
Abstract
Patient participation is a fundamental principle in modern Western health care, but not necessarily simple to achieve. During hospital ward rounds, patient participation is further hindered by the multi-party nature of the encounter: at times, members of the medical team talk with each other rather than with the patient. This article examines patients’ opportunities to participate in ward round conversations when the patient is not the addressed recipient. The data consist of 3 hours of video-recorded ward rounds in a Finnish hospital. Using conversation analysis, we study patients’ practices for getting a turn in different sequential environments. The patients monitor the ongoing conversation and exploit its sequential organisation by producing responsive turns and repair initiations, thus becoming active participants. They also produce their own initiatives, although sequential and multimodal constraints affect their possibilities for modifying the participation framework. The results of this study can be exploited to promote patient participation.
Keywords
Introduction
Patient participation 1 has been a key concept in healthcare policies throughout the Western world for the last few decades (Collins et al., 2007; WHO, 2013). Patients’ participation in the planning of treatments and decision-making is considered, for example, to increase the quality of care and contribute to patient safety (Weingart et al., 2011). However, the prerequisites, manifestations and stakes of patient participation vary greatly, according to different medical situations. The relevance of different forms of patient participation eventually depends on the objective of the encounter in question (Peräkylä et al., 2007: 140). Consequently, the practices for securing or increasing patient participation in healthcare interactions need to be adapted to the specific tasks at hand; no generally applicable approach to patient participation suits all situations (Keel and Schoeb, 2017a: 130–131). This paper explores patient participation as the patient’s opportunity to participate in conversation in a specific medical context: hospital ward rounds.
Even though patient participation is a fundamental tenet on a policy level, difficulties in achieving it in practice in different situations have been reported in many studies (see, e.g. Collins et al., 2007). The doctor’s rounds on a hospital ward comprise a significant and challenging situation from the point of view of patient participation, and there is not yet enough research on how patient participation is organised in and through interaction during actual rounds (see, however, Redley et al., 2019). Ward rounds provide an opportunity for the patient to meet the doctor and discuss the treatment with them; thus, they represent an ideal opportunity to involve patients in their care decisions. However, ward rounds have often been criticised for a lack of patient-centredness (Busby and Gilchrist, 1992; Swenne and Skytt, 2014; Walton et al., 2016). Previous research has reported that the patient-specific session during ward rounds remains brief, while a significant amount of time is spent at the organisational level (Mattila et al., 2017: 1). The fact that medical professionals cannot spend a lot of time with each patient has led to a question of whether patients receive adequate information from their doctor and whether they are able to participate in the decision-making concerning their treatment (Mattila et al., 2017: 4).
In addition to the time constraints imposed on medical staff (see also Oxelmark et al., 2018: 616), the participation framework (see Goodwin and Goodwin, 2004) of the ward round conversation sets further challenges for patient participation. Rounds consist of different phases, each creating different opportunities for the interlocutors to participate. First, there are phases that represent dyadic interaction between the doctor and the patient (Weber et al., 2007: 346). These phases resemble an interview: the patient is given a slot in which to participate, mostly by answering the doctor’s questions, similarly to many other dyadic medical encounters. Patient participation has already been studied in terms of doctor-patient interactions and other dyadic healthcare encounters (e.g. Collins et al., 2007; Ijäs-Kallio, 2011; Jones, 2009). In particular, doctor-patient consultations and the phases they contain have been well described in the literature (e.g. Heritage and Maynard, 2006), and the patients’ opportunities to participate have been examined in relation to them (Robinson, 2003).
In contrast to dyadic doctor-patient interaction, ward rounds involve multiple participants with different rights, obligations, epistemic access and responsibilities, and the participation framework is constantly negotiated between the interlocutors. The doctors may want to check something in the patient’s medical record, or they may begin considering relevant future procedures (e.g. changing the medication). These phases often include some involvement of the members of the medical team, and hence the participation framework becomes more complex. As has been reported in other multi-party medical settings, medical professionals “might orient toward each other and talk about the patient instead of addressing him or her as an active participant” (Keel and Schoeb, 2017b: 216; original emphasis). It has also been noted that during ward rounds, patients are “locked out” of the conversation (Oxelmark et al., 2018: 616). The participation of an individual participant is more challenging in a multi-party conversation in general: all parties are not guaranteed an opportunity to be the next speaker (Sacks et al., 1974). In addition to this, the participation of the patient can be hindered by the medical jargon used by the professionals (Oxelmark et al., 2018; Swenne and Skytt, 2014), or simply by the fact that the patients themselves may want to take a passive role (Oxelmark et al., 2018; Redley et al., 2019).
If we want to better understand the interactional constraints of patient participation, it is necessary to study in detail the interactional organisation of different medical encounters (see also Robinson, 2003). Using conversation analysis as a method, this article tackles patient participation in ward rounds during instances where the participation framework has grown to include other members of the medical team and the patient is not an active participant. The precondition for patient participation in these situations is for the patient to get their voice heard in the interaction with medical professionals (Schoeb et al., 2019). This study shows how patients manage to get a turn and in that way become active participants in the conversation. We investigate how patients use both conversational organisation and material/embodied resources to get a turn in a situation where they are not selected as the next speaker.
Data and method
The data of this study consist of approximately 3 hours of videotaped rounds on a surgical ward in a large Finnish hospital. Patients were admitted to the ward from the emergency clinic, and after acute care they were either discharged or provided a referral to other services. The data was recorded in 2016–2017. The recordings were transcribed using the conventions of conversation analysis (slightly adapted from Jefferson, 2004, and Mondada, 2016; see Appendix 1 for the transcription symbols). All names and other identifying information have been omitted to ensure anonymity. A research permit was granted by the local research committee and informed consent was obtained from all participants.
The medical team that performed the rounds usually consisted of the consulting doctor (a gastroenterologist), a specialising physician (a junior doctor specialising in internal medicine), the charge nurse (a senior nurse overseeing an entire ward) and a nurse (the primary nurse of each patient). The data contain bedside consultations of 29 patients; a total of two consulting doctors, three specialising physicians, one charge nurse and thirteen nurses participated in the study. Typically, a bedside consultation lasted 3–6 minutes.
The method used in this study is conversation analysis (CA; for an overview, see Sidnell and Stivers, 2013). With CA, it is possible to examine on a micro level how people mobilise different linguistic and embodied resources and practices in order to perform various social actions. CA has often been applied to study professional interaction since it can be used to challenge and complete professionals’ own ideologies about interaction (Peräkylä and Vehviläinen, 2003). In this way, CA findings can be used in making doctors and patients more aware of their actions, which contributes to improving health and healthcare (Pilnick et al., 2010).
