
Abstract
Objective
To find, critically appraise and synthesise all published studies so as to determine the safety and spectrum of use of noninvasive positive pressure ventilation for acute respiratory failure following oesophagectomy.
Design
Systematic review.
Methods
The MEDLINE and EMBASE databases were searched and the quality of the studies and any bias or confounding were rated according to established protocols. Outcomes extracted included re-intubation, anastomotic leakage, length of intensive care unit stay and mortality. The data were analysed quantitatively and qualitatively. Pooling of outcomes was considered if appropriate.
Results
The search identified four papers, demonstrating the understudying/underreporting of the topic. Three were case-series and one was a conference abstract. The overall methodological quality was low. Design-specific biases and confounding were high. Despite this, the included studies conclude that noninvasive positive pressure ventilation is safe and effective and that re-intubation rates, intensive care unit length of stay, mortality and anastomotic dehiscence is lower when it is used. Meta-analysis was deemed to be inappropriate.
Conclusions
Despite the conclusions and consensus of the included studies, there is no evidence to definitively conclude that noninvasive positive pressure ventilation is either safe or dangerous following oesophagectomy and the current literary evidence is inadequate. Current practice varies and is based on opinion and consensus. As such, randomised controlled studies are urgently required as current practice may cause undue harm to patients. The incidence of anastomotic leakage with noninvasive positive pressure ventilation use needs to be determined.
Introduction
Oesophageal cancer is a devastating illness and the ninth most common cancer in the UK with 8000 new diagnoses annually. 1 The prognosis following diagnosis is poor with 30% one-year and 8% five-year survival rates in the UK. The incidence rises with age, and chief risk factors include reflux disease, smoking, ethanol consumption and obesity. 2 Oesophagectomy is a widely accepted surgical procedure, by either open or minimally invasive means, to eradicate and treat cancer of the oesophagus. Newer, minimally invasive techniques have opened this procedure up to previously unsuitable candidates and as the number of patients with other complex co-morbidities increases, the likelihood of a post-operative critical care stay increases. 3
Once used solely for chronic hypo-ventilatory disorders and subsequently for acute hypercapnic respiratory failure, 4 noninvasive positive pressure ventilation (NPPV) is an essential tool in the armory of the physician in the increasingly complex and diverse critical care environment. 5 One such evolving application is the treatment of post-operative acute respiratory failure (ARF) in surgical patients.6–12 The use of NPPV in the post-operative course has remained a controversial topic.13,14 The mechanism of post-operative ARF is multifactorial and includes sedation, pain, atelectasis and diaphragm dysfunction.9,15 Post-operative ARF is usually transient in nature and resolves with adequate supportive care. For many years, the accepted management would be tracheal intubation and invasive ventilation; however, this has been implicated in the development of pulmonary complications.16–19 NPPV can often prevent tracheal intubation and treat post-operative ARF. 20 NPPV has also been demonstrated to be more cost-effective, when compared to invasive ventilation, in the intensive care unit (ICU) setting for treating hypoxic respiratory failure.21,22
Following oesophagectomy, both ARF and anastomotic leak are common and are associated with grave outcomes.23–25 Unsurprisingly, impairment of oxygen delivery is associated with anastomotic breakdown and as such, respiratory failure is usually treated aggressively in these patients with endotracheal intubation. Currently, the British Thoracic Society classifies upper gastrointestinal anastomotic surgery as a contraindication to NPPV. 26
There is much uncertainty regarding the balance between benefit and risk in these patients when choosing NPPV to avoid invasive ventilation. 27 There are case reports of NPPV causing upper gastrointestinal perforation and loss of integrity of oesophageal sutures.28,29 As such, it is important to weigh up the potential risks of anastomotic breakdown induced by pressure, versus the benefits of avoiding invasive ventilation and the risks of long-term respiratory complications, whilst maintaining oxygenation to prevent anastomotic breakdown from ischaemia. No high-quality systematic review has been performed to date to answer this question. We aim to extract, describe, appraise and synthesise current work in this area and aspire to detail guidance for clinicians’ practice and areas where further research is necessary.
