
Abstract
Translational research in critically ill human patients presents many methodological challenges. Diagnostic uncertainty, coupled with poorly defined comorbidities, make the identification of a suitable control population for case–control investigations an arguably insurmountable challenge. Healthy volunteer experiments using endotoxin infusion as an inflammatory model are methodologically robust, but fail to replicate the onset of, and diverse therapeutic interventions associated with, sepsis/trauma. Animal models are also limited by many of these issues. Major elective surgery addresses many of these shortfalls and offers a key model for exploring the human biology underlying the sepsis syndrome. Surgery triggers highly conserved features of the human inflammatory response that are common to both tissue damage and infection. Surgical patients sustain a predictable and relatively high incidence of sepsis, particularly within the ‘higher risk’ group. The collection of preoperative samples enables each patient to act as their own control. Thus, the surgical model offers unique and elegant experimental design features that provide an important translational bridge between the basic biological understanding afforded by animal laboratory models and the de novo presentation of human sepsis.
Introduction
In comparison to major acute medical pathologies, the comparative dearth of novel therapeutic agents, persistently high morbidity and significant mortality that characterise sepsis syndrome is striking.1–5 A lack of suitable human models that afford a methodologically robust control population for mechanistic studies may explain this lack of progress. Mechanistic research in patients with established sepsis has failed to overcome several key methodological limitations. Eliminating confounding factors from case–control study design in established sepsis is challenging, if not impossible. Age, 6 gender,7,8 ethnicity 9 and comorbidity10,11 all profoundly alter normal physiological function. Therapeutic agents commonly used to treat sepsis, including antibiotics,12,13 sedatives 14 and steroids, 15 all exert off-target immunologic and metabolic effects. These factors alter multi-organ function and therefore confound the biological and clinical interpretation of experimental readouts being attributed to sepsis syndrome per se. However, the default control population for critical illness studies using case–control methodology has typically been healthy volunteers. By contrast, elucidating mechanisms through cohort studies where a population is followed until a disease occurs is clearly more methodologically robust, because samples are taken from study participants prior to the onset of organ dysfunction. In order to be economically viable and relevant research, the cohort must have a predictably high incidence of sepsis and be comparable to the septic population of interest. This article sets out the case for major surgery fulfilling these criteria, and highlights recent data demonstrating the superior suitability of this model being adopted.
Diagnostic uncertainty confounds the study of sepsis syndrome
The definitions of sepsis and criteria for diagnosis of infection used by major clinical trials published between October 2013 and October 2014.
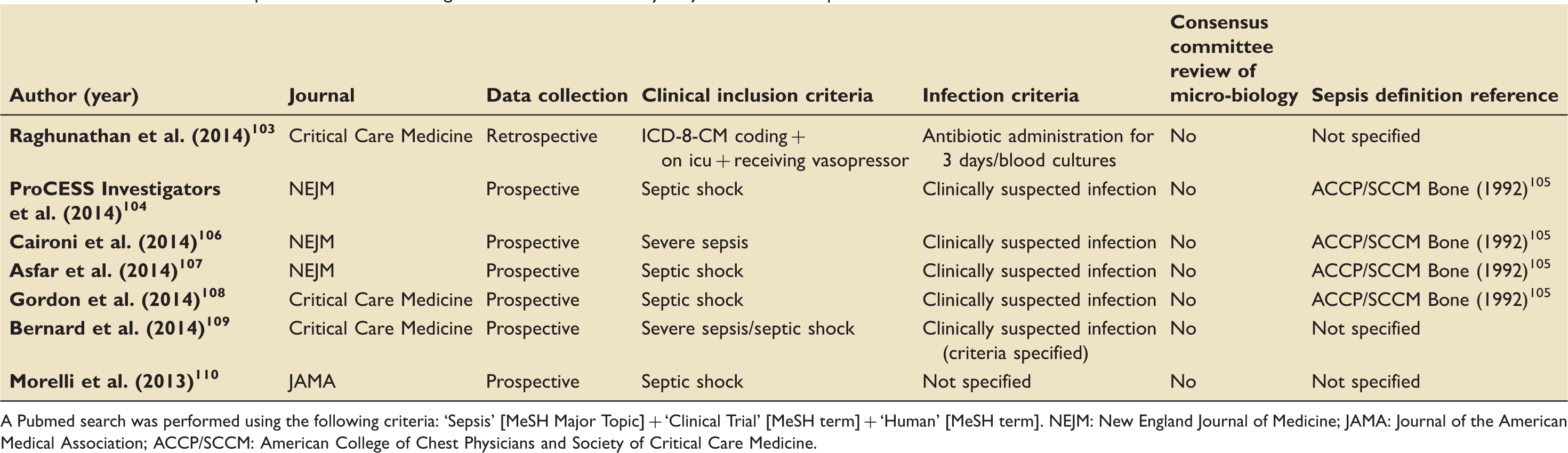
A Pubmed search was performed using the following criteria: ‘Sepsis’ [MeSH Major Topic] + ‘Clinical Trial’ [MeSH term] + ‘Human’ [MeSH term]. NEJM: New England Journal of Medicine; JAMA: Journal of the American Medical Association; ACCP/SCCM: American College of Chest Physicians and Society of Critical Care Medicine.