Getting a turn: The participation framework and selection of the next speaker
Multi-party interaction involves constantly changing roles of speakers and recipients. The concept of participation framework was first introduced by Goffman (1981: 131–133), who discerned the different statuses of a recipient of an encounter by differentiating ratified participants from bystanders and the addressed recipient from unaddressed ones. Later, CA studies have further developed the concept by extending it to also cover the speaker role. The categories of speaker and recipient are dynamic and constructed in interaction; the processes of participation modify the talk, and the talk in turn modifies the participation framework (Goodwin and Goodwin, 2004).
Moreover, the participation framework is not constituted merely through talk but also through embodied means: the positioning of participants’ bodies towards each other and the environment establishes a public, shared focus for the organisation of attention and action (Goodwin, 2007: 61). The importance of the spatial disposition of the participants’ bodies is also illustrated in the work of Mondada (2009, 2016) on the multimodal arrangement of a mutual focus of attention and the creation of a common interactional space. Interactional spaces are transient by nature, being sustained and modified by participants’ body orientations, gazes and gestures.
The alternation of static phases and transitions of the embodied participation framework is connected to the changing activities the participants are engaged in. The embodied resources and the physical environment enable the participants to subtly anticipate and negotiate transitions between different activities in order to maintain a smooth progress of interaction (Helisten, 2018). This is especially important in multi-activity situations, where the participants are involved in several activities at the same time or when several parallel, overlapping actions compete for the participants’ focus of attention.
Another aspect of participation is the selection of the next speaker in a conversation. The description of the organisation of turn-taking is one of the cornerstones of CA. The basic principle is that the current speaker can select the next speaker in any transition-relevance place; if this is not done, one of the participants can select themselves (Sacks et al., 1974). In a multi-party conversation, the selection is more complex than in a dyad, and the next speaker can be indicated, for instance, by using an address term or directing one’s gaze towards the selected person (e.g. Lerner, 2003). There are also more tacit ways of selecting the next speaker. For example, the register of the language used in the turn or the epistemic status of the participants can indicate to whom the turn is directed (Lerner, 2003).
If the current speaker selects the next speaker, it is usually this person – and not the other participants – who has the right and the obligation to take the next turn (Sacks et al., 1974: 704). However, sometimes responses from non-selected recipients are provided and not treated as violations of the turn-taking system. This can be due, for instance, to problems in the progressivity of the interaction (Stivers and Robinson, 2006), but there may also be other factors affecting the choice of the speaker in situations where more than one respondent is able to provide an answer (Lerner, 2019; Stivers and Robinson, 2006: 388).
