
Abstract
Purpose
We aimed to determine if Modified Early Warning Score could be used as a surrogate for the Association of United Kingdom University Hospitals dependency scoring in improving patient flow into higher areas of care. In particular, focus was to be placed on the impact of Critical Care expansion on the size of the populations of patients being managed outside of Critical Care with an Association of United Kingdom University Hospitals requirement of Level 2.
Materials and Methods
We conducted snapshot assessments of illness severity using Modified Early Warning Score and Association of United Kingdom University Hospitals dependency scores on all inpatients in a large, rural acute hospital during two five-day periods.
Results
A total of 3850 patients were reviewed: 1854 in Study Period 1 and 1996 during Study Period 2. A total of 3113 (80.9%) patients had an Association of United Kingdom University Hospitals care level of 0. There was no statistically significant difference between the patients reviewed in each study period when analysed by Association of United Kingdom University Hospitals care level (p = 0.575). Eighty-nine patients required Level 2 care (inclusive of those in Critical Care). Study Period 1 had 32 Level 2 patients managed on the ward. Study Period 2 demonstrated a statistically significant increase in the proportion of these patients cared for in a Critical Care environment (37.3%–68.4% (p = 0.0036)). This was facilitated by an expansion in Critical Care capacity between the two study periods as a result of the findings in Study Period 1.
Conclusion
We have shown that hospital inpatient data on illness severity are an essential tool in bed management and Critical Care capacity planning. We were able to demonstrate a fall in the number of Level 2 patients managed on a general ward environment following an expansion in Critical Care bed capacity. We also demonstrated that a Modified Early Warning Score of greater than 4 was associated with an increase in assessed care level requirement.
Introduction
The United Kingdom NHS is facing unprecedented pressure to deliver ever more efficient care. Significant focus has been placed on improved patient safety, superior outcomes and lower mortality rates. In the acute sector, workload is increasing at a rate where many hospitals struggle to provide high-quality care within budget. 1 Demands on hospital systems are greatest in unscheduled emergency care, which, in turn, has a significant adverse impact on scheduled elective care, particularly in the winter. 2
There is variation in systems dealing with emergency care across the United Kingdom. 3 NHS acute hospitals strive to maintain best practice standards for all patients. On a hospital-wide scale, this primarily requires optimal management of patient flow through the hospital, and on ensuring that all patients receive timely intervention in an appropriate clinical setting from the specialist teams relevant to their condition. The systems of bed management and flow control underpinning this approach often vary between hospitals 4 depending upon historical service development and culture. On an individual patient-level scale, there has been recent emphasis on the importance of recognition of the severity of individual patients’ illness and its impact on patient physiology and physiological reserve. These factors are coupled to plan the extent of treatment escalation or palliation in the event of deterioration. 5 Patient acuity has become a term often used to describe the severity of illness and the associated physiological impact.6,7
Tools exist to enable acute hospitals to identify acuity in their inpatient populations. The Modified Early Warning Score (MEWS) developed by intensive care physicians was recently renamed as the National Early Warning Score (NEWS) by NHS England as part of a drive to improve acuity recognition in acute NHS hospitals and trigger early referral for specialist input.8,9 The Association of United Kingdom University Hospitals (AUKUH) acuity tool is widely used to characterise individual patient care needs by assigning a level of care to each individual; this is generally a tool used within High Dependency and intensive care areas.7,10 We believe that it is possible to model the inpatient hospital population using these tools in a manner that allows tailoring of service provision to the acuity of the local population. In particular, the relative simplicity of the MEWS system makes it appealing, if it can be correlated to the more comprehensive AUKUH scale.
Methods
Details of this study were forwarded to the Research and Development Department at the Royal Cornwall Hospital NHS Trust. It was deemed that no ethical approval was required to conduct this audit as no direct patient contact was involved.
