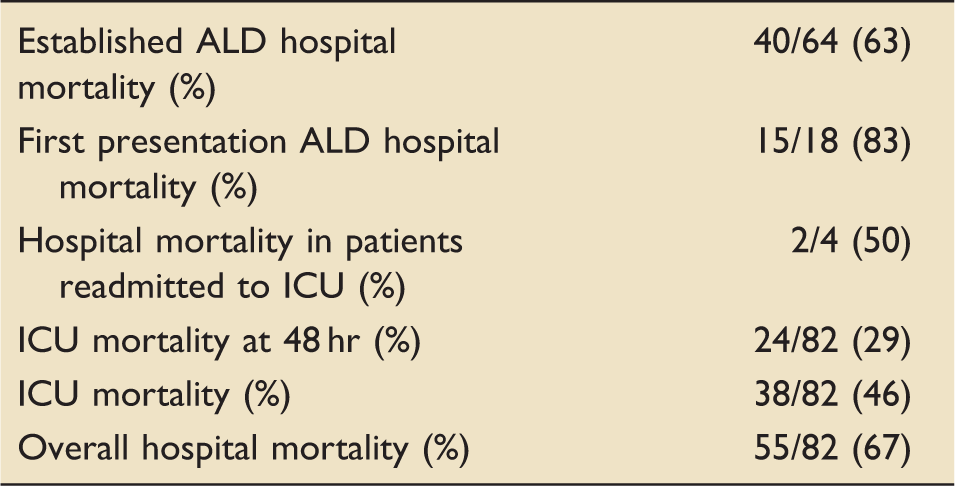
The overall intensive care unit and hospital mortality were 46% and 67%, respectively. Hospital mortality in patients successfully discharged from intensive care unit with the intent of recovery remained high at 21%. Variceal bleed was the only indicator that had a mortality <60%. Factors which suggested a poor outcome included sepsis (86% mortality) and hepato-renal syndrome (86% mortality). A Sequential Organ Failure Assessment score of greater than 10 on intensive care unit admission was associated with 97% hospital mortality. Sequential Organ Failure Assessment score increased from a mean of 10.9–12.5 in those that did not survive hospital. Patients with first alcoholic liver disease related admission had poorer outcomes.
Conclusion
These results are similar to previous studies with no significant improvement in outcomes. Alcoholic liver disease is not a contra-indication to intensive care unit admission but assessment of the individual patient is required. The most appropriate objective factors to guide prognostication are the presenting intensive care unit diagnosis and Sequential Organ Failure Assessment score. First presentation of alcoholic liver disease is not a positive prognostic indicator.
Introduction
In England, alcohol related hospital admissions exceeded one million in 2012/2013 of which over 50,000 were for alcoholic liver disease (ALD). Alcohol contributed to over 20,000 deaths in 2012 and was a direct cause in 6490 with over 5500 of these being caused by ALD and alcohol related cirrhosis. 1
Whilst the proportion of the population who are drinking has decreased, over 50% of those who do consume alcohol exceed recommended daily amounts, with over 20% drinking more than twice recommended amounts in 2012. 1
Data from the Intensive Care National Audit and Research Centre (ICNARC) Database published in 2008 estimated that there were over 1500 intensive care unit (ICU) admissions with ALD in 2005. This correlates with an annual expenditure of over 14.5 million. 2 Despite these figures there is surprisingly little published literature about ALD and ICU outcomes. The largest UK-based cohort study is from data that are nearly 15 years old. 3 Consequently, we aimed to provide more up to date data on ALD-related mortality in ICU from our own patient cohort, specifically looking at prognostic indicators within the patient’s presenting condition and subsequent clinical course.
Methods
A retrospective observational cohort study was performed on all patients admitted to an ICU bed across the Leeds Teaching Hospitals NHS Trust over a 5-year period between January 2006 and December 2010. The methodology of the study was discussed with a member of the local Research and Ethics committee and no formal Ethics committee approval was deemed necessary. The study size was set at either 100 patients or the entirety of a 5-year period, which ever came sooner. This was intended to match a previous similar study. 3
Our primary aim was to evaluate all cause hospital mortality in this group of patients. Secondary outcomes included assessing disease severity scores with a view to identifying predictive factors for survival from ICU and hospital discharge to guide clinical management decisions.
