
Abstract
Oesophageal achalasia is a condition of unknown aetiology that most commonly presents with dysphagia, oesophageal regurgitation or chest pain. A case is described of an 88-year-old lady who presented to the Emergency Department with acute stridor as the initial presentation of oesophageal achalasia. Key steps in management included prompt involvement of an appropriate multi-disciplinary team, control of the compromised airway and early decompression of the mega oesophagus. Our report particularly highlights the diagnostic challenges faced by clinicians dealing with this medical emergency. We recommend that a diagnosis of achalasia should be considered as part of the differential diagnosis in a patient who presents with acute stridor.
Introduction
Oesophageal achalasia is a condition characterised by the loss of normal inhibitory input to the oesophageal myenteric plexus. This results in failure of the lower oesophageal sphincter to relax and aperistalsis to occur. 1
The condition commonly presents between the ages of 30 and 60 years with dysphagia being the primary symptom. 2 Chest pain, regurgitation and weight loss also frequently occur. These symptoms can be insidious, and the condition can exist for years before medical attention is sought. There is a small collection of published case reports of achalasia presenting initially with respiratory distress and stridor, often after eating and particularly in the elderly female population.3–7 Whilst this is an uncommon presentation, the clinical decline can be rapid and life threatening and as such, warrants discussion.
Case history
An 88-year-old female attended the Emergency Department with shortness of breath and a cough, productive of yellow sputum. Examination and investigations were unremarkable. A presumed diagnosis of a community-acquired pneumonia was made and the patient discharged home with oral antibiotics.
The patient was known to have a small hiatus hernia. Her other co-morbidities included recurrent urinary tract infections, osteoporosis, macular degeneration, glaucoma and previous pulmonary tuberculosis in the 1950s. Her previous surgical history included right knee replacement, left neck of femur fracture repair, cholecystectomy and hysterectomy. The patient’s current medications were omeprazole, nitrofurantoin, simvastatin, amitriptyline, tramadol and strontium. She had never smoked and rarely drank alcohol.
The patient presented to the Emergency Department for the second time the following day with severe shortness of breath. Initial examination was unremarkable except for oxygen saturations of 92% on room air. Whilst in the Emergency Department, she developed acute stridor that resolved completely within a few minutes of receiving intravenous hydrocortisone 200 mg and nebulised adrenaline. Following this, a new episode of acute stridor occurred, and, once more, this appeared to rapidly resolve. The patient was able to breathe comfortably with no evidence of airway obstruction or respiratory distress after a few minutes. She was admitted to the Acute Assessment Unit for observation and further investigation.
A chest radiograph (CXR) was performed (Figure 1), and whilst the lung fields themselves were unremarkable, a soft tissue density projecting over the superior mediastinum was noted. On subsequent questioning, the patient described gradually worsening dysphagia to both solids and liquids over the previous three weeks. She denied any other symptoms and had not previously experienced any similar gastrointestinal or respiratory symptoms.
