
Abstract
As life expectancy increases among industrialized countries, age-related illnesses such as Alzheimer’s have become more common. Alzheimer’s, a common type of dementia, encompasses progressive cognitive loss, impacting memory, reasoning, and social behavior. This article explores the integration of slow memory within the MEM+ application, designed to stimulate memory and cognitive functions in people with Alzheimer’s dementia. This article presents a methodological approach to incorporating slow memory exercises into MEM*, ensuring adaptability for people with dementia across different stages of the disease. The applied methodologies encompass iterative design processes, cognitive task evaluations, and feedback collection from health professionals and people with dementia. The application’s effectiveness was assessed through a combination of quantitative cognitive impact assessments and qualitative feedback, focusing on the impact on memory retention and cognitive performance. Findings suggest that a slow memory approach, when combined with digital cognitive tools, can play a crucial role in enhancing engagement among people with dementia.
Introduction
Slow memory concept refers to the crescent process and mechanism through which each individual or the whole society processes the memories of the past, focusing on subtle and long-term changes rather than sudden and focal events. This concept emerged within the memory studies research scholars who value historical transformations—such as social, cultural, and environmental movements—that shape individual and collective narratives over time(Wustenberg, 2023). Notably, slow memory is characterized by its diffuse nature, making it difficult to identify specific moments of significance. It encompasses phenomena such as the impacts of climate change, changing gender relations, and the effects of deindustrialization, which accumulate over time yet remain largely absent from public discourse and memory politics. The complexities of slow memory raise essential questions about how contemporary societies commemorate the past and integrate these gradual transformations into their collective consciousness. The concept of slow memory is intertwined with the notion of “la longue durée,” highlighting the resilience of collective memories amid rapid societal changes. It seeks to address the memory processes that unfold across generations and within various contexts, such as educational policies and public discourse. The article proposes applying the concept of slow memory to healthcare, introducing a mindful, patient-centered approach to both the care provided and the patient experience. This perspective encourages care providers to prioritize deeper, more intentional interactions with patients, focusing on quality, empathy, and long-term well-being rather than rushed, transactional care. This approach is applied to a computerized environment designed to target people with dementia and to help them to train and promote the maintenance of their memories—individual and social ones.
Alzheimer’s disease (AD) is the most common form of dementia representing around 60% to 70% of registered dementia cases (Associação Portuguesa de Alzheimer, n.d.). Language, thinking, attention, and concentration are some of the functions affected by the disease that leads to the death of brain cells and the cutting of communication within the brain. The progression of the disease varies from person to person. But the disease eventually leads to a situation of complete dependence and ultimately death. There are no known causes for this disease and research does not yet offer answers to understand the onset of the disease, but age (over 65 years) is associated with many the cases of sporadic AD (Coentre, n.d.). Treatment involves strategies to prolong functioning for as long as possible and may include medications that can slow the progression of the disease (Huang, 2023). It is increasingly recognized that pharmacological treatments for dementia should be employed as a second approach and that non-pharmacological options should be highlighted as best practice in these situations. Although many non-pharmacological treatments have reported benefits in several research studies, there is a need for more reliable and valid data before the effectiveness of these approaches is widely recognized (Sopina, 2018). Due to AD, there are several changes that cause memory loss in the people with dementia: the cortex shrinks, which damages the regions involved with thoughts, plans, and memories; this shrinkage is mainly severe in the hippocampus, a region of the cortex that plays an important role in the formation of new memories, and the ventricles (fluid-filled spaces within the brain) become larger (Alzheimer’s Society, 2019).
Kachar (2003) in her book states that old people tend not to organize information into categories and do not form visual images, making memorization difficult, and there is a decrease in the ability to manipulate and organize information from short-term memories. Criteria for organizing, categorizing, differentiating, and discriminating information are essential for a good relationship between the elderly and interactive applications. It is essential that users’ memory is not overloaded with irrelevant procedures. Consistency of elements, coherent color coding and are indispensable. Such factors can contribute to the good use of the system (Cybis et al., 2015).
In recent years, the healthcare has been boosted by new technologies integrated into medical procedures, where the use of computers for the training and education of people with special needs stands out. Cognitive rehabilitation (CR) is a set of therapeutic processes of sensory stimulation, applied to people with dementias who have their cognitive functions compromised due to some type of brain damage. The main cognitive functions include perception, attention, memory, reasoning, and language. A CR treatment is based on the stimulation of cognitive functions, applying games that reproduce everyday situations. These games, in which the people with dementia are encouraged to interact and concentrate, can be supported by several interaction formats such as forms, images, and videos (Nascimento et al., 2008).
Joan Stiles mentions that traditional neuropsychology/biology believed that only the developing brain possessed a transient capacity for plastic reorganization, which allows it to reduce the eventual damage to the brain (Stiles, 2000). However, several studies conducted in the 1990s showed that plasticity is not transient, that is, active only at the age of development, nor only auxiliary or compensatory (as being only a process not essential to the brain’s own development) (Giulio and Mentor, 2004). This type of rehabilitation relies on the plastic capacity of the brain. With all the results of the research carried out in this area, among the different functions that emerge from the interactions between neurons, the ones that can be influenced by external factors are those associated with learning (or the ability to modify behavior in response to experience) and memory (the ability to store this change for a period). Therefore, the possibility of brain plasticity from environmental influences is essential for the development of therapeutic strategies to treat various brain disorders (Nascimento et al., 2008).
The reality of our society is that the computer, provided with several auxiliary means of dynamic interaction, is a fundamental instrument in supporting this type of rehabilitation. The most diverse daily situations can be created, reasoning exercises can be repeated exhaustively (helping with decision-making), emotional reactions can be stimulated (increasing self-confidence), and problems can be proposed in a varied manner (increasing their capacity for concentration and memory) (Nascimento et al., 2008). Rai et al. (2021) concluded from their study that the individual cognitive stimulation therapy application (iCST app) targeted at people with dementia showed being enjoyable and fun and that most of them completed the available activities faster than thought. Some of the carers in the study also stated an improvement of quality of life. Similar findings had Cavallo et al. in their study, where people with dementias in the experimental group showed a significant progress in several neuropsychological domains, which remained stable after 6 months (Cavallo and Angilletta, 2019).
