
Abstract
In May 2014, North Bristol NHS Trust merged its two existing hospitals – Southmead and Frenchay – into a new, purpose-built building. The project involved the movement of 540 patients, many over a distance of several miles. We describe the planning process and transfer of 24 level two and three patients from two intensive care units into the new hospital. These transfers were performed successfully, without significant incident and under intense scrutiny from the Trust, the patients and the media. In this paper, we reflect upon our experiences of this process, which may be of benefit to those encountering a similar move in the future.
Introduction
In May 2014, North Bristol NHS Trust merged its two existing hospitals – Southmead and Frenchay – into a new, purpose-built building on the Southmead site. The project encompassed moving 540 patients, 1 many over a distance of several miles, in addition to the associated supporting services. It was one of the largest single patient transfer operations ever conducted in the United Kingdom.
As part of this relocation, critical care services were amalgamated into a new 48-bedded intensive care unit (ICU), which involved the critical care transfer of 24 level two and three patients over three days. This article describes the planning and preparation that was undertaken to achieve this move safely, and also our reflections, which we hope may be useful to others in the future.
Preparation for the move
North Bristol NHS Trust announced in 2004 that it was going to redevelop the existing Southmead and Frenchay Hospital sites, much of which dated back to the 1940s. The private finance initiative (PFI) project involved the building of a new acute hospital at the Southmead site, where the majority of acute clinical and support services would be housed under one roof.
The construction project commenced in February 2010 and the building was handed over to the Trust on 26 March 2014. The first patients were transferred from the old Southmead Hospital buildings during the week of 12 May 2014, followed by Frenchay Hospital patients the following week.
Critical care services in North Bristol NHS Trust prior to the move consisted of a 19-bedded ICU at the Frenchay site along with a neurosurgical high-dependency unit of 12 beds and a 9-bedded ICU at the Southmead site.
The involvement of the department leads and their colleagues began early in the design process for the new building. Initial preparation for the move of critical care patients into the new 48-bedded unit began in the summer of 2013. Discussions involved the dedicated Trust relocation team (MOVE Team) and Trust Executives amongst many others.
The Trust set a window of dates in which all patients from both hospitals were planned to be relocated. These dates were chosen to fit with the PFI contract and the handover date from the contractor, Carillion. Transfer of patients was planned to occur in daylight hours only (08:30−18:00) to ensure safety and maximal availability of staff, including support services such as medical engineering and domestic staff.
The smaller Southmead ICU was planned to move a few days prior to the larger Frenchay ICU. This was done to allow a graduated step-up in the use of the new unit, to facilitate staff familiarity and to ensure that there was sufficient time to address any unpredicted challenges before embarking on a several mile road transfer for a large number of patients. All staff had attended familiarisation sessions for the new ICU prior to the move commencing. As a regional major trauma centre, the Frenchay ICU move had to co-ordinate with the Emergency Department to ensure the continuity of services.
The Emergency Department move was planned for 2 a.m. on a Monday morning and so the aim was to complete the ICU transfer by the Sunday evening immediately prior to this. There were a number of perceived advantages of choosing a weekend to transfer patients. These included quieter roads to minimise the transfer time, patient routing through the new (unopened) Emergency Department to aid easy access to the new building, and reduced surgical workload with no elective admissions.
Early in the planning process, discussions about medical and nursing staffing for the transfer week occurred. Trust-wide restrictions on leave were instigated to facilitate the additional numbers of staff required for the short duration of the move. It was necessary to staff both old and new units as well as provide the additional dedicated staff for the transfer team. As patient numbers changed, a gradual staff move from old to new units was planned. A small number of staff were planned to remain at Frenchay for the days following the move to ensure safety for patients arriving at the now-closed Emergency Department and those in the rest of the hospital waiting to move. The nursing staff were asked how they felt it best to provide care across both sites and agreed as a group that the most appropriate solution was to provide a dedicated group of four ‘transfer nurses’ for each day. These were experienced nurses with previous transfer training and experience who volunteered to be members of the team. Medical escorts for the transfers were provided by two registrars, dual-training in both anaesthesia and intensive care medicine (authors Christopher JR Gough and Scott Grier), both of whom volunteered for this role and have extensive previous transfer experience and training. In the unlikely event of an incident involving transfer team staff, resilience was provided by nursing and medical staff allocated to both old and new ICUs. All staff who volunteered had each conducted multiple transfers previously and did not suffer from motion sickness. Consultant supervision for all transfers was provided by the Clinical Director of intensive care (author Gareth J Wrathall).