Leeds Teaching Hospitals is one of the largest NHS Trusts in the UK, with over 3000 beds, serving an inner city population of 800,000 people providing secondary and tertiary services across virtually all clinical specialities. There are over 75 Critical Care beds across two University Hospital sites, one of which (St James’s University Hospital) contains the Regional Liver Transplant Centre, and is the tertiary referral centre for hepatobiliary disease. At the commencement of the study both sites accepted unselected medical admissions with ALD patients coming under general Gastroenterology teams.
Patients were identified through a number of sources: the admissions books for the ICU’s were screened for all patients with an ALD diagnosis or admitted under a Gastroenterology consultant, the ICU database was screened for likely ALD diagnoses or Gastroenterology consultants. Full notes were requested for all patients identified as potential candidates for the study. If notes had been destroyed the scanned records were accessed. Additional data were obtained from the laboratory results servers, electronic radiology system and from ICU observation charts. Only a patient’s first ICU admission during that hospital stay was used for data analysis, though information regarding subsequent ICU admissions was collected, as was their ultimate outcome (hospital mortality or discharge). If the patient was discharged from the Trust and subsequently readmitted, this was recorded as a separate admission.
The initial identification of a diagnosis of ALD was based upon documentation by the gastroenterology or ICU team caring for the patient. This diagnosis was reviewed in all cases by the investigators through an examination of the clinical history and liver screening investigations. A history of chronic excess alcohol consumption and proven liver damage in the absence of another cause was sought. Patients were excluded if, in the opinion of the reviewers they did not fulfil clinical criteria for a diagnosis of ALD (e.g. bleeding duodenal ulcer or non-alcohol related liver disease) or if the ALD diagnosis was incorrect or incidental (e.g. heavy alcohol consumer with acute surgery who had no liver dysfunction and no preceding history). Patients under the care of the specialist transplant or hepatobiliary services were not included. This was to improve the applicability of our results to general gastroenterology services in District General Hospitals. All notes used in the final results were scrutinized personally by one of two investigators (AS/PJ). Any potential discrepancies or anomalies were discussed and consensus decisions reached by the two reviewers. All data were collected on the pre-agreed data form, and every form was completed or reviewed by one of the two investigators.
Data to be collected was based upon previous published studies and was decided a priori. We collected data for both Intensive Care scoring systems and liver disease scoring systems, but prioritized Sequential Organ Failure Assessment score (SOFA) and Model for End-Stage Liver disease (MELD) as these have previously been identified as potential prognostic markers for patients with ALD. 4 Multiple calculation tools for these scoring systems are available online.
Statistics
Statistical analysis was performed using SPSS for Windows version 16. Descriptive statistics were applied to patient demographics. Continuous data were reported as mean or median (interquartile range) and differences evaluated with the Mann–Whitney U test. Categorical data were reported as whole number and percentage (%) and differences evaluated with chi-squared tests. Associations between predictive factors and mortality outcome were expressed as percentage of the mortality or survivor group. Correlation with mortality was analysed with Mann–Whitney U test and Pearson’s correlation coefficients as appropriate. Child Pugh, MELD and SOFA scores were calculated at time of ICU admission and after 48 hr stay within ICU. MELD was also calculated at hospital admission. Each score was evaluated against mortality using receiver–operator characteristic (ROC) curves. Both ICU and hospital mortality were calculated, the latter being the primary outcome.
