
Abstract
Mortality rates alone are no longer a sufficient guide to quality of care. Due to medical advances, patients are surviving for longer following critical illness and major surgery; therefore, functional outcomes and long-term quality of life are of increasing consequence. Post-operative cognitive dysfunction has been acknowledged as a complication following anaesthesia for many years, and interest in persistent cognitive dysfunction following a critical illness is growing. Psychological and neurocognitive sequelae following discharge from intensive care are acknowledged to occur with sufficient significance to have recently coined the term ‘the post-intensive care syndrome’. Rehabilitation following critical illness has been highlighted as an important goal in recently published national UK guidelines, including the need to focus on both physical and non-physical recovery. Neuropsychological and cognitive consequences following anaesthesia and critical illness are significant. The exact pathophysiological mechanisms linking delirium, cognitive dysfunction and neuropsychological symptoms following critical illness are not fully elucidated but have been studied elsewhere and are outside the scope of this article. There is limited evidence as yet for specific peri-operative preventative strategies, but early management and rehabilitation strategies following intensive care discharge are now emerging. This article aims to summarise the issues and appraise current options for management, including both neuroprotective and neurorehabilitative strategies in intensive care.
Keywords
Over the last decade, there has been an increase in the complexity of patients presenting to intensive care, due in part to the severity of co-morbidities at presentation and an increasingly elderly population. Despite this, mortality rates are improving; the long-term consequences of critical illness are thus becoming ever more relevant. The risk factors and pathogenesis of delirium and post-cognitive dysfunction have been reviewed thoroughly elsewhere. This article summarises the relevant findings in these areas and deliberately focuses on the psychological and neurocognitive sequelae following critical illness including depression, anxiety, post-traumatic stress disorder and cognitive dysfunction; reviewing the evidence for incidence, pathophysiology and management.
Psychological and neurocognitive consequences of critical illness
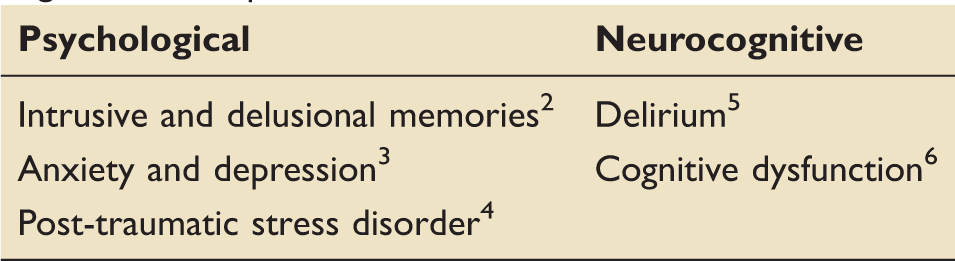
The neuropsychological sequelae that occur following a critical care admission are numerous and can be highly distressing for patients and their families. Symptoms that occur include intrusive memories, delusions, delirium, panic episodes and nightmares. Conditions such as depression, anxiety, post-traumatic stress disorder (PTSD) and cognitive dysfunction are increasingly recognised among patients who survive an intensive care admission and are described collectively as the ‘post-intensive care syndrome’. These conditions have a significant impact on the patient’s long-term quality of life. 1
Summary of the common psychological and neurocognitive consequences of a critical care admission.
Summary of the risk factors for psychological and neurocognitive outcomes following critical care admission.
