
Abstract
Background
Familiarity with environment, processes and equipment reduces the risk inherently associated with critical care transfers. Therefore, the North West London Critical Care Network decided to create a standardised ideal transfer bag and contents to improve patient safety.
Methods
A four-round modified Delphi survey developed a condensed and clinically tested content list. An expert panel then designed an ideal transfer bag based on agreed important principles.
Results
Participants completed two rounds of an electronic survey. Round 3 comprised an expert clinical panel review, while round 4 tested the contents over 50 clinical transfers. The prototype bag’s design was adjusted after clinical use and feedback.
Discussion
This project has introduced a standardised critical care transfer bag across our network. A similar technique could be used for other healthcare regions. Alternatively, the above critical care transfer bag could be adopted or adapted for regional use by clinicians.
Background
Critical Care transfers are common and inherently associated with risk. Unfamiliarity with environment, processes and equipment contribute to this risk.1–3 Frequent rotation of medical staff undertaking transfers and a lack of standardised equipment, particularly the transfer bag, are exacerbating factors. The North West London Critical Care Network (NWLCCN) has shown that patient safety during critical care transfers can be improved by standardising regional transfer training and education material. 4 These methods increase clinicians’ familiarity with transfer processes and equipment.
A vital piece of transfer equipment is the transfer bag, which contains life-sustaining and supporting equipment. Despite showing that standardisation reduces risk, there continues to be a considerable variation in the contents and designs of transfer bags even within regions and their constituent hospitals. It is not uncommon to find large wheel-based suitcases that create a struggle to manoeuvre into lifts and along corridors. Therefore, NWLCCN embarked upon a project to create the ideal transfer bag design and content list. This article describes the development of this bag and its introduction into the clinical environment.
Methods
Stage 1: Creating the bag contents list
Initial all inclusive list of transfer contents.
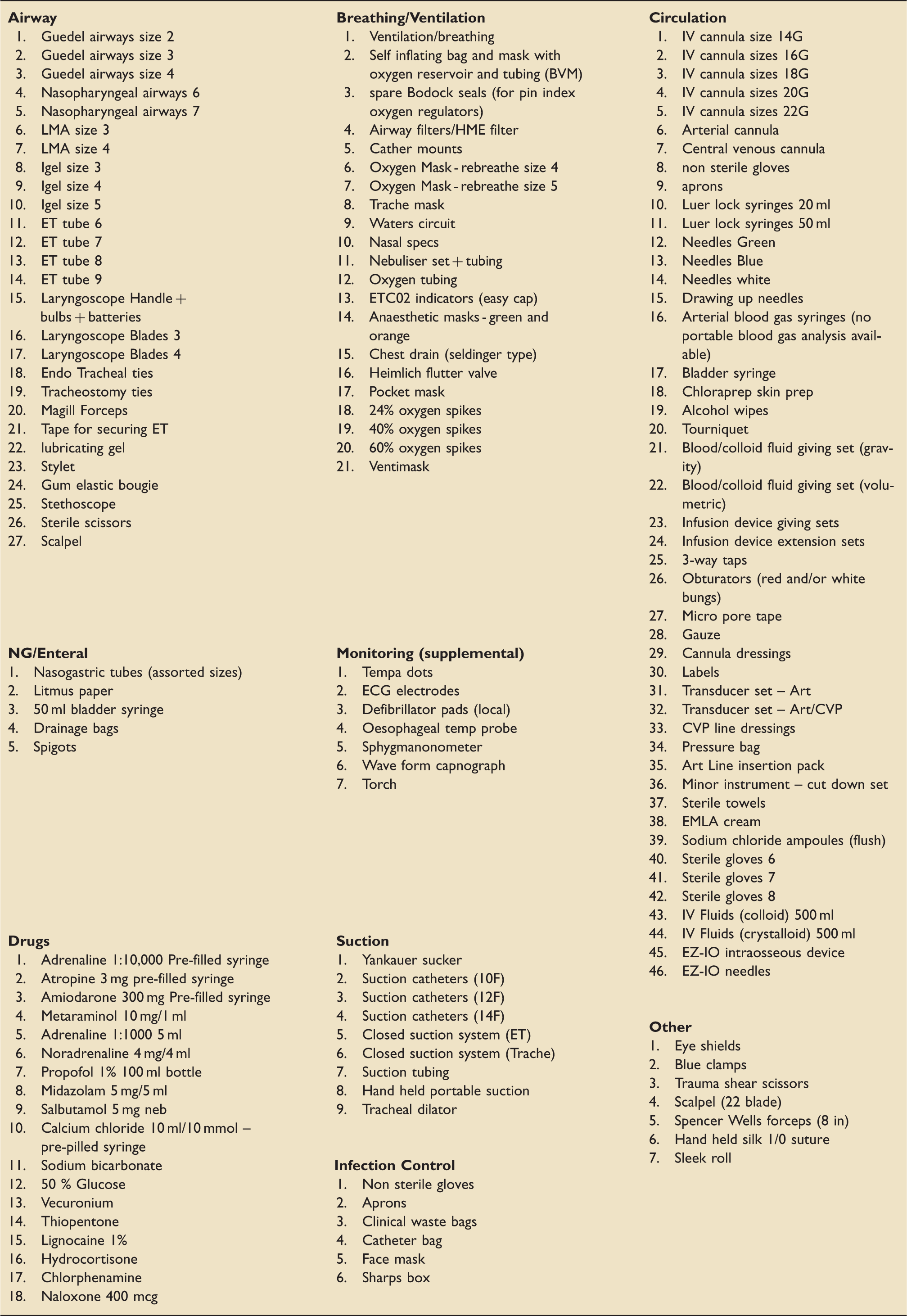
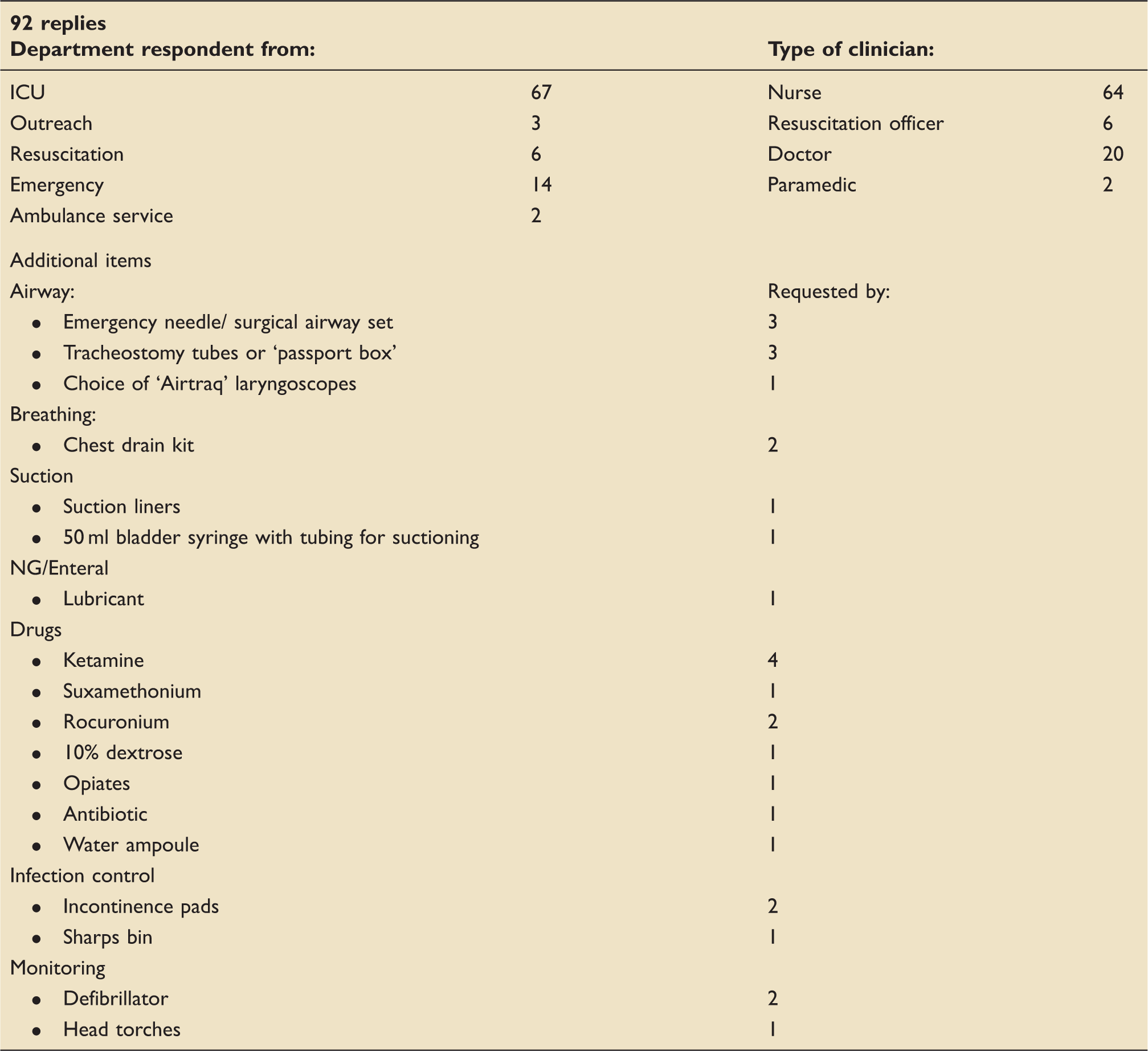
Round 1 was an electronically mailed spreadsheet of all 146 items separated into categories (Airway, Breathing, Suction, Circulation, Enteral, Drugs, Infection Control, Monitoring and Other). This was sent to clinicians within North West London comprising nurses, physicians and paramedics working within different departments (Critical Care, Emergency, Anaesthetics and Ambulance service) with a range of seniority. They were asked to rate items using a 5-point Likert scale (‘Very unimportant,’ ‘Quite unimportant,’ ‘Neither,’ ‘Quite important,’ ‘Very important’) and decide how many of each item would be needed within the final bag. An additional question asked if the clinician had used the item during any previous transfers to prompt consideration of its need in the final ideal bag. A pilot study consisting of 10 individuals was undertaken to determine if completion of the extensive questionnaire was achievable in a reasonable length of time and if adjustments were needed.