A significant proportion of the planning involved choosing the best methods of physically transferring the patients and ensuring that equipment such as ventilators and haemofilters moved accordingly. Patients on the old Southmead ICU were planned to be moved on their beds. Patients from Frenchay required road transportation. Initial discussions involved local NHS and private ambulance services, but a Royal Air Force Tactical Medical Wing ‘Jumbulance’ 2 – essentially a large truck-based ambulance allowing two patients to be carried at once with supporting staff – was sourced. The main benefit of transferring two patients at a time in the ‘Jumbulance’ was to minimise the total transfer duration.
Prior to the move, all medical equipment was serviced and additional spares made available, including ventilators, gas supplies, pumps, batteries and a defibrillator for transportation. Equipment rotation was planned during each transfer day to ensure battery charge was maintained. ICU equipment such as haemofilters and ventilators were expected to require movement during each transfer day as patient numbers changed. A ‘hot van’ to move this equipment was planned for this.
The final element of the planning process involved the communication with, and education of, patients and their relatives. The reasons for the move, along with the risks and benefits were explained to them and written information was produced to facilitate this. As the move was necessary due to the closure of the old hospital site, details of the planning process and steps taken to the minimise risks were explained to all.
Southmead move
On Wednesday 14 May 2014, the old Southmead ICU patients were moved. This included the transfer of six level two and three general medical and renal patients.
During the previous evening’s consultant ward round, the first two patients to move were provisionally identified so that preparation could be completed overnight and they were ready to move by 08:30. These were chosen as stable patients with an anticipated low risk of potential complications.
Early in the morning of the move, there was a team briefing, which included all medical staff due to be involved in the care of patients on both units during the day. At this, roles were assigned, telephone numbers and emergency contact details shared, and it was made clear that the lead consultant’s approval was required immediately prior to each individual patient move. A brief summary of each patient was provided to facilitate the continuity of care following arrival on the new unit.
Consultant roles had been established prior to the day – one to manage the old unit, one to manage the new unit and one to maintain the oversight and manage the referrals from both old and new sites. Nursing allocation included a team on the old unit providing ongoing nursing care, a team preparing the new unit to receive patients, a transfer team, a senior nurse to maintain oversight and one to manage the transfer of equipment between units.
Equipment and drugs were checked and prepared to ensure that both units and the transfer team had access to everything required to maintain patient safety.
The consultant reviewed each patient and all procedures, such as blood transfusions, radiology and line insertion, were completed prior to moving. They also decided upon the order of patients to move. In accordance with the planned protocol, those anticipated to be most complex or unstable were assigned to the middle of the day. This was felt to be safest, as the move team would then be familiar with the processes and route but not be fatigued.
Once adequately prepared and ready to move, each patient was accompanied by a nurse, a transfer doctor and two porters. As this move was an internal site transfer, each patient remained on their hospital bed. The route from old unit to new involved two lift journeys, two long internal corridors and an external route (covered by temporary structures) totalling 650 m
On arrival at the new unit, the patient’s monitoring was transferred to the new system and a verbal handover of care given. The transfer was documented in the patient notes.
In total, four level two and two level three patients were safely transferred, with the only incident being a patient who had paroxysmal atrial fibrillation (AF) developing fast AF on arrival at the new unit that required rate control.
One level three patient was not transferred due to instability and possible requirement for Interventional Radiology services, which had not yet moved to the new building. In order to maintain patient safety, she was managed in theatre recovery with intensive care nursing. The following day, she was transferred without incident.
Frenchay move
On Saturday 17 and Sunday 18 May 2014, the Frenchay intensive care patients were moved. This included the transfer of 18 level two and three patients, of which a significant proportion were traumatically injured or neurosurgical patients.
The transfer over five miles utilised the Royal Air Force’s Tactical Medical Wing ‘Jumbulance’ (Figures 1 and 2),
2
with each journey transferring two patients, two nurses and one transfer doctor. On the Saturday morning, the vehicle arrived with a dedicated driver and required stocking with appropriate equipment, spares and supplies for the move. All transfer staff were orientated to the vehicle by the driver prior to commencing transfers. Despite being a much larger vehicle, the internal layout of the ‘Jumbulance’ mirrors that of a regular ambulance with the patients being loaded head first on the driver’s side of the vehicle. All ventilators, monitoring, infusion pumps and drainage bags were located on the patient’s right hand side to facilitate safe and easy loading into the ‘Jumbulance’, as well as allowing constant visibility during transit. It was felt unnecessary to re-site patient lines to facilitate access, but security of lines was double-checked prior to transfer.