CXR revealing soft tissue density over the superior mediastinum.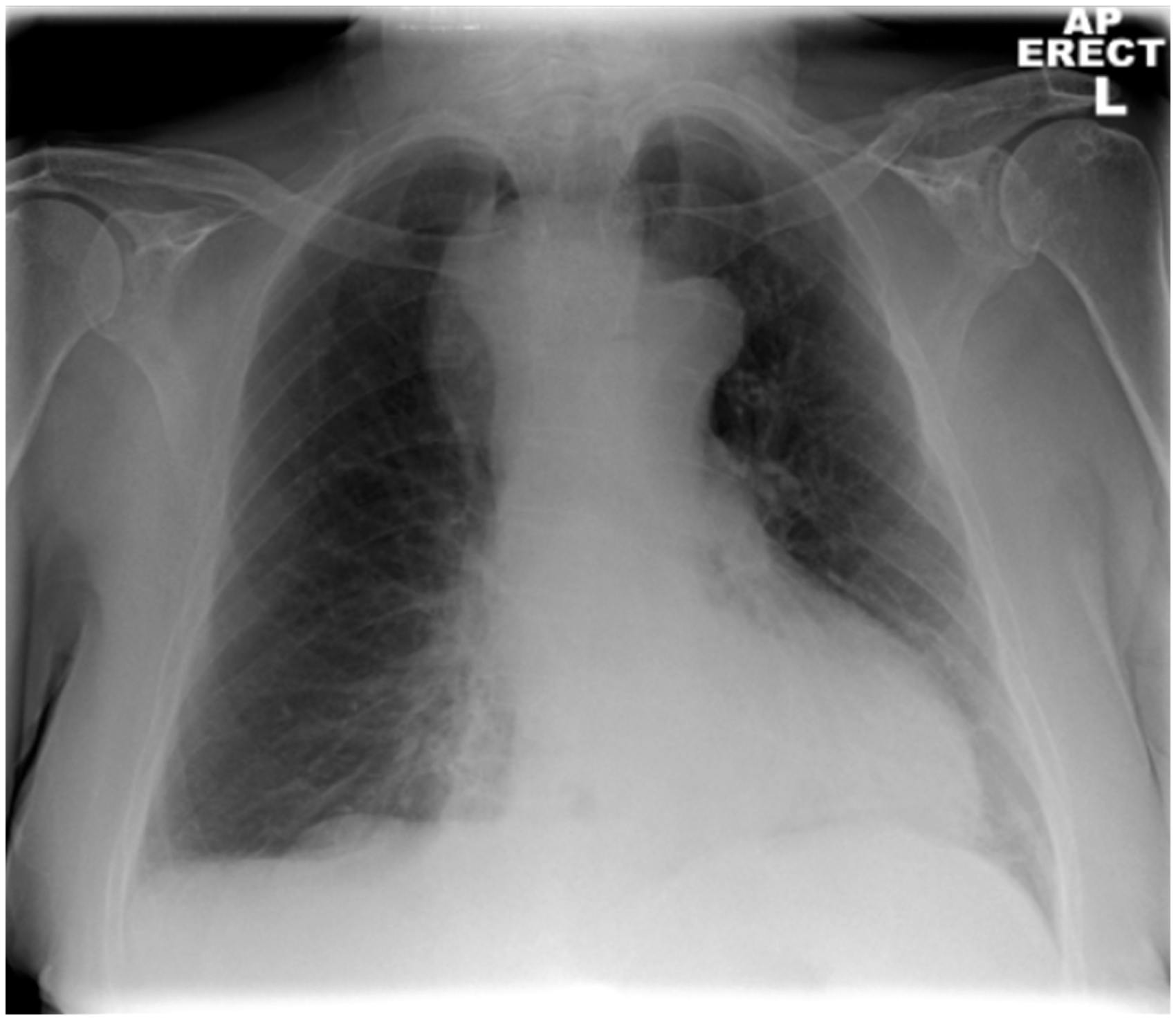
Later that evening, a further prolonged episode of acute stridor occurred. This was associated with a period of desaturation lasting approximately three minutes, with oxygen saturations of 75% on 15 l of oxygen via a non-rebreathing mask. On examination, there were no obvious abnormalities of the airway, neck, chest or abdomen. The stridor appeared to improve slightly with the patient in a semi-recumbent position, and, on this occasion, nebulised adrenaline brought no symptomatic relief. After approximately 20 min, the stridor resolved spontaneously, and the patient was able to breathe comfortably again.
An urgent Ear, Nose and Throat (ENT) opinion was requested, and a flexible nasendoscopy revealed normal appearances of the larynx and vocal cords. The trachea was electively intubated to enable the patient to undergo further urgent investigation. The intubation was straightforward following gas induction of anaesthesia with sevoflurane using standard laryngoscopy. A fibre-optic examination of the trachea through the endotracheal tube was performed, revealing constriction secondary to extrinsic compression distal to the tip of the endotracheal tube. An urgent computerised tomography (CT) scan of the neck and chest demonstrated a thick-walled, tortuous and markedly dilated oesophagus (Figure 2).