Round 2 was an electronically mailed questionnaire comprising photographs of the items (Figure 1), which were deemed ‘Very important’ or ‘Quite important’ by at least 80% of respondents from round one. This was simple and quick (less than 5 min) to complete and questioned whether the respondent agreed with the items or if additional items were needed and if so, what the rationale was.
Electronically mailed questionnaire to decide on selected transfer bag contents.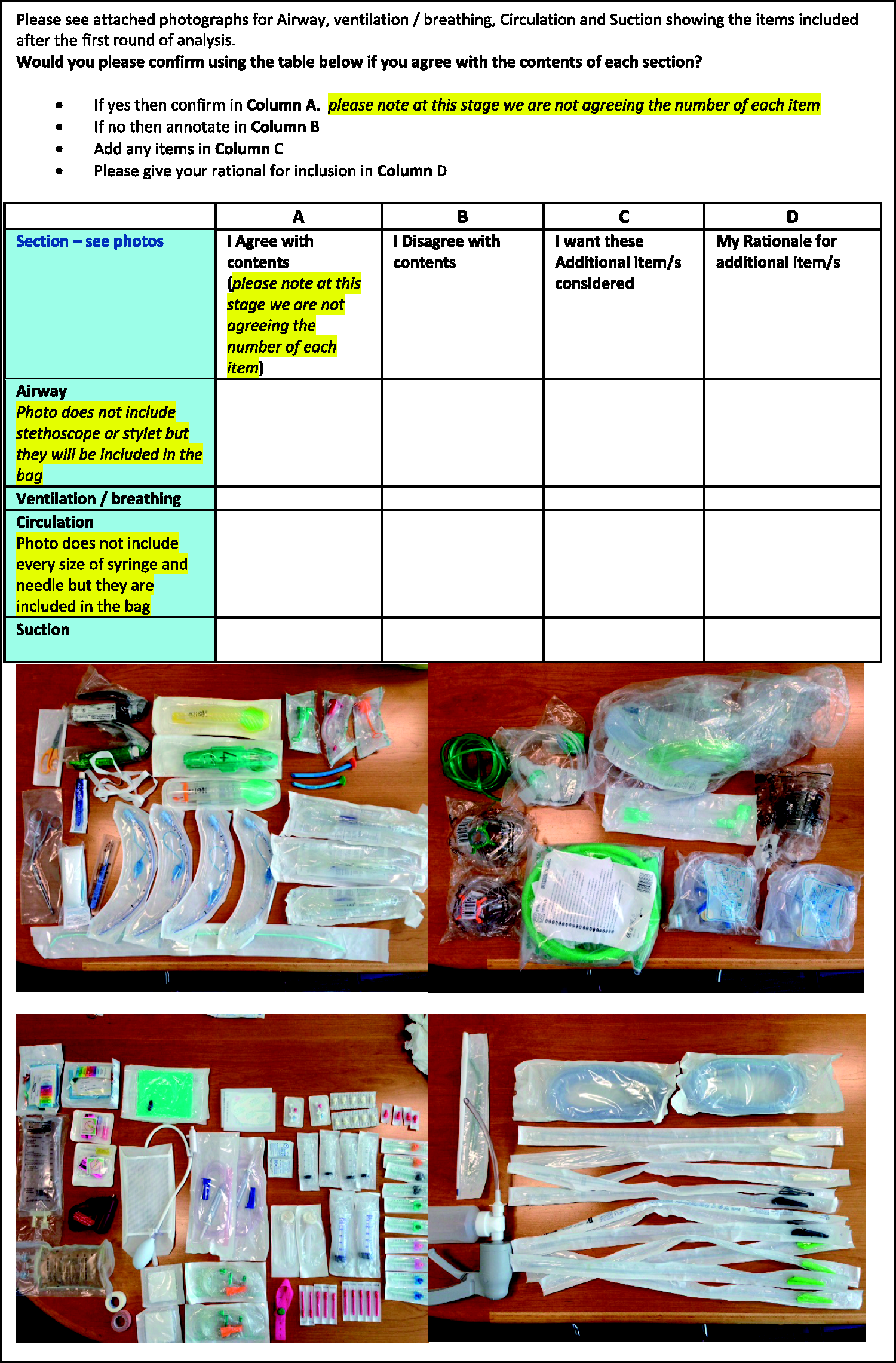
Round 3 consisted of an expert panel of 22 clinicians from the NWLCCN Transfer faculty who met face-to-face to discuss the content list and review the numbers of each item required.
Round 4 involved the clinical use of a transfer bag packed with the agreed items during 50 intra-hospital transfers in three North West London hospitals. A further 105 clinicians reviewed the contents over three NWLCCN transfer training courses. Feedback was obtained during both processes.