Animal models fail to recapitulate the clinical phenotype of human sepsis
Fundamental biological processes and signalling pathways are highly conserved across species. The unprecedented opportunity to develop organ-specific transgenic models has provided essential insights into physiological and pathophysiological mechanisms. For example, murine models of cardiac injury are highly tractable in relation to translational human work. By contrast, murine/rodent models of sepsis have garnered much criticism. In part, the combination of costly alternatives, prohibitive legislation and seductive impact of transgenic murine technology have driven sepsis research into utilising mouse models. However, the genomic responses of mouse models poorly mimic human inflammatory disease. In humans, highly conserved mRNA expression is observed in circulating leukocytes following traumatic injury, burns and endotoxin infusion.22,23 By contrast, these genomic changes do not correlate with murine homologs, which in turn demonstrate much greater variation in response to disparate inflammatory stimuli. 22 Of course, this may merely reflect the impact of clinical interventions that influence morbidity and mortality in human sepsis (e.g. fluid resuscitation), many of which are not taken into account or are technically challenging in murine research models exploring trauma/sepsis. Nevertheless, even allowing for genetic variability amongst murine strains which influence survival,24,25 other major physiologic differences in metabolism, 26 cardiovascular control 27 and gut flora 28 suggest that cautious extrapolation is clearly warranted. However, the detection of tissue injury through Pattern recognition receptors (PRR)29,30 and antimicrobial arsenal 31 also differ between the two species. Up to 10,000-fold higher doses of lipopolysaccharide are required in rodents to create a clinically significant sepsis syndrome. 32 The distribution of leukocyte subsets across sites of infection, including the lungs and gastrointestinal tract, differs substantially.29,33 Humanised immunologic murine models, where human haematopoietic cells and tissues are engrafted into immunodeficient mice, may help circumnavigate some of these challenges.34,35 Death in septic laboratory models is relatively rapid and frequently occurs as a direct consequence of early pathologic changes. 32 By contrast, in humans death from sepsis is usually from delayed multi-organ dysfunction following resuscitation and therapeutic support, rather than a rapid demise from the initial pathogenic trigger. 36 Arguably, many of the clinical features of human sepsis syndrome are difficult to disentangle from the consequences of iatrogenic intervention,37,38 which are delivered on basis of illness severity. While animal models remain essential for molecular pathway characterisation and early drug testing, there is a clear need for additional translational models that facilitate the study of human sepsis with superior fidelity.