CT chest showing a thick-walled, tortuous and dilated oesophagus.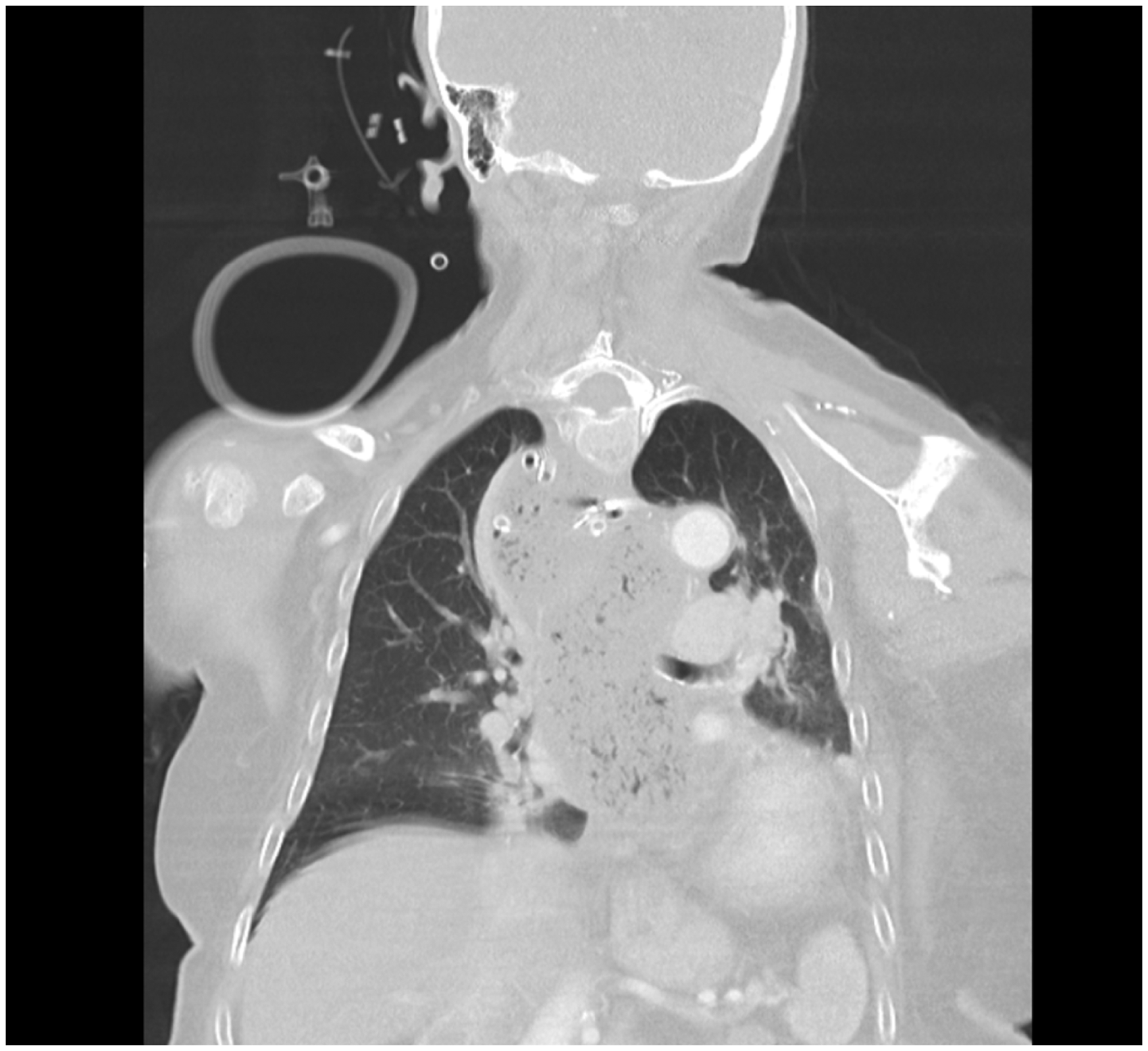
The patient was assessed by the Upper Gastrointestinal (GI) surgical team and underwent an endoscopic assessment of the upper gastrointestinal tract. A grossly dilated oesophagus filled with debris was seen, and candidiasis was noted throughout the tortuous oesophagus. A diagnosis of achalasia was made. A 34-Fr orogastric tube was used with four litres of normal saline to wash out the oesophagus; 100 U of Botox were injected into the lower oesophageal sphincter in four sites.