Stage 2: Creating the bag design
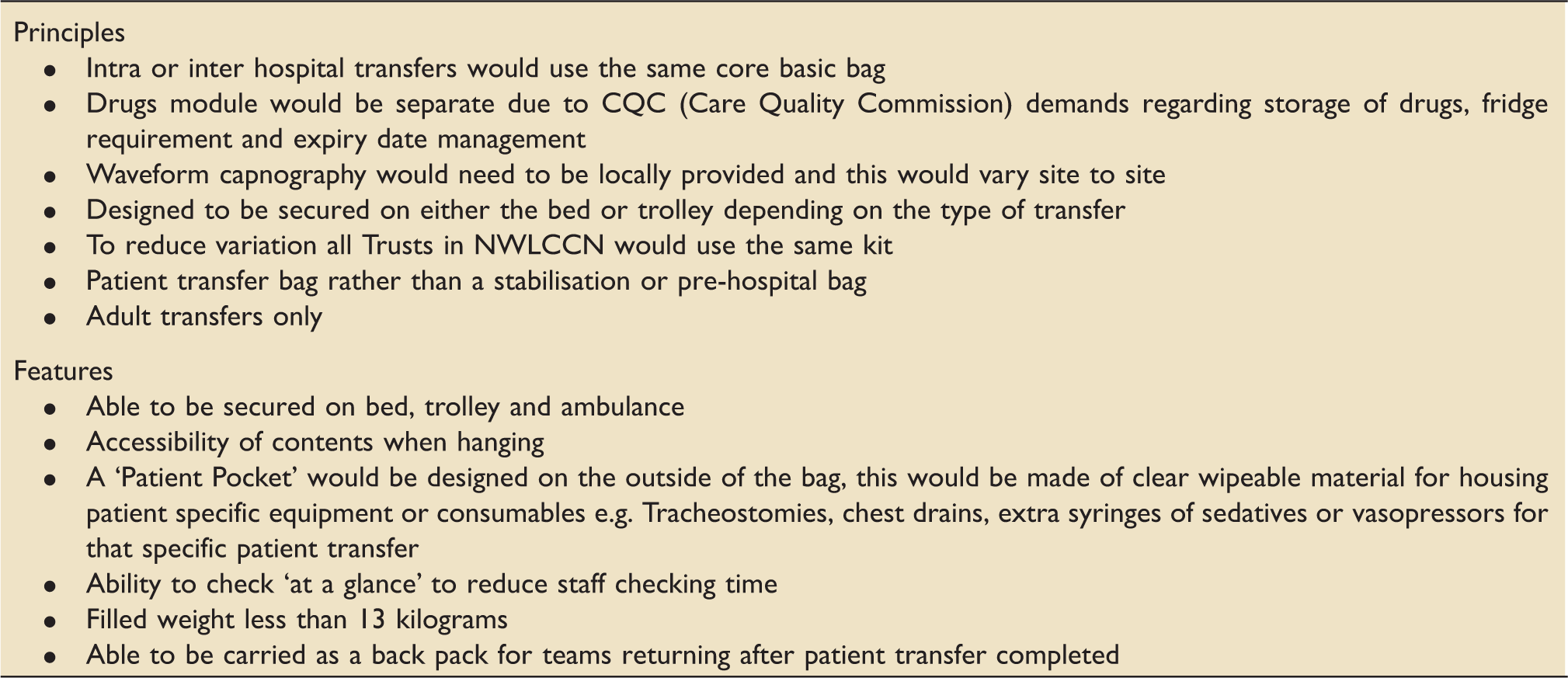
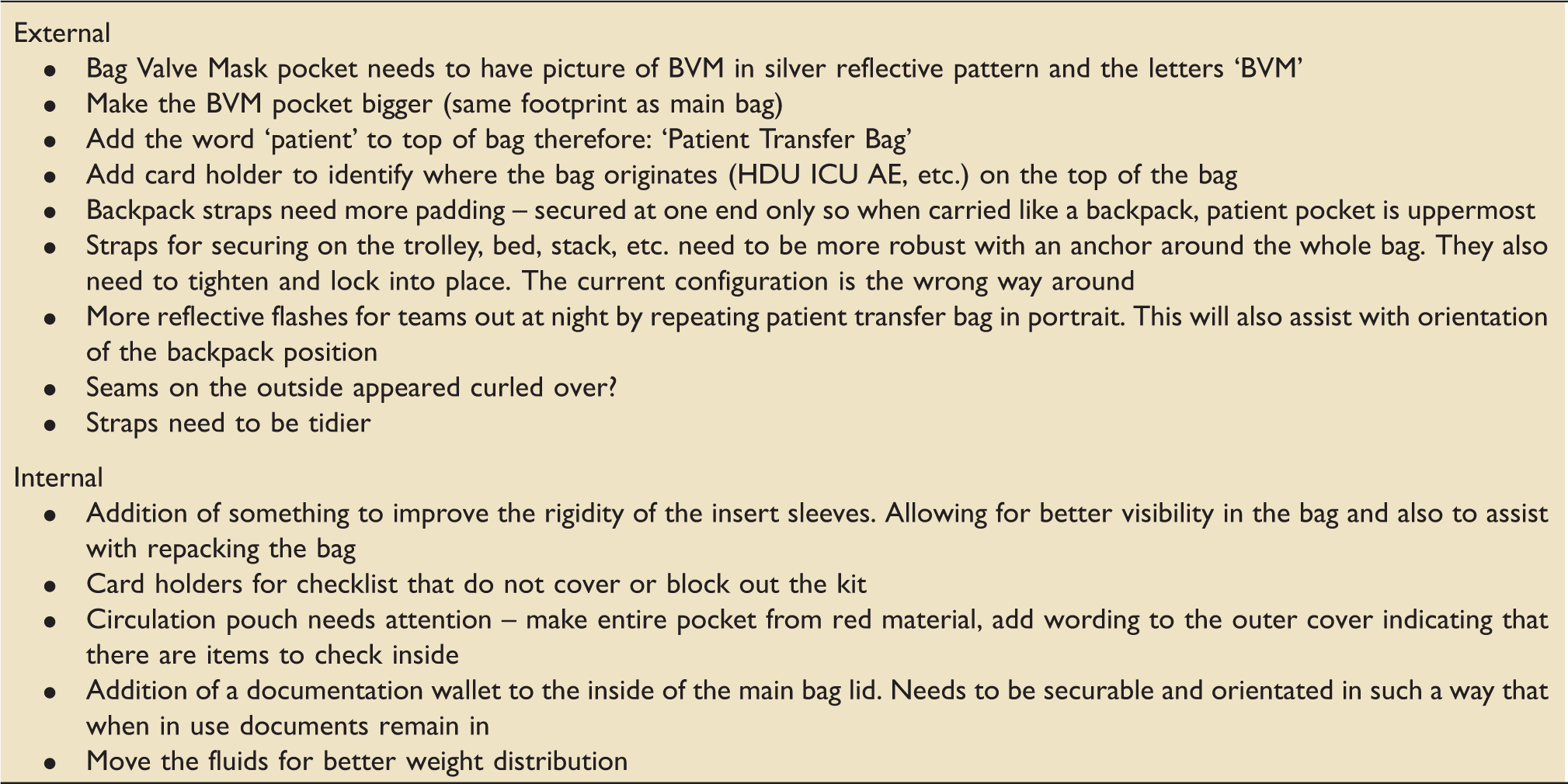
The process of designing the ideal critical care transfer bag was initiated by reviewing five transfer bags in current use across London. The same expert panel of 22 NWLCCN clinicians met to discuss the advantages and disadvantages of each. The key principles and features to be included were outlined and agreed, including the addition of a ‘Patient Pocket’ which allowed clinicians the flexibility to add bespoke items for that specific patient transfer.
Having discussed the project with several bag designers, one design company, Openhouse™, was approached with the agreed principles and features required for the ideal transfer bag. A schematic diagram was drawn up for review and discussion. The filled control transfer bag provided information about the weight and dimensions of the equipment items.