Materials and methods
Study identification
All studies published up until 1 October 2014 that examined patients who had received NPPV in the immediate post-operative period following oesophagectomy were sought for evaluation. Studies were identified using a comprehensive text word and MeSH-based electronic search of MEDLINE and EMBASE including the terms “Respiratory failure”, “Resp$ ADJ3 fail$”, “non-invasive ADJ5 ventilation”, “esophagectomy”, and “esophageal anastomosis”. A Google™ search was also performed using the terms “non-invasive ventilation” and “oesophagectomy”. Additionally, the bibliographies of relevant articles were hand-searched for additional material according to established protocols. 30
Study selection
Inclusion criteria were all types of primary research that reported post-operative data such as mode of ventilation and morbidity/mortality for patients who had an oesophagectomy for oesophageal cancer. Exclusion criteria were studies that report exclusively on other parts of the gastrointestinal tract, case reports, review articles, studies on children or animals or studies that examined invasive ventilation alone.
Data extraction and synthesis
MC, TL and SF independently extracted the data using a data extraction tool. Where possible, a risk ratio for outcomes such as anastomotic breakdown, length of stay, the rate of re-intubation and mortality was calculated with a 95% confidence interval (CI). These were considered for pooling in a meta-analysis.
Assessment of study quality and bias
MC, TL and SF independently assessed all articles that met the inclusion criteria. There is no gold-standard validated method for assessing bias and the quality of observational studies30,31 but there is consensus that the three most fundamental domains are (1) appropriate selection of participants, (2) appropriate measurement of variables, and (3) appropriate control of confounding, as well as considering design-specific biases. We therefore discuss these quality criteria for each study in a narrative fashion.
Results
Search strategy
Search strategy and results from searching the EMBASE and MEDLINE databases.
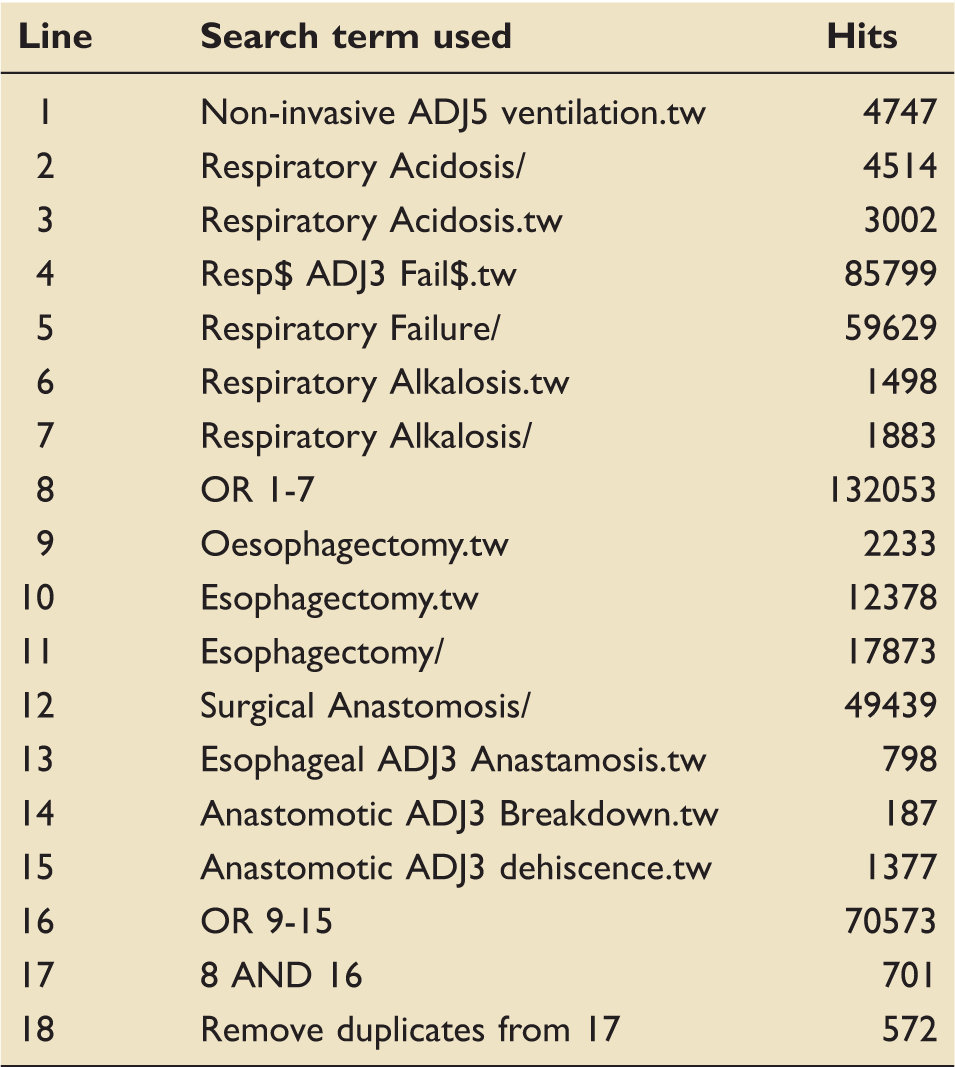
Subsequently, the title and abstracts of all articles were searched by hand. A total of 60 articles were identified for detailed analysis. Additionally, two extra article(s) were retrieved through a Google™ search and hand searching of bibliographies. These 62 full-text articles were examined and 58 studies were excluded (references available on request). Exclusions were as a result of:
No mention of ventilation characteristics (n = 37) No mention of NPPV (n = 10) No post-operative oesophagectomy data (n = 6) Review articles (n = 4) Letter to the editor (n = 1) Case report (n = 1)
Four articles were included for analysis.8,32–34 A PRISMA flow diagram
35
for the above process is provided in Figure 1.
