
Abstract
Fairy Liquid® is a detergent used daily throughout the United Kingdom. Currently, Toxbase suggests ingestion only causes nausea, vomiting and diarrhoea; however, we report a patient who developed multi-organ failure following a large ingestion and subsequent aspiration of Fairy Liquid.
Case report
We present the case of a 36-year-old male, with a background of alcohol excess and depression, who presented to the Emergency Department (ED) having been found at home with reduced consciousness. An ambulance was dispatched and on arrival in the ED his Glasgow coma score was 14 (Motor 6, Verbal 4, Eyes 4). He had been incontinent and an arterial blood gas on arrival showed a lactate of 8 mmol/L raising the suspicion of seizure activity.
Whilst in the department it was noted that he was regurgitating foam from his mouth and further questioning revealed passing similar foam per rectum. At this point it was noted by the staff that there was a ‘citrus aroma’ to both. The patient was requesting large volumes of water to drink. Within a couple of hours, and with numerous glasses of water, the oral foaming increased to such a degree that our patient began to aspirate due to the sheer volume of foam produced. At this point he was sedated and the trachea intubated to prevent further aspiration.
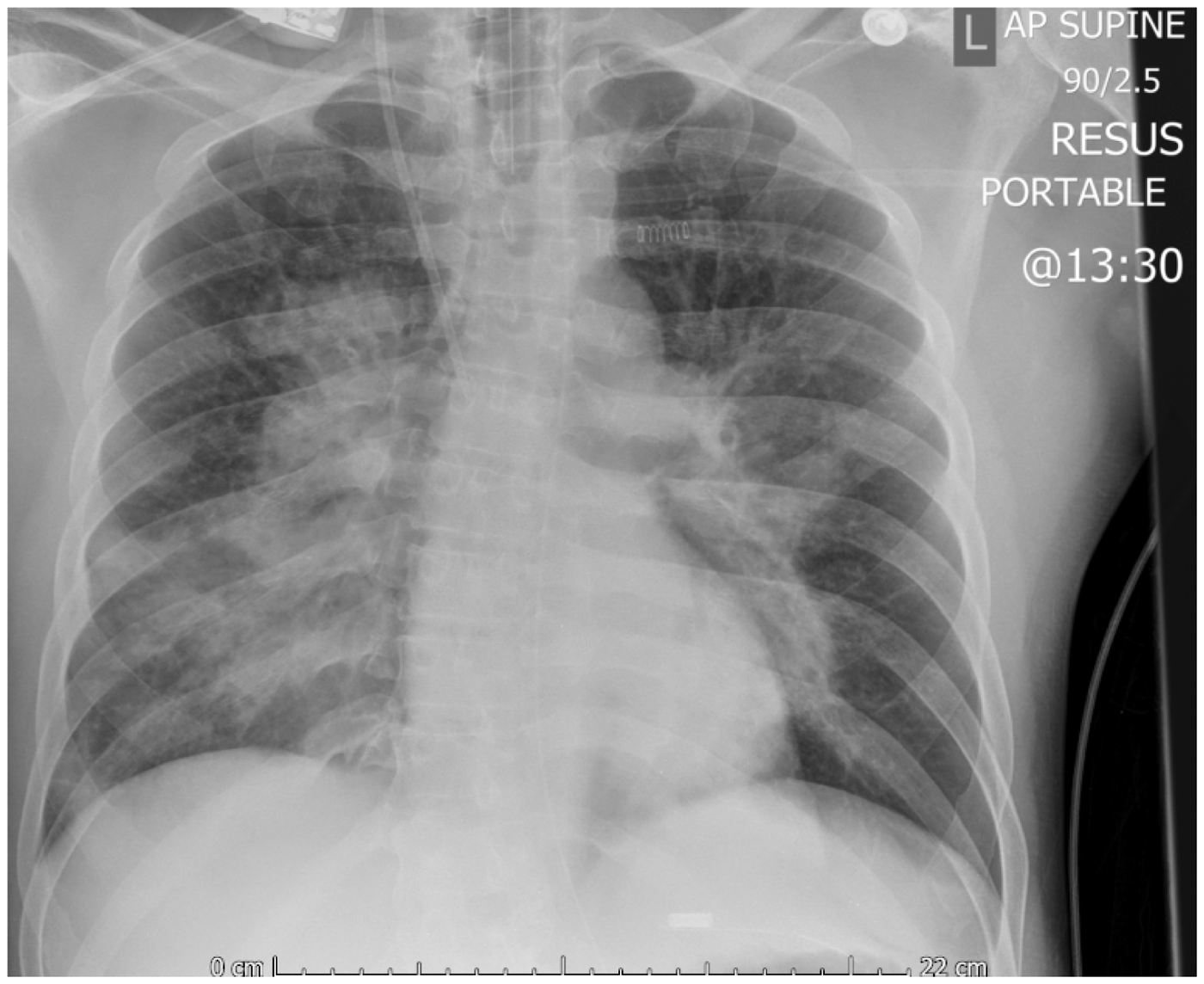