Feedback about the bag design was collected from the Annual NWLCCN Education Event where the packed prototype bag was presented to the audience with an explanation of the process leading up to it. 6 Clinicians were given an opportunity during the day to handle the bag and manoeuvre it on and off an ambulance. Afterwards, the prototype bag was taken to all the 19 hospitals in the NWLCCN and to the Emergency, Critical care, High Dependency, Outreach and Anaesthetic departments for further comments and feedback.
Once the bag design had been adjusted from the collated feedback, a further quality assessment was made in the form of ‘time to check’ tests. During several transfer training courses, candidates were timed against each other, one checking an original transfer bag and the other checking the new NWLCCN prototype, to determine which was fastest and easiest.
Results
Results –Stage 1
The pilot study revealed that the spreadsheet lines were quite hard to follow due to the extensive number of items. Alternate line shading was used to make the form easier to read. Completion took 30 min, which was considered acceptable.
Round 1: summary of responses.
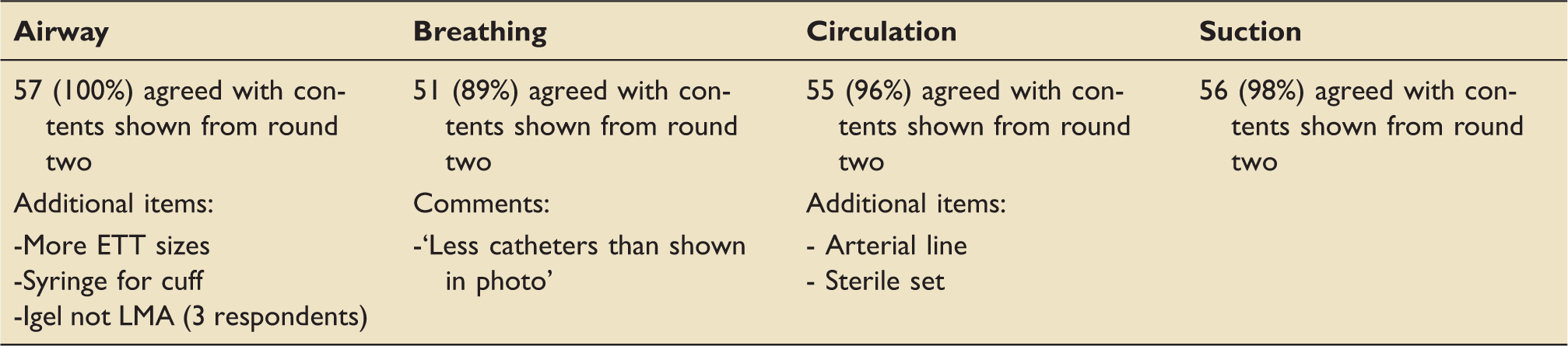
Round 2: summary of responses.