Results
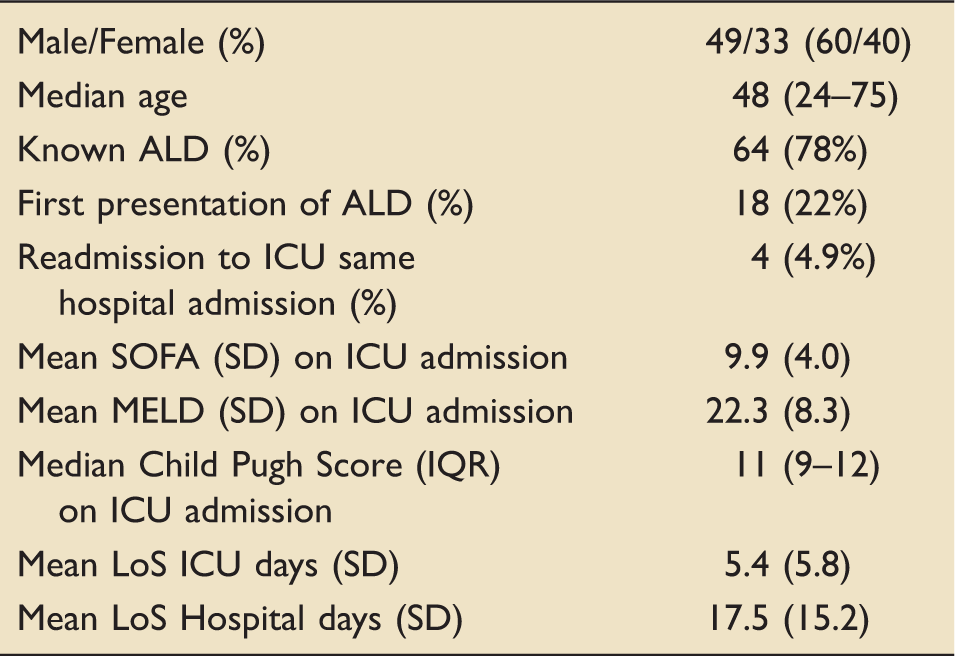
Over a 5-year period, we identified 174 patients with chronic liver disease admitted to general ITU on both sites. After review 78 were excluded as non-ALD patients. Fourteen sets of notes were not accessible. Therefore, 82 patients met the inclusion criteria and were successfully entered into the study. For the 82 with notes available all data were successfully collected in full for each patient.
Characteristics of patients admitted to ICU with ALD (n = 82).
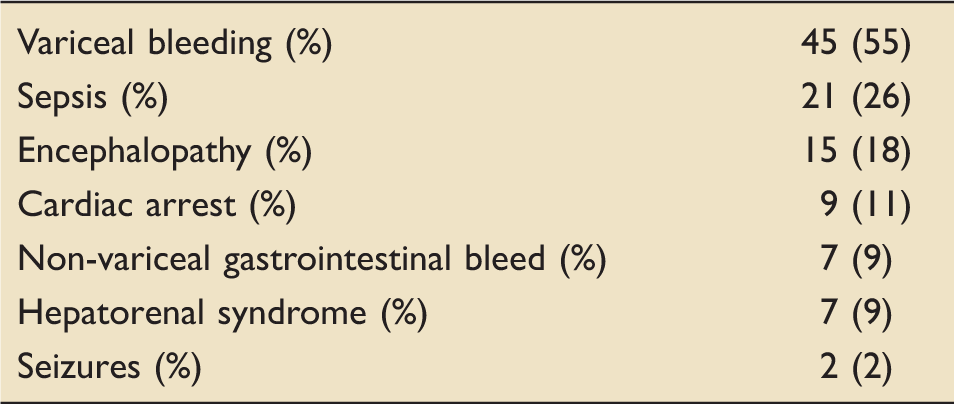