Administration of endotoxin to healthy volunteers partially mimics sepsis syndrome
The infusion of endotoxin and specific cytokines generates a short-term model that mimics aspects of the systemic inflammatory response. 39 However, for clear ethical reasons, the doses administered cannot either replicate, or trigger the sequelae leading to, end-organ dysfunction following severe sepsis. Dynamic changes in cytokine expression – a commonly used descriptor of inflammation – following the administration of endotoxin 40 differ markedly from the patterns observed in patients with established sepsis. 41 Furthermore, comorbidities,10,11 medication12,14,15 and clinical interventions42,43 are important features of patients that impact on these signatures of inflammation. 44
Sepsis following elective surgery is sufficiently common to make cohort studies of clinical sepsis feasible
Approximately 234 million surgical procedures are performed worldwide each year, 45 and sepsis syndrome is under-appreciated (yet frequently observed) within selected high-risk surgical groups. 46 Even in prospective randomised controlled trials that aim to reduce surgical site infections, the incidence in either trial arm frequently exceeds 15%.47,48,49 Comorbidities associated with the greatest risk of postoperative complications and sepsis syndrome, include immunosuppressive disease, 50 malnutrition,51,52 advanced age50,53–55 cancer50,53,56 and congestive cardiac failure,50,56,57 all of which are similarly over-represented in the non-surgical population who acquire sepsis syndrome. 58
Major elective surgery is undertaken in a highly phenotyped population
Major elective surgery provides a model whereby a known reproducible inflammatory insult may be administered at a specific time to a patient that acts as their own control. The magnitude of the surgical insult can be predicted and/or relatively controlled by standardised surgical and peri-operative interventions. Protocolised clinical management may minimise variability. 59 Patients undergoing major surgery can undergo extensive pre-operative phenotyping, enabled by the full range of ‘omic’ technology, including characterisation of baseline organ function (imaging, biochemistry, exercise capacity) and the detection of overt or occult pathophysiology. 60 Since the volume of surgery is huge (estimated at >234 million procedures/year worldwide), 45 large numbers of patients may be recruited.
Timing is everything: Serial accessibility of tissue and physiologic data