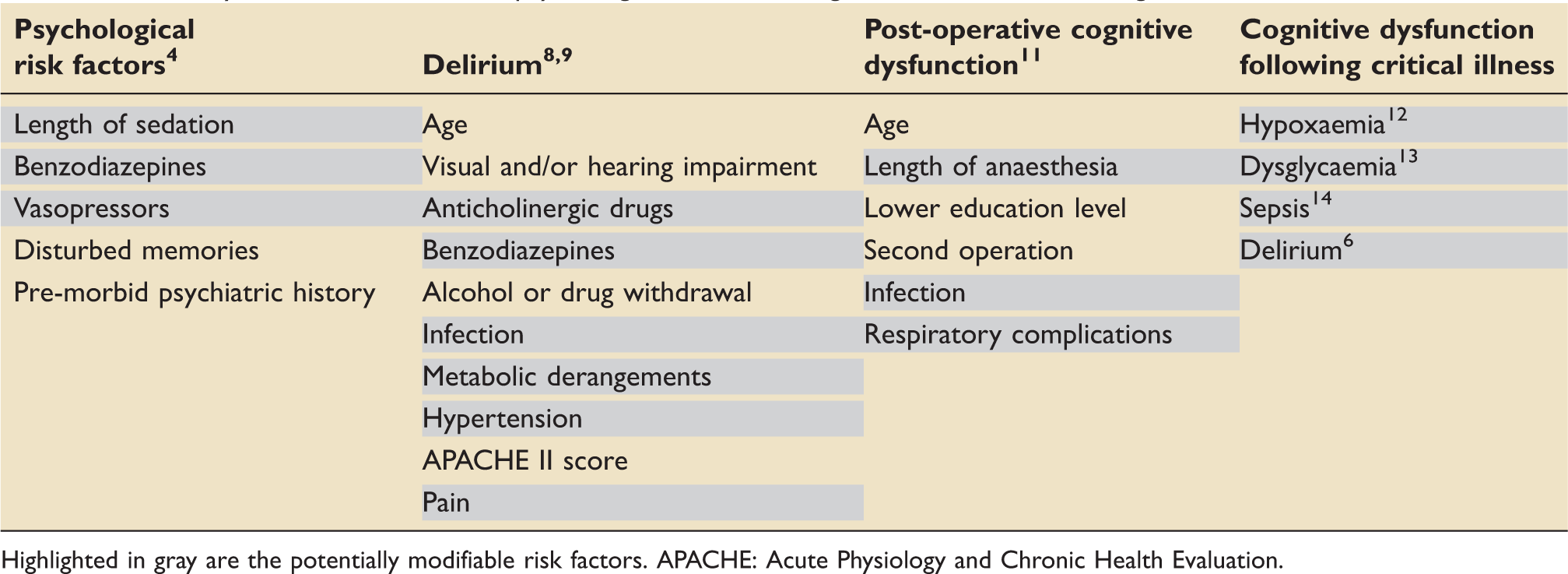
Highlighted in gray are the potentially modifiable risk factors. APACHE: Acute Physiology and Chronic Health Evaluation.
Pathogenesis
The pathogenesis of delirium, cognitive dysfunction and psychological sequelae following critical illness is not fully understood, though considered to be multi-factorial in nature.
The leading theories for the pathogenesis of delirium and cognitive dysfunction following anaesthesia and critical illness include those of neurotoxic, neuromodulatory and neuroinflammatory mechanisms. 17 There is mounting evidence revealing anaesthetics to be powerful modulators of neuronal development and function, both in the young developing, and aging brain. 18 Many factors, including medications, disturbed sleep, hypoxia and dysglycaemia, may alter neurotransmitter synthesis, function and availability and could result in psychological manifestations during critical illness, or present as delirium.18,19 It is increasingly understood that the immune system and inflammatory mediators have a key role in the formation of memory, and consequently that their dysregulation has a role in the pathogenesis of cognitive dysfunction. 20 Neuroinflammation is precipitated by systemic inflammatory insults like sepsis and acute respiratory distress syndrome (ARDS), 21 with increased production of cytokines and reactive oxygen species activating microglia and leading to synaptic and neuronal disruption.22,23 Some researchers present the argument that disturbed sleep on the ICU, associated with the effects of acute illness, sedative medications and environmental factors, can also influence these neural pathways, and as well as delirium and cognitive dysfunction, may also lead to psychological symptoms.24,25
Preventative and neurorehabilitative strategies
Summary of the psychological and neurocognitive management options available for critically ill patients.
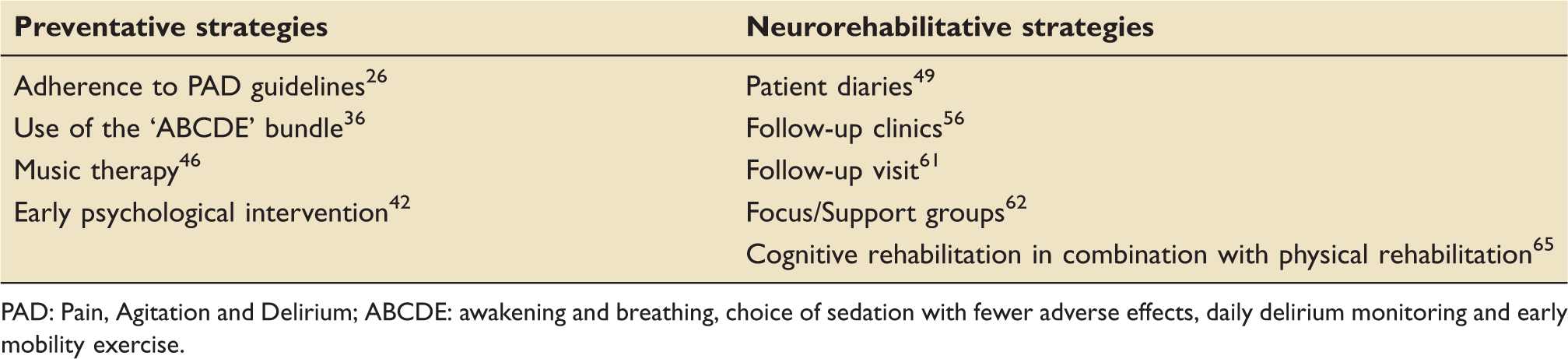
PAD: Pain, Agitation and Delirium; ABCDE: awakening and breathing, choice of sedation with fewer adverse effects, daily delirium monitoring and early mobility exercise.
