
Abstract
Background
Critical care management of patients undergoing transcatheter aortic valve implantation (TAVI) is a major determinant of their outcome.
Aims
The aim of this study was to compare the prognostic performance of four general scoring systems [Acute Physiology and Chronic Health Evaluation (APACHE), Simplified Acute Physiology Score (SAPS), Sequential Organ Failure Assessment (SOFA), and MultiOrgan Dysfunction (MOD) scores] in TAVI patients.
Methods
Between 1 June 2008 and 30 June 2014, 75 patients (81.2 ± 6.4 years old, 36 men and 39 women) who underwent TAVI were scored during the first 24 h of their stay at the intensive care unit (ICU). The outcome measures were in-hospital and 30-day mortality and in-hospital and 30-day morbidity defined as myocardial infarction, implantation of permanent pacemaker, stroke, tamponade, major bleeding, vascular access site complications and prolonged ventilation.
Results
Four patients (5.3%) died in ICU and one more during follow-up, indicating a 30-day mortality rate of 6.6%. Regarding in-hospital mortality, the area under the ROC curve (AUC) was 0.92 for SAPS II, 0.88 for APACHE II, 0.73 for MODS and 0.74 for SOFA. Regarding 30 day-mortality, SAPS II and APACHE II performed equally higher (AUC = 0.88) than the other two scores (0.79 for MODS and 0.80 for SOFA). SAPS II had the best calibration among all four scores for in-hospital and 30-day mortality (χ2 = 3.06 and χ2 = 3.29, respectively). AUCs for in-hospital and 30-day morbidity were above 0.7 for SAPS II and APACHE II.
Conclusions
SAPS II and APACHE II are reliable mortality and morbidity risk stratification models for TAVI patients with high calibration and discrimination.
Introduction
Transcatheter aortic valve implantation (TAVI) is an increasingly common procedure in high-risk and inoperable patients with severe aortic stenosis.1,2 Patients undergoing TAVI are elderly with multiple co-morbidities and considerable frailty, generating a population of high acuity with great risk of perioperative mortality and morbidity; therefore, post-TAVI Intensive Care Unit (ICU) management has become more complex and challenging.3,4 Despite the less-invasive nature of TAVI compared with conventional open heart surgery, a number of postoperative events and complications have been identified and need to be diagnosed and managed appropriately by intensivists. 5 Aggressive therapies and all manner of support necessary may be utilized in the acute setting, including temporary hemodialysis, intensive treatment of respiratory disorders and early use of broad-spectrum antibiotics as sepsis is often masked in the elderly. 4
Scoring systems were introduced into intensive care medicine to provide valuable tools for judging a patient’s condition and likely outcome. TAVI patients are critically ill patients who require robust models for mortality prediction. Furthermore, the prognostic power of different performance measures has to be evaluated in order to reduce financial costs and improve quality of care.6,7
The purpose of our study was to compare four scoring systems commonly used in critical care management [Acute Physiology and Chronic Health Evaluation (APACHE), Simplified Acute Physiology Score (SAPS), Sequential Organ Failure Assessment (SOFA), and MultiOrgan Dysfunction (MOD) scores] with regard to their immediate and short-term predictive values and clinical applicability for TAVI patients.
Methods
The study sample included all patients with symptomatic aortic valve stenosis (aortic valve area ≤ 0.6 cm2/m2), who underwent TAVI to our department between June 2008 and June 2014. All patients were deemed inoperable or at high surgical risk for conventional surgery by a multidisciplinary team consisting of cardiothoracic surgeons, cardiologists, and anesthesiologists. Screening for TAVI included medical history, physical examination, trans-esophageal echocardiography, carotid ultrasonography, right and left heart catheterization, coronary angiography, aortography and iliac-femoral arteriography, and computed tomography angiography.
