
Abstract
This paper relies on 327 video recordings of well-baby visits in U.S. community practice clinics to explore when and how pediatricians transition to assessing children’s growth. Using conversation analysis supplemented by descriptive frequencies, we examine the primary ways in which participants transition into the activity of assessing the child’s growth. We argue that physicians most commonly orient to the discussion of physical growth as disjunctive with the prior activity. However, when physicians wind up at odds with a parent over whether or not there is a cause for concern with the child, they more often rely on conjunctive activity transitions. Surprisingly, the activity transition into growth assessment becomes a resource that physicians rely on to persuade parents of their view.
As babies develop, they are closely monitored through well-child visits. In the US, these visits are to pediatricians or family medicine physicians who act as the child’s primary care provider. During these visits, physicians evaluate babies for appropriate physical growth (head circumference, length, and weight), motor development (holding their heads up, rolling over, crawling, standing, reaching, and pointing), and cognitive development (babbling, producing words, or responding to directions and corrections). If babies fail to meet developmental milestones, primary care physicians may refer them to relevant specialists (e.g. neurologists, speech therapists, or gastroenterologists). In addition to monitoring development, the CDC’s (US Centers for Disease Control) recommended vaccination schedule aligns with these monitoring visits. Thus, the primary business of these clinic visits is both monitoring and vaccination (Prettner et al., 2024; Ranzani, 2023).
In these visits, participants progress through monitoring activities (e.g. identifying progress in sleeping, eating, locomotion, and language). One particularly salient transition is into the assessment of babies’ physical growth which commonly entails physicians’ sharing visual access to the growth chart. There, the baby’s height, weight, and head circumference are tracked from birth. Based on the chart, it is possible to see what percentile the baby has reached relative to other same-sex, same-age babies. Thus, a baby who is at the 56th percentile is bigger than 56% of same-age, same-sex babies in the US. Reporting the baby’s growth is standard in these visits. In our sample, all physicians reported this information to parents during their visits, and this was most commonly positioned at the transition between physicians asking parents for updates on progress and concerns with development and physically examining the baby.
In this study, we focus on the process of transitioning from one monitoring activity into the growth monitoring activity. We show that most of the time, physicians treat the two activities as separate and highlight this separation through disjunctive transitions. However, physicians sometimes blur the boundary between the prior activity and the growth assessment activity, what we term conjunctive transitions. By blurring the boundary between the two activities, physicians work to leverage the child’s growth assessment as an element of persuasion in addressing a concern (either a parent or physician concern). This matters because the use of a conjunctive transition becomes an unexpected resource through which physicians orient to the need to go beyond offering conclusions; rather, they work to persuade parents to see things their way when physicians and parents are in opposition regarding some aspect of the child’s development.
Background
In this paper, we bring together research on the accomplishment of activity transitions in social interaction, on the one hand, and authority, agency, and accountability in clinical care, on the other. Our contribution to extending knowledge and theory in social interaction resides at the intersection of these two strands of literature and thus contributes to both of these.
Activity transitions
Activities are generally discussed as coherent stretches of conduct that are managed across a series of action sequences (Levinson, 1992; Robinson, 2012). Although activities are ‘fuzzy categories’ (Levinson, 1992: 69), they usually involve goals and constraints on ‘allowable contributions’ (Levinson, 1992: 69). Transitions between activities rely on systematic interactional practices. Research has documented that these practices involve lexicon, prosody, social action, and visible behavior (Couper-Kuhlen, 2001; Goldberg, 2004; Robinson and Stivers, 2001; Schegloff, 1998). They can involve dedicated sequences (Talkington and Maynard, 2021), and are frequently marked by sequence closing objects like ‘Okay’, ‘Alright’, or even ‘Yeah’ (Beach, 1995; Jefferson, 1993; Keevallik, 2010; Schegloff, 2007). Figurative expressions are also resources for topic closure (Holt and Drew, 2005). While inbreaths have not been systematically examined for activity transitions, they are associated with building distance in dispreferred answer turns (Torreira et al., 2015). Within medical visits, requests can be relied on to initiate transitions (Frankel, 1983; Heath, 1986). These ways of marking activity closure are all resources for indicating a boundary and thus may accentuate the next activity as relatively disjoined from the prior activity.
There are also discursive resources dedicated to marking new activities as relatively more conjunctive or disjunctive with the prior activity. Turn prefaces are one consistent way of indicating this. For instance, Mazeland and Huiskes (2001) found that the turn preface ‘But’ orients to a disjunct between activities as do some uses of ‘Oh’ (Bolden, 2006; Heritage, 1998). In contrast, ‘So’ can mark a resumption and thus while the next activity is disjunctive with the just prior activity, it is not completely disjunctive because it returns to something that had been lying in wait (Bolden, 2006). Finally, in contrast with marking disjunction, ‘And’ prefaces work to mark a sequence as the next in a series, thus continuing an in-progress activity (Heritage and Sorjonen, 1994).
While turn prefaces constitute overt markers of conjunction or disjunction, this is not the only way to convey the degree to which activities are connected. People also rely on syntax and other aspects of turn design as has been shown for proposals (deSouza, 2020; Stivers and Sidnell, 2016), requests (Rossi, 2012), and offers (Curl, 2006). For example, naturally occurring requests in Italian interactions include the turn-initial dative pronoun mi ‘to/for me’ in two different constructions – imperative and interrogative – to solicit help with a project. Which one is relied on depends upon whether the project has already been established to be joint or not (Rossi, 2012). Relatedly, during children’s unstructured playtime in a classroom, proposals done through the Let’s X design (e.g. ‘Let’s play robbers’) treat the proposed activity as disjunctive with the prior activity, whereas those done through the How about X design (e.g. ‘How about playing robbers’) treat the proposed activity as conjunctive, providing an incremental modification of an ongoing activity (Stivers and Sidnell, 2016).