Diagnosis in patients admitted to ICU with ALD (n = 82).
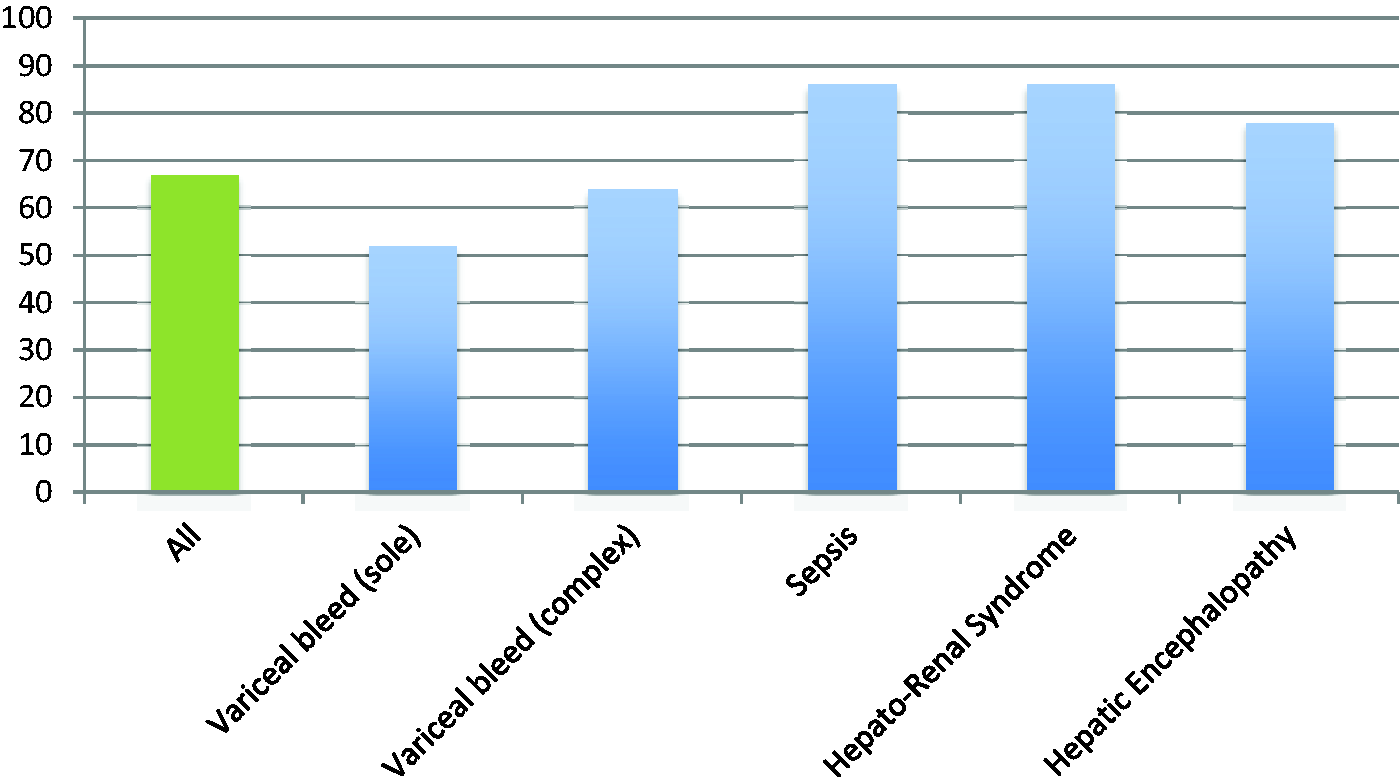
Hospital mortality (%) by ICU admission diagnosis.
Mortality
Mortality in patients admitted to ICU with ALD (n = 82).
Mortality varied by diagnosis (Figure 1), with isolated variceal bleeds having the best outcomes and sepsis and hepatorenal syndrome having the worst. Variceal bleeds complicated by further pathology (e.g. cardiac arrest) still had a better prognosis than other diagnoses.