Procedural and prosthesis details
Details of the device and the technical aspects of the procedure have been previously described. 8 Briefly, the device used was the 18-french third generation, CoreValve Revalving System which is a self-expandable biological valve. It was inserted using femoral, subclavian or transapical arterial approach. Circulatory support with the insertion of an intra-aortic balloon pump was used only in one case due to severe left ventricular dysfunction. All procedures were performed with surgical back-up and under deep sedation and local anesthesia. General anesthesia and mechanical ventilation were employed only when the subclavian or the transapical arterial approaches were used or when trans-esophageal echocardiography was deemed necessary. Vascular access was performed with the aid of an artery hemostatic device, the Prostar TM XL 10-F system (Abbott Vascular, Redwood City, CA, USA).
Prophylactic antibiotic therapy was administered 1 h prior to the procedure. Pre-procedural medication consisted of aspirin 80 mg and clopidogrel 75 mg once daily, which was also recommended for six months post-implantation followed by aspirin 80 mg indefinitely.
A comparison of the variables included in different scoring systems post-TAVI.
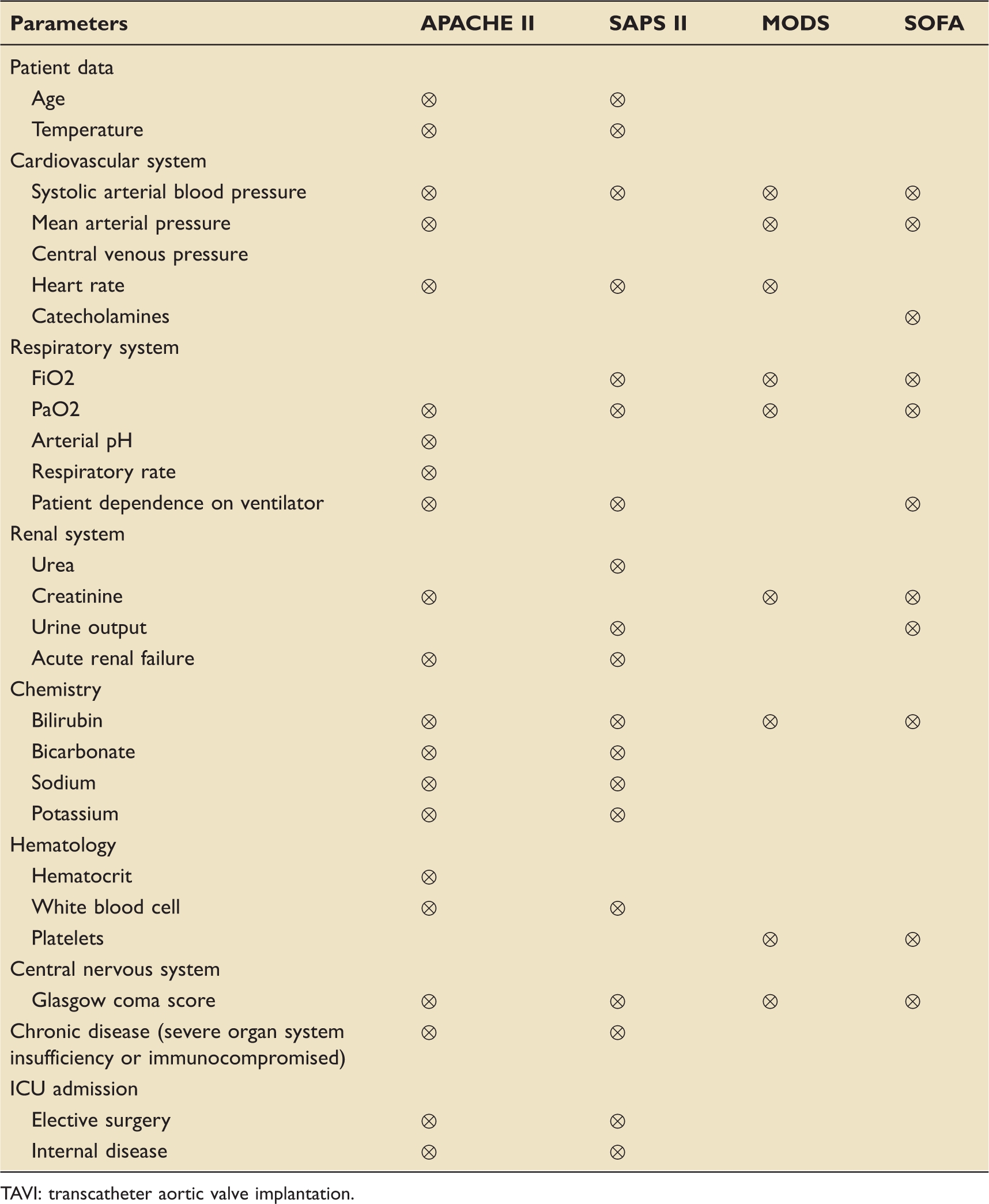
TAVI: transcatheter aortic valve implantation.