Taken together, initiations of activity transitions rely on a variety of resources to convey both that a transition is being initiated and what type of relationship is projected between the new activity and the previous one. Following Stivers and Sidnell (2016), we identify disjunctive transitions as those through which speakers ‘highlight the [prospective] activity as new and disjoined from prior interaction’ (p. 155). Conversely, conjunctive transitions ‘downplay the disjunctiveness’ (p. 155) or, we would add, blur the boundary between the two activities in terms of prosody, body behavior, lexical choice, prefaces, or other non-verbal behavior. We extend prior literature on activity transitions by showing that blurring transitions can do persuasion work in clinical encounters.
Authority, agency, and accountability in clinical care
Research on clinical communication across the last 25 years has consistently identified tensions between patient agency and physician authority (Stivers and Tate, 2023; Timmermans, 2020). Patient agency is found in a variety of communication practices concerned with shaping diagnostic and treatment outcomes including how problems are presented (Karasz et al., 2012; Stivers, 2002; Tate, 2020), how questions are answered (Stivers, 2007; Stivers and Timmermans, 2021), and how diagnoses and treatment recommendations are received (e.g. Kushida and Yamakawa, 2020; Stivers, 2005; Stivers et al., 2018).
This tension is visible in well-baby visits, as documented by European scholars exploring advice-giving (Caronia and Ranzani, 2024; Heritage and Lindstrom, 1998; Heritage and Sefi, 1992; Ranzani, 2024; Zanini and González-Martínez, 2015). Specifically, in contrast to adult care encounters, both parents and clinicians have substantial knowledge of children’s health, complicating the epistemic landscape of the interactions (e.g. Heritage, 2012). However, the type of knowledge varies, and this is further complicated when it comes to deciding whether and how to change caregiving behavior in the home (Heritage and Lindstrom, 1998; Heritage and Sefi, 1992; Ranzani, 2024; Stevanovic and Peräkylä, 2012). The inherent tension that exists between two natural experts over the child’s well-being is visible anytime a concern manifests by one party but not the other. In the American context, a physician is the primary clinician whereas in the European contexts for similar monitoring visits, the clinician may be a nurse.
While researchers continue to find that physician medical authority is visible across clinical contexts, there are nonetheless hints in physician communication that they are oriented to a need not only to offer their conclusions but also to persuade parents to see it that way. For instance, researchers note shifts to less presumptive language in treatment recommendations (e.g. Opel et al., 2013; Stivers et al., 2018). The jury is still out on whether presumptive language is itself persuasive or is simply more often used with families who are already buying into recommendations, but the fact that physicians are deploying a variety of treatment recommendation formats suggests that they recognize the need to secure patient compliance but to do so in a way that is sensitive to maintaining or even fostering patient participation (Stivers and Timmermans, 2020).
Scholars also consistently find more frequent displays of physician accountability than in the past (e.g. Maynard and Turowetz, 2017; Peräkylä, 1998). One unexpected way that this manifests is when physicians provide patients with insight into their examination findings through ‘online commentary’ (Heritage and Stivers, 1999). In cases of viral upper respiratory conditions, for instance, no-problem online comments such as his ears look good or no sign of infection in her throat lay the groundwork for no-problem diagnoses which help remove some potential bases of parent resistance (Heritage and Stivers, 1999). In well-baby visits, clinicians also commonly provide direct access to infants’ vitals including height, weight, and head circumference, providing a basis for subsequent assessments of normality (Ranzani, 2023).
In other domains such as diagnosis and treatment, physicians sometimes provide accounts for their diagnoses or treatment recommendations. In doing so, physicians orient to the relevance of displaying a rationale for their thinking and recommendations. Such explanations are associated with reduced medical authority precisely because they offer patients insight into the thinking behind the physician’s position (e.g. Stivers and Tate, 2023). In this paper, we see that a growth chart (and how the participants transition to discussing it) can become an epistemic resource for persuasion, similar to the articulation of a child’s physical signs in online commentary (Heritage and Stivers, 1999). In this way, we show that the way an activity transition is done can also contribute to physicians’ displays of authority.
Data and method
This study draws on 327 video recordings of well-child visits that occurred with 14 pediatricians in five separate clinics in Southern California. Visits included babies between 2 and 20 months old who were being seen for routine visits between December 2019 and October 2021. All visits were conducted in American English, and parents provided informed written consent to the recording of the visits. In 290 of these visits (89%), physicians showed parents the electronic growth chart on their monitor as part of explaining the baby’s physical development.
In these clinical encounters, parents and children are brought into one of the clinic’s examination rooms by a medical assistant. That assistant asks parents to undress the babies. Once that is done, babies are weighed and measured. Data are entered into electronic medical records, and parents are told that the physician will be in shortly. Physicians have access to medical records but rarely review them before entering the examination room. Most commonly they move from one examination room to the next. However, as they ask opening questions, we observed that clinicians commonly skim the chart looking for any red flags or concerns, and this can include the growth chart. This was not specifically recorded and due to the angle of the camera, we have inconsistent access to whether and when physicians look at the data entered by the medical assistants. Our focus was when clinicians turn to the growth chart as the primary activity.
Consistent with principles of conversation analysis (CA), we approached the question of how participants transition into a discussion of physical development by looking for points of similarity and difference in the various interactional activities in these visits (Sidnell & Stivers, 2012). From there we identified the two primary practices for transitioning into this environment (disjunctive and conjunctive) and focused on how the contexts of these respective transitions differed (in the context of parent/physician concerns or not).
Once we identified the two transition types and the primary context difference, we operationalized these for structured coding in order to assess the robustness of the patterns we found using CA. This would also allow us to identify potential deviant cases for further analysis (Stivers, 2015). Specifically, we coded all 290 visits for who initiated the transition to the physical growth activity; which of the two types of activity transition (disjunctive or conjunctive) they relied on; and whether the transition occurred in the context of a concern or not, whether by parent or physician.