In this paper, we will investigate how the patients get a turn in ward rounds, especially outside the dyadic phases between the patient and the doctor. We will demonstrate how the patients exploit the conversational organisation in order to get a turn in multi-party situations where they have not been selected as the next speaker. Firstly, we will investigate instances where the patient produces a second pair part of an adjacency pair (Sacks, 1992), even though the first pair part is not directed at them. Secondly, we will illustrate how the patient can get a turn by producing a repair initiation on something that the medical team discusses. Finally, we will discuss instances where the patient produces (or attempts to produce) their own initiative.
Exploiting the preceding conversation
In this section, we will examine situations where the patient exploits the structure of the preceding conversation in some way to enter the conversation. These cases can thus be considered as reactive turns. Firstly, we focus on responsive turns, that is, cases where the patient produces a second pair part even though they have not been addressed recipients of the first pair part. Secondly, we will investigate cases where the patient produces a repair initiation concerning a trouble turn that has not been addressed to them.
Patient produces a responsive turn
When the patients are not addressed recipients in the ward round conversation, they can still take turns in different sequential environments. We will begin by examining situations where the patient produces a responsive turn (i.e. a sequentially timed second pair part), even though the first pair part has not been addressed to them.
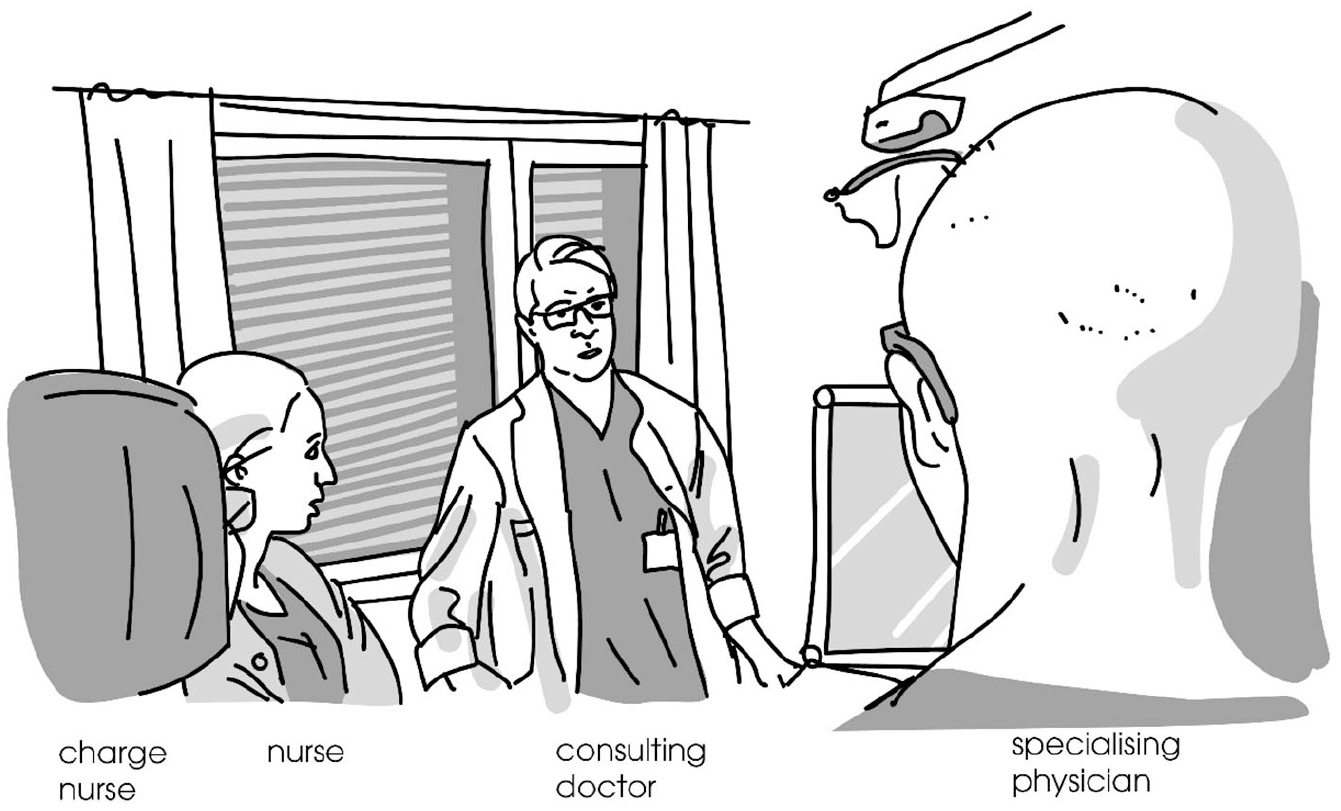
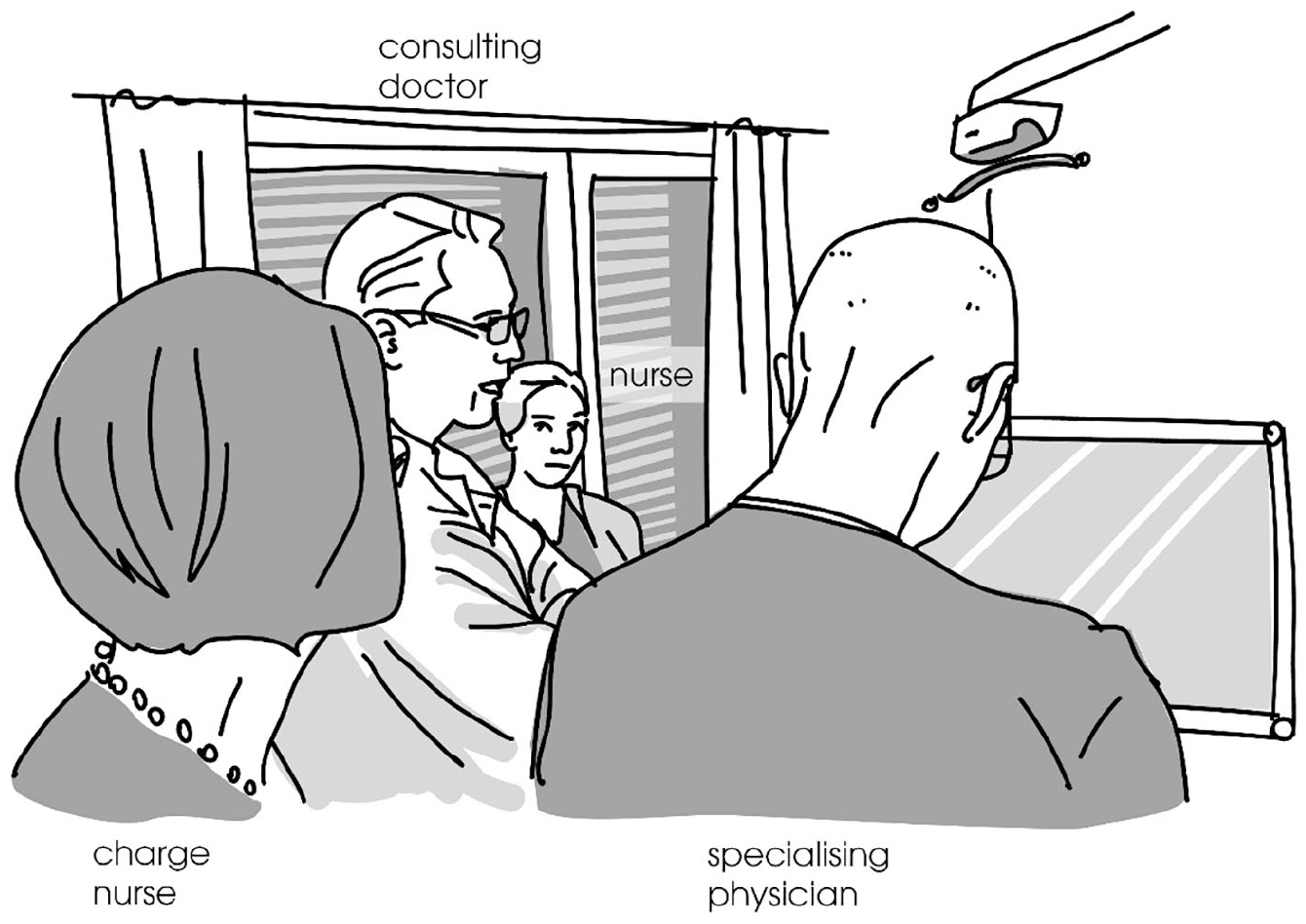
In Extract 1, the patient (P) lies in bed, the consulting doctor (D) is standing next to the bed, the nurse (N) is standing closer to the foot of the bed, slightly withdrawn to the side, and the specialising physician (SP) is at the foot of the bed facing the computer screen with the patient’s electronic file (see Figure 1 for a general illustration of the body positioning of the participants during the extract). Before the extract, the doctor has been palpating the patient’s abdomen and they have had a dyadic exchange about the patient’s use of alcohol. The doctor has just straightened her back, taken a step backwards from the bed and placed her hands behind her back.
Just before the extract, there is an embodied transition of activity: the doctor has ended the physical examination of the patient and moved away from him closer to the nurse. This distancing from the patient can be seen as a way to adjust the spatial organisation of the encounter in order to potentially enlarge the participation framework and include the other members of the medical team.