A collateral history was sought from his family which revealed the identification of around 700 ml Fairy Liquid® (pomegranate and citrus flavour) missing from a bottle found under the patient’s bed. No other substance was identified as missing by the family and paracetamol and salicylate levels were both normal. Whilst initial chest radiograph (Figure 1) was unremarkable, a repeat just 4 h later (Figure 2) reported extensive peri-hilar consolidation in both lung fields most likely due to non-cardiogenic pulmonary oedema due to aspiration. The patient was transferred to the intensive care unit (ICU) where his oxygenation became problematic requiring an inspired oxygen concentration of 100% and airway pressure release ventilation (APRV). Over the next 12 h he became cardiovascularly unstable requiring noradrenaline, adrenaline and vasopressin infusions to maintain an adequate perfusion. At this point he had an adequate urine output for his body weight; however, he developed a mixed acidosis requiring initiation of continuous veno-venous haemodiafiltration (CVVHDF).
Initial chest radiograph. Chest radiograph 3 h after the initial radiograph.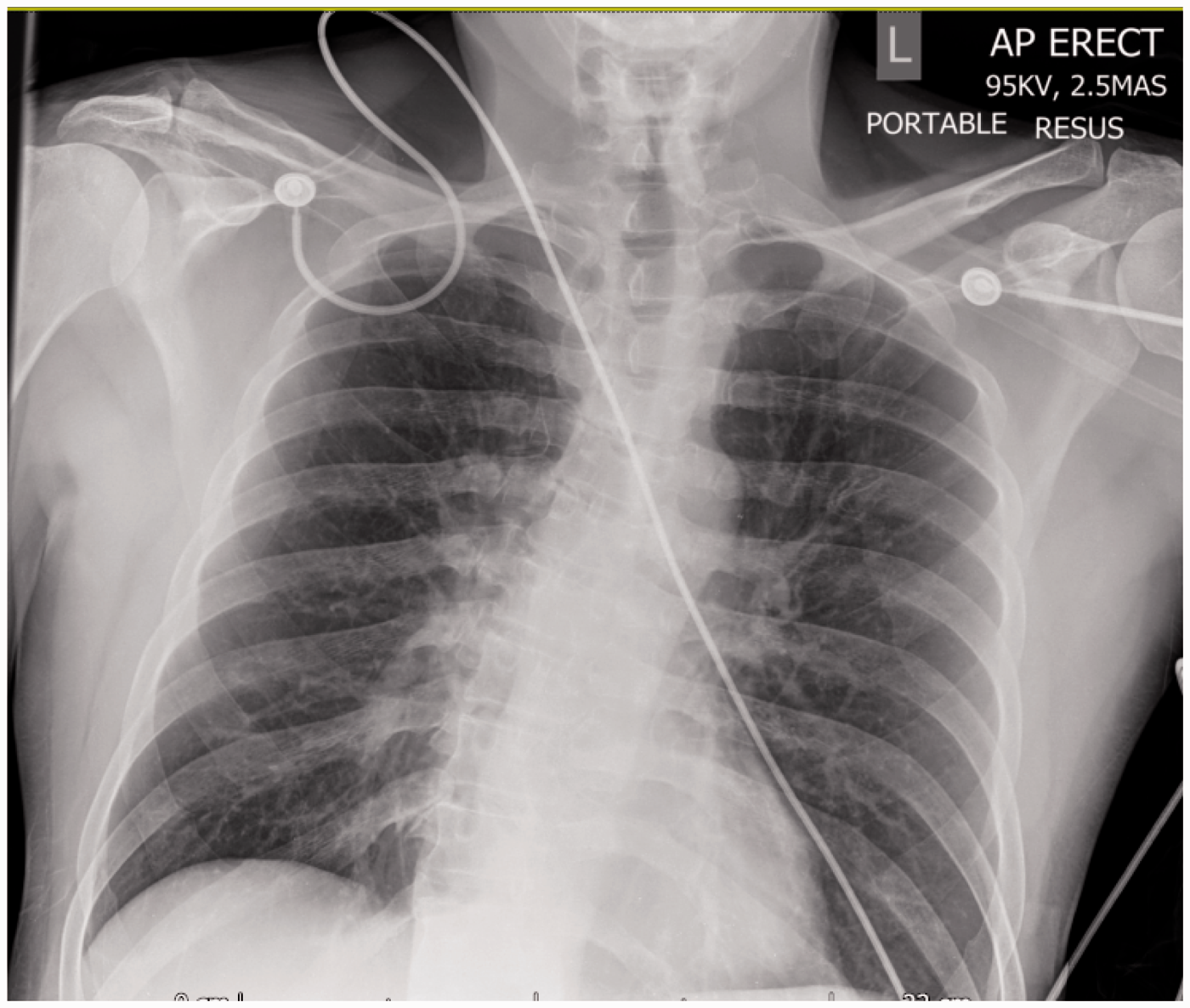
Over the following five days both his ventilatory and cardiovascular support improved markedly and on day six the vasopressor support was stopped. He developed an ongoing ventilator requirement and had a tracheostomy inserted. Following successful weaning from the ventilator the tracheostomy was removed and the patient discharged. His renal function had returned to normal on discharge although had required two weeks of CVVHDF.