Analysis
As mentioned earlier, during well-baby visits, physicians assess many aspects of children’s development. Our interest is in the process through which physicians transition into reporting and assessing children’s physical growth. We considered an initiation to be a statement or question about growth. For instance, turns like ‘Let me show you her growth’; ‘Do you want to see her growth chart’; or, from the parent, ‘How’s her weight doing?’. Transitions are most commonly initiated by physicians (90% of the time, n = 262). Parents occasionally initiate the transition, usually by asking about growth (10%, n = 28), but both physicians and parents consistently orient to this as dispreferred. Parents orient to this through accounting for bringing up a transition or marking it as out of place; physicians orient to the dispreference through treating the initiation of the transition as ill-timed.
Physician-initiated transitions are usually done disjunctively (79%; n = 206). In what follows, we focus on these transitions. We begin by illustrating the two main ways physicians transition to assessing physical growth and then turn to the contexts in which these transition types are relied on.
Types of activity transition
As mentioned, by disjunctive, we follow Stivers and Sidnell (2016) in operationalizing this as a highlighted boundary between the prior activity and sequence relative to the growth assessment. (1) offers an example of a prototypical case. Prior to (1), the physician reviewed many aspects of the child’s health and development including most recently whether the parents have started brushing her teeth and the need to visit a pediatric dentist, then turning to who is caring for the child during the day. Line 1 represents the last topic in this updating activity before the shift to discussing growth – the presence of siblings in the household.
In the previous activity, the physician mostly focuses her eye gaze on the computer screen while typing, shifting her gaze toward the mother occasionally (lines 5–7). Evidence that the transition is best understood as disjunctive is first that the prior sequence and activity are brought to possible closure at line 7 with the physician’s positive sequence closing third assessment (Schegloff, 2007). A second form of evidence is that there is a 9-second silence where the physician is typing, breaking all eye contact with Mom. The clinician then treats this as the conclusion of the previous activity with the sequence closing third ‘Alright’ in line 9. While Beach shows that both Okay and Alright can mark activity transitions, he suggests that the latter is stronger (Beach, 1995). Taken together, we see the prior activity strongly boundaried off from the growth assessment.
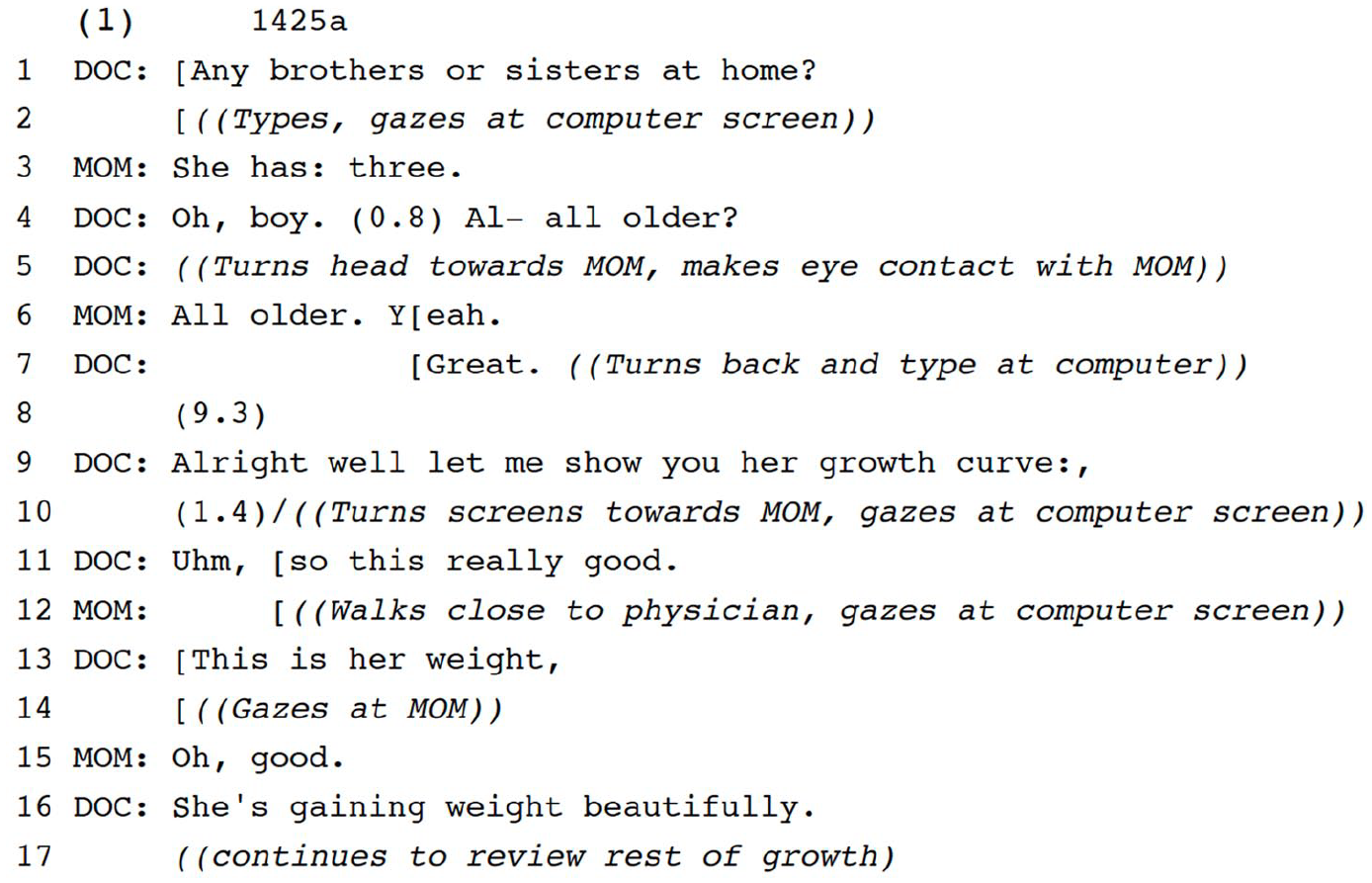
The growth activity begins with the preface ‘Well’ which has been found in first position actions when there are topic shifts like this one (Heritage, 2015). In this case, the shift is from an activity where the physician was soliciting information from the parents about the child’s development to an activity where the physician is providing information about the child’s growth. Thus, consistent with Heritage’s findings about ‘Well’ prefaces, here we see a clear topic and activity shift. Finally, in the actual move to share the growth chart with ‘Well let me show you her growth curve:,’ there is no additional work to link back to the prior topic of siblings. Thus, through the marking of prior activity closure, silence, and two vocal boundary markers, the growth activity is treated as disjunctive with the prior discussion.