The patient was woken the following day, and the trachea was successfully extubated. She completed a course of fluconazole, and an oral diet was gradually re-introduced over the next week. The patient was discharged home with outpatient follow-up with the Upper GI team six weeks later.
At this follow-up appointment, the patient denied recurrence of either dysphagia or stridor. However, she has subsequently had two short admissions (less than 48 h duration) to the Acute Assessment Unit with pneumonia. The first of these was at seven weeks, and the second at nine weeks after the initial presentation described above. During the later admission, a repeat CT chest was performed, which demonstrated a markedly dilated oesophagus with food debris seen within it. The patient is currently awaiting outpatient endoscopic evaluation of her upper gastrointestinal tract by the surgical team.
Discussion
Stridor is a high-pitched, harsh sound caused by turbulent gas flow through a narrowed, partially obstructed airway. It can take different forms depending on the site of the narrowing. In general, inspiratory stridor is associated with pathology above the glottis, expiratory stridor with subglottic or intrathoracic pathology, and biphasic stridor can be heard if the pathological cause is at the level of the glottis or below. 8 The more common pathologies causing acute stridor are infection, trauma, foreign body, airway burns, neurological injury and tumour growth. Oesophageal achalasia is rarely included in the differential diagnosis of acute stridor.
A recent literature review of published case reports looked at acute stridor in adult patients who had presented directly from the community to the Emergency Department. 9 The authors found 99 relevant publications with the most common systemic cause for stridor being neurological pathology. The most common local cause was vocal cord abnormality. Significantly, an oesophageal cause was documented in 16 of the 99 case reports. Whilst achalasia is the most frequently reported oesophageal cause of stridor, more unusual oesophageal causes exist. These include oesophageal schwannoma, 10 oesophageal mucocele (presenting post-operatively), 11 nutcracker oesophagus 12 and oesophageal foreign body. 13
Oesophageal achalasia is a condition caused by failure of the lower oesophageal sphincter to relax. An inflammatory process causing the loss of inhibitory ganglia cells of the myenteric plexus is a consistent pathological finding in achalasia cases, and the aetiology of this process remains largely unknown. 14 There is no definitive treatment for the condition, and the management is by symptom control. This can be achieved pharmacologically, surgically or by endoscopic intervention. 15
Stridor and respiratory distress in patients with achalasia is thought to be as a result of extreme oesophageal distension causing compression of the trachea against the sternum. 3 This usually occurs after a meal and deterioration can be rapid. Two hypotheses exist as to the mechanism involved. One is the cephalad movement of the dilated oesophagus behind the upper oesophageal sphincter muscle where it becomes wedged causing a one-way valve effect, with air able to enter the oesophagus, but not leave it. The second is upper oesophageal sphincter dysfunction where air is trapped with swallowing but unable to escape due to extreme sphincter contraction and loss of normal belch reflex. 4 Failure of upper oesophageal sphincter relaxation during increased intra-oesophageal pressures (the belch reflex) has been consistently found to occur in achalasia patients; however, in a study of manometric findings of 50 achalasia patients against 45 controls, no other changes in upper oesophageal sphincter tone were found. 5