Discussion
Bates reports that a detergent is any substance that reduces the surface tension of water; they are also known as surface-active agents or surfactants.1,2 They are commonly found around homes in many forms, including washing-up liquids, to remove fat-based compounds from eating apparatus. Detergents can be classified into three groups: anionic, non-ionic and cationic with the latter being the most toxic. 2 Whilst the detergent properties of such compounds are well known to medical personnel, the effects of aspiration in our patient were potentially surprising.
Type two pneumocytes in the lungs produce pulmonary surfactant (di-palmitoylphosphatidylcholine) to decrease surface tension and therefore the work of breathing. The absence of surfactant has recognised complications in premature babies causing respiratory distress syndrome. It would stand logically therefore that aspiration of exogenous detergent could decrease the work of breathing, the opposite of what our patient experienced.
We suggest that the cause for our patient’s rapid respiratory deterioration is due to chemical pneumonitis and the development of non-cardiogenic pulmonary oedema. Alternative or additional pathology could have been due to co-aspiration of the acidic stomach contents. Mendelson’s syndrome (aspiration of stomach contents) is said to develop with aspiration of as little as 25 ml of stomach contents or aspiration of fluid with a pH of less than two and a half.
Bates' advice following ingestion of anionic and non-ionic detergents is to drink a glass of water or milk. 2 With a large volume of detergent ingested, the situation with regard to aspiration deteriorated significantly when our patient consumed water. It would make sense that the water, when mixed with stomach contents increases the volume of foam produced. We question the rationale of this suggestion and propose that it might make more sense to suggest consumption of a highly fat-based fluid (for example vegetable oil) which, when mixed with the water of stomach secretions and detergent will emulsify and prevent foam production.
Consultation with Toxbase suggested that low volume ingestion of Fairy Liquid causes no ill effects; however, if a large volume is ingested nausea, vomiting and diarrhoea will result. 1 This is something well documented in the literature, Farber et al. 3 reported after ingestion of surfactant containing products, gastrointestinal symptoms occurred in nearly half of all patients. Whilst our patient did not report nausea or vomiting he did suffer diarrhoea.
Mercurius-Taylor et al. 4 showed that detergents have a potent effect on cell membranes. At low concentrations they form complexes with brush border enzymes and at high concentrations solubilize membranes by forming micelles with the lipid protein components. They chronically exposed rats to low doses of Fairy Liquid and found that whilst the stomach was unaffected, the small intestine showed significant decrease in the size and number of villi, some being necrotic. Large intestine mucosa also showed glandular atrophy. Both large and small bowel changes were irreversible after 12 weeks. Whilst our patient, to our knowledge, has not been exposed chronically to Fairy Liquid, the high concentration he consumed could explain the diarrhoea he experienced.
Conclusion
Our case report appears to be the first published case where a volume of washing-up detergent has been ingested, causing severe respiratory and multi-organ failure.
Information currently available suggests this is a non-toxic detergent; however, in light of our case report we feel this should be re-evaluated.
It would also make sense to attempt ingestion of a fat-based fluid to aid in emulsification of the detergent thereby decreasing the risk of aspiration.
Footnotes
Acknowledgement
The author thanks Dr. N. Hollister for his assistance in editing this report.
Consent
Written consent for publication of this report has been received from the patient.
Declaration of Conflicting Interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.