Preventative strategies
Current strategies towards psychological and cognitive neuroprotection on the intensive care focus mainly on the detection, treatment and management of delirium using conservative approaches to control the environment, ‘treating the cause’ and managing agitation. However, preventative strategies focus on modification of daily intensive care management that might have a direct effect on patient long-term neurocognitive outcomes.
There are potentially modifiable risk factors for the prevention of post-intensive care syndrome (Table 2). The American College of Critical Care Medicine and the Society of Critical Care Medicine recently developed evidence-based guidelines to aid clinicians in the assessment and management of Pain, Agitation and Delirium (PAD guidelines) on ICU. 26 They recommend regular pain, sedation and delirium assessments and advocate treating pain symptoms in the first instance. Sedation guidelines advocate minimal use of sedation, using either a sedative interruption strategy (i.e. spontaneous awakening trial) or a targeted sedation strategy (continuous light levels of sedation). It has been recommended that non-benzodiazepines drugs (e.g. propofol or dexmedetomidine) are used for sedation where possible, as meta-analysis has demonstrated them to be associated with reduced length of mechanical ventilation and intensive care length of stay. 27 Dexmedetomidine has also been shown to reduce the prevalence of delirium following cardiac surgery, 28 to improve early cognition scores in sedated brain injured and non-brain injured patients as measured by the Johns Hopkins Adapted Cognitive Exam (ACE) 29 and to reduce the prevalence of delirium in comparison with benzodiazepines.30,31 However, the majority of recommended management strategies to prevent delirium are non pharmacological, such as early and progressive mobilisation, sleep hygiene and environmental control measures; no specific recommendations for first line pharmaceutical options have been made as evidence is lacking or contradictory as to the relative safety and efficacy of different antipsychotics such as haloperidol.32,33
Landmark studies in the prevention of delirium include the Awakening and Breathing Controlled Trial, 34 and work from Schweickert et al. 35 which demonstrated the benefit of early mobilisation leading to better independent functional status and a shorter duration of mechanical ventilation and delirium. These studies led to the development of the ‘ABCDE’ bundle to reduce delirium (awakening and breathing, choice of sedation with fewer adverse effects, daily delirium monitoring and early mobility exercise 36 ); a strategy which can be combined effectively in conjunction with the PAD guidelines described above. The use of statins on ICU has been shown to reduce the incidence of delirium.37,38 The use of bispectral index (BIS) has been demonstrated to reduce anaesthetic exposure, incidence of delirium and likelihood of POCD in the context of anaesthesia and surgery,39–41 and therefore may have a role in intensive care in monitoring the depth of sedation and preventing cognitive dysfunction.