Interventions on ICU included intubation and ventilation (64 patients, 78% hospital mortality), inotropic support (41 patients, 83% hospital mortality) and renal replacement therapy (10 patients, 80% hospital mortality).
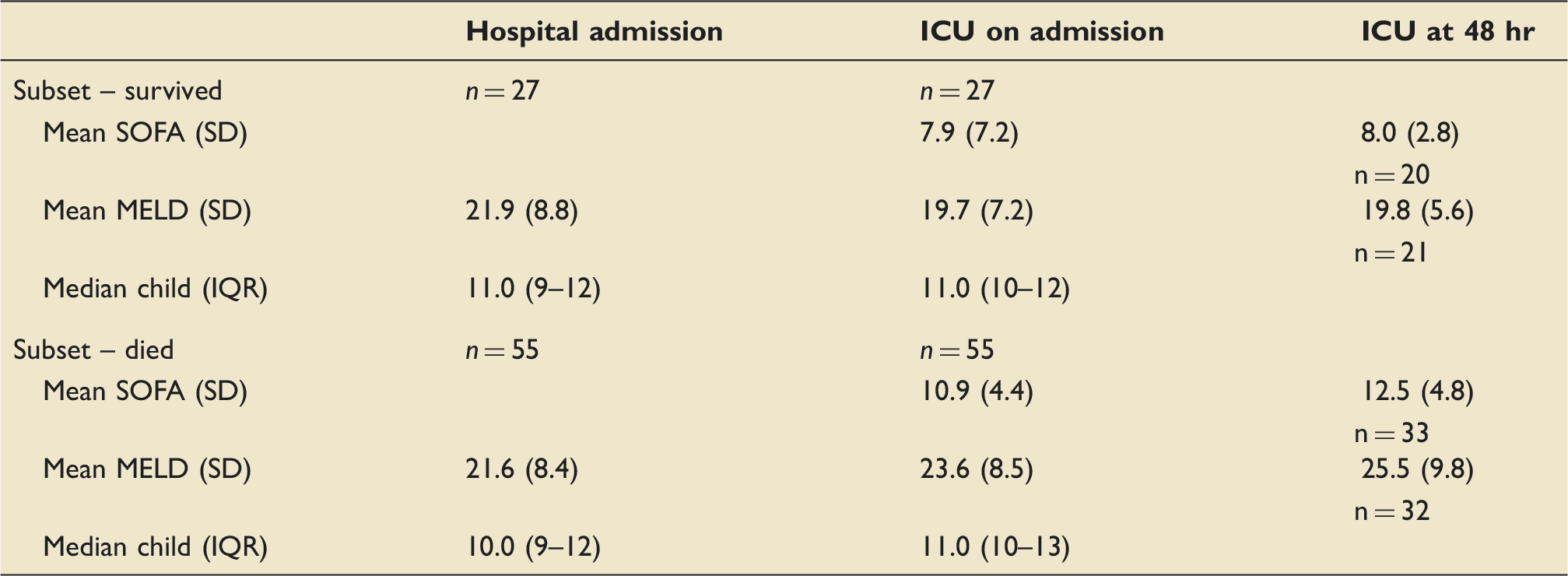
MELD, SOFA and Child Pugh scores at hospital admission, ICU admission, ICU at 48 hr in hospital survivors and non-survivors.
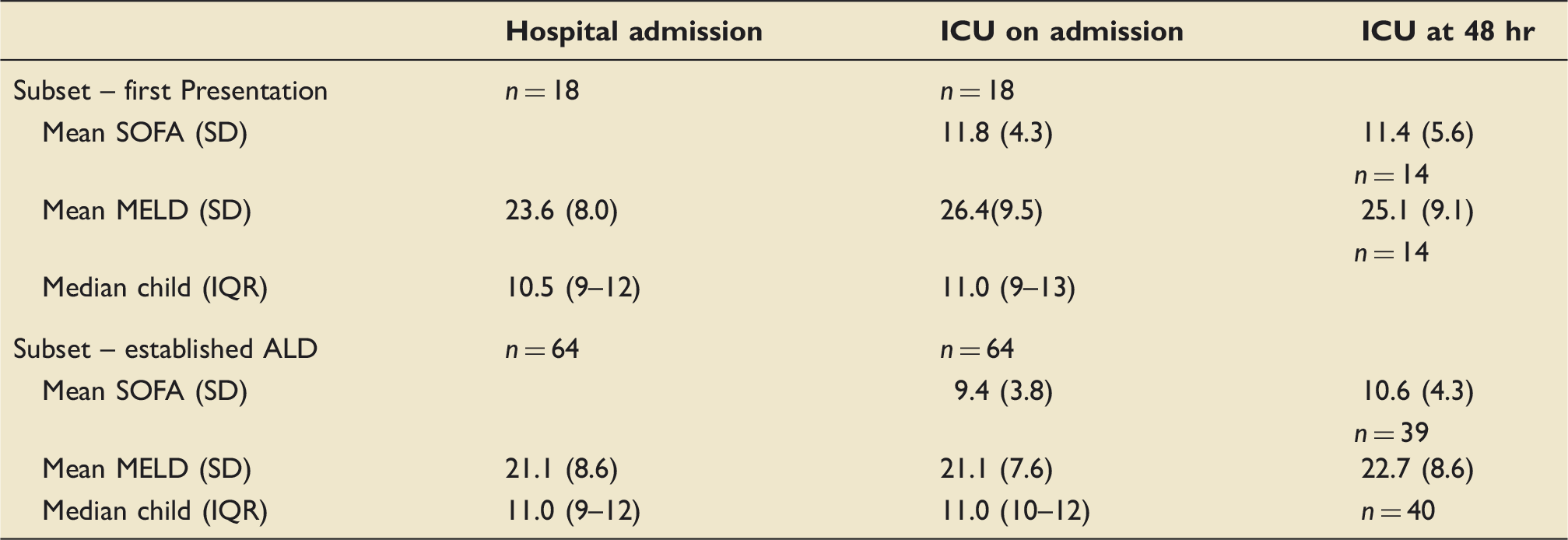
MELD, SOFA and Child Pugh scores at hospital admission, ICU admission, ICU at 48 hr in first presentation patients and established ALD patients.
