
Abstract
Introduction
Bereaved ICU family members frequently experience anxiety, depression and post-traumatic stress disorder, which have been associated with significantly impaired quality of life. Recognising that their needs extend beyond the support provided by their friends and family, the Intensive Care Society had published in 1998 recommendations around bereavement care.
Objective
The aim of the present national audit was to compare bereavement services in England against the nine recommendations set out by the Intensive Care Society guidelines.
Methods
A telephone audit was carried out in all adult ICUs in England.
Results
A total of 144 NHS Trusts (179 ICUs) met the inclusion criteria and 113 responses were collected (78% of Trusts, 63% of individual ICUs). Although most ICUs provided administrative information (96% had an information booklet), training (53%), auditing (19%) and adequate facilities (27%) did not meet the recommended standards.
Conclusion
Bereavement care is underdeveloped in English ICUs. This important but underreported topic should be prioritised in the critical care research agenda.
Introduction
The death of a relative or a friend is a painful, albeit normal, life experience that frequently has a profound effect on the life of the survivors. 1 Following bereavement, family members may experience feelings of anxiety, depression, debilitating physical features (such as tiredness or sleep disturbances) and symptoms of post-traumatic stress disorder.2–4 These adverse sequelae have been associated with significantly impaired quality of life and negative health outcomes, 4 increased economic burden 5 and high prevalence of psychiatric illnesses, 6 that appear to be more prevalent when the death occurs in an intensive care unit (ICU). The unexpected nature of the loss, its frequent occurrence after life sustaining treatment decisions and a discordance between the caregivers’ preferred and actual roles in these decisions have been highlighted in the ICU literature as major stressors, with significant consequences over and above the death of a family member.2,6–9
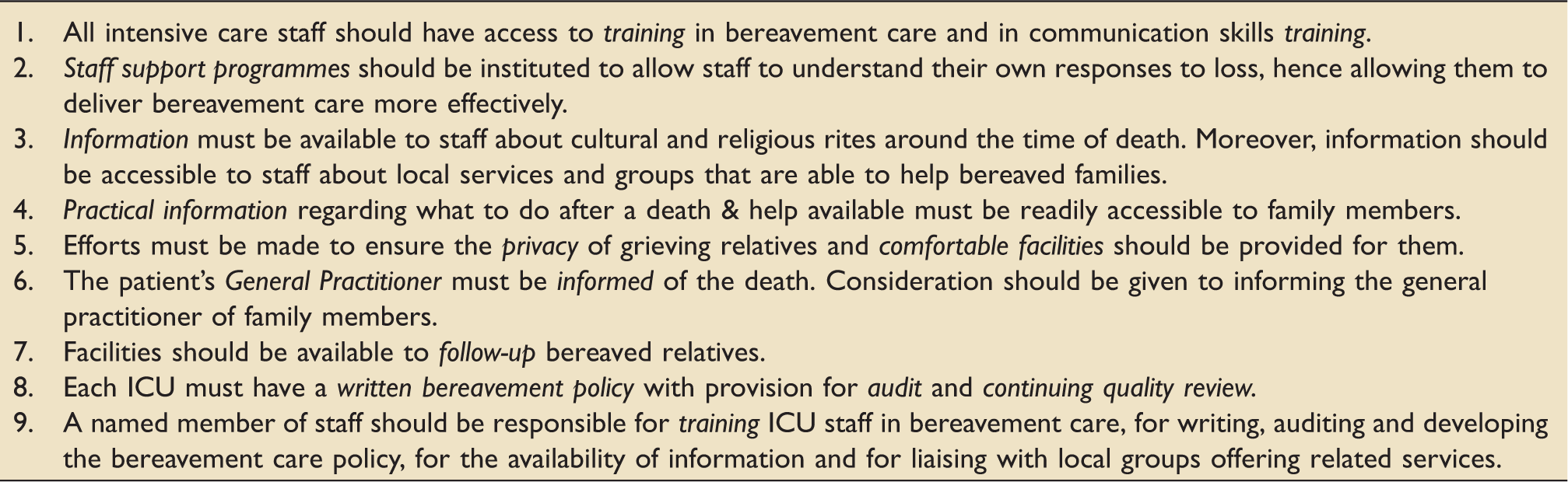
In this context, the needs of the bereaved are likely to extend beyond the support provided by their friends and family. As a result, a formalised bereavement service after an ICU death has been advocated by some Critical Care Societies.10,11 In 1998, the UK Intensive Care Society (ICS) published comprehensive guidelines outlining the importance of a bereavement service in ICU, following a nation-wide survey. 11 Training in bereavement care (BC) and communication skills, identifying a named lead for BC, as well as providing information around local services and groups able to help bereaved families were some of the recommendations stated in the document. The importance attached to BC by the ICS guidelines has not been mirrored in the Guidelines for Provision of Intensive Care Services – the recently published ‘reference source for the planning and delivery of UK Intensive Care Services’ – which makes no mention of BC. 12
Key recommendations of the 1998 ICS bereavement care guidelines.