PRISMA flow diagram demonstrating how the final four articles were elucidated.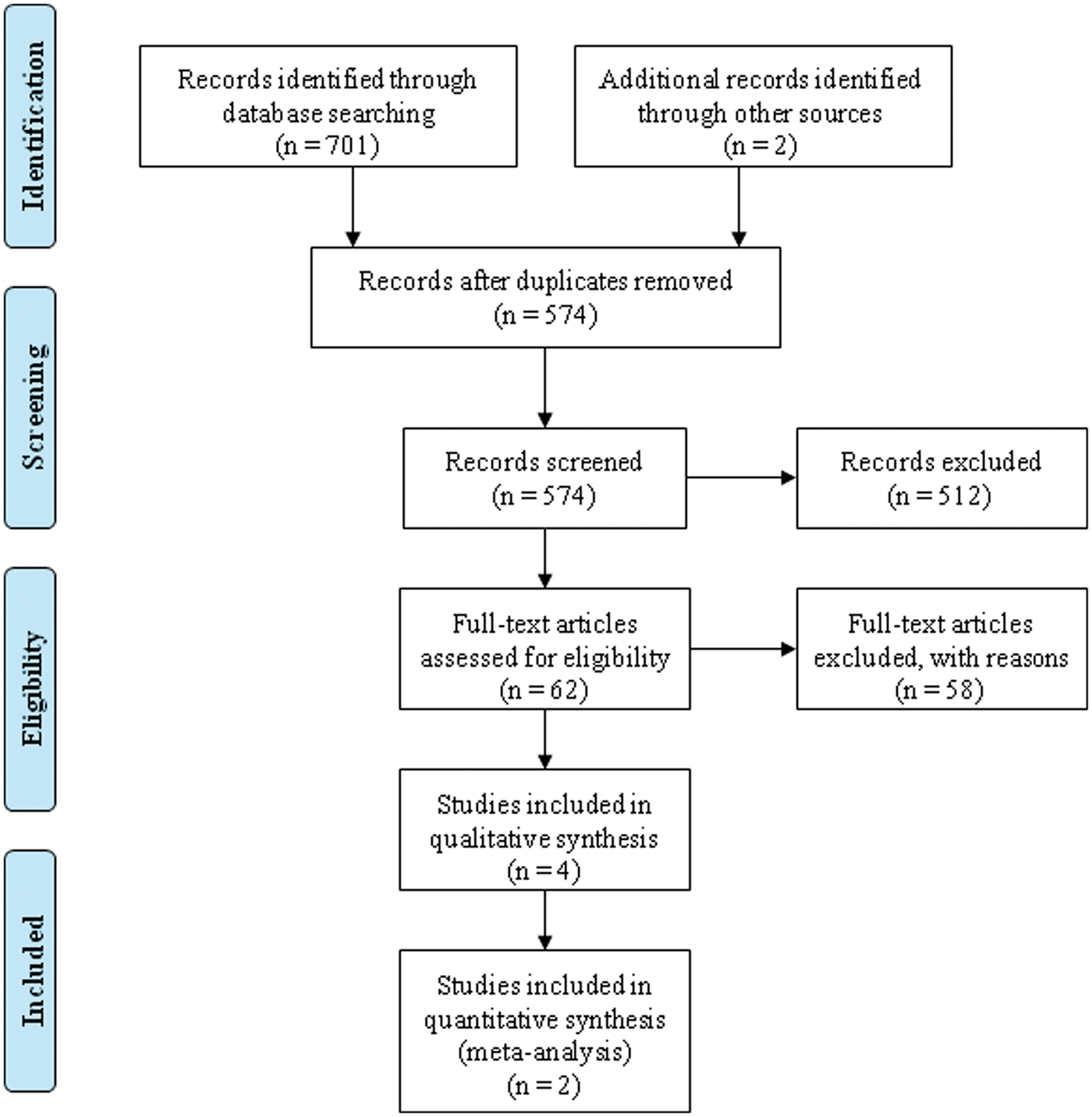
Overview of included studies
Data extraction tool summarising the key data from included studies.