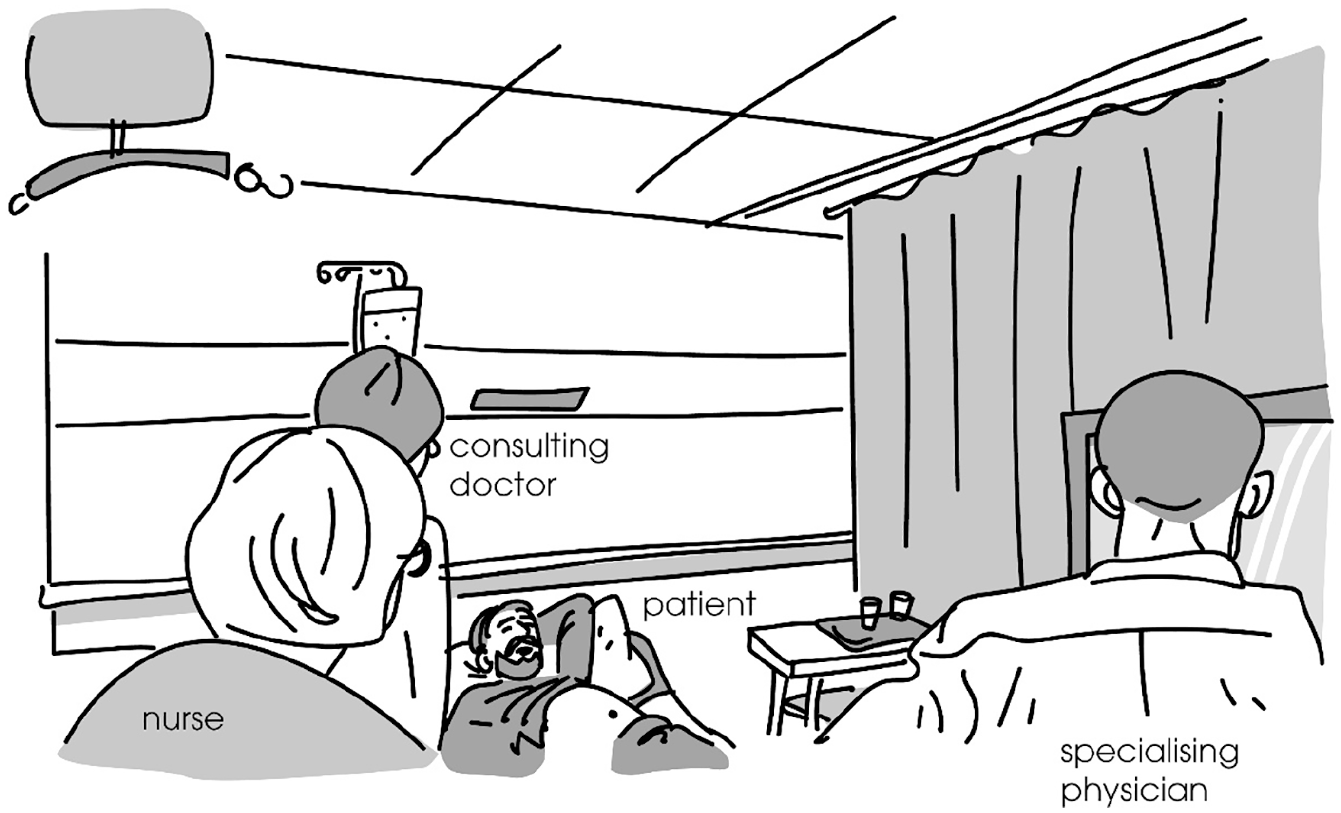
Body positioning of the participants during Extract 1.
The doctor now produces a hesitation particle tuota (‘um’) and then turns her head towards the drip-feed bottle. 2 The change of gaze direction anticipates a change of topic: the doctor is moving towards checking the patient’s fluid balance and nutritional state. She produces a statement about the patient’s food intake (line 1). The statement is, in a way, part of a list of constitutive elements that the doctor segues through during the round (consisting of respiration, urine excretion, etc.). This has an effect on the formulation: the turn begins with the key content, eating. The intonation rises in the end, which projects an upcoming continuation of the list and induces a (minimal) response from the recipients (Ogden and Routarinne, 2005).
The intonation inducing a response is in line with the fact that the doctor’s turn (line 1), although not grammatically formulated as a question, can be interpreted as a request for confirmation: it is a declarative sentence making a statement about a ‘B-event’ (i.e. something that the recipient has the right to know more about than the speaker) (Labov and Fanshel, 1977; see also Stivers, 2001). From an epistemic point of view, the next speaker could be either the patient or the nurse. The patient has primary epistemic access to the topic (Keel and Schoeb, 2017b): he has exclusive knowledge about not only what has been served but also what he has eaten and how he felt about it. Also, the nurse possesses first-hand information about the patient’s meals.
The doctor’s turn (line 1), however, is not addressed to the patient: she refers to him with a third-person pronoun hän (‘he’) (see also Keel and Schoeb, 2017b; Stivers, 2001). Also, at the end of the turn she turns her gaze towards SP and the screen. As far as the patient is concerned, there is thus no ambiguity about who is selected as the recipient of the turn and as the next speaker. Yet, in spite of the design of the doctor’s turn, it is the patient who produces the response, telling the doctor that he has just eaten (line 2). The patient’s response is also enabled by the fact that the doctor’s first pair part is clearly audible to the patient and denuded of professional jargon. He produces his response in a timely fashion, without there being any problems in the progressivity of the interaction (see Stivers and Robinson, 2006). The patient also displays engagement in the conversation by actively searching for eye contact with the doctor (lines 1 and 3). Following the patient’s turn, there is a pause (0.8 seconds, line 3), during which the patient turns his gaze to the doctor and the doctor turns her head towards the patient’s face. The doctor then confirms the patient’s response (line 4). Starting at almost the same time, the patient continues his turn and provides the doctor with supplementary information about his eating (line 5).
Extract 1 illustrates the flexibility of the participation framework during a ward round and the possibilities offered for patient participation by the structure of the conversation. The patient exploits the sequential structure of the interaction and his own epistemic status to produce a responsive second pair part in a situation where he is not selected as the next speaker (see Lerner, 2019). After his turn, the focus of the conversation is located between him and the doctor; he has thus managed to become an active participant in the conversation and his responsive turn is not treated as a violation of the norms of the interaction. By taking a turn, the patient increases his possibilities of making his own experiences and insights heard during the ward round. Even though the matter at hand is not of utmost importance to the patient’s care, his participation increases his agency in the situation.
Patient produces a repair initiation
As became clear from the previous section, adjacency pairs offer one environment for the patients to enter the conversation, even in cases where the first pair part is not addressed to them. In these cases, the patients produce a responsive turn (i.e. their participation is defined by the first pair part and thus complies with the initiative that is set by one of the medical professionals). Another way for patients to get a turn in a ward round discussion is through repair initiations. In multi-party conversations, repair initiations can be used to regulate the participation framework; they are a means for a non-active participant to join the conversation in a legitimate way (e.g. Egbert, 1997; Haakana et al., 2016: 285). When producing a repair initiation, one also exploits the preceding conversation to take a turn, but the action is less defined by previous turns than in second pair parts. In this section, we will examine repair initiations produced by patients in connection to trouble turns that were originally addressed to a third participant. In other words, with the repair initiation, the patient enters the discussion between two members of the medical team.