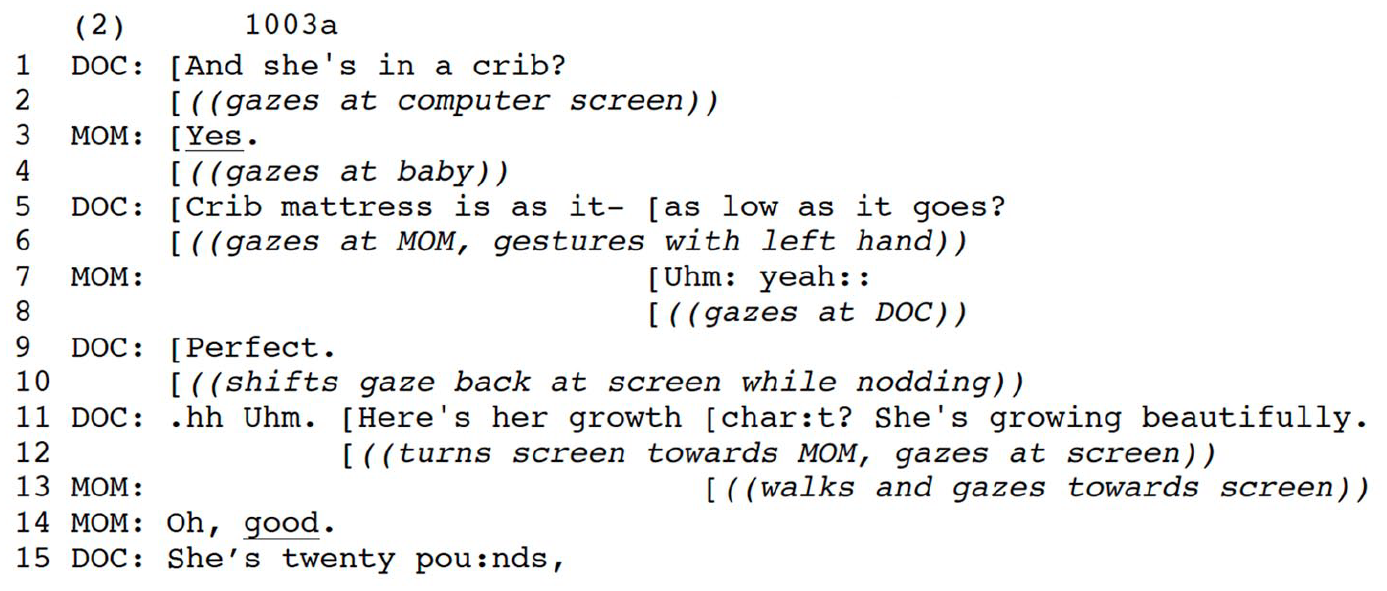
A second case of a disjunctive activity transition is shown in (2). While (1) has silence which does extra work to distance a previous activity from a next, silence is not criterial. What matters for a disjunctive transition is that a boundary is oriented to between the prior and next activities. In (2), the physician initiates a sequence in line 1, part of a series of questions on sleep habits. The And-preface marks this as the next question in a series (Heritage and Sorjonen, 1994). After the base question is answered, the physician expands the sequence requesting confirmation that the mattress is ‘as low as it goes?’ which is confirmed in line 7. Like (1), we see that the prior sequence is marked as complete with the positive sequence closing third assessment (line 9) (Schegloff, 2007). In this case there is no silence and no verbal preface, but the new sequence is initiated with an audible in-breath and an ‘Uhm’, both of which build space between the prior activity and the next (line 11). Once again, in line 11 when the physician launches the growth discussion, the announcement ‘Here’s her growth char:t?’ does no work to link to a prior topic or activity.
Across (1)–(2), there is a boundarying off of the previous sequence and activity drawing on lexicon, body orientation, silence, vocal delay, and audible in-breaths. These resources help to project that the new growth discussion activity should be understood as disjunctive with what has come just before. While there is variation in how distinctly boundaries between previous activities and growth activities are constructed, as can be seen if we contrast (1) and (2), disjunctive cases look distinct from conjunctive cases because instead of constructing and highlighting a boundary between two activities, physicians blur the boundary such that the two activities become interwoven.
Conjunctive cases account for 21% (n = 56) of cases in our collection. In (3) they are discussing feeding when Dad brings up that they have not increased the amount of milk his daughter is receiving despite her now being 4 months old and growing. In lines 9–11 this is turned into a question of whether to feed her more with the dubitative marking ‘wasn’t sure if’ (Riccioni et al., 2018).