The Royal Air Force ‘Jumbulance’. Interior of Royal Air Force ‘Jumbulance’.

Following the Southmead unit move, a similar approach was taken, with early morning team briefings, staff allocation, and patient review by a consultant prior to each transfer. Transfers were commenced with those anticipated to be most stable and those predicted to be most unstable or complex transferred in the middle of each day. All procedures and investigations were completed prior to transfer.
The additional complexity of this move necessitated a detailed plan for the day with timings for each move ‘cycle’ along with progressive transfer of staff to the new unit across each day as patient numbers changed (Figure 3). Care was taken to ensure that the dedicated transfer team of four nurses and one registrar each day received sufficient breaks with food and drink to avoid fatigue.
Planned transfer cycle timings from Frenchay Hospital to Brunel Building, Southmead Hospital.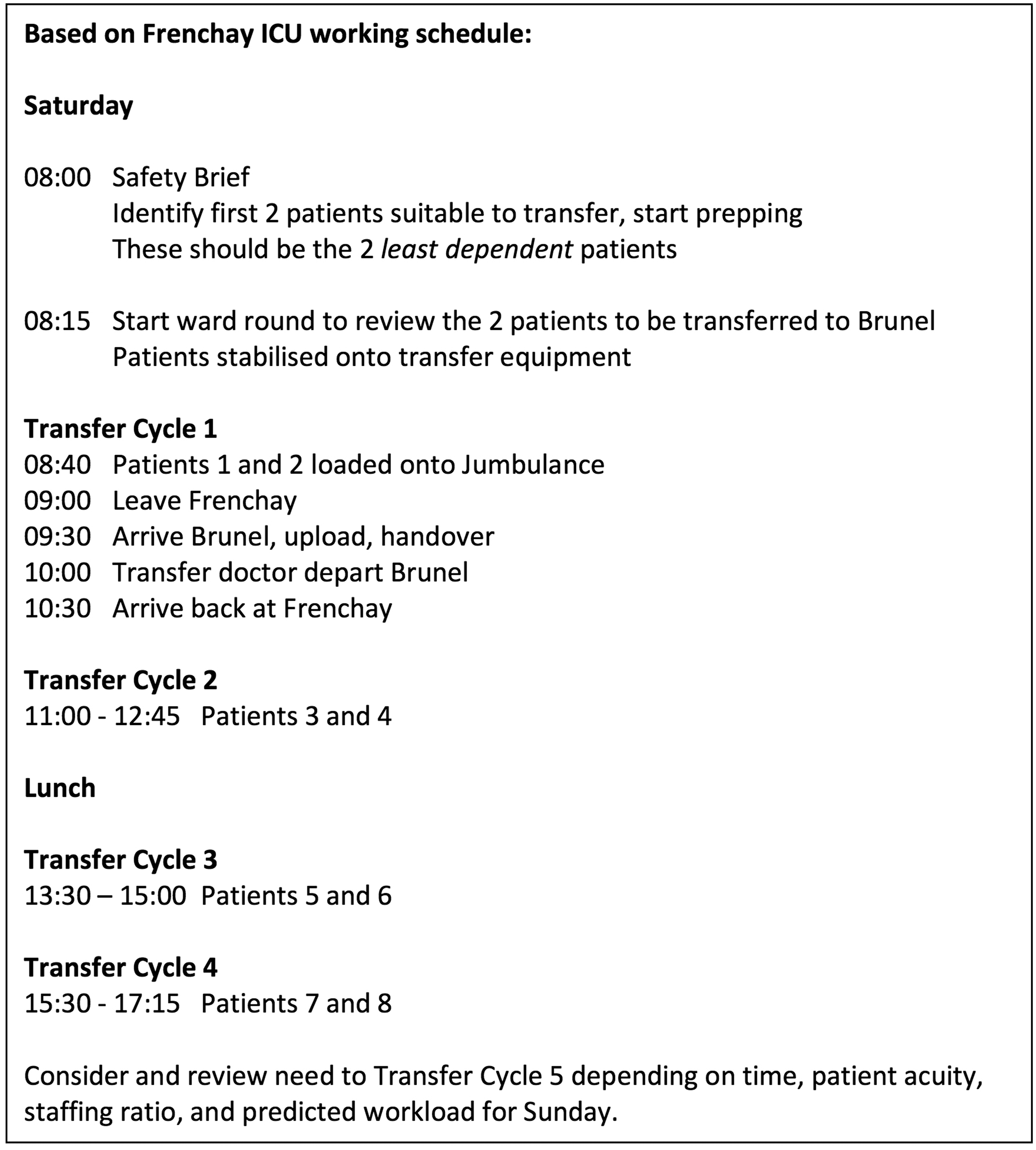
At the beginning of each transfer, the patient was moved onto an ambulance trolley and equipment safely secured prior to leaving the unit. Two patients at a time were then loaded into the ‘Jumbulance’, which was parked immediately outside the unit.