Cognitive training has been established as a viable intervention for early-stage dementia (Clare and Woods, 2004; Jean et al., 2010). To maximize results, our approach tries to leverage the relative preservation of self-related processing in dementia (Kalenzaga et al., 2013) by using autobiographical narratives as the primary stimulus for cognitive exercises. This approach directly targets the episodic memory, the decline of which is a feature of AD (El Haj et al., 2015).
The goal is to apply the concept of slow memory to healthcare, introducing a mindful, patient-centered approach to both caregiving and patient experiences. This perspective encourages healthcare providers to prioritize deeper, more intentional patient interactions, focusing on quality, empathy, and long-term well-being rather than rushed, transactional care. With this goal in mind, MEM+ is presented and discussed from a slow memory perspective.
MEM+
MEM+ was developed using a participatory design approach, guided by the principles outlined by Schuler and Namioka (1993). This process involved collaboration among specialized professionals and technicians from various fields, including psychology, physical therapy, and medicine. One of the challenges faced was the inclusion of individuals with dementia—who are the end-users of MEM+—as they often feel uncomfortable having their vulnerabilities exposed.
The participatory design took place through informal meetings between developers and these specialized professionals. Typically lasting about 1 hour, these meetings allowed professionals to share insights about their daily routines with people living with dementia. The developers aimed to achieve two main objectives during these discussions:
To understand how the daily routines of individuals with dementia can be represented in a computerized format and what benefits this computerization could bring.
To explore ways in which these routines could be enhanced or extended through the use of computer technology.
Research on AD has shown that a computerized environment can be particularly beneficial for individuals with mild dementia (i.e. people with mild dementia, defined as a global Clinical Dementia Rating (CDR) score of 1 (Morris, 1993), exhibit significant impairment in instrumental daily activities while retaining basic self-care abilities) or those in the early stages of moderate dementia, as confirmed by experts in the field. The MEM+ project aimed to:
- Collect information about the patient’s life story and develop a series of questionnaires to track the progression of the disease.
- Construct narratives based on the information gathered from each questionnaire.
- Create personalized cognitive stimulation games.
- Design everyday life games, such as those focused on identifying colors, daily activities, and professions (see Figure 1).
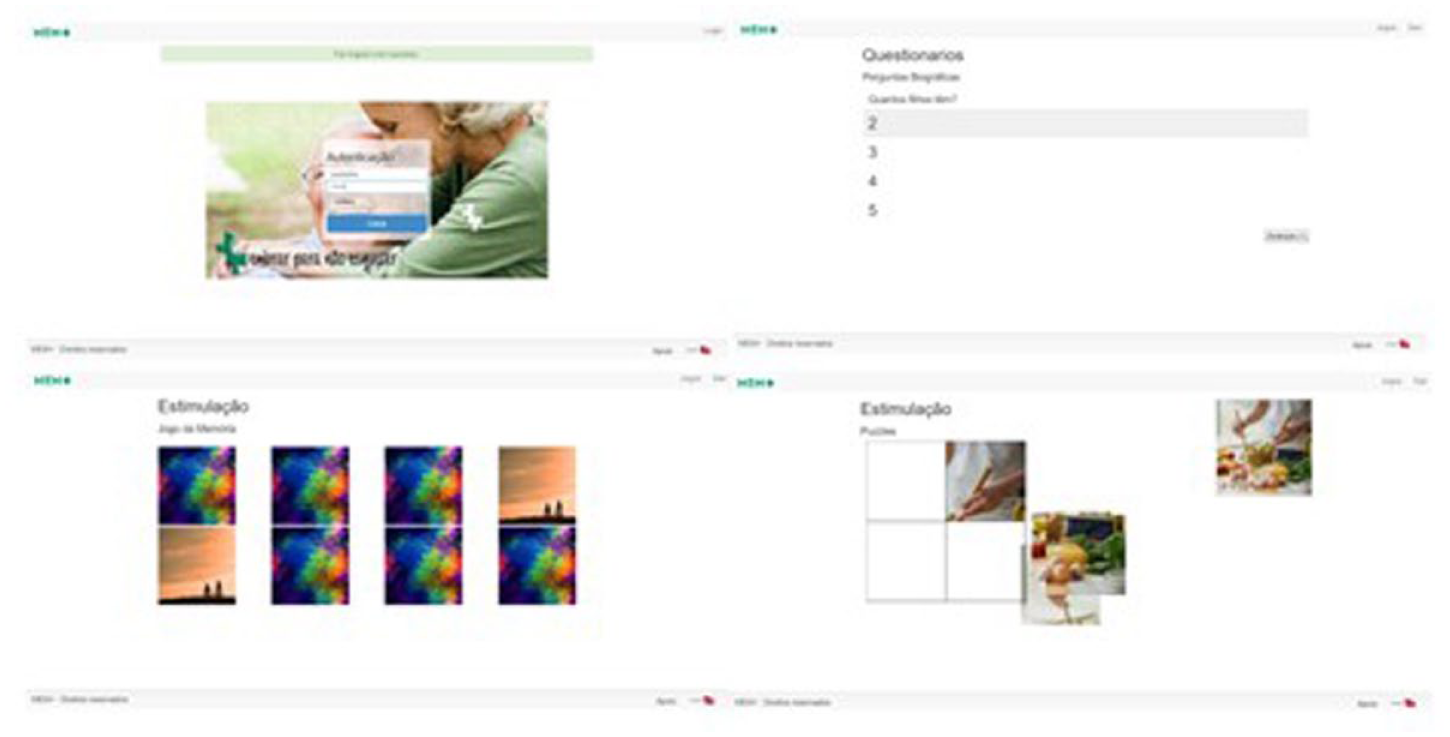
MEM+ application. Image by author.