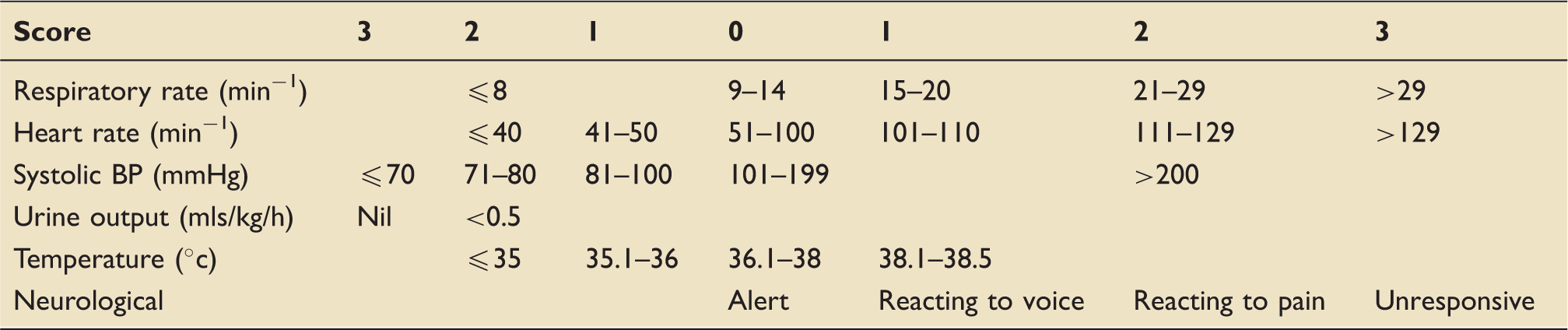
Modified early warning scoring system. 11
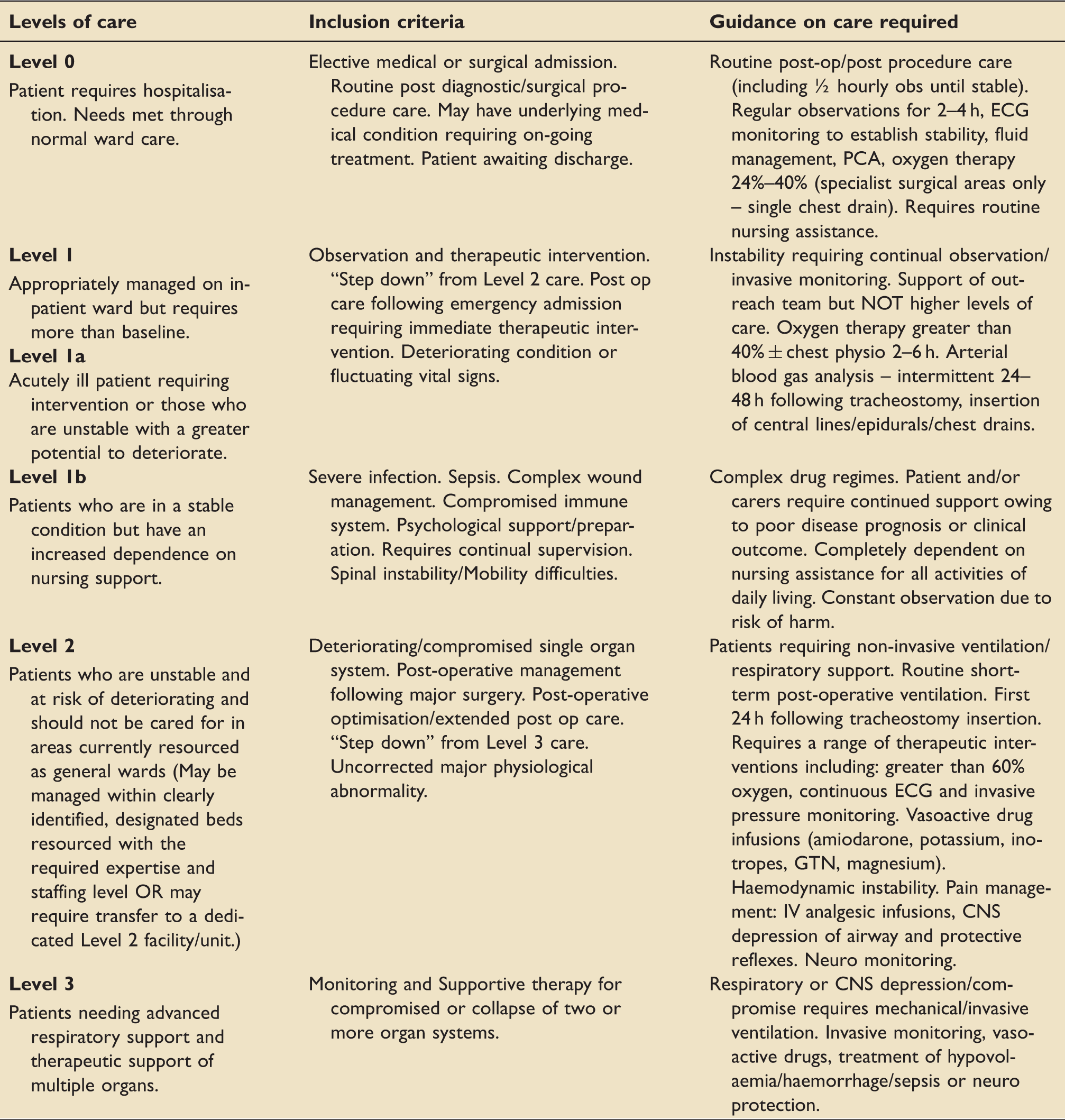
AUKUH dependency tool. 7
Information was sought via discussion with ward staff and review of nursing observation charts and medical notes. For each patient, we calculated MEWS, AUKUH acuity care level and recorded whether the patient was receiving oxygen therapy, had an intravenous cannula or urinary catheter in situ and whether the patient had a “Do Not Attempt Cardiopulmonary Resuscitation” (DNACPR) order in place.
The results and subsequent analysis of this exercise directly informed a decision to expand the Critical Care facility to provide more high dependency (Level 2) capacity. Following this expansion, the exercise was repeated over a second 5-day period in February 2012 (Survey Period 2).
Individual patient data were recorded on an encrypted laptop on a predesigned Microsoft Excel spreadsheet. 