With carefully considered experimental design, many surgical procedures permit the concurrent acquisition of tissue and physiologic data. Beyond the potentially highly phenotyped standardised pre-operative workup, the serial sampling of tissue (including blood, 61 muscle, 62 wound63,64 and indwelling catheters 65 ) coupled with advanced non-invasive imaging modalities66,67 afford increasingly sophisticated readouts referenced to an individual’s own control data.
Surgery as the definitive human model of damage-associated molecular patterns-induced sepsis syndrome
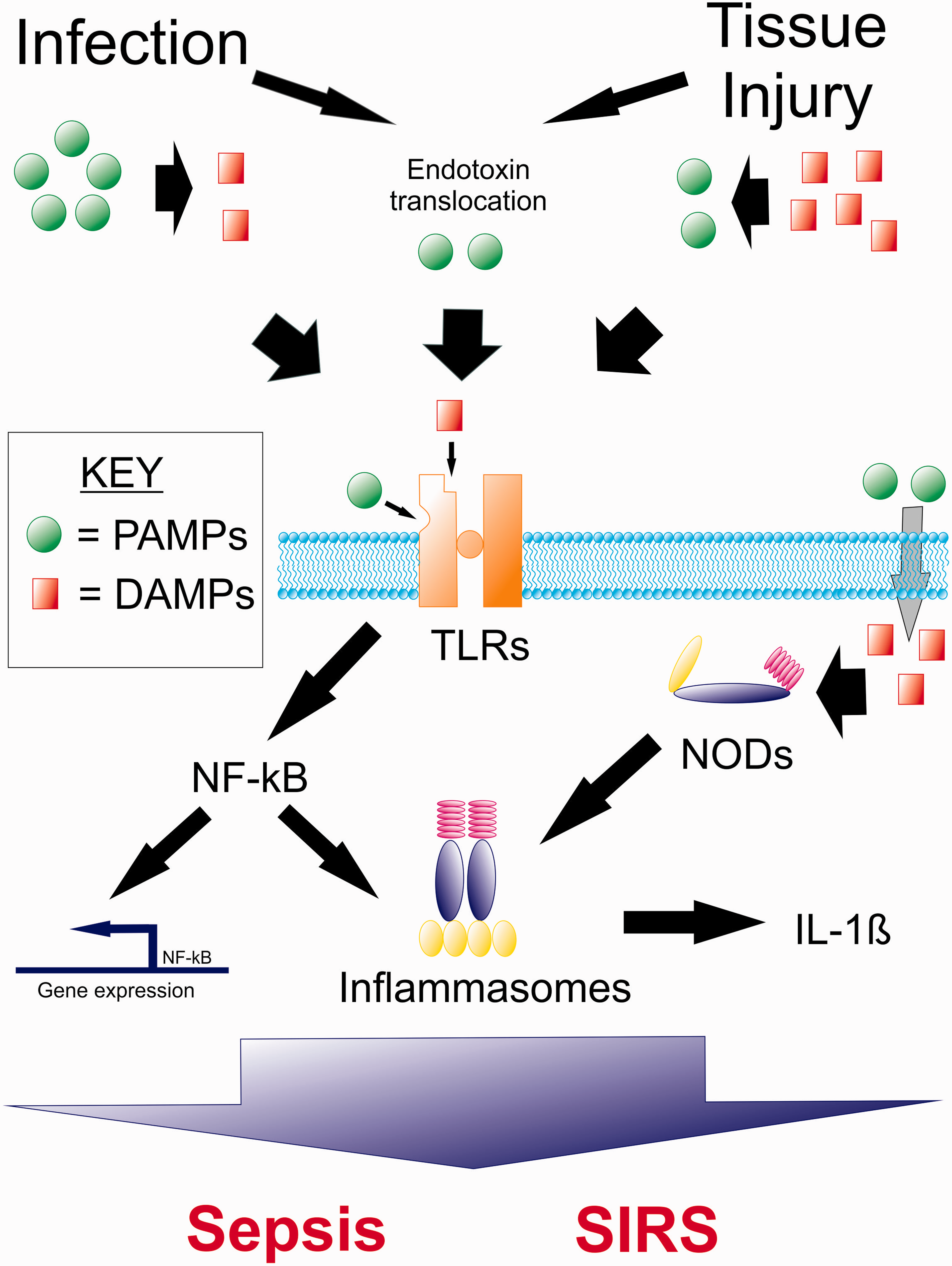
Surgical or traumatic tissue injury causes a systemic inflammatory syndrome that clinically mimics sepsis syndrome. Damage-associated molecular patterns (DAMPs) released following cellular injury activate innate and adaptive immunocytes through PRRs, in a manner broadly similar to pathogen-associated molecular patterns (PAMPs) (Figure 1). Circulating levels of mitochondrial DNA are a thousand-fold higher in major trauma patients compared to healthy volunteers,
68
and post-injury plasma levels are associated with mortality.
69
Infusion of mitochondrial formyl peptides into rats recreates a sepsis syndrome phenotype characterised by neutrophil, albumin and fluid accumulation within the lungs. Co-administration of formyl peptide blocking antibodies limits this injury. The observation that both DAMPs and PAMPs trigger a similar clinical appearance is biologically predictable, since tissue trauma releases these mitochondrial-derived DAMPs that share evolutionarily conserved signalling properties with bacterial PAMPs.70,71 The interaction between conserved, shared signalling mechanisms used by DAMPs and PAMPs is likely to be critical for understanding both the development and response to sepsis syndrome.
Critical shared steps during the inflammatory response to infection and tissue injury. Infection causes local tissue injury and tissue injury predisposes to infection – both stimuli lead to release of Damage Associated Molecular Patterns (DAMPs) and Pathogen Associated Molecular Patterns (PAMPs). DAMPs and PAMPs are recognised by the same Pattern Recognition Receptors, including Toll-Like Receptors (TLRs), Nod-Like Receptors (NLRs) and Rig-Like Receptors (RIGs). Activation of these receptors leads to NK-kB expression and formation of a range of inflammasomes. Inflammasomes are large subunit oligomers that represent an all-or-nothing step in the summation of a cells response to inflammatory stimuli. They are platforms where pivotal pro-inflammatory compounds such as IL-1β are synthesised. Adapted from Mollen et al.