The questionnaires were generated with information of each individual, and the categories presented were previously chosen by the specialized professional. The questions were grouped according to the following categories: patient, relative, and event. Questions about the category patient are all related to the patient (for instance, name, age). Questions about the category relatives are all family-related. Relatives are divided in two types: the ones that influenced the patient on childhood and adolescence, like their parents and siblings, among others, and the ones that later influenced the patient’s life, like husband/spouse, children, grandchildren, and so on.
The cognitive stimulation games were designed and chosen with the help of specialized professionals since they were adapted from physical games that were used in their daily routines. The cognitive stimulation games developed were memory game, dialing a phone number, ordering daily activities (dress up, lay the table, identifying winter and summer clothes), selecting the notes and coins for a specific amount. For the memory games, the images used were personalized to each individual and increasing levels of difficulty were introduced.
As an interdisciplinary tool in narrative intelligence, the application generates a story or narrative through a series of questions posed to the patient about their life experiences. Each set of questions forms a questionnaire. The answers for each question are generated based on information previously provided by a relative or someone close to the patient. For each question, the patient selects the appropriate answer before proceeding to the next question and its respective answers. At the end of the session, the application presents a short story or history for the patient, highlighting the questions they answered incorrectly. This narrative is enhanced with multimedia files that may aid in the recall process.
This version was applied for a year within the daily routines of one of the centers of the Portuguese Alzheimer’s Association, without a formal study being conducted.
During this time, health professionals identified several issues, some related to the interface designed for individuals with dementia and others stemming from additional needs in their daily activities, highlighting the necessity for further development. Throughout this year of usage, some individuals with dementia left the institution for various reasons, including health deterioration and death. Those who remained engaged mainly with the questionnaires and games. Unfortunately, this limited participation made it difficult to obtain more concrete data to support our conclusions. Although no formal evaluation took place, technicians reported challenges such as:
- Individuals with dementia were confused when interacting with the questionnaires, particularly when they could not proceed because there was not a back button.
- The puzzles presented two types of challenges: it was unclear what the word level entailed, and there was no option for individuals who were unable to complete them.
A key consideration was the games, as in the initial version of MEM+ did not provide adequate data collection for valid diagnoses. In addition, there was a lack of an interface to visualize game results. Furthermore, the interaction of individuals with dementia with the application highlighted the need for a simpler and more intuitive design. Technicians also faced challenges in managing the application independently, leading to requests for enhanced functionality. With these goals in mind, an MEM* was developed to enhance the interactions available for its stakeholders (people with dementia and technicians).
Evolving MEM+ into MEM*
To address the limitations of MEM+, another participatory design approach was initiated, starting with the identification of necessary changes. This new study involved collaboration with the Portuguese Alzheimer’s Association and other healthcare centers for people with dementia. A primary focus was on enhancing the gaming aspect of the application. The previous version of MEM+ did not provide sufficient data for accurate diagnoses, and there was no interface to visualize game results. It was also crucial to improve how individuals with dementia interacted with the application by creating a simpler and more intuitive user experience. Moreover, technicians lacked autonomy in managing the application, which led to a request for improved functionality in this area.
Designing a computerized environment to support memory in dementia care requires a thoughtful combination of cognitive support, sensory engagement, and emotional well-being, which can be thought of as a slow memory approach. To achieve this, a requirements analysis was conducted. The stakeholders of MEM*—the augmented version of MEM+—include administrators, who manage the entire application; technicians, who assist and interact with individuals with dementia; and the individuals with dementia themselves, who only have access to a list of activities associated with them and can perform those activities. Please refer to the list of requirements in Table 1.
Requirements analysis.
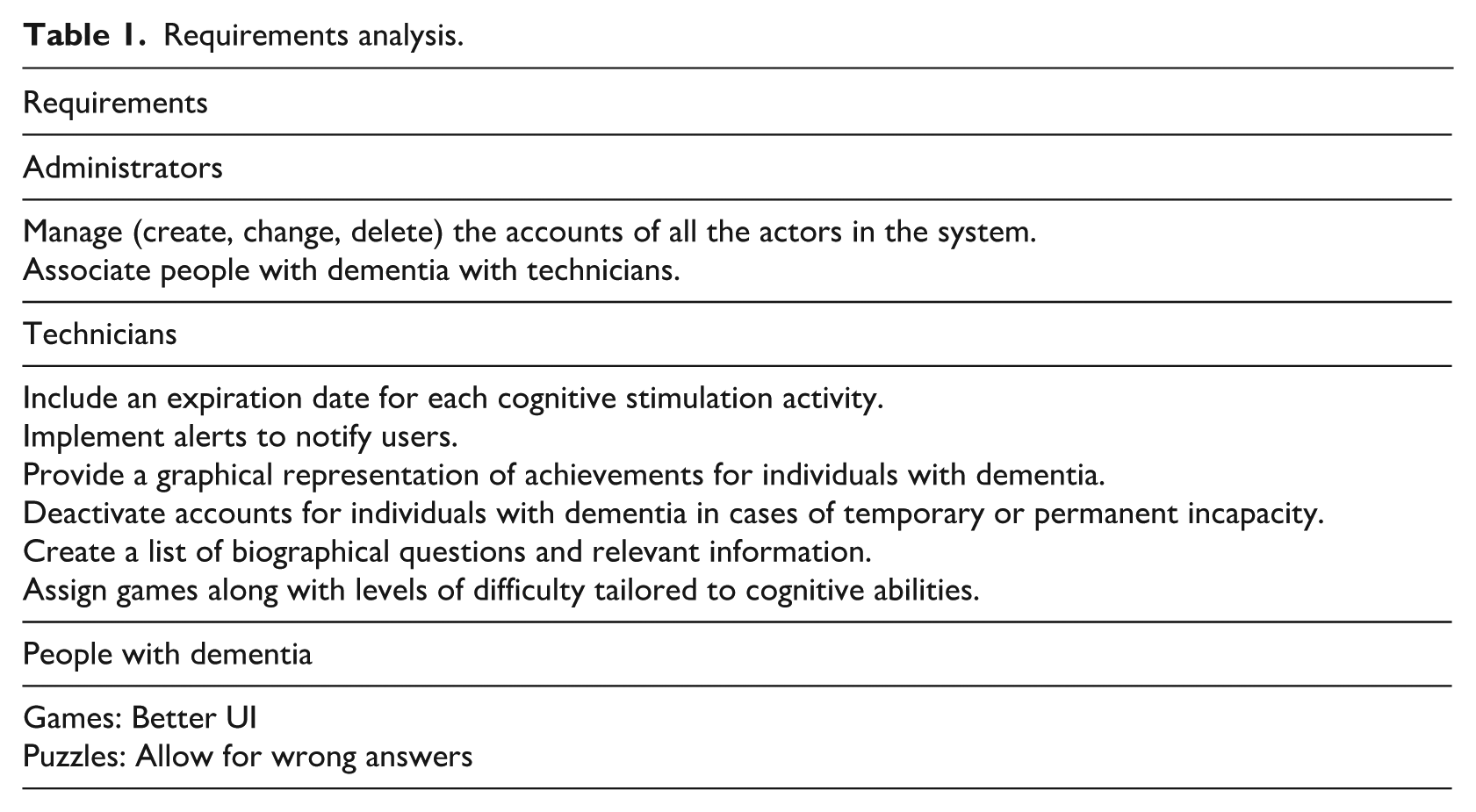
The implemented expiration date feature alerts technicians when a specific activity is about to expire or has already expired. If a technician wants individuals with dementia to engage in the same activity multiple times, they can easily duplicate it. This duplication enhances the reliability of subsequent analyses, as it allows for comparisons of activities involving the same games and levels.