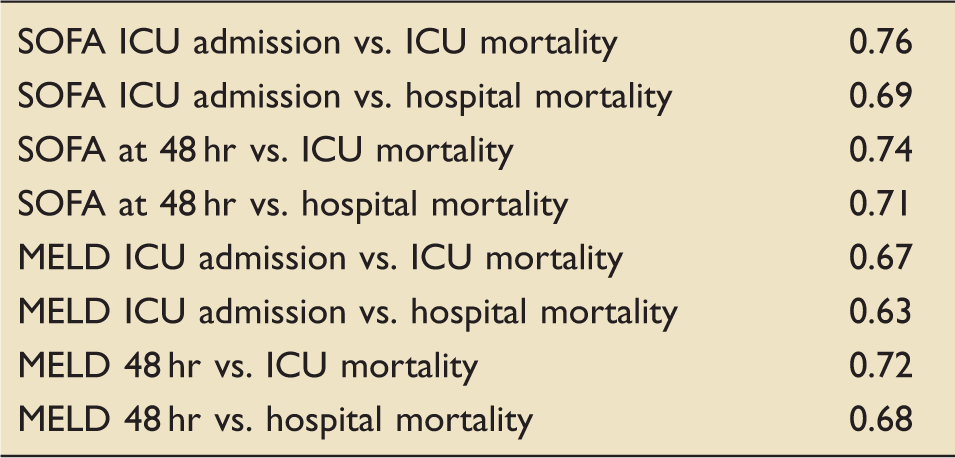
Area under the receiver–operator curve.
A SOFA score of greater than 10 on ICU admission was associated with 97% hospital mortality. SOFA score did not change at 48 hr in survivors but increased from a mean of 10.9–12.5 in those that did not survive hospital. Notably, the subset of 28 patients who survived greater than 48 hr and whose SOFA score was higher at 48 hr than at admission to ICU had a 79% hospital mortality.
Discussion
Decompensated ALD is associated with poor outcomes once a patient is unwell enough to require critical care input. However, we have identified a sub-group of patients whose outcomes are, whilst still poor, substantially better than average for the cohort. We have also added to the evidence base in support of utilizing the SOFA score to aid prognostication and decision making in this patient group. Our results are in the line with the previously published United Kingdom study by Mackle et al. 3 In the decade since their data collection no improvement in outcome is shown.
Patients presenting with a variceal bleed as their sole indication for ICU admission had an ICU mortality of 29% and hospital mortality of 52%. The study average hospital mortality was 68%. In contrast sepsis and renal failure both carried hospital mortality rates of over 80%. Presenting diagnosis matters and this should be part of the consideration of the decision to admit to ICU. A large number of patients with variceal bleeds, even with severe liver disease, can survive to hospital discharge after an ICU stay. It should be noted that deterioration from admission, unsurprisingly, carries a poor prognosis. The 28 patients whose SOFA score was higher at 48 hr than at admission to ICU had a 79% hospital mortality. This figure does not include the 20 patients who deteriorated and died in less than 48 hr, adding these patients leads to a 88% hospital mortality amongst those who worsen from admission. Any degree of inotropic requirement was associated with a greater than 80% hospital mortality. A previous systematic review has identified an escalating mortality with increasing number of organ failures, reaching 90–100% for three organ failure. 5 Reassessment of progress at 48 hr with a further multi-disciplinary discussion should be therefore undertaken.
Of the scoring systems we have studied SOFA correlates most closely with outcome. It has previously been identified as one of the better scores to evaluate critically ill ALD patients, performing better than the Acute Physiology and Chronic Health Evaluation (APACHE) II score and Child-Pugh score.4,6 In this study, SOFA also outperformed the MELD score, which has previously been demonstrated to be the most useful of the liver specific scores for this patient group. 4 A SOFA score of greater than 10 at admission to ICU was, in this study, associated with a 97% hospital mortality. This cut off for a very poor prognosis has been previously noted. 7 We would suggest a SOFA score is calculated to aid prognostication and discussion with the patient, family and parent teams. It should be noted that scoring systems do not replace clinical acumen and should only be part of an overall clinical assessment. It has been previously suggested that SOFA is more accurate when used to predict mortality at 48 hr from ICU admission. 7 However, whilst we recommend reassessment of progress at 48 hr, our study did not show an improved correlation with hospital mortality between SOFA scores at admission and 48 hr.