The primary outcome was in-hospital mortality, defined as any death occurring before hospital discharge. Morbidity was defined by the following points:
intra- or post-TAVI myocardial infarction, verified by positive creatine kinase-MB in combination with either typical electrocardiographic changes or echocardiographically detected new left ventricular wall motion abnormalities; implantation of permanent pacemaker; stroke (verified by neurological consult or computerized tomography-scan); tamponade; major bleeding; vascular access site complications and prolonged ventilation (>48 h).
Clinical and echocardiographic follow-up was continued for 30 days post TAVI. Thirty-day mortality included any death within 30 days from TAVI.
Statistical analysis
We used t-test for two independent samples or Mann–Whitney test to investigate differences in continuous variables between groups (in-hospital or 30-day mortality/morbidity). Categorical variables were tested using chi-square (χ2) or Fisher’s exact test. Spearman correlation coefficient was used to assess the association between continuous variables. Logistic regression was used to assess the effectiveness of each of the four general scoring systems on mortality/morbidity. The Hosmer & Lemeshow goodness-of-fit test was used for calibration of the models. Α low χ2 value and p > 0.05 indicate good calibration. The area under the receiver operating characteristic (ROC) curve (AUC) was used to asses the discriminative ability (the ability of a scoring system to distinguish between mortality/morbidity or not) of the models. The overall correct classification (OCC; the ratio of correctly predicted mortality/morbidity or not to the total number of patients) was also calculated. All tests were two-sided in a 5% level of statistical significance.
Results
A total of 75 patients underwent TAVI and admitted to the ICU for further care. All TAVI procedures were performed electively and completed successfully in all cases. Transfemoral access was used in 59 (78.6%) cases, transsubclavian in 14 (18.6%) and transaortic in 2 (2.6%) cases. Aortic valvuloplasty was performed prior to the procedure in all patients. A 29 mm CoreValve prosthesis was implanted in 36 cases (48%) and a 26 mm prosthesis in 33 cases (44%). Small 23 mm CoreValve prosthesis and large 31 mm were rarely implanted in three cases each (4%). In five cases, a second valve had to be implanted with a good final result during the same procedure, owing to the fact that the first one was implanted too high. At admission and during the first day of ICU stay, 30 (40%) patients required mechanical ventilation, two (2.6%) received therapy with vasopressors, and two (2.6%) suffered from acute renal failure.
Patients’ characteristics and clinical outcomes including comparison of survivors and non-survivors.