Methods
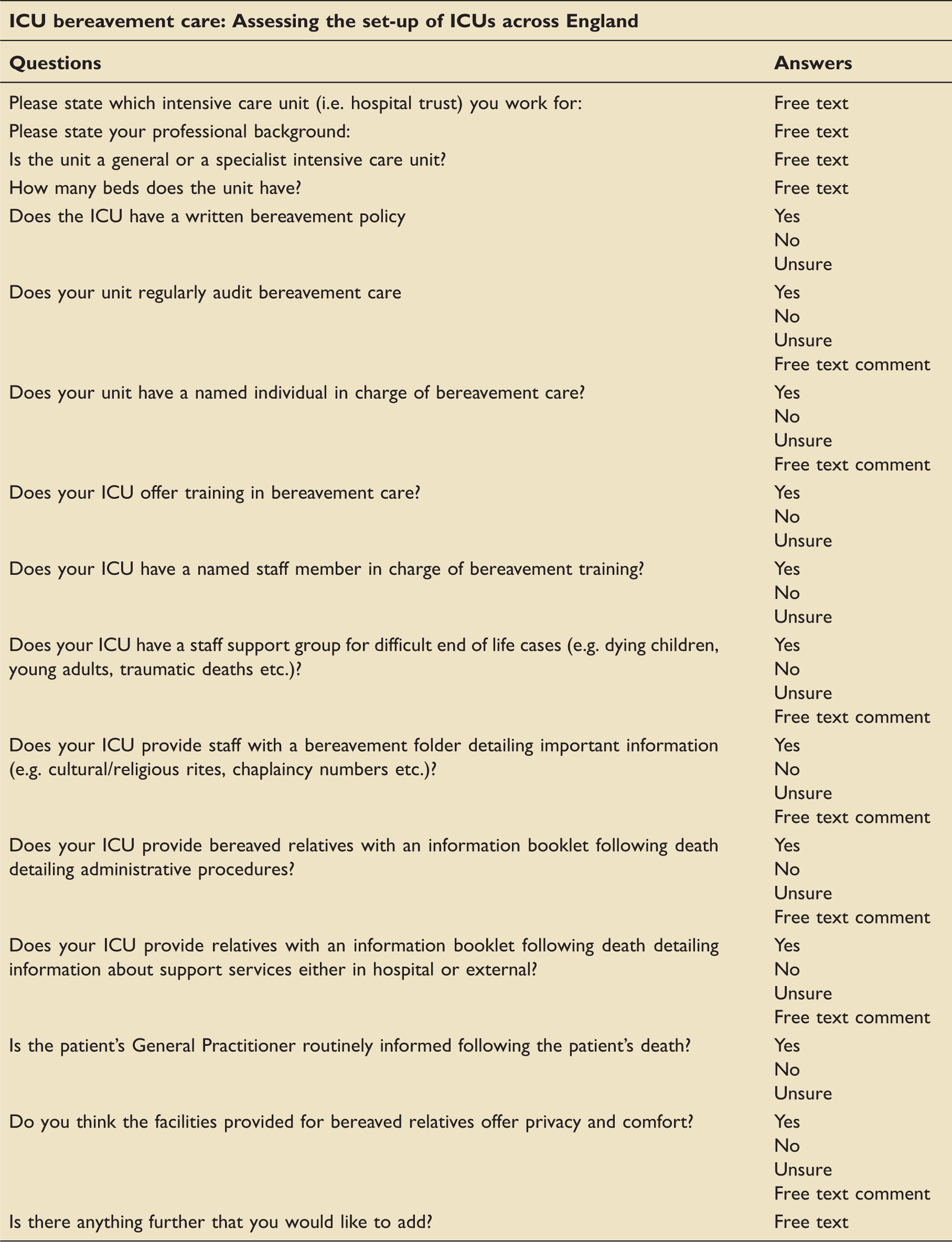
Using the Health and Social Care Information Centre website (http://www.hscic.gov.uk/catalogue/PUB10416), 153 NHS Trusts submitting critical care data were identified in England (appendix I in the supplementary material, available online). Paediatric and neonatal ICUs, units with less than four beds and those providing solely High Dependency Care (as defined by the ICS), were excluded from the survey, whereas information was gathered from both specialist and non-specialists units.