The Trust Control Room was alerted prior to each patient transfer, and again within 2 min arrival at Southmead Hospital, to ensure all staff were present and thoroughfares were cleared.
On arrival at Southmead Hospital, the patients were offloaded and moved through the unopened Emergency Department to the new unit via a lift. An extra doctor from the new unit along with porters facilitated this journey from the ‘Jumbulance’ to maintain patient safety.
On arrival at the new unit, monitoring was transferred and a verbal handover given. The transfer was documented on the South West Critical Care Transfer Form, which included routine patient observations, ventilation parameters and drug infusions.
Towards the end of the days, the lead consultant and senior nurse contacted staff due to work that night to confirm the location that each person was required to work. They also ensured that the day staff were repatriated to Frenchay if needed.
A short debrief was held at the end of the first day to reflect upon our experiences and discuss the need for any changes. The nursing and medical teams were happy with the conduct and logistics of the transfers and it was agreed that no changes were required.
In total, 5 level two and 13 level three patients were transferred over the two days. The only incident was a small leak of urine from a collection bag after it was caught in the ambulance trolley wheel.
One level three patient with an unsurvivable brain injury was not transferred pending brainstem death testing and organ donation. This eventuality had been anticipated in the planning stages and was communicated early to family members who were in agreement. Once again, this patient was moved to theatre recovery with accompanying intensive care nurse.
Reflections
Our experience led to us reflecting upon and debriefing the process. A number of practical challenges present themselves when moving into a new hospital building, ranging from ensuring teams do not get lost, to provision of food and drink.
A significant challenge with two sites and a new unit was to ensure that equipment and drugs – such as ECG machines, haemofilters and anaesthetic drugs – are in the correct location when needed. Whilst there were spare haemofilters available, at Southmead ICU, at the time there was only one ECG machine and so a decision was made as to the most appropriate time to move that and other similar equipment.
The transfers themselves were both mentally and physically exhausting for staff. We ensured that food and drink were provided (the new building café had not opened) and regular breaks taken. On the longer transfers, the conservation of power and medical gases was essential, and checks were made prior to each ‘cycle’ to ensure that each was adequate. Spare batteries, pumps and ventilators were made available. Sufficient power supply was available to negate the requirement for a power inverter, although this was considered before use of the ‘Jumbulance’ was confirmed.
A further challenge was to maintain the provision of effective and safe intensive care at both sites throughout the transfer period. As patient numbers increased in the new unit, staffing levels needed to change to reflect this. Junior doctors and some nurses were transferred at stages during the days.
Frenchay Hospital remained the regional Major Trauma Centre until 2 a.m. on 19 May and so staffing was maintained for potential admissions. After this time, there was a gradual movement of ward patients from Frenchay and so a contingency plan was put in place in anticipation of management of any deteriorating patients.
Finally, throughout the planning and the transfer period, emphasis was made on ensuring that each patient was in the most appropriate location for their clinical needs. This necessitated changing the order of transfers during the day, and as previously described, delaying the transfer of one patient from each unit.
Overall, we reflected upon our experiences and would not change the way in which we approached the task, the planning or the execution. Over the course of three days in May 2014, a total of 24 critically ill patients were transferred by the critical care transfer team into the new Brunel building at Southmead Hospital. The transfers were performed without significant incident, without any patient or relative complaint, and under intense scrutiny from both the Trust and the media. This success, possible only through the planning and efforts of all the ICU staff, was formally recognised by the executive team. The ICU team were asked to make one of only two clinical presentations at the Trust’s annual general meeting to show the public the success of this transfer process and were encouraged by the executive team to publish our experiences.
Footnotes
Acknowledgements
The authors would like to acknowledge the staff members of the ICU, Southmead Hospital for their contribution to the content of this work: Dominique Duma, Matron; Dr Jasmeet Soar, Consultant in Anaesthesia & Intensive Care; Ms Clare Soppitt, Senior Sister; Dr Ian Thomas, Consultant in Anaesthesia & Intensive Care; Dr Curtis Whittle, Consultant in Anaesthesia
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.