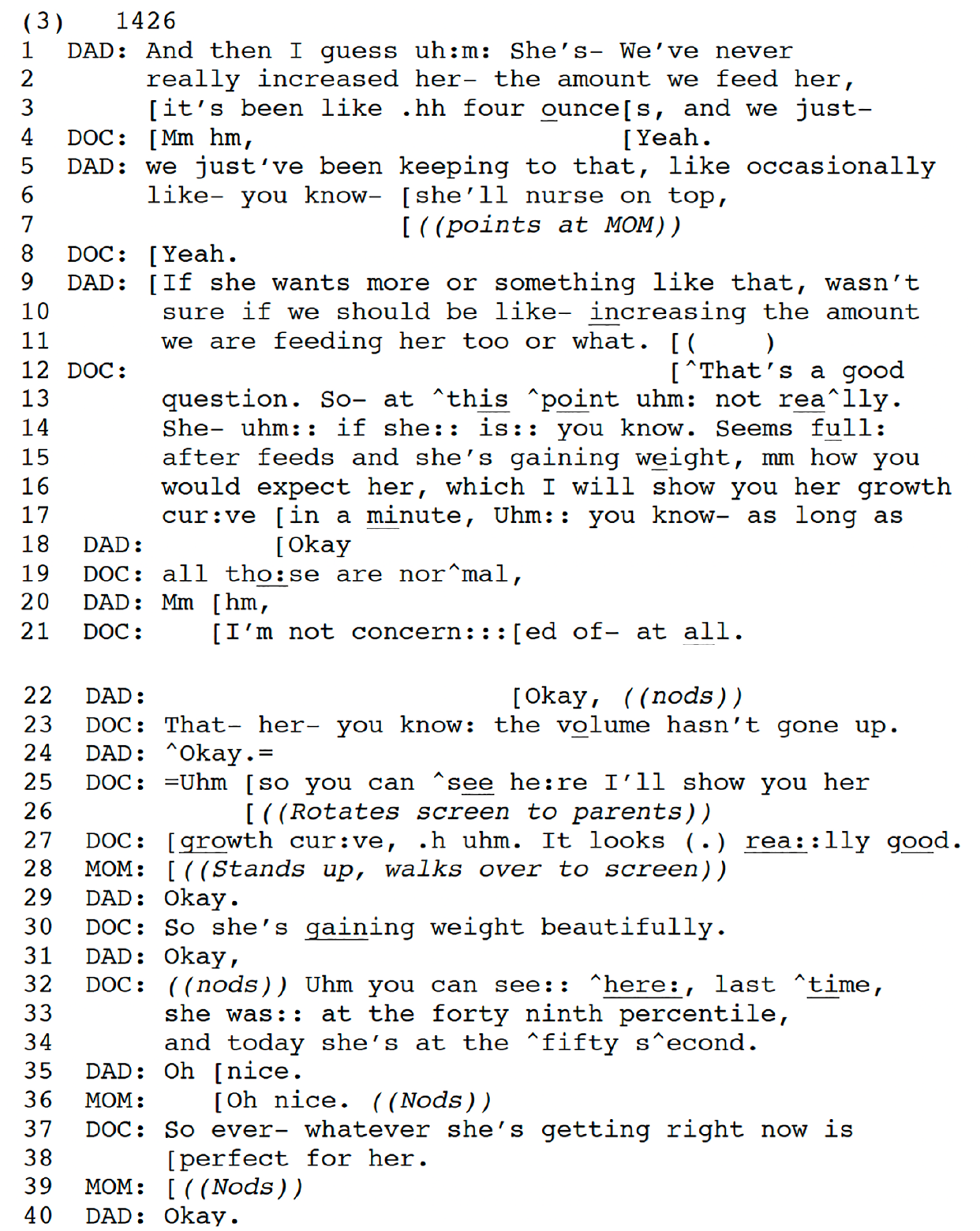
The physician first answers Dad’s question with a transformative and qualifying So- at this point uhm not really (line 13) (Stivers and Hayashi, 2010) but then expands this with two contingencies for her position: if the baby seems full and if she is gaining weight as expected, then her milk intake is no cause for concern. We focus on how, in lines 16–17, the physician blurs the boundary between this question sequence and the growth assessment activity. Specifically, she invokes the next activity while still answering the question with Which I will show you her growth curve in a minute (Mazeland, 2007) and treats the growth chart as an opportunity to address the contingency of weight gain. Then, in overlap with So you can see here I’ll show you her growth curve, the physician rotates the screen which makes it more visually accessible to the parents and invites their joint attention (lines 25–27). This physical change is done while the physician is still addressing Dad’s concern about feeding.
During their discussion of feeding, the physician projects that looking at the growth chart will be part of the activity of making sure that there is no reason for concern (line 16). The So-preface in this case marks this as a resumption of that in line 25 (Bolden, 2006). Yet, across this transition we see that the boundary between the feeding discussion and the growth discussion is blurred, not highlighted. Rather than boundarying off a discussion of eating from a discussion of growth, growth is explicitly connected to eating with So.
Once looking at the growth chart, the physician assesses the baby’s growth in line 27 with initiated It looks really good and asserts So she’s gaining weight beautifully in line 30. The physician adds further details before returning to her response to the father’s question when she says So whatever she’s getting right now is perfect for her (lines 37–38), making explicit with the upshot version of ‘So’ that this is the inference to be drawn from their discussion that allows her to finally answer the father’s question (Raymond, 2004; Schiffrin, 1987). Thus, the evaluation of the child’s growth is treated as part of answering the father’s question rather than as a disjunctive activity from that question and the physician’s answer. The physician could have simply answered the question that their current practice is fine and then disjunctively moved into the growth assessment similar to cases (1)–(2). Instead, the transition in (3) is blurred, being constructed as part of the response.