Survey questionnaire.
Themes extracted from the ICS bereavement guidelines.
The survey was endorsed by the ICS.
Results
A total of 144 NHS Trusts (179 separate ICUs) met the inclusion criteria and 113 complete data sets were collected (Figure 1). This corresponds to a response rate of 78% of the participating Trusts and 63% of the individual ICUs. The majority of the participating units were general ICUs (80%) with a median number of beds of 12.
Results.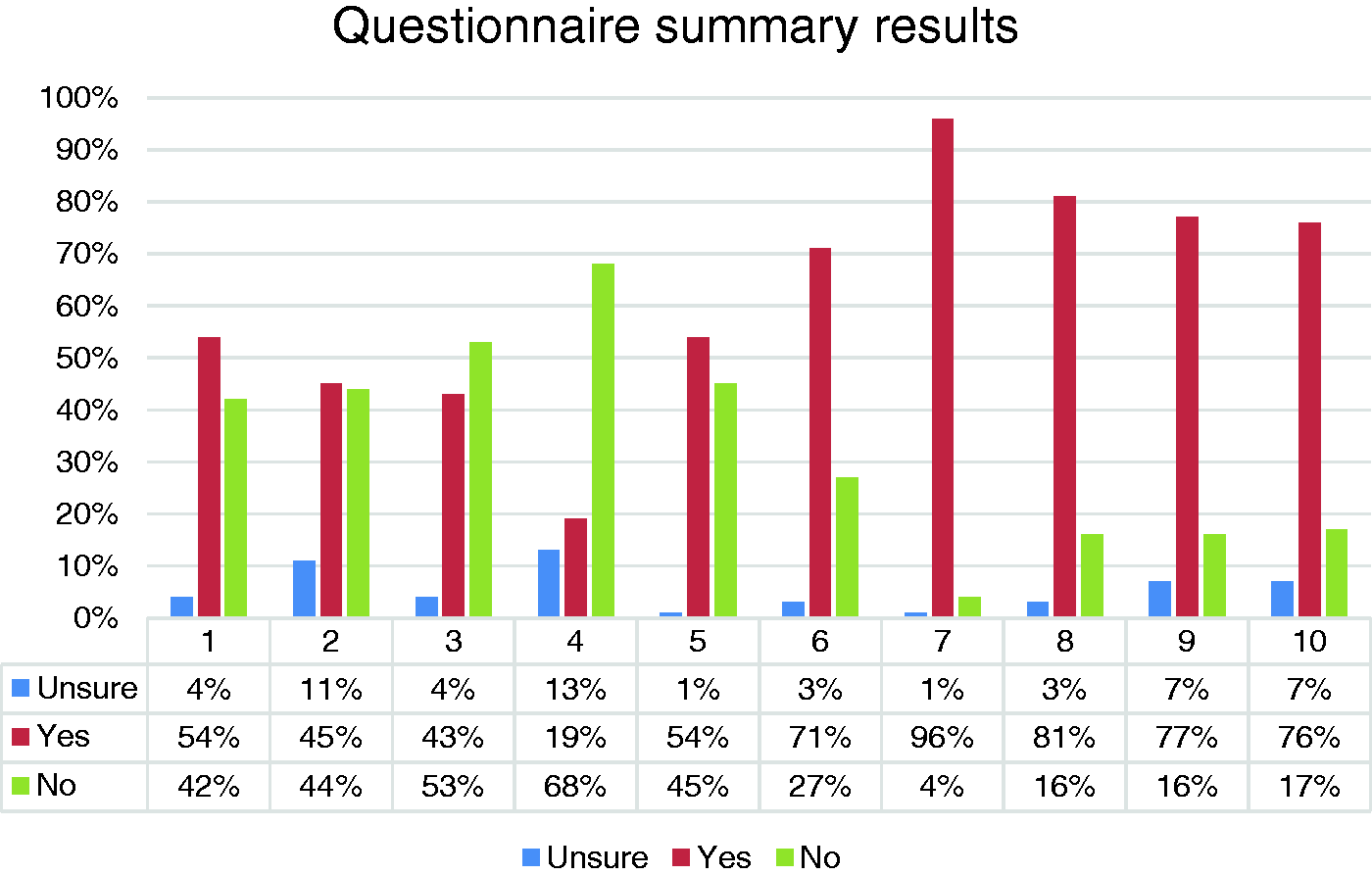
Training
More than half of the responders (53%) denied access to training in BC and communication skills, with even fewer being aware of a named member of staff responsible for this training (20%).