The assignment of individuals with dementia to specific technicians means that each technician can only view and manage people associated with them. However, any administrator has the ability to modify this configuration and reassign an individual with dementia to a different technician.
The results from individuals with dementia can be visualized using graphics, and these data can be exported to an Excel document. This feature allows professionals to analyze the progression of the disease more effectively. When the administrator or technician updates the status of individuals with dementia by indicating that they have passed away or are hospitalized, the accounts of these individuals will be deactivated.
During the creation of activities, only games suitable for individuals with dementia will be displayed. If certain information is not available in the database, it will not be included in the list. For example, if there are no grandchildren or children registered in the database for a specific individual, related questions will not appear for the technician. In addition, the technician must select the appropriate level of stimulation for the game when creating the activity.
Each time the technician opens the application, the alert table on the home page will be updated. The activities listed will only include those associated with the individuals with dementia linked to the technician currently in session. In the details of the therapy session, the progress of the activity will be noted as either “Finished” or “In Progress.”
Applying slow memory approach in MEM*
At this stage, we must clearly identify the connection between MEM* and slow memory concept. This raises an important question: How can we effectively design and implement a computerized environment that leverages slow memory concept to enhance care for individuals with dementia? By exploring the integration of these concepts, we aim to create a supportive setting that caters to the unique cognitive needs of people with dementia, ultimately fostering improved engagement and quality of life.
People with dementia express a progressive memory loss which affects different types of memory. Dementia impacts various types of memory, starting with short-term memory loss, which makes it difficult for individuals to remember recent events or retain new information. As the condition progresses, long-term memory loss begins, resulting in forgotten significant life events and personal histories. Procedural memory loss complicates once-automatic tasks, such as cooking or dressing (De Wit et al., 2021), while semantic memory loss creates challenges in recalling facts, recognizing objects, or understanding language (Hodges, 2006). Episodic memory loss affects personal experiences and the context of past events, and social and emotional memory loss hampers the ability to recognize familiar faces and maintain emotional connections(Hodges, 2006). As dementia advances, spatial memory loss can lead to disorientation and difficulty navigating familiar places, while working memory loss makes it hard to follow conversations or complete immediate tasks. In severe stages, autobiographical memory loss can erode one’s sense of self, causing confusion about personal identity(Addis and Tippett, 2004). Even implicit memory, which governs unconscious actions like reflexes, can deteriorate over time. Understanding these different forms of memory loss is crucial for providing support in MEM*.
Suggested methodologies
The most relevant methodologies identified were:
Memory-Centered Design Approach—Since the inception of MEM+, there has been a strong focus on collecting photos and memory artifacts for use in various components of the computerized environment. The aim is to encourage a slow remembrance of events, details, or even loved ones that may have been forgotten. In this new version of MEM*, particular attention has been given to reducing the cognitive load for individuals with dementia by providing simpler interactions.
Minimalist User Interface—Usability is defined as “the extent to which specific users can use a product to achieve specific goals with effectiveness, efficiency, and satisfaction in a specific context of use” (Nielsen, 1994). The aging process brings certain limitations, including reduced visual ability, decreased attention, loss of movement accuracy, and challenges with short- and long-term learning and memory (Dickinson, 2021). To address these challenges, usability standards should take into account factors such as the organization of information, ease of interaction, font size, and the use of specific colors. We must acknowledge that many people struggle to differentiate between similar shades or colors, such as blue and green, especially as they age. Seniors and individuals with low vision find it easier to read Arial or Helvetica typefaces, with Sans Serif fonts being the most suitable choice. However, it is also important to consider font size. In the design of websites and web applications, there is often a tendency to use small fonts with low contrast, which can be problematic. While it is possible to increase the font size in a browser, many older users may not know how to do this. Therefore, it is crucial to design for all audiences (Hou et al., 2022). Icons and buttons should be large and distinguishable from the surrounding text. Links must have descriptive and easy-to-read text that includes verbs to indicate actions clearly. These considerations not only enhance usability but also support memory stimulation and help compensate for abilities affected by various conditions, improving overall comprehension of the information presented (see Figure 2 depicting this minimalist interface design).