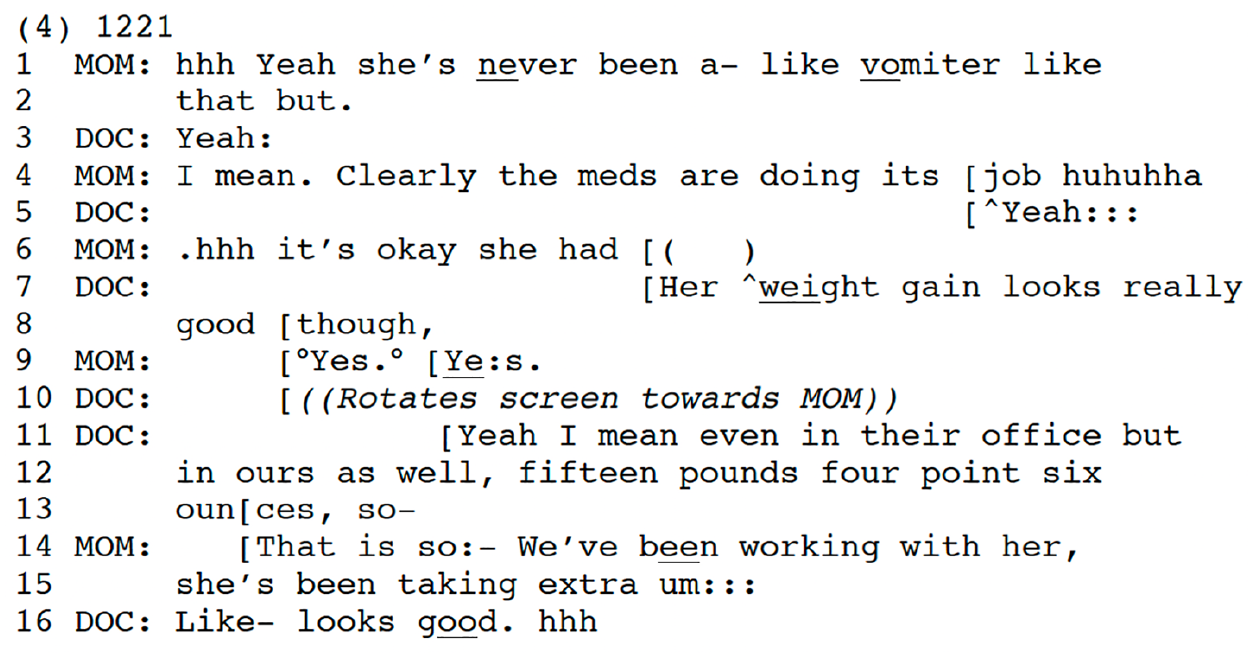
In (4), we see another illustration of a conjunctive activity transition. This 6-month old girl is under the specialty care of a gastrointestinal physician. Recently, that physician suggested reducing medication that the baby has been taking to aid digestion. That reduction did not work well, and she began vomiting, which, in hindsight, demonstrated the effectiveness of the higher dosage of the medication at controlling vomiting (lines 1–4). In the context of Mom’s mention of significant vomiting, the physician states that Her weight gain looks really good though (lines 7–8). Again, this begins the next activity (growth) while addressing a concern in the previous activity of updates about feeding and medication. The boundary is again blurred. There is no closure of the previous activity, and Mom is still talking about this (line 6). The physician’s use of the contrastive marker ‘though’ in turn final position clearly indicates that this is addressed to what has come before regarding the child’s vomiting. Thus, the physician builds a connection between the prior activity of managing the child’s eating and vomiting and the current growth discussion.
In this section we established the two main ways that physicians transition into the activity of assessing children’s growth. We showed that in disjunctive transitions, the most common type, there is a highlighting of the activity boundary such as closing down the prior sequence and activity with a sequence closing third, silences before the transition to the new activity, prefaces, or audible in-breaths. In contrast, in conjunctive transitions, although the same embodied work is going on to engage parents in joint attention to the child’s growth chart, there is work to blur the boundary between the prior activity. This can involve different prefaces or other contrastive lexical items or through the introduction of the child’s growth chart in a way that is interwoven with an ongoing discussion. Prior sequences in these transitions are rarely closed with sequence closing thirds, but instead are often expanded into the growth chart activity.
The contexts of use for conjunctive and disjunctive transitions
We now turn to when physicians rely on disjunctive and conjunctive transitions. Physicians consistently build transitions as conjunctive when addressing concerns. In (1)–(2), the activity transition was disjunctive, and there are no parent or physician concerns. However, we see concerns in (3)–(4) where the transitions were conjunctive. We argue that when physicians blur the transition, they leverage the growth chart to build a more persuasive case relative to a problem or concern that has been introduced. When there is no concern, physicians are more likely to address the question (whether it is about feeding, sleeping, mobility, or language) and then move to the growth chart disjunctively.
In Table 1 we see that this pattern is robust across the data: Transitions that are done in a conjunctive way are much more likely to be preceded by concerns than those that are done in a disjunctive way.
The relationship between transition type and concerns.