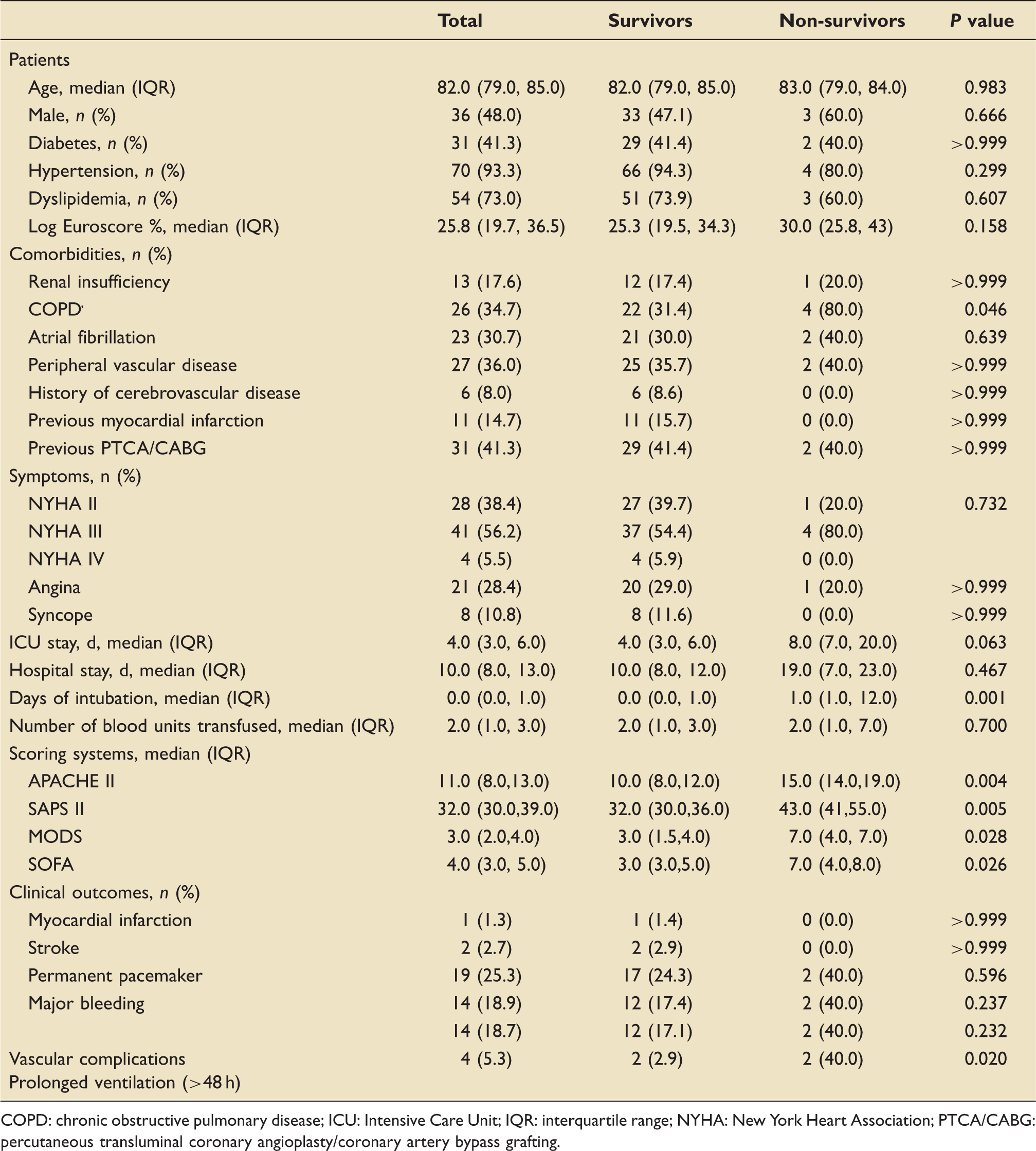
COPD: chronic obstructive pulmonary disease; ICU: Intensive Care Unit; IQR: interquartile range; NYHA: New York Heart Association; PTCA/CABG: percutaneous transluminal coronary angioplasty/coronary artery bypass grafting.