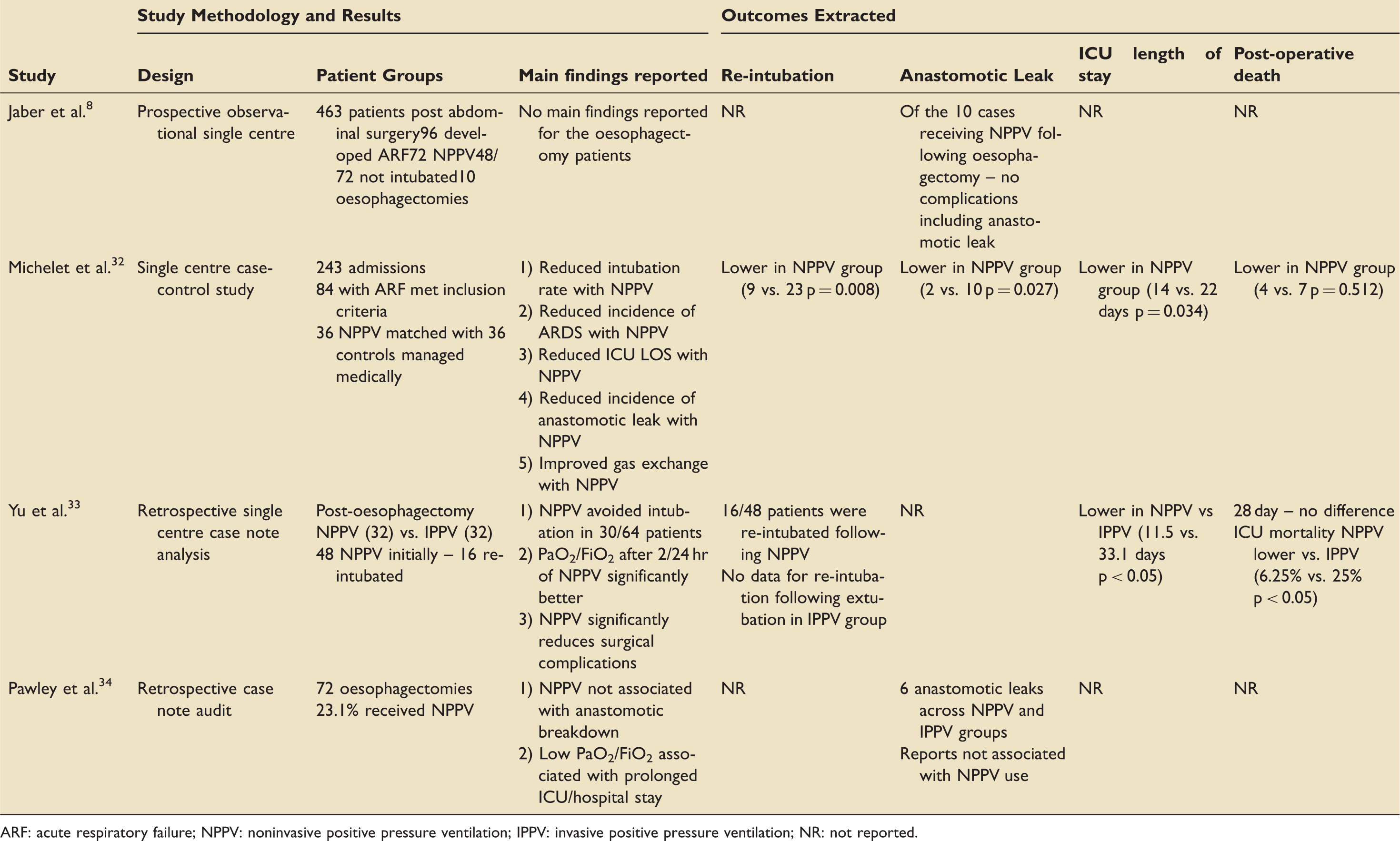
ARF: acute respiratory failure; NPPV: noninvasive positive pressure ventilation; IPPV: invasive positive pressure ventilation; NR: not reported.