In the next extract, the doctor (D) has been examining the patient (P), who is lying on her bed, by asking her questions and then palpating her abdomen. While palpating, she has asked the specialising physician (SP) questions about the patient’s laboratory test results. Just before Extract 2, SP has mentioned a particular medicine that the patient has been given, and then reflected on the possible rationale for the prescription. While listening to SP, the doctor moves to the end of the bed to stand next to him in front of the computer station, and they both look at the screen. Figures 2 and 3 illustrate participants’ body orientations at specific moments of the extract (see transcript).
SP pursues his talk by pointing out bacterial growth (E. Coli bacteria) marked in the patient’s records (line 1). The doctor and SP continue their exchange (see Figure 2) on the urine test results until the doctor presents a conclusion: the patient has a urinary infection (line 7). This statement is made with a falling intonation, and the turn is followed by a relatively long pause (line 8). During this exchange, the patient is looking forward/down except for a very brief glance at the doctor (line 5). This could mean that she is planning to take a turn; looking towards participants of a conversation can be a means for a non-participant to prepare to join in (Tuncer, 2018; see also Ford and Stickle, 2012).
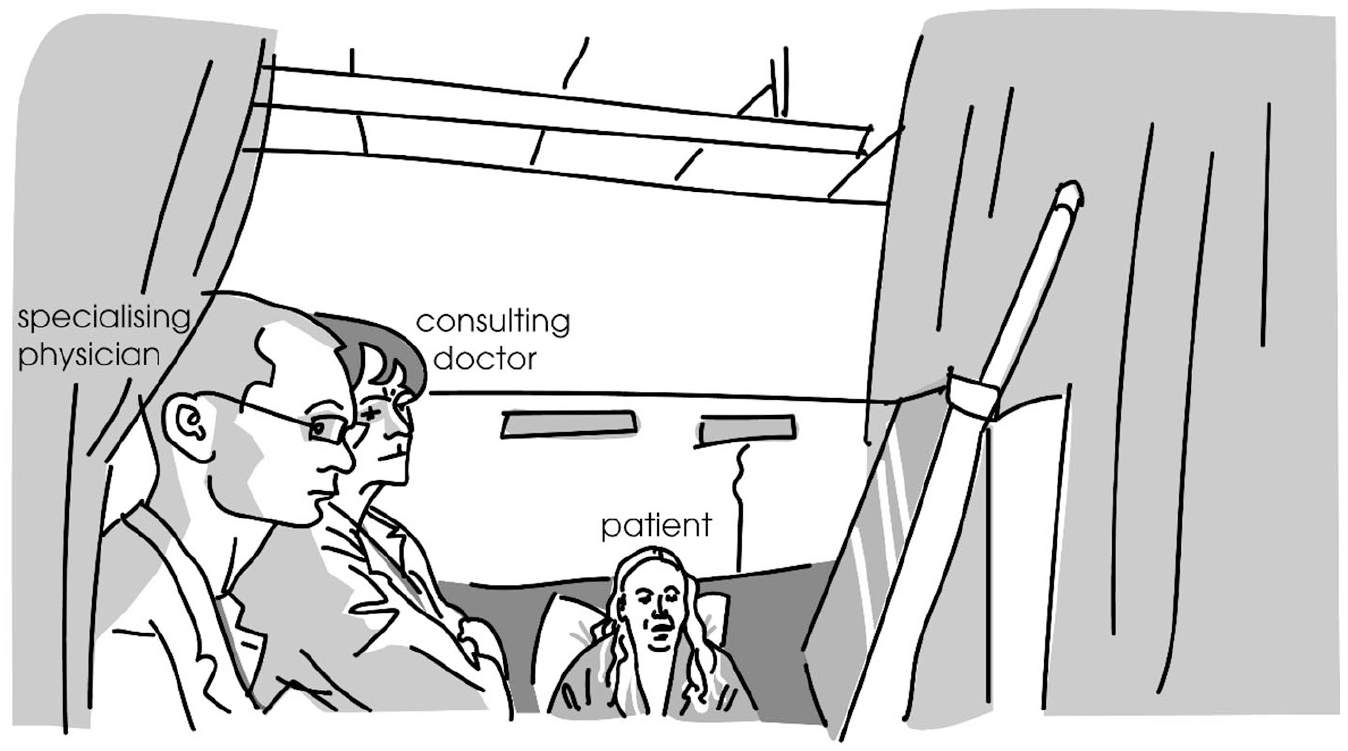
Participants’ body orientations, line 4 of Extract 2.