There is relatively little literature published regarding direct psychological intervention on intensive care. However, at least one study has shown that early psychological intervention for conscious patients, delivered by trained clinical psychologists and nurses significantly reduced the percentage of patients who required psychiatric medications at 12 months and the likelihood of PTSD. These psychological interventions consist of stress management approaches, such as cognitive and emotional restructuring, counselling and psychological support, educational interventions and coping strategies. 42 Nursing care can also have a positive effect on psychological well-being. Facilitating communication, explaining care and rationalising interventions, ensuring patients are oriented to time and place, reassuring patients about transfer and providing patients with information about critical care before admission are all practices that have a beneficial effect. 43
Music therapy is another psychological technique often employed as an early intervention to reduce anxiety and sedation levels on the intensive care. Music is involved in specific brain functions such as memory and emotion and has been seen to bring about a state of relaxation, improve temper and increase motivation. 44 From a biological perspective, it can decrease peripheral levels of catecholamines. 44 A recent randomised control trial has demonstrated reduction in levels of anxiety and sedation requirements in mechanically ventilated patients who had self-directed music via headphones whilst on the ICU. 45 However, interestingly there was no difference in levels of anxiety or sedation between the self-directed music listening group compared with a self-directed noise block-out group, 45 which may indicate a role for control perception in reduction in anxiety. Another interesting study looked at the use of music therapy to assist with respiratory weaning from a ventilator, significant differences were found in heart and respiratory rates between the onset and offset of music therapy sessions. This indicated a reduction in anxiety, although no difference was seen in reduction in days to wean between the study and control groups. 46
Neurorehabilitative strategies
Neurorehabilitative strategies explored in the literature are mainly based on activities to assist the patient to overcome their psychological trauma, vulnerability and regain their independency after their critical illness. Neurorehabilitative strategies to re-establish cognitive function are not being fully developed yet. Neurocognitive strategies currently described in the literature focus mainly on patient diaries, patient follow-up and cognitive rehabilitation.
Patient diaries
One of the explanations for emotional problems following discharge from intensive care is that many patients have little factual memory of their experiences and instead have the presence of delusional memories or ‘odd perceptual experiences’. It may be that patient diaries can help to explain or fill these memory gaps. 47
The use of patient diaries is varied both internationally and nationally, although they are generally viewed as a record of events kept by the nursing staff or family on behalf of the patient, to be voluntarily read after recovery. Diary use is not yet considered routine practice, with the majority of reported usage being within Scandinavian countries 48 and the UK. 49 The literature published to date tends to be positive towards their use; however, there remain questions as to the primary objectives, methodological considerations and efficacy. Some of the methodological concerns are that there is no consistency in the emphasis on medical-based information versus social or environmental information provided, the number of entries made, or the timing and support at the time of diary provision. Experts comment that although the use of patients diaries may be very beneficial, improper use or implementation of these diaries could potentially result in poorer psychological outcome and that further directed randomised controlled trials are required prior to their implementation in routine clinical practice. 49
A recent qualitative study on the use of patient diaries reported mixed emotional feelings following their use. They were generally seen as a way of gaining a sense of reality, feeling cared for, and connecting with loved ones. However, feelings such as shock and fear were also experienced. Despite the negative emotions evoked, all patients felt they would recommend the use of a diary to other patients and families on intensive care.50,51 Previous research has supported the use of patient diaries to ‘help to construct an illness narrative’ and also reported having benefits for friends and relatives. 52 Using focus groups these researchers also highlighted that pictures were an important part of the diary, that patients wanted to know how they behaved and what they said, that the family should be able to write entries, and that the optimal timing for the diary handover varies between patients. 53 Patient diaries have been shown to reduce PTSD symptoms 52 and improve quality of life. 54
Patient follow-up
Formal intensive care follow-up is now recommended in UK guidelines 55 ; however, recent reviews demonstrate a wide variability in follow-up practice.56,57
In the UK, of those ICUs that offered a service, the organisational structure varied between operating principally as a referral service to involving a multidisciplinary team. 56 The inclusion criteria ranged from an intensive care stay of 48 h to five days; with time to follow-up varying from prior to hospital discharge to 12 weeks post-discharge, and the number of follow-up clinics ranging from 1 to at least 3. Attendance rates varied between 30% and 67% for mixed High Dependency Unit (HDU)/ICU clinics; cancellation and non-attendance rates varied from 10–16% and 5–31%, respectively. 56 One interesting feature was that the majority of clinics was nurse-led. 56 Although referral to other services was not well reported in this study, in a previous survey of UK practice 51% of ICU follow-up clinics reported not having direct access to other services. 58 Similar variability was reported in Scandinavia. 57