12 The data were analysed by MEWS and AUKUH care level separately. In addition, we undertook a comparative analysis to determine if there was any correlation between MEWS and AUKUH that may inform changes to care escalation triggers in the MEWS. We performed a priori sub-group analysis of the Level 2 patients, stratifying by care location (General ward vs. Critical Care). Statistical comparisons were made between study periods using the Mann–Whitney U test, stratified by AUKUH care level. In addition, Chi-squared analysis was undertaken to compare proportions of Level 2 patients managed in and out of Critical Care across the two study periods. Significance was presumed at a confidence level of p < 0.05.
Results
Showing patient acuity by care level during Survey Period 1 and Survey Period 2 (n = 3850).

Values in parentheses are percentage of total for the Survey Period.
Location of Level 2 patients.
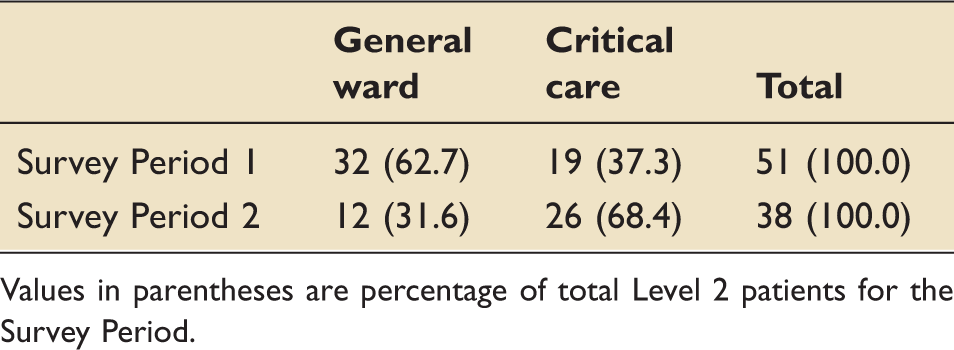
Values in parentheses are percentage of total Level 2 patients for the Survey Period.