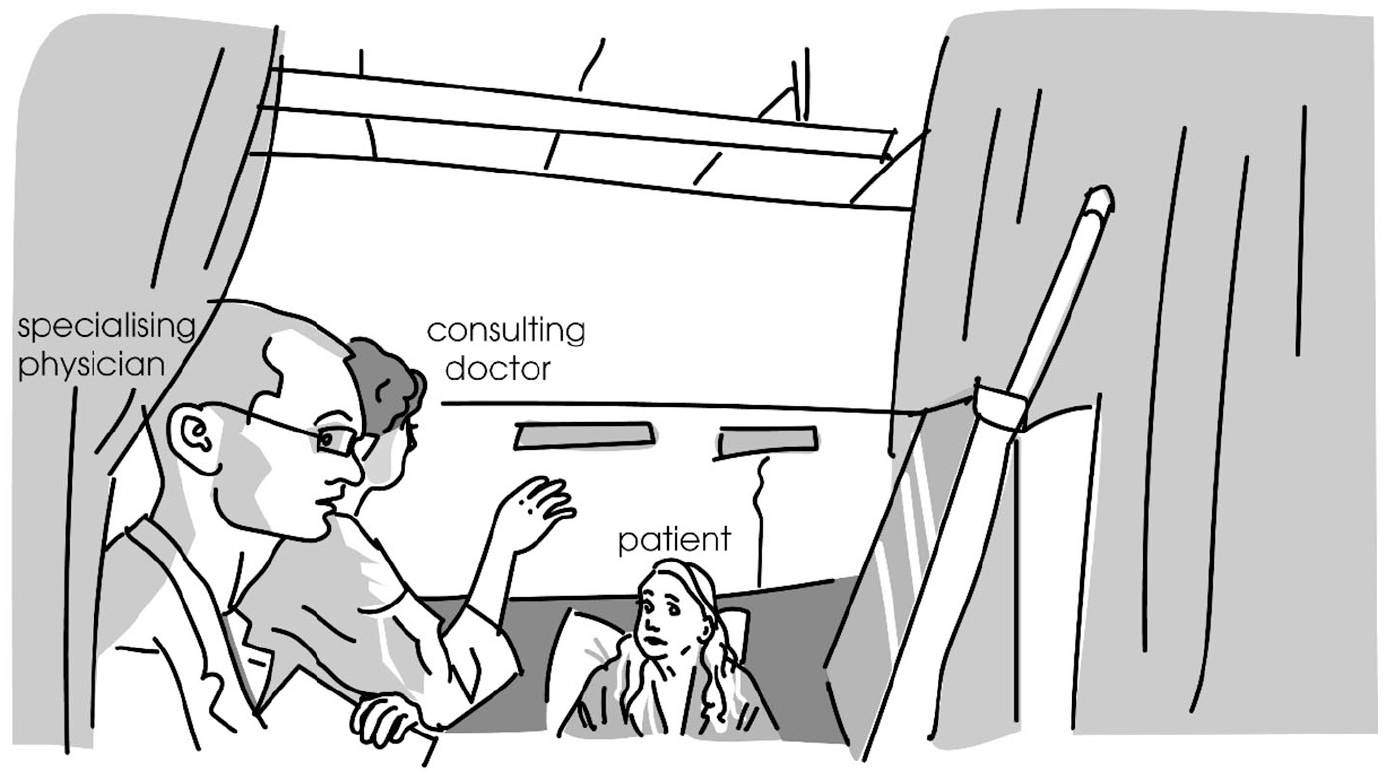
Participants’ body orientations, line 12 of Extract 2.
After the pause (line 8), the doctor turns her head towards the patient and, simultaneously, the patient takes a turn with a repair initiation (line 9). 3 She poses a question that seems to include a conclusion of what she has heard, since she begins her turn with a marker of inference, the particle siis (‘so’) (Hakulinen et al., 2004: § 1132). The content of the question – whether she has a tumour – is not related to the preceding conversation, but the connection seems to lie in the resemblance of the phonetic form of the Finnish words kasvaa (‘to grow’) and kasvain (‘tumour’). The patient has heard SP pronounce the word form kasvanu (‘grown’, line 1), and made her own interpretation of it. During her question her facial expression changes from neutral to somewhat incredulous: she raises her eyebrows. However, she has not shown in any way her concern or surprise before this.
At the end of her question, the patient turns her gaze towards the doctor, who has already turned towards her (line 9, Figure 3). The patient thus directs the question to the doctor, even though the trouble-source – the word kasvanu – has originally been produced by SP. It is thus a case of ‘other’-selection in other-initiation of repair (Bolden, 2011). In this extract, the doctor and SP can be seen as a party acting as a collectivity (see Bolden, 2011: 260), since they both share the necessary knowledge about the patient’s situation. For this reason, the patient can direct the repair initiation to the doctor, who is her default interlocutor during the ward round.
The patient’s repair initiation (line 9) occurs several turns after the trouble-source turn (line 1). Even though other-initiated repair is usually initiated already in the following turn, especially in multi-party conversations the repair initiation can occur further in the conversation (Haakana et al., 2016: 285). In this extract, the trouble-source turn is first of all marked with a level intonation that projects a continuation; when there is a larger unit in progress, the repair initiator often waits until this unit is brought to completion before initiating repair (Schegloff, 2000: 214). Moreover, the turn is addressed to the doctor. Even though it is not a first pair part but rather an answer to the doctor’s prior enquiry about the laboratory results, it evokes a response from the doctor. The patient thus monitors the conversation until the doctor and SP appear to have completed their exchange, and it is only at that point (after the pause, line 8) that she initiates the repair (see also Schegloff, 2000: 216–219).
The doctor answers the patient’s question (lines 12, 14 and 16). She corrects the patient’s misunderstanding as quickly as possible by beginning with the particle chain eiku siis (‘no, I mean’, line 12), which implies that a prior stretch of talk has been wrong and projects an explanation, including a modal meaning of self-evidentiality (Laakso and Sorjonen, 2010: 1158, 1168). The doctor then produces a paraphrase of what SP had said earlier: kasvanu bakteeri teillä virtsassa (‘grown a bacterium there in your urine’, lines 12 and 14). The fact that she begins with the word kasvanu suggests that she has located that word as the source of the misinterpretation. The doctor’s repair turn replaces the understanding of prior talk provided by the patient: the doctor and SP were talking about bacterial growth, not a tumour. During her explanation, the doctor starts smiling, and so does SP (line 13); the patient also produces a (somewhat inaudible) response, smiling and laughing a little (line 15). The patient seems to express relief. The doctor then goes on to reassure the patient further by saying that the infection can be treated with antibiotics (lines 14 and 16).
In this extract, the patient exploits the responsive character of the repair organisation to adhere to the preceding conversation. She monitors the interaction between the medical team in order to locate a suitable moment to bring up a serious concern and thus adjusts her participation to the ongoing situation. Between the moment when she hears something alarming and this moment, she does not manifest any signs of anxiety and hardly any signs of willingness to take a turn. When the patient does pose her question, she formulates it in a way that shows that she is inferring something from the preceding conversation. This helps the doctor to locate the source of misunderstanding and repair it. The doctor thus legitimates the patient’s participation and reacts to her concerns.
Patient produces an interactional initiative
The participation of patients is not limited to only reacting to the doctor’s turns; they may also have an interest in initiating their own questions or concerns (see also Stivers and Heritage, 2001). Instead of exploiting the sequential projection of the previous turn, the patient has to find another way of entering the conversation. In the following section, we will investigate the patients’ ways to get a turn in cases where they produce an initiative rather than responsive turn.
The notion of ‘patient initiative’ was introduced by Drew (2001: 263), who discusses how patients manage to establish an agenda of their own in dyadic doctor-patient interactions. We will explore instances where the patient produces an initiative turn, a first pair part, in a multi-party situation where they are not the addressed recipient. These initiatives can be either successful or unsuccessful (i.e. being responded to or not evoking a response from the medical team). Through investigating both an unsuccessful and a successful initiative by the patient, we will illustrate the constraints shaping the patients’ opportunities to participate in the ward round conversation.