A recent qualitative analysis following interviews of 34 former ICU patients from all around the UK demonstrated that patients generally valued some form of ICU follow-up; feeling that the follow-up had an important impact on physical, emotional and psychological recovery in terms of continuity of care, receiving information, gaining expert reassurance and giving feedback to ICU staff. Information about physical, emotional and psychological recovery was particularly important to patients, as was information that helped them make sense of their ICU experience. Those without access to ICU follow-up care often felt abandoned or disappointed because they had no opportunity to be monitored, referred or to get more information. Some patients, however, found that their healthcare needs were unmet because hospitals were unable to provide the specific aftercare they required. 59
A multicentre randomised control trial in the UK investigated the cost-effectiveness of a nurse-led follow-up clinic combined with a self-motivated self-help physical rehabilitation programme. 60 They found that a programme that included a three-month, six-month and 12-month follow-up sessions had no significant effect on improved quality of life as measured by SF36 self-assessment questionnaires, and therefore that it was not cost-effective to offer this type of followup and rehabilitation. 60 Interestingly, however, it was demonstrated that intensive care consultant input was required in half of all follow-up visits, specialist (including psychology) referrals were made in one-third of the patients and three quarters of patients took up the offer to visit the ICU following discharge, indicating that patients were experiencing ongoing problems. 60 The positive effect of visiting ICU after discharge has been previously demonstrated in a qualitative study that interviewed patients who revisited the ICU; patients expressed value in the experience, allowing them to express gratitude, finding it helpful in learning what had happened during their illness and also to suggest improvements. 61 One centre in the UK found an additional benefit from a patient focused ‘drop-in’ forum for patients and relatives to share their experiences in addition to a formal ICU follow-up process. 62
Cognitive rehabilitation
Due to growing evidence of the presence of cognitive dysfunction following discharge from intensive care following a critical illness, specific cognitive rehabilitative therapies are becoming increasingly relevant. Cognitive rehabilitation focuses on improving memory and executive function but is also a functional process that enables an individual to cope within their own environment by mediating awareness, and utilising internal and external aids for compensation strategies.3,63,64 Cognitive rehabilitation is still a growing field but, encouragingly, in relation to cognitive dysfunction following TBI or stroke, there is sufficient robust evidence to make practice standard recommendations for therapy. 64 Of relevance to future strategies for cognitive rehabilitation following discharge from intensive care are specific research questions: Which patients will benefit, when should cognitive rehabilitation begin and what interventions are effective for intensive care patients?1,23,63
Much of the current literature is focused on the combination of physical exercise and cognitive rehabilitation. Evidence indicates that exercise has beneficial effects on cognition, 65 and that cognitive impairment predicts poor outcome from physical rehabilitation. 66 Therefore, several randomised controlled trials of the combined use of physical and cognitive rehabilitation strategies have been initiated to evaluate their utility in improving cognitive, physical and functional outcomes following discharge from intensive care. The RETURN study found a significant improvement in cognitive function following a 12-week programme of rehabilitation compared with the ‘usual care’ package of sporadic rehabilitation, 65 whereas the Activity and Cognitive Therapy (ACT) in the ICU trial demonstrated the feasibility of providing combined cognitive and physical rehabilitation for mechanically ventilated patients whilst on the ICU. 67 Interestingly, physical rehabilitation has also been shown to improve psychological symptoms following discharge from the ICU. 68
Unfortunately, however, despite on-going research, a recent systematic review has failed to demonstrate the cost-effectiveness of rehabilitation interventions following intensive care discharge. 68 This may be due to the fact that rehabilitative strategies to manage the post-intensive care syndrome are neither understood nor well defined; hence, timing of delivery for such a strategy is yet to be defined. The most positive effects were seen for ICU-diary interventions in reducing the incidence of PTSD. 69 The authors conclude that more directed interventions and further research are needed before definitive conclusions can be drawn.53,70
The future
Mindfulness meditation is a technique that has been used in other specialities to assist with reducing anxiety, stress and depression, improving coping strategies, reducing mental fatigue, with an overall aim to improve cognitive function and overall quality of life. Similar techniques could be used during and following the ICU admission, with both patients and families. This hypothesis has been assessed in a recent randomised control trial investigating mental fatigue following TBI and stroke. Authors found that there was a significant improvement in mental fatigue, anxiety and depression self-assessment scores and word fluency and information processing speed following an 8-week programme using a mindfulness-based stress reduction (MBSR) approach. 69 Potential mechanisms are thought to be mediated by structural changes in the left prefrontal cortex and associated with changes in emotion regulation that can impact on cognition, emotion and behaviour. 71
Conclusion
Current research indicates a significant incidence of long-term cognitive dysfunction and psychological sequelae that impact on long-term function and quality of life in both younger and older patients discharged from critical care. Exact pathophysiological mechanisms are not yet elucidated but are likely to be associated with neuroinflammation and disruption of neurotransmitter function; suggesting pharmaceutical targets may be available in the future. In addition, cognitive and physical rehabilitation strategies appear to improve outcomes, although the cost-effectiveness remains to be proven. Clinical research needs to concentrate on preventative interventions, combined with effective long-term follow-up and rehabilitation of patients, to improve the long-term psychological and neurocognitive outcomes following critical illness.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.