Slow Interaction Approach—The system is designed to foster meaningful and deliberate interactions rather than fast ones. Users are encouraged to engage at a comfortable pace. This alert serves as an essential notification for technicians, indicating when a particular individual has not yet completed a designated activity. To ensure that users feel supported, it can be advantageous to provide gentle encouragement or additional assistance when necessary. However, it is crucial to maintain the activity on the task list, as removing it may lead to confusion for people with dementia. This approach not only respects the user’s pace but also helps to enhance their sense of autonomy and understanding as they navigate their tasks. The cognitive stimulus games are thoughtfully designed to respect each user’s individual pace by offering a range of difficulty levels tailored to accommodate varying skill sets. This flexibility allows users to engage at a level that feels comfortable for them, fostering a positive and encouraging experience. Moreover, if a user encounters a challenge that feels overwhelming, they have the option to exit a specific interaction. This feature serves as a clear signal to the technician, highlighting the need for potential adjustments to enhance the user’s experience.
Reminiscence Therapy—This therapy is a vital approach in dementia care, effectively enabling individuals to reconnect with significant memories through powerful mediums such as photos, music, and storytelling (Woods et al., 2018). When a new participant begins using the MEM*, their family members are expected to contribute multimedia elements to their profile. These contributions are essential for creating detailed biographical questionnaires and crafting a compelling narrative that reflects the individual’s life. The story is presented through a timeline audio recording, often enhanced by photographs that illustrate their memories and experiences. Figure 3 illustrates one of the stimulation games that is personalized with photos but due to privacy issues is exemplified with a random image.
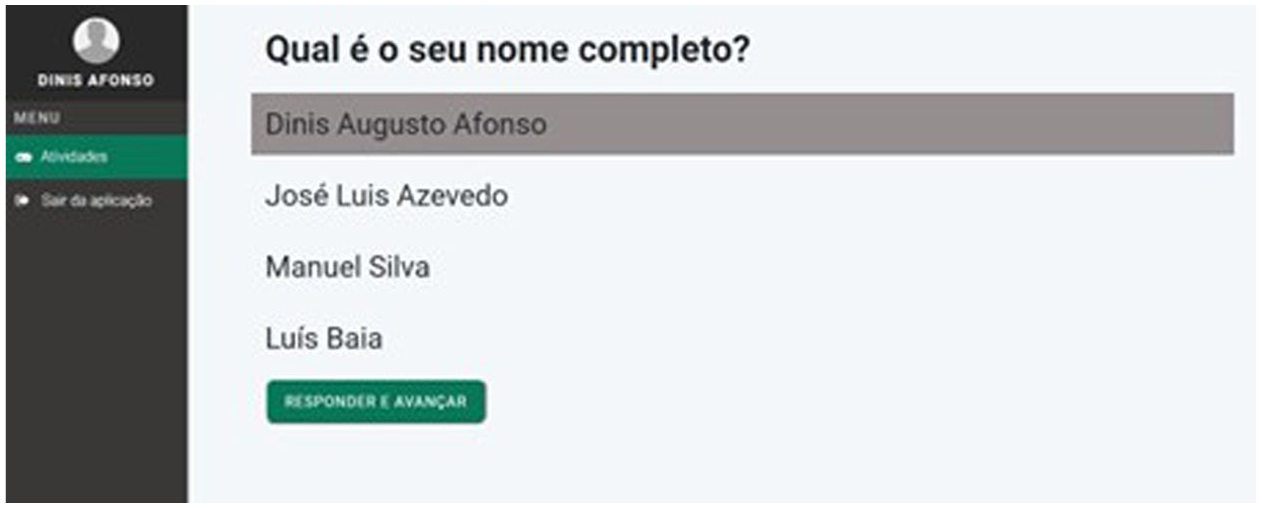
Minimalist interface. Image by author.
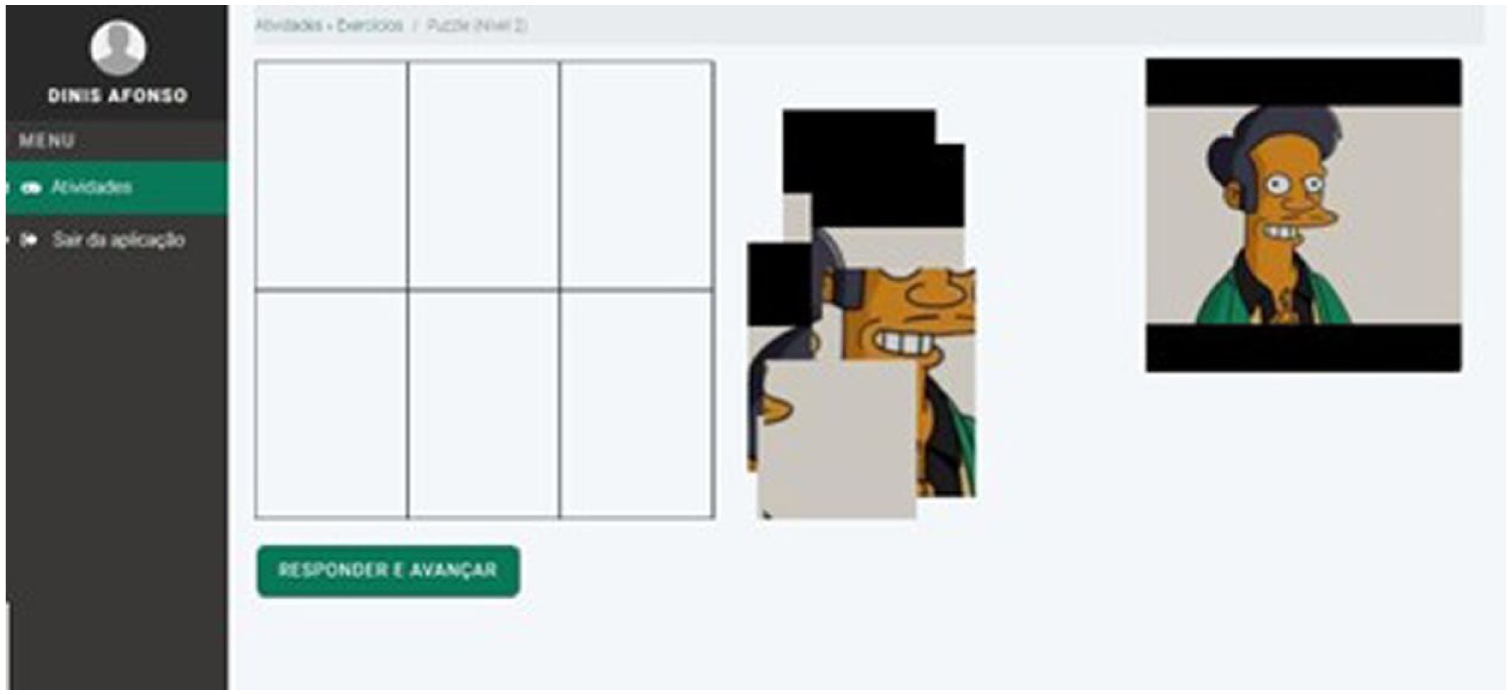
Stimulation game. Image by author.