Staff support
Only about half of the ICUs (54%) reported access to formal staff support groups. However, some form of informal mechanism, aimed at helping staff cope with challenging end-of-life situations, was mentioned in 47% of the surveyed ICUs.
Information provision
The majority of the interviewed nurses (81%) reported that a bereavement folder was available in their ICU, allowing them to comprehensively inform bereaved families about cultural and religious rites, as well as suggest local services and support groups available to help them. The presence of an information booklet was reported in 96% of the ICUs, ensuring that administrative information on the actions following a death was offered. In 77% of the cases, the individual’s death was routinely passed on to their general practitioner (GP), whereas the relatives’ GP was informed on a completely ad-hoc basis.
Facilities
About one quarter of the responders (27%) felt that the available facilities for grieving families were neither comfortable, nor respecting their privacy.
Follow-up services
A structured booklet listing organisations and groups available at a local and national level which could provide follow-up bereavement support was given to the next of kin(s) in 76% of the cases. A minority (17%) of ICUs did not provide any information at all regarding follow-up.
Governance
A named member of staff responsible for writing, auditing and developing BC policy was identified by half (54%) of the participants. A written BC policy and regular audit of the service was available in only 45% and 19% of the interviewed ICUs, respectively.
Discussion
This is, to the best of our knowledge, the first national audit of the ICS guidelines on BC since their publication in 1998. The last national survey that took place in 1995 and resulted in the publication of these guidelines revealed considerable shortcomings in BC, with lack of training in dealing with the bereaved, suboptimal facilities and follow-up support featuring prominently. The publication demonstrated feelings of inadequacy among staff because of the inefficient care provided and a widespread interest in improving facilities and receiving appropriate training. 13 Against this backdrop the ICS, recognising the importance of BC, attempted to map out best practice guidelines. 11
The present audit assessed whether the recommendations issued by the ICS more than 15 years ago were embedded in everyday ICU practice. It was a snapshot of the BC provided in England, as perceived by senior critical care nursing staff. It was welcomed by all the units, with the participants engaging strongly with all the themes presented, either to present the positive processes in place (information provided, staff support) but mainly to express frustration about the lack of these (facilities, leadership and training).
Approximately one in five patients will die in ICU14,15 and the transition from curative to palliative care might be fast and frequently unexpected. Nurses have traditionally been the healthcare providers spending the largest amount of time with patients and their families, and describe a strong sense of commitment that extends beyond the care of the living to the facilitation of a ‘good death’. 16 This aspect of the nursing role can be a source of considerable stress, leading to feelings of incompetence, discomfort, grief, compassion fatigue and moral distress.17–19 Similar negative emotions have also been reported by senior and junior ICU clinicians. 19 Easy access to communication fora and the presence of staff support groups are well-recognised measures for minimising unhealthy behaviours and attitudes.18,20 In the current survey, just over half of the NHS Trusts surveyed had formal groups available, an increase from the 1995 survey where only 23% reported such services. Even though the absence of formal arrangements does not necessarily mean a lack of support for the caregivers, creating a firmly embedded forum might enable staff to understand their own responses to grief and deliver care more effectively.