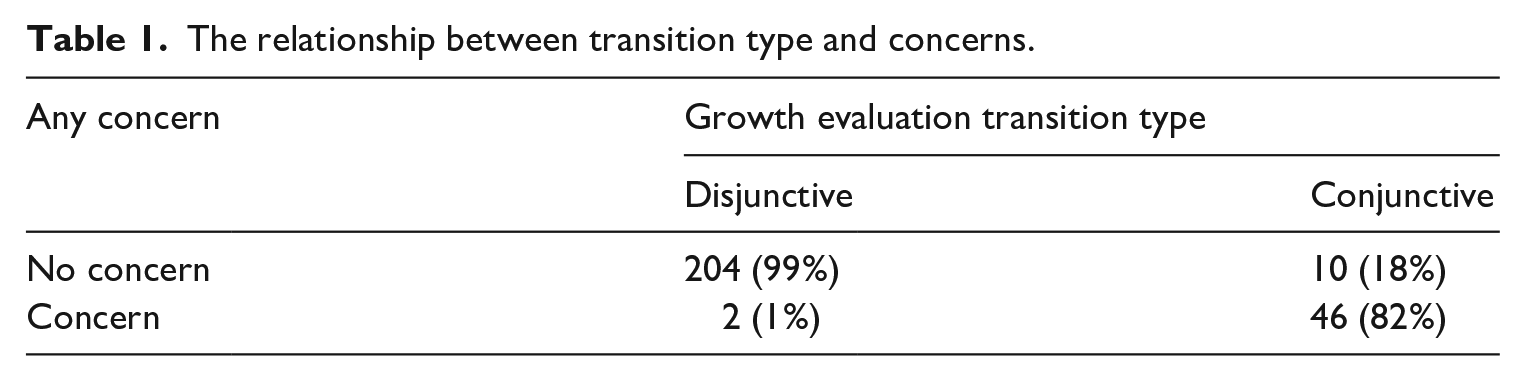
Of the 56 cases in which physicians presented the growth chart in a way that was conjunctive to the just prior activity, 82% of them involved a concern. In contrast, of the 206 cases where physicians transitioned to the growth evaluation in a disjunctive way, only two of these involved a concern. This difference was statistically significant (χ2(1) = 193.8714; p < 0.001). The vast majority of the concerns presented are parents’ (88%; n = 42 vs 12%; n = 6), so the most typical situation is that physicians are addressing a parent’s concern although at times physicians may be working to convince a parent that s/he should be concerned. Returning to (3) and (4) we can see data internal evidence that concerns are implicated in the transition type. In (3) the father introduces that they have not increased the amount of food they are giving their daughter and are unsure about whether they should do so. This is the last topic before the growth chart discussion, and the physician relies on the growth chart as an epistemic resource to address this concern and specifically to bolster her position that there is no need to increase the amount of food they are giving their daughter. The blurred transition aids the physician’s presentation that she is ‘not concern:::ed of- at
In (4), the mother has recounted that following a reduction in medication, her baby began vomiting. She contrasts this period with her daughter’s normal behavior in lines 1–2, that ‘she’s
If we consider the additional work that physicians are doing across the transition, in the disjunctive cases there is an absence of persuasive work – work to convince parents that their child has no problem and there is no cause for concern (or, occasionally, that there is cause for concern). Rather, in disjunctive cases, there is only an assessment of the length, weight, and head circumference.
Potentially deviant case
In the prior section, we argued that physicians rely on conjunctive transitions primarily when they are addressing a concern. Returning to Table 1, we can see that there are occasionally cases that do not follow this pattern. In this section, we examine one of these seemingly deviant cases. We argue that these cases reveal a more fundamental explanation: physicians rely on conjunctive transitions in contexts where they have made a claim for which the growth chart can be leveraged to persuade parents. In (5) the father asked how many meals they should be feeding their son who is there for his 9-month check-up. As the physician responds, he explains that by 9 months ‘it’s getting closer to balance’ meaning half solid foods and half breast milk. The transition to discussing his growth is blurred when he says Uh for you guys I’m not worried about him cuz he’s growing (lines 8–9) and then just after that he says Uhm let me show you the picture real quick just so you can see (lines 12–13). Like our other conjunctive cases, this one too uses a question about feeding to begin the transition to the growth chart, blurring the boundary and without having clearly closed the prior activity. However, unlike (3)–(4), neither the parent nor physician has expressed any concern (typically leading to a disjunctive transition).
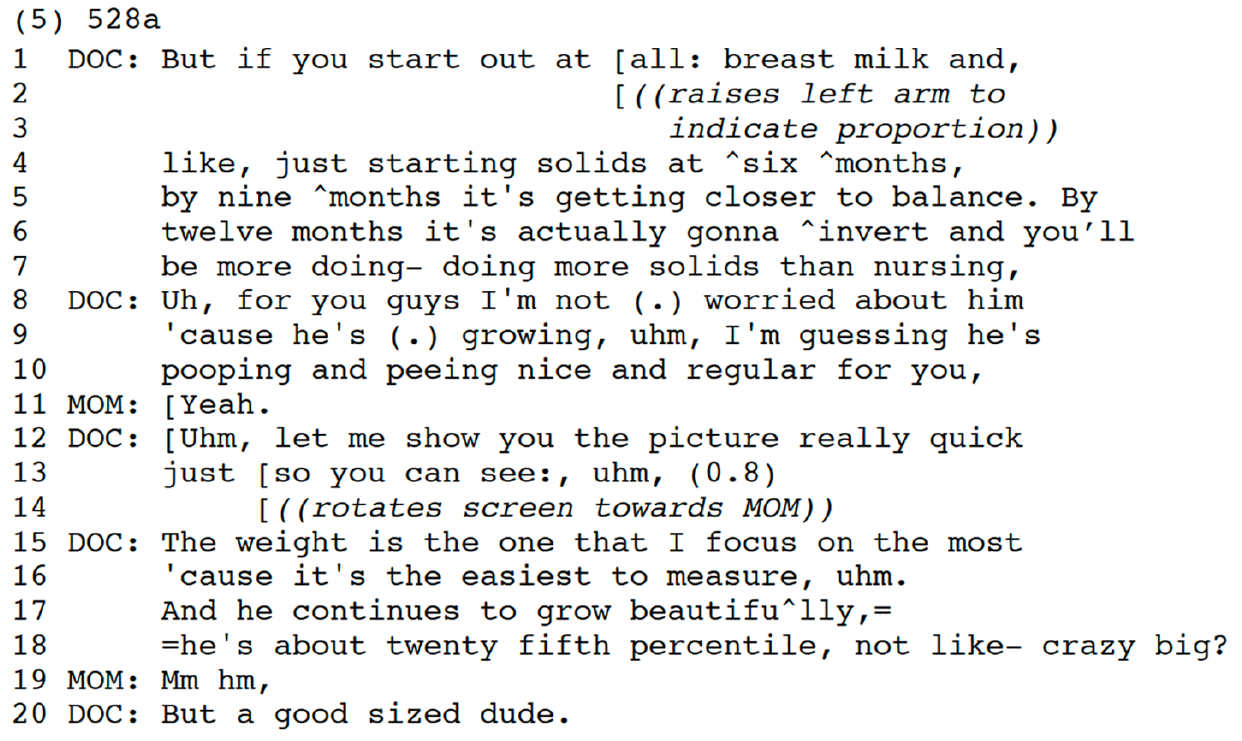
Even though conjunctive transitions are primarily used in the service of responding to concerns, in this case even in the absence of a stated concern, we see support for our primary analytic claim that the growth chart is being leveraged to persuade parents of the physician’s position with a conjunctive transition. Normally, persuasion is invoked in the context of a concern, but as we see here, the physician is laying out a plan to gradually increase the amount of solid food in this infant’s diet. This position is preceded with the reason for him showing the growth chart as ‘just so you can see:,’ (line 13) which orients to a logical argument he is making for which he wants parent buy-in. His position is reinforced by his appeal to the growth chart showing that he ‘continues to grow beautifu^lly’ (line 17) and that he’s ‘a good sized dude.’ (line 20).