In patients who present with acute stridor, prompt assessment and stabilisation must first occur. The airway should be assessed as safe before investigations are performed. This may require gaining a definitive airway, usually in the form of endotracheal intubation. The decision to intubate should be made by an anaesthetist as complicated laryngoscopy is anticipated in the acutely stridulous patient. Involvement of the ENT surgical team may be appropriate where time allows. A fine nasendoscopy, if tolerated without distress, may provide valuable information about the aetiology of airway obstruction and the likelihood of straightforward intubation. Once a definitive airway has been obtained, radiology provides invaluable diagnostic benefit. CXR often reveals a large and dilated oesophagus. These findings can be confirmed by CT scan, which may also reveal the presence of food in the oesophagus. CT scanning should always be considered where suspicion of oesophageal perforation exists. In a non-emergency presentation where the patient is stable, barium swallow may reveal a tortuous and dilated oesophagus with a ‘birds beak’ appearance at the gastro-oesophageal junction. Oesophageal manometry confirms aperistalsis. 5
Suspicion of achalasia will warrant discussion with the gastroenterology team to discuss the treatment options. Emergency management is by decompression of the mega-oesophagus by an oesophageal tube or rigid oesophagoscopy to release the trapped air. The successful use of glyceryl trinitrate (GTN) to relax oesophageal sphincter tone has been documented. 6 In that case report, sublingual GTN was administered to cause the lower oesophageal sphincter to relax with almost immediate relief of symptoms, allowing food to enter the stomach relieving the compression on the trachea.
One case report of stridor secondary to achalasia noted fine nasendoscopy findings of an inflamed glottis in addition to the compression of the glottic region by the dilated oesophagus. 2 This was attributed to chronic reflux caused by achalasia. This patient had undergone previous cricopharyngeal myotomy, which may have contributed to enhanced reflux and glottic inflammation. In this case, the patient’s symptoms resolved with the use of intravenous steroids.
More definitive management includes balloon dilatation, botox injection, Heller’s myotomy, cricopharyngeal myotomy and oesophagectomy for which surgical opinion will be sought. 3 Where abnormal tissue is found, then a biopsy should be performed and the sample sent to pathology for tissue diagnosis.
Reported emergency presentations of achalasia with stridor often include common features such as the occurrence symptoms after a meal and the presence of a palpable, non-pulsatile neck mass. 5 The patient may offer a history of recent worsening dysphagia and weight loss. The case we have reported lacked many of these features. The multiple episodes of stridor observed were unrelated to food intake and appeared most often to resolve spontaneously and unpredictably. There was an inconsistent response to administered medications, such as nebulised adrenaline. On one occasion, symptomatic relief was observed when the patient was placed in a semi-recumbent position. The presence of a neck lump was not found. Further questioning did elicit a recent history of progressive dysphagia though no history of weight loss was offered. This report highlights the diagnostic challenge to clinicians who are dealing with this medical emergency, as the presentation can be highly non-specific. A high index of suspicion should be maintained in any patient who presents with, otherwise unexplained, acute stridor. The clinician should be especially mindful if the patient is from the elderly female population.
In conclusion, although the occurrence is seemingly rare, oesophageal achalasia can present initially with acute airway obstruction and should be considered as part of the differential diagnosis in the acutely stridulous patient. Early management of the compromised airway is critical, along with timely decompression of the mega-oesophagus. The management of this patient requires a true multidisciplinary approach.
Key points in the acute management of this patient.
Initial ABC assessment and involvement of key specialties Early strategy for definitive airway management Imaging to aid diagnosis – likely CT chest Urgent decompression of the mega-oesophagus Treatment of achalasia to achieve symptom control Effective communication and teamwork across specialties
Key members of a multi-specialty approach.
Emergency medicine Anaesthetics and Intensive Care Radiology Ear, Nose and Throat surgery Gastroenterology Upper GI surgery Pathology Dietetics
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Patient consent
The report is published with the written consent of the patient.