All these approaches rigorously follow established ethical and privacy guidelines, which ensure that each MEM* user’s data remains confidential and accessible only to the individual and their designated technician. This safeguarding of information is paramount in maintaining trust and integrity within the therapeutic relationship. Progress reports are generated solely for the purpose of equipping medical technicians with crucial insights, enabling them to make informed adjustments to therapeutic plans. These reports are instrumental in analyzing the effectiveness of current interventions and in devising tailored strategies for future care, ensuring that each user receives personalized therapeutic support that meets their unique needs.
Validation of user interface of MEM*
An informal evaluation session was conducted to validate the changes implemented in the new MEM*. In this meeting, the head of the elderly care service and two technicians from the center, who interact directly with individuals with dementia, participated. The application was demonstrated, and its objectives and functionalities were explained in order to gather feedback on the improvements made. The session lasted for the entire morning and followed this structure:
Presentation of the application and its main objectives.
Demonstration of the key functionalities across all user profiles.
Individual testing of the application by each member of the team.
Group discussion and collection of suggestions.
This project was conducted in 2019. The meeting was held in person, and the researcher took written notes throughout various stages of the discussion.
The feedback received was positive; however, several suggestions were made:
- One suggestion from the interaction between the technician and the application was to include an analysis graph for each session, in addition to the existing graph per activity.
- Another suggestion from the social center concerned the analysis of results. It was proposed to assign a score to each game, allowing for a comparison of scores based on the Mini-Mental State Examination (Upton, 2013). This approach enables health professionals to analyze results more reliably than when solely considering the duration of the game, which was the initial focus.
- Some areas for improvement were identified regarding the games, particularly concerning the text and questionnaires. It was recommended to replace text with images to make the application more intuitive and less overwhelming for individuals with dementia. This change would also enhance accessibility for all individuals with dementia, including those who are illiterate.
- In the game “Order of Dressing,” it was suggested to allow more than one correct answer, as the current version only permits one specific order: boxers, trousers, t-shirts, shoes, and jackets.
- In addition, an improvement was proposed for future versions of the games, allowing players to advance without answering questions. This would enable individuals with dementia to return to the game later, helping prevent boredom and discouragement.
The integration of graphics and effective export features was considered very beneficial; however, the elements involved should be reviewed and analyzed in greater detail. This implementation would lead to more conclusive diagnoses and more productive follow-ups for individuals with dementia. At that time, information about activities carried out in the centers is stored on paper. This functionality would allow institutions to transition to a new digital format without losing important information. This interaction with the care professional—qualitative study—was important to gather data about their satisfaction and also to evaluate MEM* adequacy to their daily routine with the people with dementia.
Evaluation of MEM* with people with dementia
After validation by experts (technicians from partner associations), an evaluation study was conducted involving 35 individuals with dementia across three different associations, primarily women (see Figure 4).
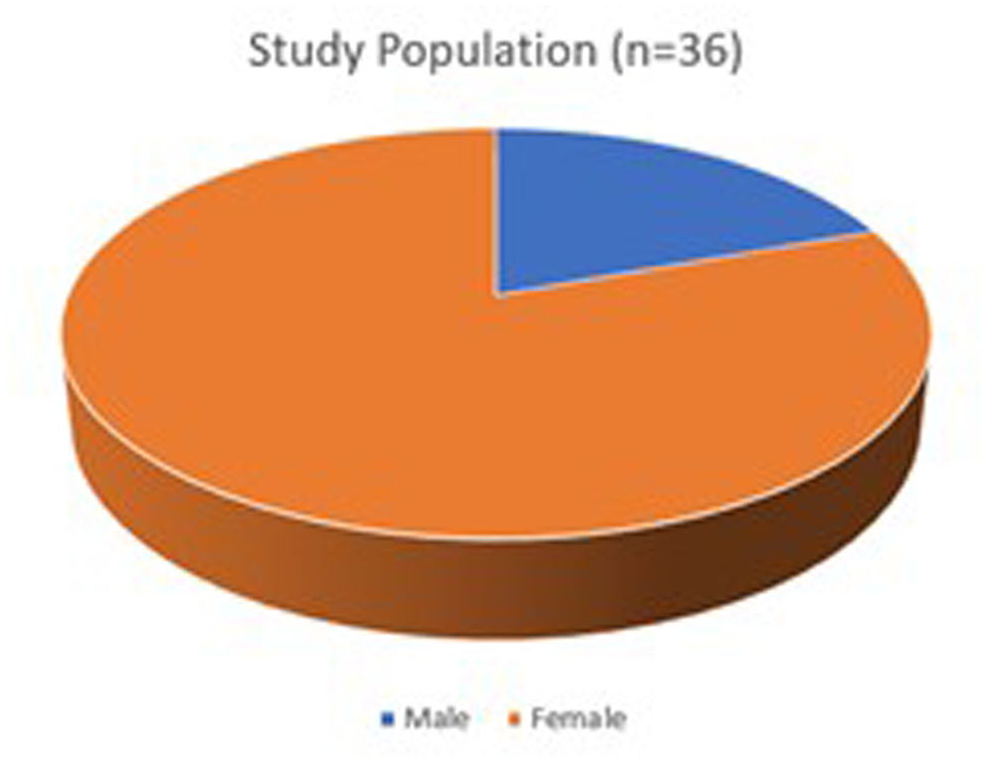
Study population. Image by author.