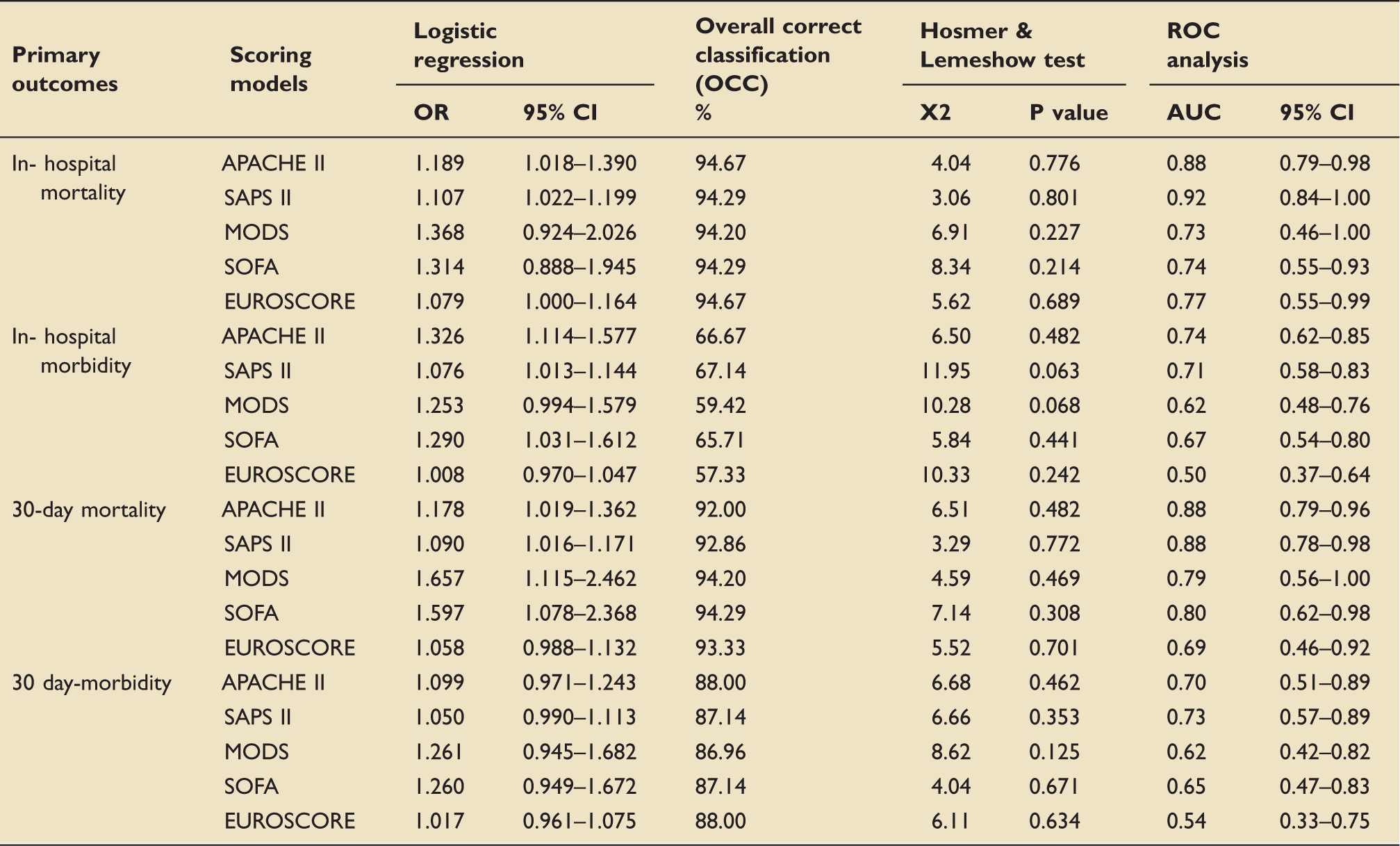
Predicted value of risk scores.
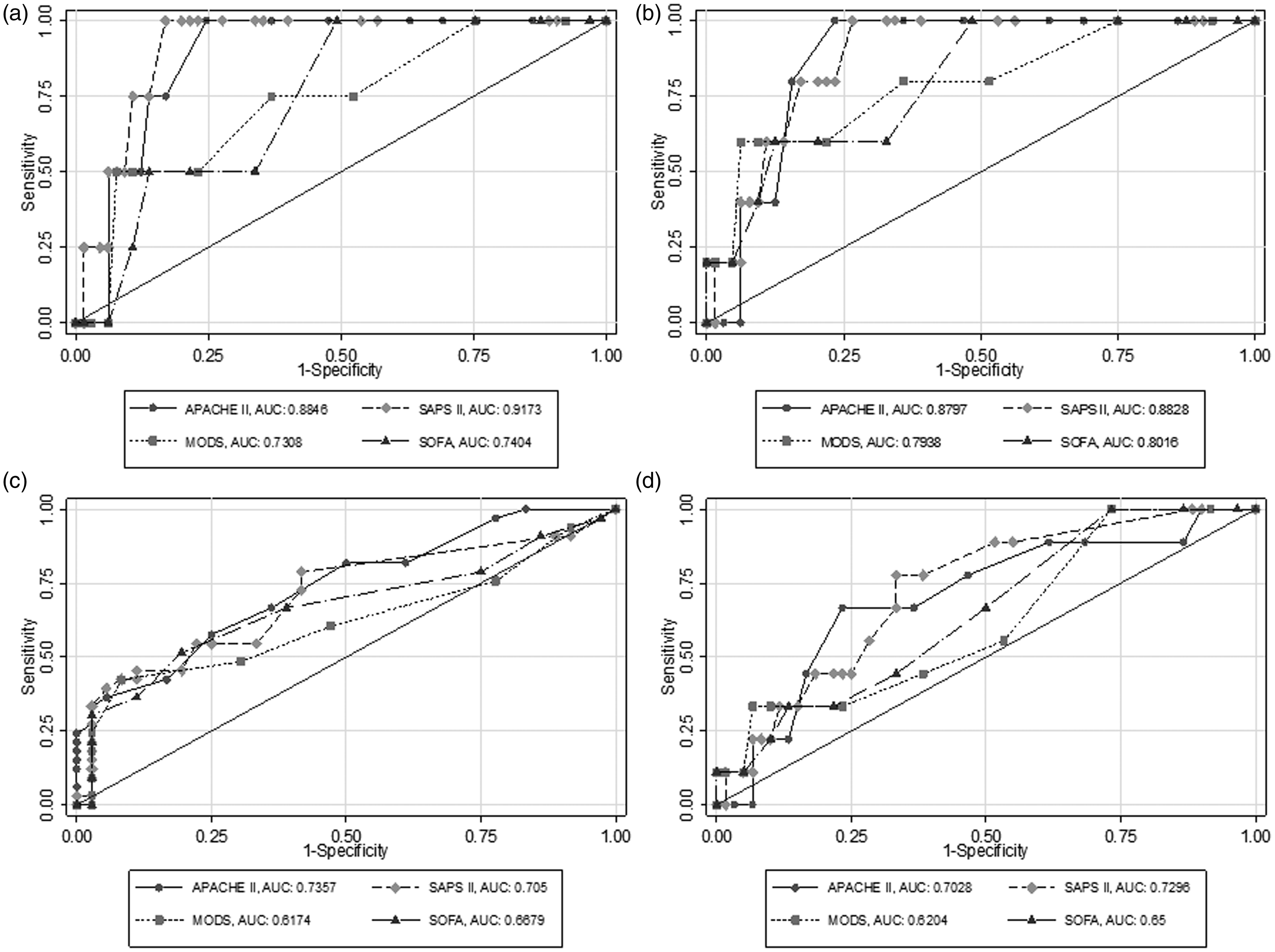
Receiver operating characteristic curves of APACHE II, SAPS II, MODS and SOFA for in-hospital mortality (a), 30-day mortality (b), in-hospital morbidity (c) and 30-day morbidity (d).
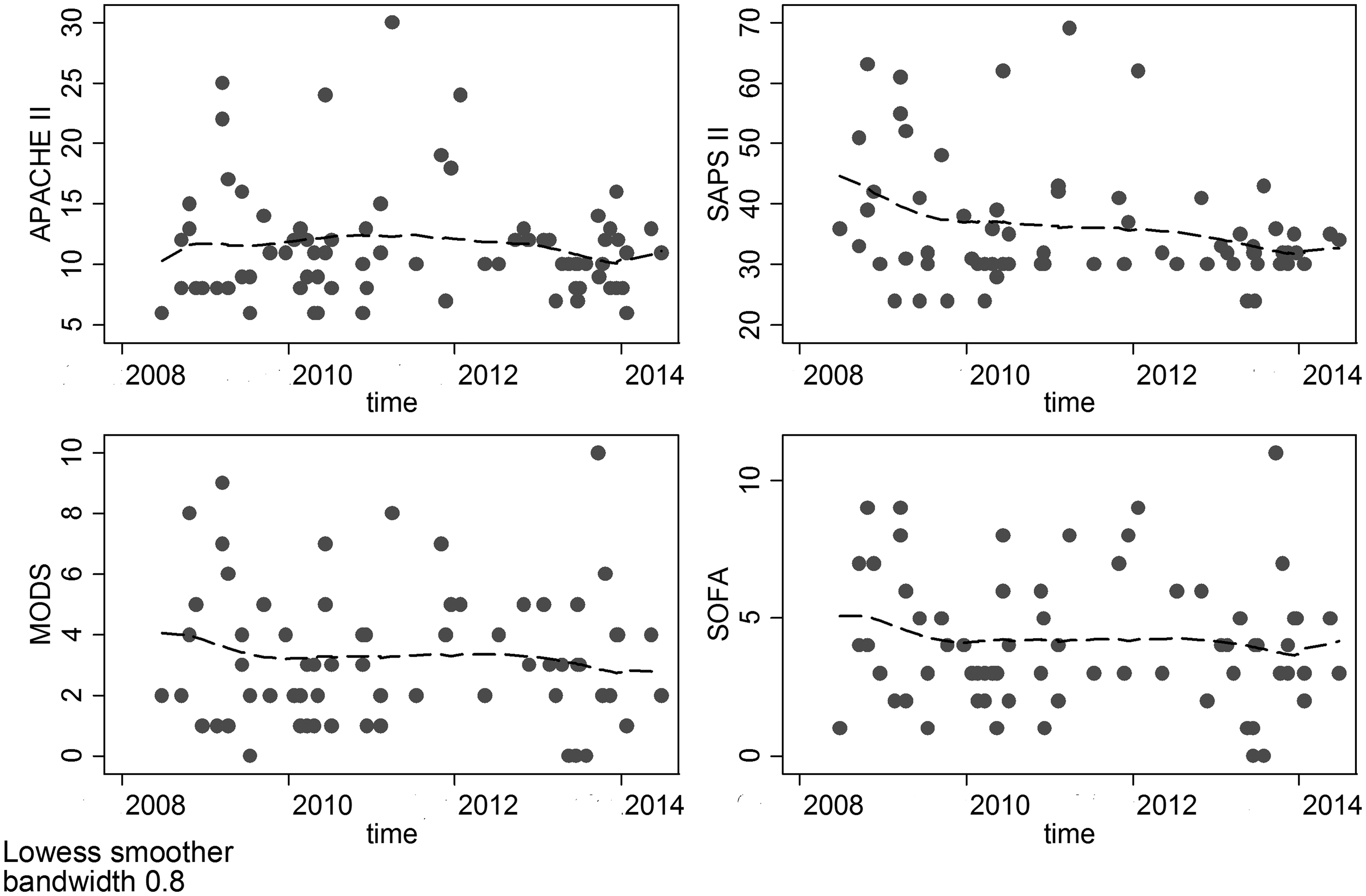
APACHE II, SAPS II, MODS and SOFA over the course of the 6-year study period.
APACHE II and SAPS II were significantly associated with ICU length of stay (r = 0.44, p < 0.001 and r = 0.36, p = 0.002, respectively), days of hospitalization (r = 0.27, p = 0.020 and r = 0.44, p < 0.001, respectively) and number of blood units transfused per patient (r = 0.44, p < 0.001 and r = 0.30, p = 0.012, respectively). MODS and SOFA were significantly associated with ICU length of stay (r = 0.27, p = 0.02 and r = 0.44, p < 0.001, respectively) and number of blood units transfused per patient (r = 0.28, p = 0.022 and r = 0.27, p = 0.022, respectively).
Discussion
The main findings of our study are: (1) SAPS II and APACHE II outperformed MODS and SOFA scores in terms of in-hospital and 30-day mortality. (2) The predicted value of all of the studied risk models for mortality were greater than that for morbidity. (3) Patients with high severity of illness, as assessed by SAPS II or APACHE II, have longer ICU and hospital stays as well as are more frequently transfused. To our knowledge, this report is the first to compare ICU scoring systems with regard to their validity in a cohort of TAVI patients.