The next extract begins with the doctor (D) talking to the patient (P), standing next to his bed. Prior to the excerpt, the medical team has checked the patient’s urine production in the computer files and noted that it has been low.
At the beginning of this extract, the central participants are the doctor and the patient: the doctor is standing by the patient’s bed, his gaze directed at the patient, and he uses the second person form when addressing the patient (voi
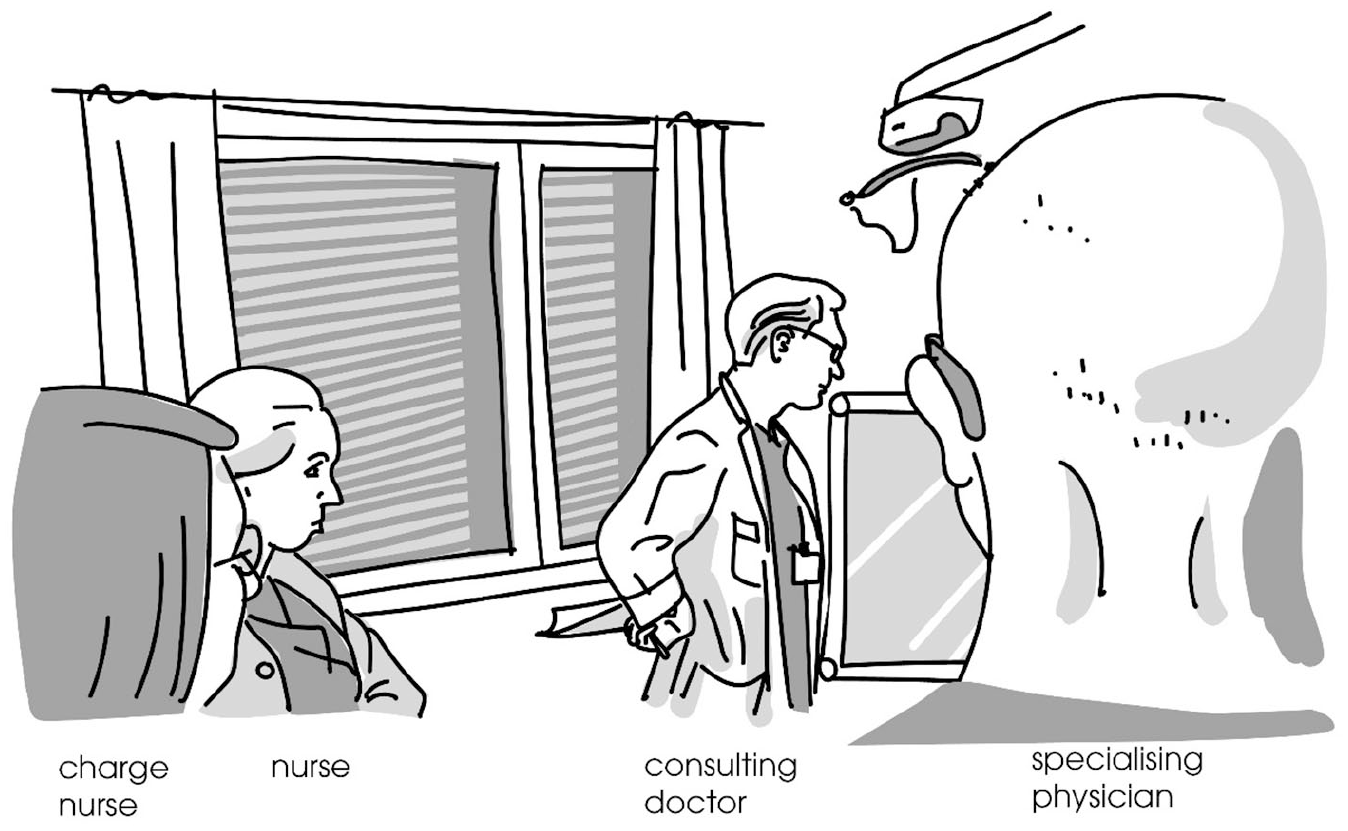
Participants’ body orientations, line 2 of Extract 3.
The change in the participation framework is evident to the nurses as well; they both respond to the doctor’s turn (lines 7–9). The focal point of participation is being moved from doctor-patient interaction to the medical-team interaction. The charge nurse (CN) uses the inclusive ‘we’ referring to the medical team, and she uses professional instead of lay terminology (‘diuresis’) to refer to the actions concerning the patient (lines 8–9). After the doctor has confirmed the nurses’ turns (lines 10–11), the medical team has reached an agreement on the need and use of the catheter, and they orient even more strongly away from the patient: the doctor leaves his position by the side of the patient’s bed and starts walking towards the computer (see Figure 5), and the nurse (N) uses the third person pronoun (sille) when referring to the patient (line 13: saaks
Participants’ body orientations, line 13 of Extract 3.
It is at this point that the patient tries to enter the conversation and re-introduce the subject of the catheter. He initiates a turn with the particle ni (line 15), indicating a return to a previous (main) topic (see Hakulinen et al., 2004: §811). He begins his turn simultaneously with the nurse, who is completing her own question to the doctor (line 14). The patient continues his question when he is in the clear and brings it to completion (line 15). The doctor, however, responds to the nurse’s (rather than the patient’s) question, in overlap with the patient’s turn (line 16). At this point the doctor has reached the computer and is adjusting the screen, and while doing it he provides a turn (lines 17–19, see Figure 6) that both confirms the nurse’s suggestion and informs the specialising physician (SP) about what to write in the patient’s files. The medical team has now rearranged themselves around the computer, SP starts typing the information in the electronic form, and no one responds to the patient’s question about the catheter (line 20). The patient does not manage to change the participation framework to become an active participant instead of the one who is being talked about.
Participants’ body orientations, line 17 of Extract 3.
Later in the same encounter, the patient brings up the question about the catheter again.
Just before the extract, SP, who is still standing by the computer, turns his head towards the doctor and asks if they ‘should put down any limit for the haemoglobin’. The doctor, who has taken some steps backwards towards the door of the room, stops (line 1) and provides the inquired information (the time of the control, ‘3 pm’, and the HB limit, ‘85’) (lines 2–3). SP starts typing this information in the computer (line 3), and the whole medical team becomes static. It is at this point that the patient asks about the catheter again.