AUKUH and MEWS analysis
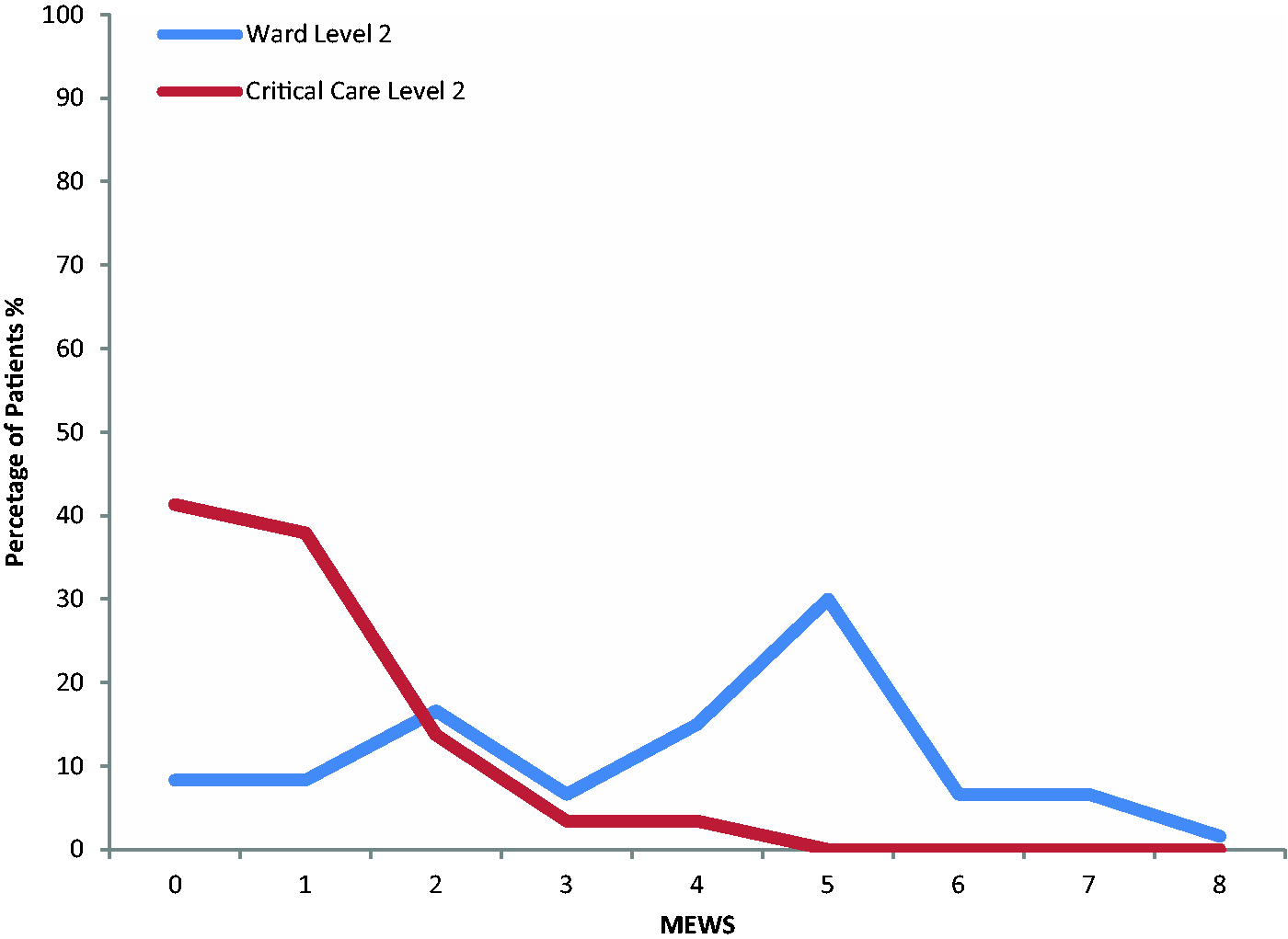
Figure 1 illustrates the range of MEWS within each of the AUKUH groups. Figure 2 demonstrates the sub-group analysis of the relationship between MEWS and AUKUH for Level 2 stratified by care location. Those managed on the ward have a median MEWS of 5 compared with a MEWS of 1 for those managed in Critical Care.