111
Examples of peri-operative biology preceding pivotal advances in critical illness
Mechanical ventilation is a common mode of injury in both critically ill and surgical patients, which may be, in part, determined by DAMP release. While lung protective ventilation has an established role in the management of Acute Respiratory Distress Syndrome (ARDS)
42
randomised controlled trials of this strategy in elective surgical patients provided some of the first and most robust human data that specific ventilation practices alone directly cause alveolar injury.
72
Elsewhere one lung ventilation during elective surgery has been used as a model of human acute lung injury for characterising the anti-inflammatory properties of beta agonists and 3-hydroxy-3-methyl-glutaryl-CoA (HMG CoA) reductase inhibitors.73,74 prior to investigation of the same agents in those with established critical illness.
75
Key contributions from peri-operative biology to our understanding of sepsis syndrome are detailed in Figure 2.
Mechanisms of sepsis syndrome uncovered by studying the biology of elective surgery.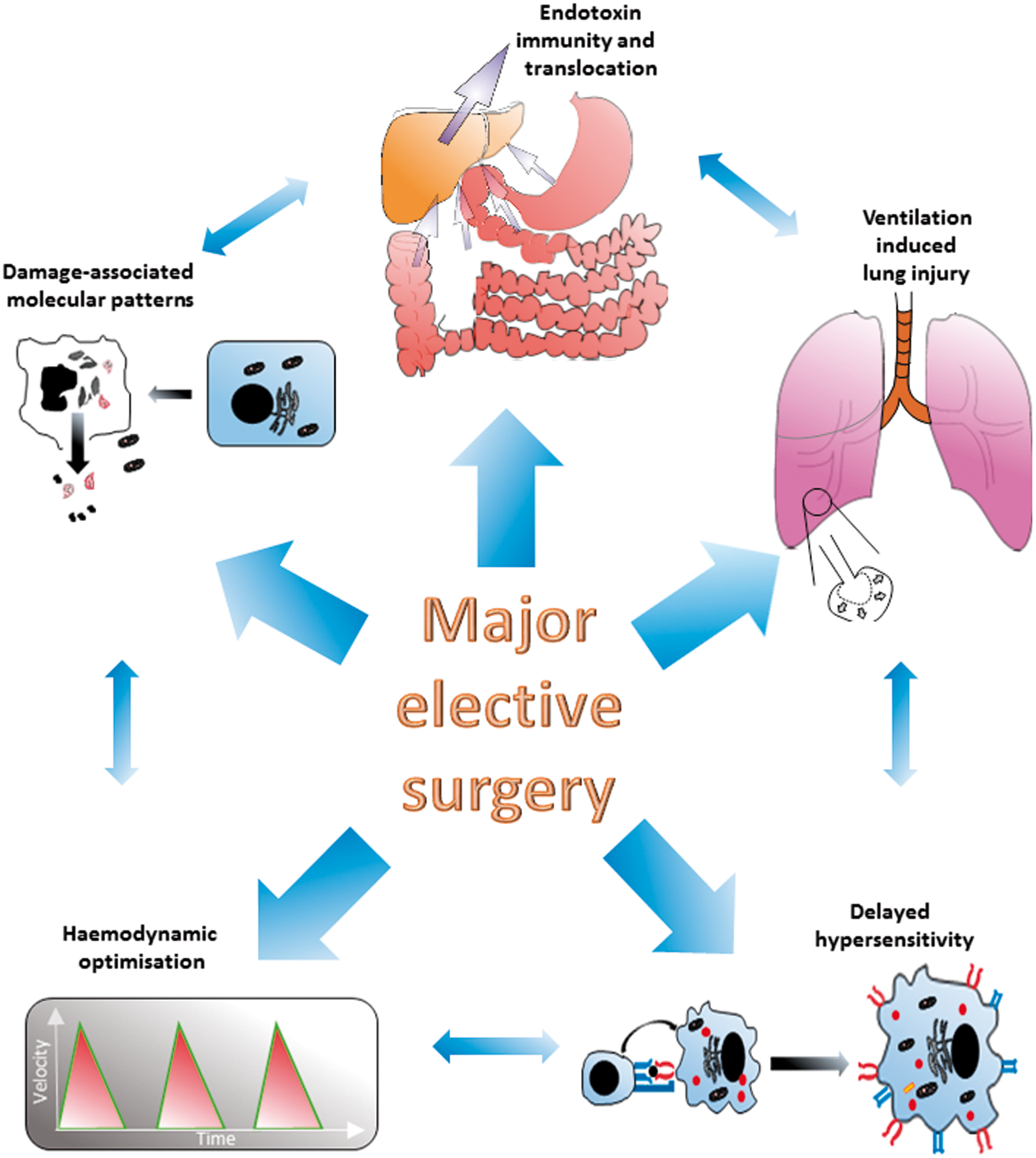
Priming of organ injury is a ubiquitous feature of major surgery
Priming describes how the serial application of otherwise innocuous insults leads to far greater inflammatory response than would be expected from the summation of the two insults. In murine experimental models, ischaemic-reperfusion injury to the gut, followed by endotoxin, dramatically increases mortality when compared to either insult alone. 76 At a cellular level, priming may be partly explained by changes to neutrophil functionality and endothelial activation. 77 The same processes may explain the high incidence of ARDS and multi-organ failure that occur in trauma patients who suffer early complications. 78 It follows that major surgery may therefore prime patients for exaggerated responses to early postoperative complications. Interactions through Toll-Like Receptor 4 (TLR4), and associated pattern recognition receptors, provide a molecular explanation for the priming phenomenon. In murine models, functional TLR4 has been shown to be critical for the development of lung injury following haemorrhagic shock.79,80 Beyond epithelial/immune cell interactions haemorrhagic shock has also been associated with activation of the NLRP3 inflammasome within lung endothelial cells. 81 Thus, surgical tissue trauma priming provides an opportunity to investigate how subsequent cellular responses to endogenous (e.g. gut derived bacterial endotoxin) 82 or acquired PAMPs alter subsequent cellular responses to further DAMP and/or PAMP encounters.