This time the situation is clearly different: having acknowledged the doctor’s answer with the particle joo ‘yes’ (line 4), a small pause has occurred in SP’s typing (line 5), and all the team members are static. The patient does not have trouble in getting the medical team’s attention, even though the medical team is physically away from his bed, gazing at the computer: the doctor begins turning his head towards the patient shortly after the patient has begun his turn (line 6), and the nurse starts answering his question already in overlap with the end of the turn (line 8) as soon as the content of the question is understandable.
When comparing the unsuccessful initiative (Extract 3, line 15) with the successful one (Extract 4, lines 6–7), the role of the parallel embodied actions become clear. The patient’s successful and unsuccessful initiatives occur in different environments: the former initiative takes place in the middle of a transition phase when the medical team members are physically rearranging their positions and interactionally involved in negotiating about the patient’s treatment, whereas the latter is produced in a more static situation.
The transition phase (within which the patient’s first initiative occurs) involves a reorganisation of the interactional space (Mondada, 2009): in (3), the doctor walks from the patient’s bed to the computer, turns the computer so that he (and others) can see it, and the other team members are repositioning themselves in relation to the doctor and in relation to the computer that has been focalised by the doctor’s action (lines 12–17). Thus, the interactional space is filled with the team members’ ongoing embodied activities, which involve temporal synchronisation with each other (see also Haddington et al., 2014). In contrast, the latter initiative by the patient is produced in a “calmer moment”: there is an ongoing parallel activity (SP’s typing), but the medical team is immobile. Even if the doctor is not orienting to the patient in this case either – he gazes at the computer screen when the patient starts asking his question – the stability of the interactional space gives prominence to the new action by the patient rather than overriding it, and hence the patient manages to become an active participant in the conversation.
Thus, the embodied and multimodal activities by the participants play a crucial role in defining the patient’s possibilities to enter the conversation. Even though the patient could be thought to be an “omni-relevant” (Sacks, 1992: 594–595) participant in interaction, given that he (his illness and treatment) is the reason for the whole encounter to take place, it is clear that the opportunities for the patient to participate are locally negotiated and contingent on sequential as well as multimodal constraints.
Conclusion
In this paper, we have explored patients’ opportunities to participate in the discussion concerning their care and treatment during a ward round. In particular, we have investigated how the patient gets a turn in a ward round encounter, which represents multimodally rich, multi-party interaction with strict time constraints. The round involves phases where the medical team discuss with each other about the patient’s medical record or their treatment and medication, for instance, and in these phases the talk is not usually addressed to the patient (see also Oxelmark et al., 2018). Hence, the patient needs to do active interactional work if they want to become a ratified participant in the discussion.
When not the addressed recipient, the patient may employ different means to enter the conversation. One way is to exploit the sequential projection of previous turns. In cases where a first pair part is produced, the patient can provide a second pair part, even if the first pair part is not directed to them by gaze or verbal means. In addition to the sequential organisation, the patients may make use of repair organisation. Repair actions can supersede other actions (Schegloff, 2000: 208): repair initiations may be produced at any time in conversation, and the problem they are targeting should be clarified before the talk-in-progress is continued (see Schegloff et al., 1977). By shifting focus to something in the prior talk through a repair initiation, patients can enter the conversation even in cases where the prior talk was not directed to them. Thus, the sequential implication of first pair parts and repair initiations can be used as means to become a ratified participant in the discussion.
However, building on the sequential projections of the previous turns is not the only way for patients to get a turn. As shown in Extracts 3–4, the patients also try to enter the conversation by asking questions. A question is a first pair part that strongly projects a second pair part; the recipient is expected to produce an answer and failing to do so results in a “noticeable absence” (see Schegloff, 2007: 20). Even though the patient asks a question in (3), no one provides an answer or any account for its absence. The first pair part by the patient does not reach the medical team, which is in the process of reconfiguring itself: the members move both physically in the location and interactionally from one phase to the next. In these dynamic transitions, it seems that the mobile members of the medical team are orienting to each other rather than to the (immobile) patient or his turns. The absence of a verbal second pair part is perhaps not as noticeable when the interactional space is filled with multimodal actions. It is only when the medical team becomes more static that the patient’s first pair part receives attention and is granted a response. Thus, both the sequential and multimodal constraints shape the patient’s opportunity to modify the participation framework, in order to become a ratified participant in the discussion.
What conclusions can be drawn on the basis of this analysis? An important question is how patient participation could be promoted throughout the round, given that ward rounds evidently involve instances where the medical team members need to discuss with each other. First, if the medical professionals talk clearly and without highly technical language, their turns are available to the patients as well, even if they are not directly addressed to them. This makes it possible for the patient to respond to these turns, thereby displaying their willingness to actively participate in the conversation, as shown in Extract 1. The importance of clarity and the sufficient audibility of the medical team’s (mutual) talk can also be seen in Extract 2, where the patient’s contribution (i.e. her repair initiation) results from her not quite hearing or understanding what the doctor and the specialising physician are saying to each other while going through the patient’s results in the electronic document. The patient’s partial hearing raises serious concerns, which she manages to bring up through a repair initiation when a quiet moment emerges.
In general, calm moments are important for patient participation. As we showed in Extract 3, the patient may have difficulty in participating in the conversation in transition phases when the medical team is rearranging itself and the interactional space. In these multimodally intensive moments, even the patient’s turns with normative sequential projections, such as questions, may not be responded to. Therefore, it is of crucial importance that the rounds not be too hasty, so that – despite time constraints – the medical team would be able to proceed unhurriedly, allowing calmer moments, particularly after phases that involve physical movement and reconfiguration of the interactional space and its material objects. Efficiency (and how to increase it) is a topical issue in Western healthcare, but compressing ward rounds to eliminate “empty” or “ineffective” parts, for example, would probably have negative consequences on patients’ possibilities to participate in interaction; calmer moments offer opportunities for the patients to introduce their own initiatives.
Finally, as noted by previous research (e.g. Collins et al., 2007), the aim of patient participation is not necessarily to maximise the patient’s responsibility in planning their treatment and care. It is possible that the patients may instead want to leave the decisions about their treatment and care to the medical professionals, and this should be a possible alternative for them. Similarly, it is not an end in itself that the patient would talk as much as possible during a ward round. However, it is important that the patients have a chance to participate in cases when they need or want to say something. Exploring ward round interaction in detail helps to identify possible obstacles that may hinder the patients’ attempts to be seen, heard and understood in their encounters with medical professionals.
Footnotes
Appendix 1
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by a grant from Kone Foundation.