Distribution of MEWS amongst patients stratified by AUKUH care level (n = 3850). Distribution of MEWS for Level 2 patients stratified by care location (n = 89).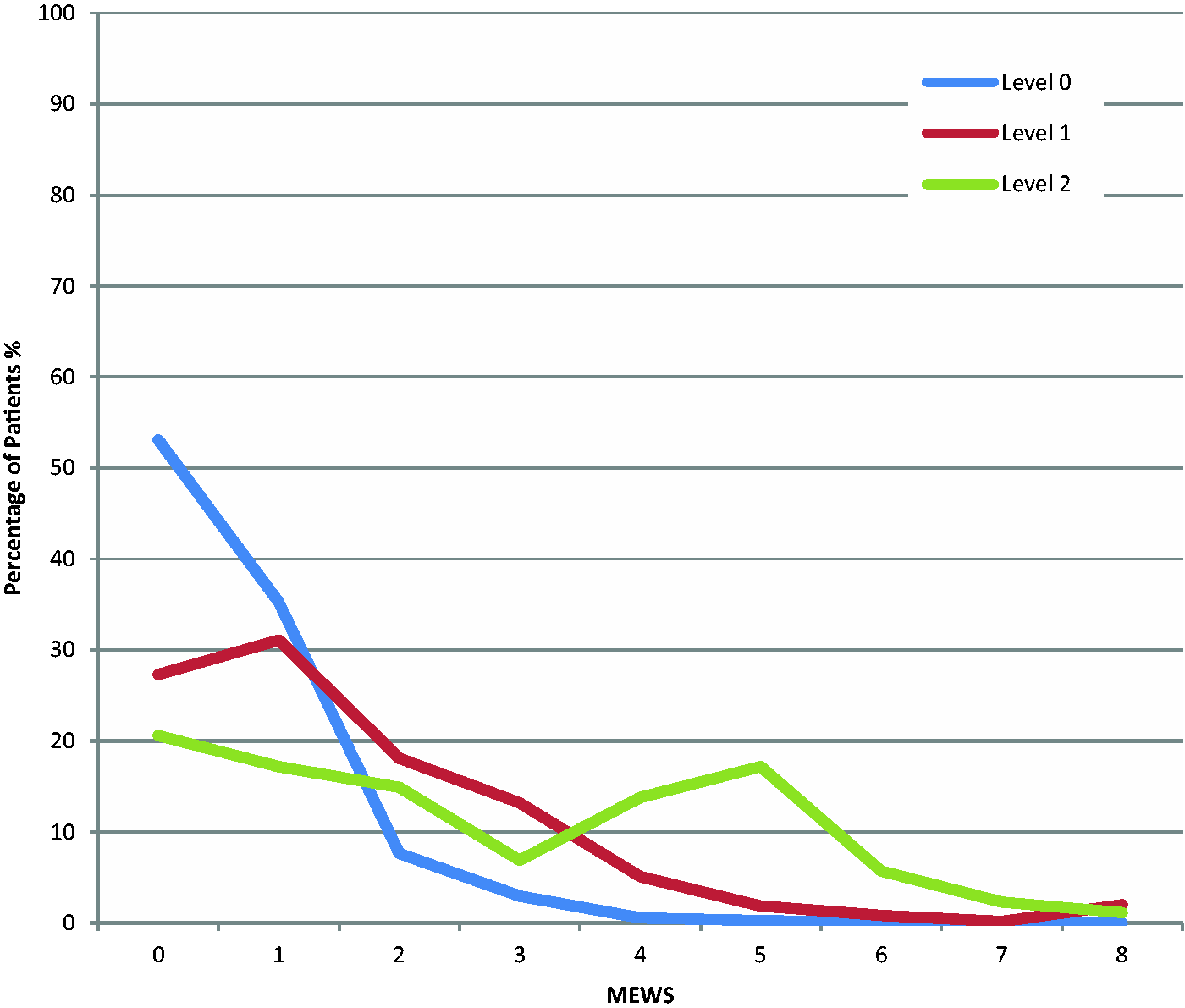
Discussion
We believe that this survey is the first in the United Kingdom to examine the acuity of all inpatients in an acute hospital. The data generated by both surveys confirm that most patients in an NHS acute hospital have low acuity. Of the 3850 patients surveyed, 3335 (86.6%) required Level 0 care. This demonstrates that only one in six inpatients have care requirements that are not met by a standard ward environment. Potentially the MEWS tool may therefore be used to identify those patients who require increased levels of care in an environment appropriate to their illness severity.
In total, 587 patients required Level 1 care (1, 1a or 1b). This increased level of care requirement may suggest a benefit from cohorting patients to maximise benefits of both economy of scale and safety. By concentrating relatively small numbers of appropriate specialist medical and nursing staff in one area, higher levels of support can be delivered with the least economic and logistical burden. These areas should be specialty specific, including both medical and surgical units.
Within the Level 2 population, there is an apparent skew towards a MEWS of 4–5, but equally, a similar proportion of equally acute patients had a MEWS of 0 (Figure 1). Superficially, this tends to suggest that MEWS has a poor sensitivity for high acuity patients although it may have a greater specificity at higher MEWS. However, when ward-based and Critical Care–based Level 2 patients are analysed separately (Figure 2), a much clearer trend emerges towards a MEWS cut-point which could be used as a surrogate marker of those requiring Level 2 care. Those on Critical Care meanwhile may still fulfil the definition of Level 2 care but have normalised physiology and a correspondingly low MEWS, e.g. the non-invasive ventilation patient who has optimised oxygen saturations and respiratory