All participants were in the mild stage of dementia, and Figure 5 illustrates the age distribution among them. The majority had minimal experience using computers, tablets, or smartphones. Most participants owned conventional mobile phones that did not have Internet access.
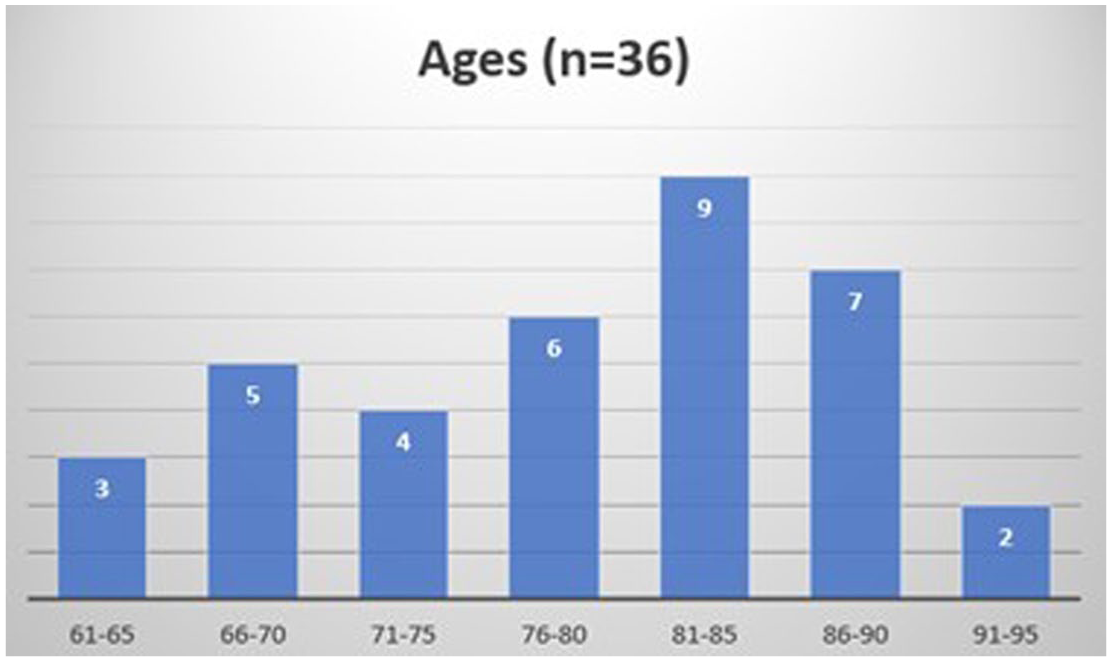
Age of study population. Image by author.
The study involved integrating MEM* into the routine of each association and the daily lives of individuals with dementia. It ran for 3 months, starting in September 2019, with a minimum of one interaction per week. Prior to the study, informed consent was obtained from each person with dementia.
In cases where individuals were unable to provide consent, their caregivers gave the necessary approval. It is important to note that individuals with dementia attended the institution only during the day and returned to their homes or families for the night. None of the participants had any prior experience with MEM+ or MEM*. Before the study commenced, personal information (biographical data) and meaningful photos were collected for each participant in order to personalize their experience. A researcher, using an administrator profile, entered these data and created accounts for the technicians involved in the study. The research used a post-intervention evaluation design which did not include a control group. The evaluation process took place after participants used the application when healthcare professionals (technicians) conducted the assessment. The researchers did not apply control groups and pre-test assessments because of three essential factors: the researchers encountered an impossible task when they tried to involve enough participants who met the criteria for equivalent groups in their controlled trial; the distinct ways dementia progresses in each person creates problems when trying to establish comparable groups for research; and finally, MEM* intervention uses individualized biographical information which creates distinct experiences for every participant. The application provides individualized results which prevents researchers from conducting standardized assessments between participants or against a standard control group.
The research design assessed how well the application worked and its user interface and professional value from the caregiver’s point of view.
The technicians received a 3-hour training session before conducting therapy sessions with the individuals with dementia. The timing for encouraging individuals with dementia to interact with MEM* was tailored to each person’s routine and varied by association, as each organization had different activities planned for their patients. The length of these interactions also depended on the individual with dementia and the technician involved. However, some of these individuals could interact independently in certain situations, although most required the support of a specialized technician.
This study aimed to assess whether the new user interface was well-received by individuals with dementia and to determine if they could successfully complete the challenges, primarily the stimulation games, implicitly evaluating if the slow memory approaches to dementia care were also well succeeded. To achieve our first goal, we aimed for a target of zero abandonment or give-ups. For the second goal, we sought to have the majority of the participants (more than two-thirds) successfully complete the challenges.