Cell-mediated immunosuppression following sepsis and surgery
The immunosuppressive phase of sepsis that follows the primary trigger is characterised by reactivation of latent viruses83,84 and a failure to eradicate opportunistic and/or endogenous (gut) pathogens. 85 Experimental and clinical data show that apoptotic depletion of lymphocytes 86 increased T regulatory 87 and myeloid-derived suppressor cells 88 contributes to sepsis-induced immunosuppression. In surgical patients, pre-operative lymphopenia89–92 and the failure to demonstrate a delayed-hypersensitivity response to intradermal injections of recall antigens (anergy) 93 are associated with an increased risk of developing sepsis syndrome postoperatively. Thus, striking similarities exist between the hyporesponsive phase following the onset of sepsis and the immunosuppression observed postoperatively.
A common mechanistic role for endotoxin?
Estimates of human bacterial floral content place the endogenous endotoxin reservoir within the order of grams, 94 many-fold more than the nanogram doses required to initiate a systemic inflammatory response. 95 Hypo-perfusion leading to translocation of gut derived endotoxin 96 may provide a common mechanism that drives the inflammatory response to diverse intestinal pathogens expressing virulence determinants triggered by environmental signals indicating host stress 97 (Figure 1). Endotoxaemia is detectable in patients who have severe sepsis regardless of causative organism,98,99 and in those undergoing major surgery, such as vascular repair. 99 Within general intensive care patients endotoxaemia is associated with the severity of sepsis syndrome. 98 Pre-operative deficiency in antibodies to endotoxin is associated with higher levels of postoperative inflammation and excess morbidity.100–102
Conclusion
Fundamental limitations in both animal and patient models have contributed to a lack of therapeutic progress in human sepsis. Surgery provides a biologically and clinically relevant model that avoids many such limitations. This human model enables the investigation of a timed, major inflammatory insult in highly phenotyped patients serving as their own control. Beyond the biological modelling of sepsis on the initial surgical insult, sepsis syndrome is sufficiently common and predictable within the large numbers of patients undergoing surgical procedures to enable cohort studies of sepsis itself. This clinical population offers an unparalleled opportunity to combine carefully planned mechanistic work as part of clinically relevant outcome, a feature frequently absent in critical care trials.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.