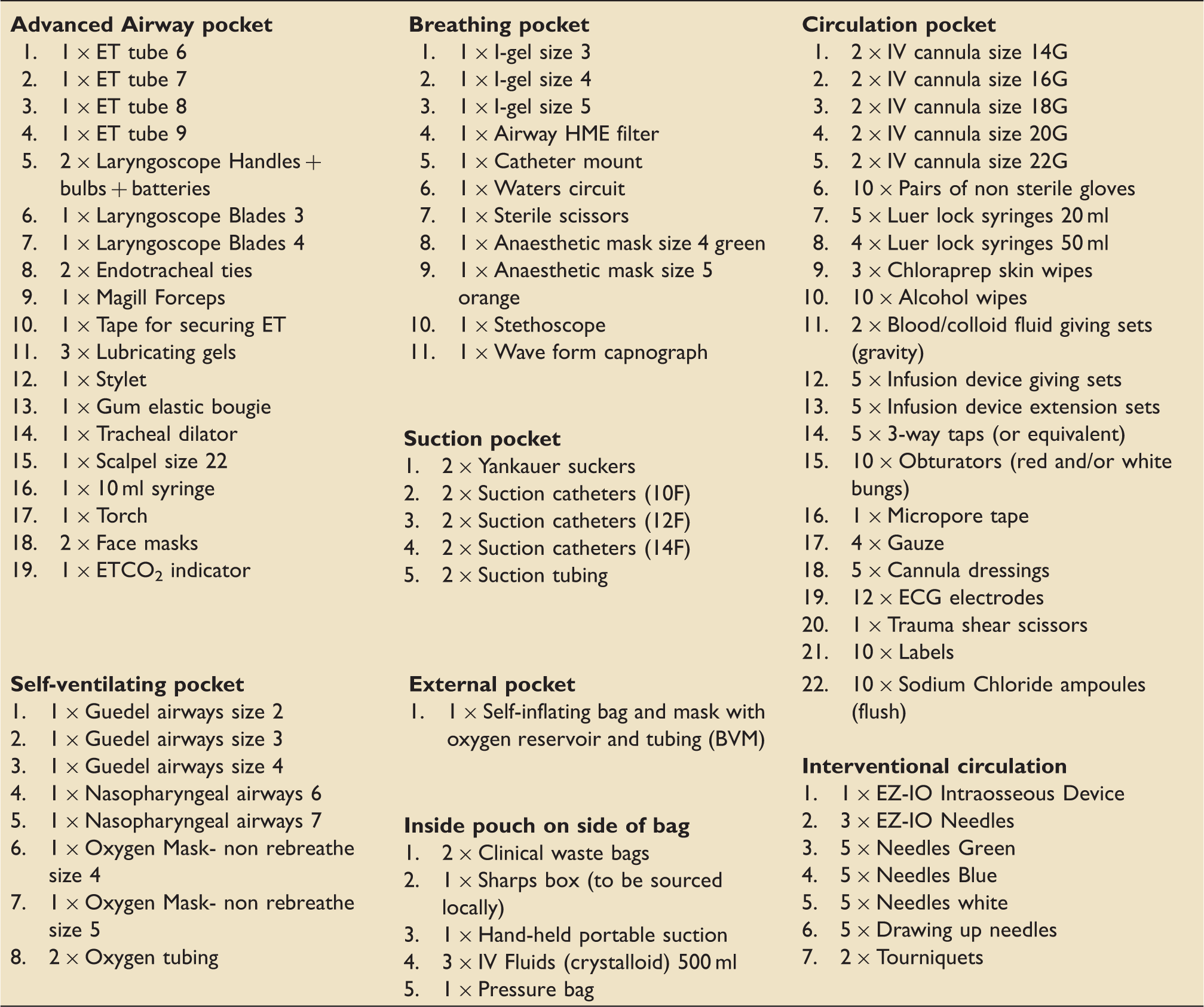
The finalised contents list.
Round 4 (clinical transfers) tested the contents during 50 transfers across three North West London Hospitals. Feedback received was very positive, particularly in regard to the reduced weight with the condensed kit. Over a 10-week period, very little kit was actually used which demonstrated the feasibility of equipment reduction. The outreach team’s broader use for the bag (patient stabilisation), which was not part of the bag’s remit, meant that the lack of arterial lines and transducer set was highlighted –a ‘grab bag’ is in development for these teams. Specialised services, for example, Extra-corporeal Membrane Oxygenation (ECMO) acknowledged that they would need to add to the standardised transfer bag.