Jaber et al. 8 in their 2005 publication report the outcomes of patients admitted to ICU for post-operative care following abdominal surgery where NPPV was used. The design is a single-centre prospective observational study. The quality of the methodology was rated as low and the risk of bias and confounding was rated as high. The most significant problem with using this study to answer our question is that of the 72 patients who were treated with NPPV for post-operative ARF; only 10 were following oesophagectomy. There is no comparison between the types of operation or those who were invasively ventilated vs. those who received NPPV. They report no incidence of anastomotic leakage in these patients; however, this finding alone in so few patients cannot allow conclusions to be drawn. No other outcomes of interest were reported.
Michelet et al. 32 in their 2009 paper report the results of a single-centre case–control study investigating the role of NPPV following oesophagectomy. This is the most cited of the included studies. The design is a case–control study; however, when the study is scrutinised, it cannot be classified as a true case–control study. Two case-series are selected from different time periods. The cohorts from 2003 to 2006 are labeled as controls (no NPPV) and those from 2006 to 2009 are labelled as cases as they received NPPV. A true case–control study would usually start at the ‘case’, such as, for example, anastomotic leakage, and then look back in time for the exposure, such as NPPV. Selecting two historically distinct cohorts of patients introduces other problems such as improvements in care over time. As such, the quality of the methodology was rated as low and the risk of bias and confounding was rated as high. Data are provided for all outcomes as demonstrated in Table 2. These outcomes demonstrated a favorable effect of NPPV and the paper concludes that NPPV is safe for use following oesophagectomy for post-operative ARF. Overall, the design, methodology and small number of included patients make this conclusion difficult to accept and challengeable.
Yu et al. 33 in their 2013 paper evaluate the use of NPPV for acute respiratory distress syndrome (ARDS) following oesophagectomy. The design of the study is a retrospective single-centre analysis of case notes. The quality of the methodology was rated as very low and the risk of bias and confounding was rated as high. The main problem with the design and methodology is that it is both retrospective and based on a treatment algorithm that prescribes either NPPV or invasive ventilation for post-operative ARF. How rigidly was this algorithm followed? The study reports the rate of re-intubation in NPPV patients but not those that are invasively ventilated. Other outcomes reported are ICU LOS, 28-day mortality and ICU mortality. ICU length of stay and mortality were lower in the NPPV group. Another setback is that the study reports post-operative ARDS and not ARF. These are two distinct pathologies but there is no mention of ARF as opposed to ARDS. The authors conclude that the use of NPPV following oesophagectomy is an effective option but they have not tackled the issue of anastomotic leakage satisfactorily; the design and methodology make it difficult to accept this conclusion.
Pawley et al. 34 in their 2014 conference proceeding abstract report a retrospective case note audit from a large UK teaching hospital. They use the notes of 72 patients who have received an oesophagectomy and were admitted to intensive care. Baseline demographical data, length of ICU/hospital stays and anastomotic leak rate were reported. Of the 72 patients, 23% received NPPV. It is reported that NPPV was not associated with anastomotic breakdown in these patients. Data for outcomes such as re-intubation rate, ICU LOS and post-operative death in patients receiving NPPV were not reported. Unfortunately, the nature of the data, in a short abstract, does not lend itself towards more detailed analysis. It is not possible to comment on the methodological quality but the study will be prone to the same bias and confounding issues as the other included studies. An attempt to contact the authors and request more of their data was unsuccessful.
Meta-analysis of reported outcomes
Outcomes were set as re-intubation, anastomotic leak incidence, ICU LOS and ICU mortality.