rate albeit with organ support. This post-intervention bias could undermine the potential use of MEWS for triggering care escalation in ward patients; in our opinion, these patients are a different Level 2 population, requiring consideration separate from those within a Critical Care environment when determining acuity assessment methods. Our stratified analysis accounts for this.
We recommend that acuity surveillance undertaken by bed management teams, at least daily, will allow high acuity patients to be identified and transferred to Critical Care immediately. In addition, regular reporting of patient acuity in Critical Care in the same forum, will lead to timely discharge from Critical Care as patients recover, accepting that both level of care and MEWS must be considered jointly to avoid post-intervention bias. This will reduce the likelihood of delayed admission to Critical Care of Level 2 patients and reduce the associated potential harm.
Conclusion
We have demonstrated a relationship in the distribution of patient acuity, using the AUKUH tool and the MEWS using data from 3850 patients. Current care pathways for patients in the MEWS systems recommend escalation, if the MEWS rises above 5. 8 Our data confirm that the patient acuity increases towards Level 1b and 2 when the MEWS increases above this point. We have also demonstrated that those with Level 2 dependencies being managed outside of Critical Care have an increased median MEWS compared with those managed within Critical Care due to the effects of organ support.
We successfully used these data to evidence the requirement for Critical Care expansion in our hospital with a significant reduction in higher dependency patients being managed in a general ward environment. We believe that this methodology can be used both for effective service planning and development as well as to deliver daily improvements in flow of patients to the right care areas and plan to apply this for the benefit of our Level 1 patient population.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.