An integral aspect of working in ICU is the assumed responsibility not only to support the bereaved emotionally after a death, but also to provide practical information about the next steps. 21 In order to achieve that staff need to be aware of the psychological aspects of bereavement, the cultural and religious rites associated with dying, the available support mechanisms for relatives and the administrative and legal requirements after a death.11,22 A clear gap between the current education delivery for ICU staff and the expected skills in family support, communication and counselling has been identified by the current survey and is in accordance with previously reported data.16,23 Less than 50% of the interviewees were offered any training in BC, despite a well-documented willingness to receive such formal training. 24 The reported lack of a named individual responsible for training and of written BC polices further emphasises the absence of formalised structures, leading staff to utilise peer mentoring and role-modelling in order to ‘learn’ how to provide better BC. 16
In order to provide high quality BC, ‘all efforts must be made to ensure the privacy of grieving relatives and comfortable facilities should be provided for them’; a recommendation clearly stated in the ICS guidelines. These facilities would not only assure privacy for the bereaved, but also enable the presence of relatives and friends at the time of a patient’s death, a well-recognised positive factor in facilitating bereavement.23,25 Only 26% of the participating ICUs reported the availability of such structures in the audit, while the majority of the interviewees commented negatively on either their absence or their poor functionality.
In agreement with recent publications,26,27 limited, inconsistent provision of BC follow up was noted in the present survey. Although the actual support measures,28,29 the timing30,31 and even the absolute need for a bereavement intervention are widely contested,1,26,32,33 a follow-up meeting after a death has been reported to be of benefit both in the paediatric and the adult ICU population.24,34,35 The complete lack of reference to BC in the recently published Guidelines for Provision of Intensive Care Services 12 highlights the varied (and often non-existent) focus on bereavement pathways in critical care medicine in the UK, a need already addressed in the US recommendations. 10 For a substantial minority, the normal, natural experience of the death of a loved one will result in severe grief-related disorders, like prolonged grief disorder and complicated grief, conditions that require formal support.26,36 Although there is no evidence to support routine intervention for all bereaved individuals, 1 ‘universal and equitable’ access to bereavement services is recommended by the Department of Health, 26 even if it is only to understand the cause of death. 34 The role of the GPs is paramount in this process, 37 as recognised by 77% of the NHS Trusts that reported the presence of structures in their ICUs which enabled the follow up of bereaved relatives by GPs.
Our survey has several limitations. Out of the 179 separate ICUs contacted, there were 113 completed datasets collected, a response rate (63%) that is lower than the recommended for medical literature. 38 However, almost all of the 113 hospitals were part of a different acute NHS Trust and the working assumption was that the existence of established BC policies and structures would be unified in all hospitals of the Trust or at least known to the senior members of staff that were interviewed. It was also asserted that when BC services were absent from the largest hospital in a Trust, it would be unlikely to be present in the other (smaller) hospitals. Even though this was not specifically assessed in the study, it is logically plausible, and it would mean that the presented results may have actually underestimated how underdeveloped BC is in England. The reason the questions were addressed to the senior nursing member of the particular shift was the assumption that they would be more readily available and better informed about their hospital’s policies and procedures on BC than their medical colleagues. Another limitation is the inherent bias of the research method used, as survey questionnaires provide a limited amount of information and are heavily dependent both on the posed questions and the participant replies. The questions of the current survey were based on the 1998 ICS guidelines, which enabled direct comparisons but could not completely eliminate any systematic source of error. The conclusions drawn are dependent on the individual responses which could be erroneous, such that a discrepancy between the survey results and the reality of BC in England could not be ruled out. A strong argument against this view, however, is the consistency of the practices described in the present study with those in the international literature.
In summary, although several aspects of BC such as information provision are adequately addressed in the surveyed English ICUs, others like training, staff support and the existence of robust governance structure and appropriate facilities are still underdeveloped. Even though the ICS guidelines provided a number of BC quality indicators, their current validity, relevance and applicability needs to be subject to rigorous scrutiny and evaluation. Research-based data to support the introduction, exact structure, timing of initiation and duration of bereavement pathways in everyday ICU practice is paramount. Their importance, as described in the conclusion statement of the Society’s 1998 publication, still stands true: ‘… improvements may reduce not only levels of stress amongst staff but also post-bereavement morbidity or mortality amongst patients’ relatives’.
Footnotes
Acknowledgement
We thank all participants who answered our telephone questionnaire.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.