Re-intubation – Two papers32,33 reported data for re-intubation rate. It was decided that there was insufficient data from one paper
33
as it does not report re-intubation rate in one group. Therefore, it was not possible to formulate an odds ratio for rate of re-intubation when NPPV is used as opposed to conventional treatment for ARF following oesophagectomy. Anastomotic leak incidence – Three papers reported data for the incidence of anastomotic leak.8,32,34 Only one paper
32
reported anastomotic leak incidence for each group so there were insufficient data to formulate an odds ratio for anastomotic leak incidence when NPPV is used as opposed to conventional treatment for ARF following oesophagectomy. ICU LOS – Two papers reported ICU LOS for NPPV vs. conventional medical treatment.32,33 Only one paper reported the standard deviation of the ICU LOS;
32
therefore we could not combine these results. Attempts were made to contact the authors for the standard deviations but these were unsuccessful. ICU mortality – Two papers report ICU mortality and a meta-analysis was possible.32,33 Due to the methodological problems described, it was decided that a meta-analysis for this outcome would not be appropriate as the conclusions from its calculation would be difficult to interpret.
Discussion
The aim of this study was to find, critically appraise, synthesise and draw conclusions from all available published literature regarding the controversial topic of using NPPV following oesophagectomy for post-operative ARF as opposed to invasive mechanical ventilation. Current practice appears to be based on consensus and opinion and there is often a different viewpoint taken between anaesthetists and surgeons. We included four studies using a search strategy of high sensitivity and low specificity. This demonstrates that this topic has been understudied, underreported and/or underappreciated.
The main issue with any primary study that aims to answer this question is of bias and confounding. Investigators may have already made their mind up about the question before setting out to answer it. Randomisation is difficult as some patients may simply be too sick for NPPV. When comparing two groups, the sicker of the two groups will be those who are invasively ventilated. How is anastomotic leakage diagnosed? Do we go looking for it or does it come looking for us? When anastomotic leakage presents, is it the fault of the surgeon, the anaesthetist, neither or both. How many studies that add to the overall picture and help answer the question have not been published? Indeed, all included studies are prone to one or more of these design-specific biases.
Of the four papers identified, three are primary studies and one is a conference proceeding abstract. The three primary studies have significant methodological flaws in addition to the confounding and biases described. Despite this, they suggest and strongly claim that NPPV is beneficial and safe when used for post-operative ARF following oesophagectomy. The overall suggestion that anastomotic leakage incidence is lower when NPPV is used is difficult to defend. The major clinical hazard of NPPV in these patients is anastomotic dehiscence induced by pressure distension. Currently, the evidence for this hazard is limited to case reports and theory.28,29 More has to be done to answer this important and sensible clinical question regarding anastomotic leakage. The difficulty is that the complications from anastomotic leakage in these patients are severe and unforgiving.
We were only able to combine data from two studies for one outcome, ICU mortality.32,33 It was not possible to extract and pool any other outcomes from other included studies. It was decided that to pool these outcomes together would be unwise, as the result would be difficult to interpret.
Overall, there is a distinct lack of evidence. This finding makes it difficult for the clinician to judge whether to use NPPV or invasive ventilation when faced with the dynamic and time-pressured scenario of a patient acutely deteriorating with respiratory failure following oesophagectomy. Despite this, there is sufficient evidence that NPPV has a growing role in post-operative ARF. 36 It could be argued, however, that avoiding the use of NPPV without any evidence of danger could be exposing patients to the risks of invasive ventilation. Despite the lack of evidence to suggest NPPV being dangerous following oesophagectomy, many centres would not use it as a first-line against post-operative ARF as likewise, there is no evidence to suggest safety.
There has been much debate in the literature regarding this topic and yet the question remains, in part, unanswered. Currently, practice is based around opinion, consensus, individual experience and local policy. Potentially, patients will be at risk, as the best practice is not established. A prospective study, ideally a large multi-centre randomised controlled trial would give the answer. Additionally, a large prospective cohort study could be employed, but it would have to be very large and via a national registry or similar. A well-designed case–control study that uses cases of anastomotic leak and controls with no leak following oesophagectomy could be commissioned. The centre would have to be somewhere that already uses NPPV and a lot of data would be needed to control for the confounding of sicker patients being invasively ventilated. Finally, it would be useful to build up a database of patients receiving NPPV following oesophagectomy and attempt to determine the anastomotic leak rate. If the rate is as low as has been previously reported, this could alleviate the fear of NPPV in these patients and lead to better outcomes.
Footnotes
Acknowledgements
The authors acknowledge the Department of Critical Care Medicine at Bradford Royal Infirmary, Bradford, UK.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.