SAPS II and APACHE II are two of the most frequently used general mortality prediction models, which have been extensively validated.9–11 The accuracy of prognostic scoring systems depends on the assessment of both calibration and discrimination.12,13 SAPS II and APACHE II demonstrated better calibration and highest discrimination in our study population compared to the other two scores, indicating their superior performance. Our study shows that scores using a large number of data inputs outperform simpler scores in TAVI population. Although greater score complexities may increase the barrier to calculation, as it increases the likehood some required variables may not be available, it seems that additional clinical information account for the better mortality prediction in our study population.
The good prognostic abilities of SAPS II and APACHE II in this study suggest that they could be used to prospectively identify sicker patients who may require more aggressive post procedural care and for whom increased resource utilization may be justified. SAPS II and APACHE II, which include not only risk factors but also information about the patient situation after the procedure, seem to perform better than Euroscore, a specific purpose risk model, which considers only patient preoperative conditions.
All studied prediction models in TAVI patients demonstrated a similar pattern for morbidity – worse discrimination and poorer calibration compared to mortality. Only SOFA showed better calibration for morbidity compared to mortality, as expected, since it was specifically designed for the prediction of morbidity in patients with sepsis. 14 Mortality is the most frequently reported outcome parameter in evaluating risk scores due to objectivity in data acquisition, whereas the objective parameters for morbidity are harder to define. 15 Candidates for TAVI have several comorbidities and are at greater risk for postoperative morbidity; therefore, prompt recognition of complications is critical to improve patient outcome. Several postoperative events, such as atrioventricular blocks, myocardial infarction, stroke or vascular complications, have significant impact not only on patients’ outcome after TAVI but on health care cost and quality of life as well. 16 The heterogeneity of morbidity parameters, like the need for mechanical device or reoperation for bleeding, along with the initial lack of standardized definitions makes it difficult to find common risk factors for a statistically sound prediction of overall morbidity. 17 However, risk stratification using SAPS II and APACHE II and for at least certain morbidity events appear to be acceptable according to our findings.
The length of ICU stay is commonly used as measure of cost and for assessing adequate unit efficiency, despite variations which may be attributed to patient and selected institutional characteristics. 18 It is shown that all studied risk scores could be reliable in predicting ICU length of stay in TAVI population, likely due to the standardized therapeutic management during their ICU stay. SAPS II and APACHE II could also identify patients at risk for a prolonged hospital stay post-TAVI. It seems that these two scores are better indicators of the severity of complications arising during prolonged ICU stay compared to MODS and SOFA. Furthermore, these risk scores can be used so that patients at risk are not discharged too early potentially leading to ICU readmission and/or prolonged hospital stay, both of which are associated with higher mortality rates.
Blood transfusions are frequently required after TAVI even in the absence of overt bleeding or vascular complications and have been significantly associated with impaired short- and mid-term outcome.19,20 Based on our results, total transfusions indicate TAVI patients of higher risk and worse outcome as reflected by their correlation with the studied severity-of-illness scores evaluated over the first 24 h of ICU admission. Since multiple blood transfusions are associated with considerable risk, including immune suppression and increased risk of nosocomial infections, therapeutic interventions and prevention methods to reduce transfusions will potentially benefit post TAVI patient care.
It is important to recognize inherent limitations, which exist in the application of prognostic scoring systems to individual patients. Our study is also limited due to its retrospective nature, small sample size, long data collection period and single institution design. It seems likely that TAVI complications, management and approach to ICU care – which may be important determinants of mortality – have changed during the observation time period, although no significant change was observed over the course of time. Similarly, it is probable that patient selection and the perioperative handling could vary between different ICUs. Further prospective studies with a larger sample size and comparison among medical centers are needed to estimate the prognostic ICU performance of risk scoring in TAVI patients.
Conclusions
As the actual TAVI procedure becomes increasingly streamlined in high-risk elderly patients, it stands to reason that patients’ comorbidities and acute illness following TAVI will be the most important predictors of morbidity and mortality. Therefore, accurate clinical risk predictors will likely have an important role in assessing outcomes and quality. Although accurate risk predictors will probably rise out of the TAVI registries, it is also important to assess the performance of current models as they pertain to TAVI. SAPS II and APACHE II seem to be the most appropriate general ICU scoring systems for immediate and short-term mortality prediction in TAVI population allowing for earlier more aggressive therapeutic interventions.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.