Results – Stage 2
The initial schematic diagram of the bag is shown in Figure 2. This was the result of the key features and principles (Table 5) that were decided on by the panel of NWLCCN clinicians in June 2014. Several further adaptations were made after the prototype bag. Initial adjustments were made after comments (Table 6) were received from the majority of the 89 attendees at the annual NWLCCN event in December 2015. Further modifications were needed after the bags were tried and tested on various trolleys and beds within different hospitals across North West London and on London Ambulances (Figures 3 to 7).
Initial schematic diagram of the transfer bag. ® This design is copywritten. Key principles and features as outlined by NWLCCN transfer and retrieval faculty. Modifications following NWLCCN annual event and feedback from pilot sites. The critical care transfer bag showing the insert sleeves and clear patient pocket. The ‘open book' design and clear panels enabling quick retrieval and checking of equipment. The transfer bag securely attached to a hospital bed. The bag attached to an Emergency or Theatre patient trolley with easily accessible insert sleeves. The transfer bag attached to an ambulance patient trolley.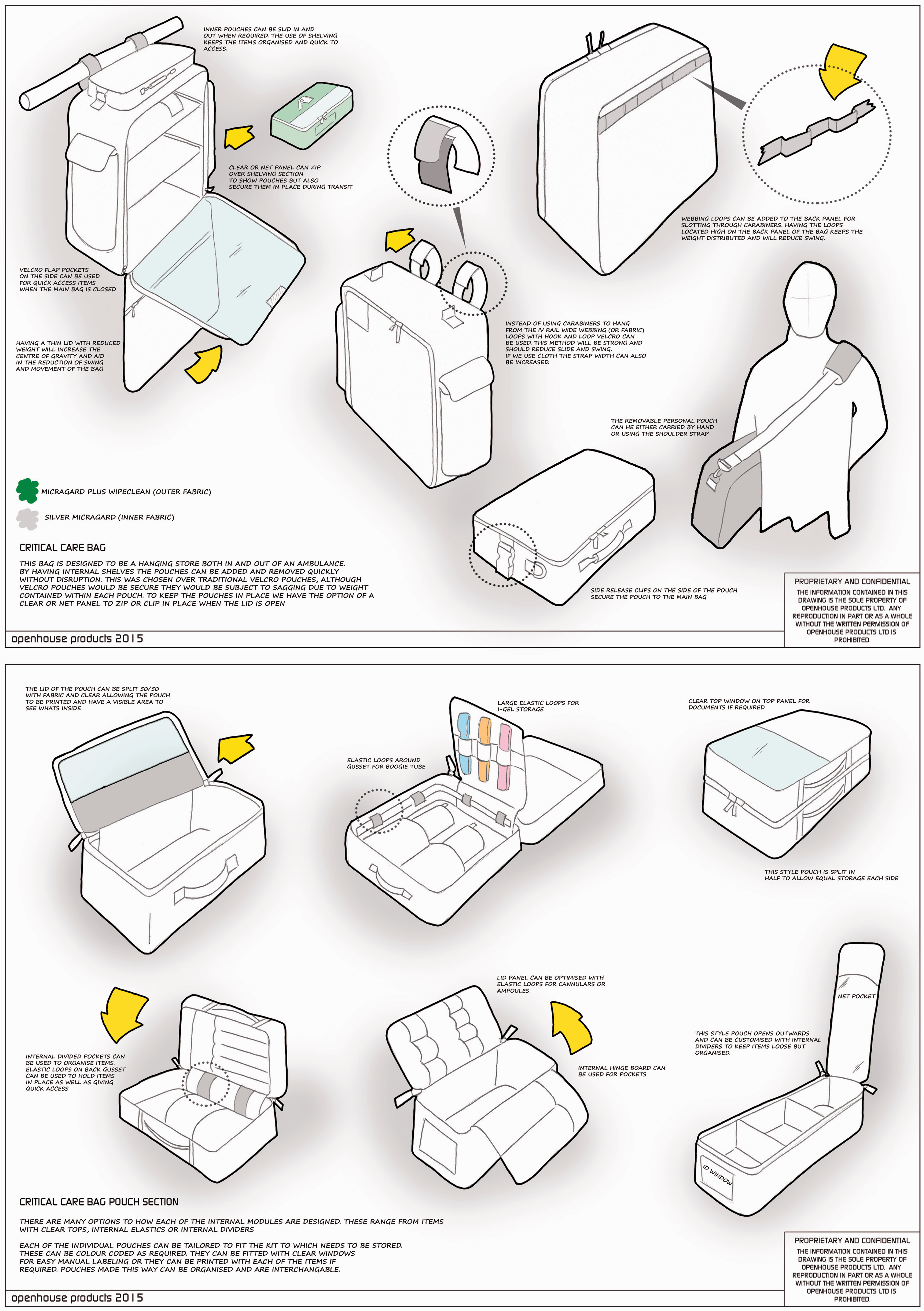

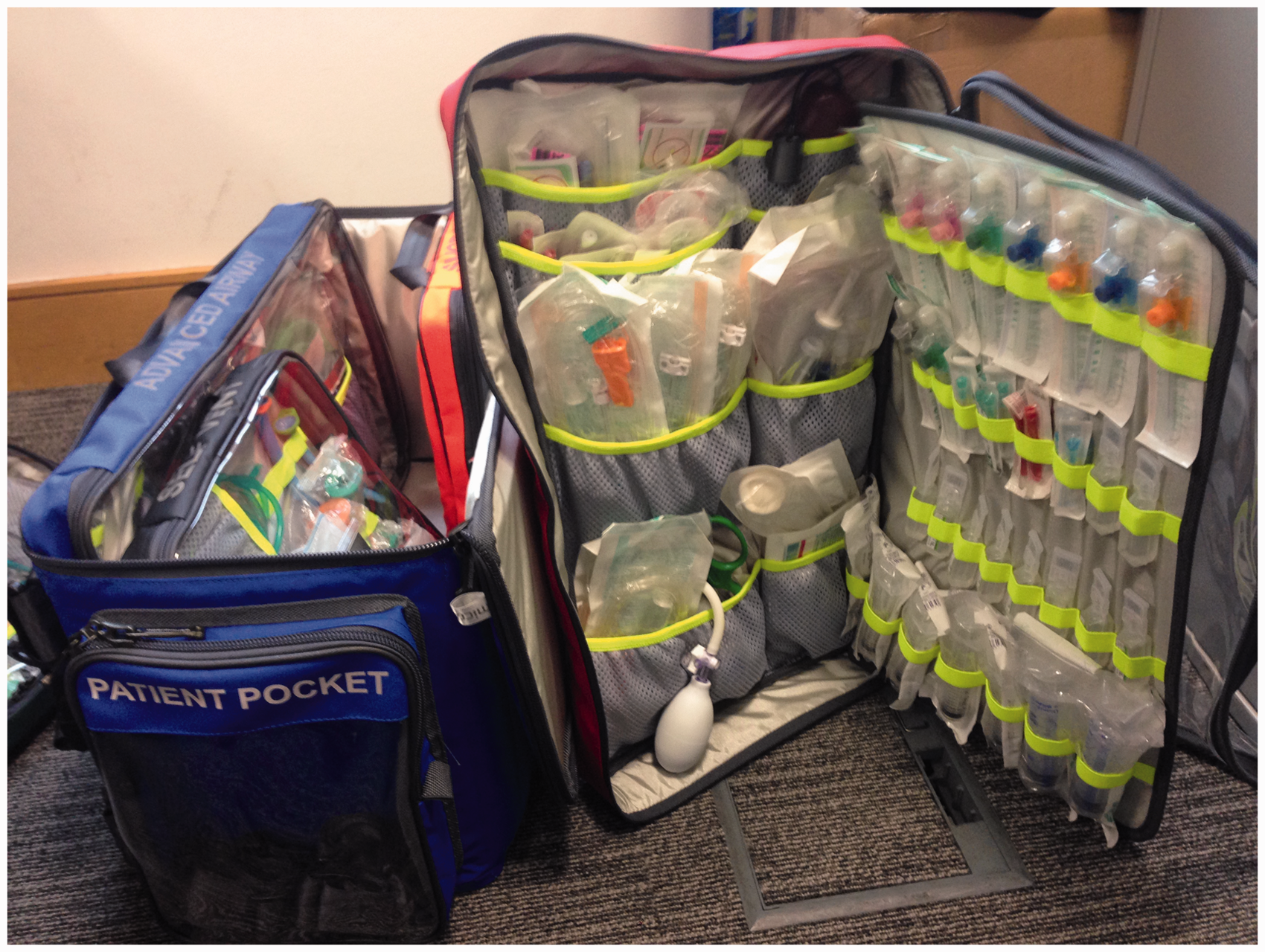



The ability to check the bag ‘at a glance’ due to the clear panels or ‘open book’ design of the pockets drastically reduced the time to check compared to the conventional critical transfer bags in use currently. The results from the trials timing staff checking the contents of transfer bags revealed an average time of less than 5 min for the NWLCCN prototype versus a minimum of 20 min for the current bags in use.
Discussion
The original aim of this project was to create a standardised ‘ideal’ critical care transfer bag with a condensed list of contents to reduce the problem of unfamiliarity with equipment that has been shown to increase the risk associated with critical care transfers. The modified Delphi method used has enabled a large group and a wide variety of clinicians to be involved in this process. The NWLCCN Transfer Bag and its contents have been ‘road tested’ in the clinical environment in multiple settings by large numbers of personnel to enable further modifications to make sure it is as ideal as possible. The NWLCCN Network is now applying the same methodology to paediatric and ECMO transfer bags.
This critical care transfer bag provides a standardised solution for our critical care network. A similar technique could be used to design a transfer bag for other regions. Alternatively, readers are welcome to adapt or adopt the above critical care transfer bag.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.