It is sometimes suggested that patients presenting with ALD for the first time have an improved outcome, with first presentation frequently being cited as a reason for ICU admission in otherwise dire circumstances. In order to investigate this, we recorded whether a patient was presenting for the first time with ALD or had an established diagnosis of ALD. Whilst there could be a perceived moral argument differentiating between a recidivist and a patient who has not had the shock of a hospital admission to promote abstinence our data do not support this view on clinical grounds. Our study has shown an increased mortality in patients presenting to ICU during their first ALD related hospital admission, albeit not reaching statistical significance, with an outcome as poor as the sepsis group. The first presentation group had significantly worse MELD and SOFA scores on admission to ICU when compared with those with known ALD. The difference in MELD score was not present on admission to hospital.
These data suggest that the severity of presentation predicts outcome more accurately than the number of previous presentations. This is understandable as ALD follows years of chronic liver damage therefore even the first presentation is likely to have significant underlying disease. 8 Furthermore, it may be that patients presenting critically unwell during their first admission with ALD have avoided healthcare previously and correspondingly have more severe chronic disease leading to a more rapid deterioration in hospital. Further study of larger numbers of patients is needed to reach firm conclusions regarding this subset of patients.
Outcomes amongst patients admitted, treated and then discharged from ICU with the intention of recovery are still poor. Of 33 patients discharged from ICU with the intent of recovery over 20% died subsequently during the hospital admission. As such we consider hospital mortality to be of greater importance than ICU mortality when making decisions on ICU management.
We recognize the limitations of a retrospective study. We have not controlled or analysed the decision making process for the management of patients included. The intention was to provide a pragmatic review of outcomes of typical ALD management in this country. There may have been some eligible patients missed and we were unable to locate the records for 14 patients which could bias the results. Furthermore, we have no control group in the form of ALD patients not admitted to a critical care area. It is possible that outcomes of patients who either died before ICU or were not admitted to ICU could be different to those that we have included. In particular, due to potentially very rapid blood loss some patients with massive GI bleeds may die on the ward or during endoscopy, which may skew the ICU survival figures for this patient group.
Whilst the numbers of patients are smaller than some large database based studies we have undertaken a detailed review of every patient included, rather than relying on coding and summary data. The accuracy of identification of ALD patients and the data is therefore a strength of this study. As this is a detailed retrospective study, the data are from some years ago. Whilst this could be considered to have a negative impact on the relevance of our results, substantial changes in the management of ALD have not occurred in this time frame and we are of the opinion that the results remain valid and informative. However, our results are similar to the article published by McPhail et al., 9 the main difference being that our data is based on general ALD presentations to ICU with the exclusion of specialist transplant cases.
These data are not strong enough to provide clear guidance on who should be admitted or declined ICU care. It does however provide information to aid clinical decision making and communication between specialty teams and with patients and their families. This is particularly valuable in this patient group, with the possibility of recurrent presentation to ICU and poor overall outcomes.
In summary, decompensated ALD is not a contraindication to ICU admission, even with severe underlying disease, though prognosis remains poor. Decision making and communication is best made on the basis of thorough clinical assessment, presenting diagnosis and SOFA score. Isolated variceal bleeds in particular have a reasonable survival rate. In patients where suitability for escalation is unclear admission with review at 36–48 hr may be appropriate and worsening clinical condition should prompt reconsideration of active critical care management.
Footnotes
Acknowledgements
With thanks to Caroline Booton for statistical assistance. The methodology of the study was discussed with a member of the local Research and Ethics Committee and no formal Ethics committee approval was deemed necessary.
Author contributions
JB was involved in data collection, analysis and write up of first draft. AS was involved in study design, data collection and draft revision. SE was involved in study design, analysis and draft revision. PJ was involved in study design, data collection, analysis and draft revision.
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: All authors have completed the ICMJE uniform disclosure form at ![]() and declare: no support from any organization for the submitted work; no financial relationships with any organizations that might have an interest in the submitted work in the previous 3 years; no other relationships or activities that could appear to have influenced the submitted work.
and declare: no support from any organization for the submitted work; no financial relationships with any organizations that might have an interest in the submitted work in the previous 3 years; no other relationships or activities that could appear to have influenced the submitted work.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.