The results gathered from the data collected by the application—quantitative assessment—indicated a positive evolution in most participants regarding their correct responses and outcomes from the cognitive stimulation games. The participants of the study had the possibility to interact with the games/activities proposed by the technicians in a continuous way; therefore, it was possible to compare the results (success/failure) and the time of each interaction. From the stored data, it was possible to conclude that 74% of the participants demonstrated improved performance since their first interaction with the application. Furthermore, individuals with dementia showed progress across games of varying complexity (showed by the level of each cognitive game played). However, it was not possible to draw any conclusions regarding the progression of the disease due to the short assessment period. Another positive outcome was that none of the study participants expressed frustration or chose to disengage during the interactions, which fulfilled the study’s first objective and maybe implicitly showing that a slow interaction approach is beneficial. Also, it was not possible to conclude that the improvement of the performance in the games was transferred to daily life activities.
Conclusion
This article presents a twofold participatory design of a computerized environment aimed at assisting people with dementia. The primary focus was on identifying the issues revealed by MEM+ and applying slow memory methodologies to the new version (MEM*). By determining the new requirements, additional research was conducted to address the problems with the graphical interface in particular.
Taking into account the unique needs of our target population, we conducted a study to develop an adequate user interface that minimizes opportunities for errors, misunderstandings, and fatigue. The new version was validated through feedback from technicians, as conducting formal usability testing with the target audience—people with dementia—would have been overwhelming for them. The feedback gathered allows us to conclude that the usability and accessibility features implemented were crucial to the application’s success. In addition, the changes made to the games enable the collection of more data for health professionals’ diagnoses. However, there is always room for ongoing improvements.
On the other hand, the analysis of data through graphical elements has enhanced the work of professionals. However, more data are needed to incorporate additional graphics and statistics for a deeper understanding. These graphical elements make assessing the progression of dementia in individuals more effective and portable, as they can be exported to a standard digital format.
From the study of people with dementia, we obtained positive and encouraging results. However, due to the study’s limitations—specifically its short duration and small number of participants—these results cannot be generalized. It is also important to note that conducting usability testing with older adults, particularly those with dementia, can be quite complex and challenging due to their physical and cognitive conditions. Unfortunately, this aspect was outside the scope of our research due to limited resources. This was the primary reason we chose to validate our findings with technicians and focus solely on the results obtained during the 3-month study, accounting for any participant withdrawals.
The goal of our intervention is aligned with CR, which is based on stimulating cognitive functions by applying games that reproduce everyday situations. One of the limitations is the impossibility to assess if such improvements were also transferred in the wider context of their daily life, and which could only be measured using standardized clinical tools in future longitudinal studies.
The MEM* application translates the collective concept of slow memory—traditionally focused on gradual societal transformations and “la longue durée”—into a personalized clinical intervention by treating an individual’s life story as their own long-term narrative. Utilizing a memory-centered design and reminiscence therapy, the system shifts care from a transactional to a patient-centered approach, prioritizing the preservation of the “self” through autobiographical narratives and personal artifacts, such as family photos and recordings. This echoes Conway and Pleydell-Pearce’s (2000) proposal that autobiographical memory underpins personhood and grounds the working self within a hierarchical knowledge base. This transition is further supported by a slow interaction approach, which emphasizes meaningful, deliberate engagement at the user’s pace to reduce cognitive load and prevent frustration. Furthermore, the application aligns with (Thomsen, 2009) research, which identifies “chapters”—temporally extended structures—as the primary units organizing life stories, providing thematic and causal coherence for maintaining identity even as specific episodic details fade.
Future directions
Considering the significance of an MEM* and the imperative to support individuals living with dementia, there exists an opportunity to integrate innovative features that can aid their family members and caregivers during their journey. The objective is to provide a platform that not only assists individuals with dementia in preserving their memories but also enables them to construct a new narrative based on their life experiences and emotions in this new stage of their lives.
Caregivers are essential in executing these strategies, as they cultivate supportive environments that promote meaningful interactions and personal reflection.
By utilizing digital devices, informal caregivers can compile voice recordings and photographs to develop a personalized memory bank, which can be accessed and consulted regularly. This thoughtful approach significantly elevates the quality of care while deepening the bonds between caregivers and those they support.
By harnessing the power of AI-driven tools, caregivers can collaboratively craft a personalized storybook that portraits the lives of their loved ones, drawing from past memories and meaningful moments. This co-creative journey not only offers individuals with dementia an engaging and fulfilling activity but also serves as a gentle catalyst for reminiscence, weaving together past experiences into a rich tapestry that fosters the creation of impactful moments in the present.
Caregivers can spark profound conversations during uniquely designed memory-triggered events, carefully tailored to captivate individuals with dementia. These gatherings aim to cultivate a sense of involvement and belonging in their everyday lives. By lovingly revisiting cherished memories and familiar experiences, caregivers can orchestrate moments that are both delightful and enriching.
Moreover, MEM* can provide insightful suggestions, guiding caregivers to identify and implement activities that resonate with the individual’s past, thereby enhancing the overall depth of connection and interaction. In addition, offering daily structured, slow-paced assistance can represent an innovative facet of MEM*, emphasizing adaptive task guidance that’s finely tuned to the cognitive load and emotional well-being of both the caregiver and their loved one. By fostering flexible and familiar routines, this approach creates a nurturing environment where the principles of slow memory can flourish, helping to avoid the sense of haste or overwhelming experiences.
Footnotes
Acknowledgements
This research project could not have been developed without the collaboration of Portuguese Alzheimer’s Association and the other Social Care Associations. A special thank you to the people with dementia and their families who facilitated the acquisition of data and information to personalize the interactions in MEM+ and MEM*.
Ethical considerations
The Ethical Committee of Instituto Universitário de Lisboa (Iscte) gave a positive evaluation to the research and informed consent statements (EC 15/2015).
Funding
The author disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The author received financial support for the research from Fundação EDP—project “Lembrar para Não Esquecer” (2013–2019). This article is based upon work from COST Action Slow Memory: Transformative Practices for Times of Uneven and Accelerating Change, CA20105, supported by COST (European Cooperation in Science and Technology).
Declaration of conflicting interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.