Discussion
In this paper, we documented that in most cases of well-child check-ups, pediatricians shift between a previous activity and the activity of assessing the child’s growth with a clear and disjunctive boundary between the new activity and what came previously. In these cases, physicians rely on closure of the prior sequence (e.g. assessments), silences between turns, and turn prefaces to mark off the growth activity. In contrast, we showed that physicians only sometimes weave their activity transition to the growth chart into the previous activity (e.g. addressing a parent question) and rely on lexical items that link the growth chart discussion to previous discussions (e.g. ‘though’), constituting a conjunctive activity transition.
We argued that clinicians rely on conjunctive transitions in contexts where there is a tension between a concern that the parent has and a lack of concern by the physician. Here, they can leverage the growth chart to persuade parents of the physician’s position such as that the child’s food intake is adequate or that the vomiting is not detrimental to the child receiving adequate nutrition. Evidence for this claim came from the frequency with which conjunctive transitions occur in environments where there was a concern in the just prior activity that physicians address through the growth chart as well as the qualitative evidence that the growth chart is being mobilized to bolster physicians’ positions. A deviant case further revealed that while concerns are the most common basis for interweaving the growth chart assessment and the prior activity, this same pattern can be found in cases where physicians are leveraging the growth chart to bolster their positions, whether that is rooted in disputing a parent’s concern, addressing parent resistance, or making a stronger case for something the physician believes.
This paper extends research on how participants jointly accomplish activity transitions. We add to work examining activity transitions in healthcare (Maynard and Turowetz, 2017; Robinson and Stivers, 2001) and further contribute to our understanding of how speakers build activities as more or less connected through their transitions. We see that while the embodied behavior is similar across the two main types of transitions, participant reliance on a variety of resources can increase or decrease the separation between the two activities. We extend this line of research on transitions by exploring the ends to which physicians use these conjunctive transitions.
Activity transitions might not be the first place we would expect to find persuasive work, but the fact that a child’s growth measurements can be leveraged for persuasive purposes in physicians’ interactions with families suggests that we should further explore the varied ways in which physicians draw on information in the medical record for bolstering their positions in medical visits. Moreover, we should examine other activity transitions not only for how they are accomplished but also for what this way of accomplishing the transition facilitates for participants.
Our study also contributes to the literature on medical authority, agency, and accountability in clinical communication. The epistemic access afforded by physicians sharing the medical record in these cases is somewhat analogous to physicians’ use of online commentary in physical exams. In both cases, the physician gives parents access to findings they might not otherwise know. Specifically, when a physician tells the parent what she sees in the ear, she makes it at least partially accessible to the parent. When the physician tells the parent what the child’s growth metrics are, parents then have access to this as well. In both cases, this access facilitates parent engagement. However, in both of these cases, it also works to fend off potential or actual threats to medical authority in the form of parent resistance (e.g. to a no-problem diagnosis) and helps persuade them toward the physician’s position (Heritage and Stivers, 1999; Stivers and Timmermans, 2020). If the physician has told a parent that the ears, nose, throat, and lungs all sound fine, then it becomes harder to resist when the physician subsequently diagnoses the child with a self-limiting viral infection (Heritage & Stivers, 1999). In our case, physicians draw on evidence of the child’s growth to support a claim that the child is fine (or, occasionally, in need of something additional).
Finally, although parents have primary epistemic rights over what the child has been doing at home, physicians have primary epistemic rights to tell parents about their child’s growth and their status relative to other children through their various percentiles (Heritage, 2012). This offers a site for future research since it can become a potential source of conflict when parents mobilize their knowledge of their children’s behavior at home, but physicians mobilize growth chart measurements to dispute parents’ concerns. While reliance on medical authority may vary, physicians are generally relying less on a paternalistic brand of medical authority complete with accounting for recommendations and diagnoses and a greater provision of epistemic access (e.g. Peräkylä, 1998). This paper’s findings illustrate another way in which patient access becomes a resource for working to secure parent buy-in rather than presuming it.
Footnotes
Acknowledgements
Thank you to Andrew Chalfoun, Steve Clayman, Keith Cox, Lor Martin, and Giovanni Rossi for their comments on an earlier draft of this paper. This project was presented at the 26th Annual Conference on Language, Interaction, and Social Organization (LISO) and the 117th Annual Meeting of American Sociological Association (ASA). Thank you to those who asked questions or provided comments.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed consent
This study was approved by the relevant Human Subjects’ Protection Committee and all participants provided written informed consent.
IRB
Due to IRB restrictions, video data are not publicly available.