
Abstract
Perioperative smoking cessation reduces wound-healing complications, yet its long-term effect on sustained abstinence after elective plastic surgery remains uncertain. This study examined patients who underwent elective plastic surgery and participated in a follow-up interview to assess whether adherence to short-term perioperative smoking cessation instructions was associated with continued abstinence post-surgery. All smokers were instructed to quit at least 4 weeks prior to surgery and remain abstinent for at least 4 weeks afterwards. Patients were categorised as either compliant or non-compliant with preoperative guidance. The findings suggest that elective plastic surgery may serve as a teachable moment that extends the immediate smoke-free period; however, short-term instructions alone seldom result in lasting abstinence. Integrating structured cessation programmes with perioperative counselling may be required to transform temporary compliance into enduring behavioural change.
Introduction
Tobacco smoking is the leading preventable cause of early mortality worldwide. According to the World Health Organization, over 7 million deaths each year are linked to tobacco use, including about 480,000 deaths annually in the United States alone. Along with its well-documented connection to chronic diseases, smoking also places a significant economic strain on healthcare systems worldwide (García-Gómez et al 2019, Jalali et al 2021, Raja et al 2021, Rinker 2013, World Health Organization 2014).
The harmful effects of smoking on postoperative healing are well-known and especially significant in surgeries that involve extensive tissue manipulation (Sørensen 2012). The impaired wound healing among smokers is thought to be caused by reduced tissue oxygenation, mainly due to nicotine-induced vasoconstriction, catecholamine release, and carbon monoxide’s high affinity for haemoglobin, which diminishes oxygen delivery to peripheral tissues (Bonilla et al 2025, McDaniel & Browning 2014, Tanayah Uma et al 2024).
While many patients try to quit smoking, only a small number succeed in maintaining long-term cessation. Data from the Morbidity and Mortality Weekly Report (MMWR) indicates that only 7.5% of adult smokers in the United States manage to quit for 6–12 months (Creamer et al 2019). Relapse remains common, particularly within the first year after quitting (Robinson et al 2019, Rodríguez-Cano et al 2021). The initial 2 weeks of quitting are crucial because withdrawal symptoms such as irritability, sleep disturbances, and cravings are at their worst (Piasecki et al 2003, Shiffman et al 2006).
In plastic surgery involving extensive tissue manipulation, a patient’s smoking status can significantly influence the surgical outcome. Systematic review and meta-analyses have demonstrated that smoking increases the risk of complications such as necrosis, wound dehiscence, and infection, especially in reconstructive procedures with implants, with an odds ratio of up to 3.6 (Sørensen 2012). This systematic review also found that preoperative smoking cessation reduced the risk of surgical site infection by 57% in four randomised controlled trials. A propensity score–matched analysis of 36,454 patients found smoking as an independent risk factor for postoperative complications, including deep incisional surgical-site infection (Toyoda et al 2018). Based on this risk, the American Society of Plastic Surgeons (ASPS) published a practice reference for managing the risks of smoking in plastic surgery patients. They recommend complete smoking cessation at least 4–8 weeks before surgery and continued abstinence for 4 weeks after the procedure (ASPS 2024).
The perioperative period of an elective plastic surgery can serve as a unique motivational window. A study of patients who underwent cosmetic plastic surgery found that 40.5% of the patients were no longer smoking cigarettes daily, including 23.8% who had not smoked since their surgery (Van Slyke et al 2017). This study also found that 70.8% of the patients who reduced their cigarette consumption agreed that discussing adverse surgical outcomes related to smoking influenced their ability to quit or reduce. We may assume that those patients seeking optimal aesthetic results often demonstrate greater adherence to instructions, including temporarily stopping smoking. If a structured perioperative cessation period can lead to lasting behavioural change, it could open a new pathway for smoking cessation efforts. As supported by the ASPS practice reference, in our institution, every smoking patient is asked to complete smoking cessation at least 4 weeks before surgery and maintain abstinence for at least 4 weeks after the procedure (ASPS 2024).
The objective of this study is to examine whether adherence to short-term smoking cessation instructions before elective plastic surgery is associated with sustained long-term smoking abstinence.
Methods
This retrospective cohort study with a prospective component included patients who underwent plastic surgeries involving significant tissue dissection at our institution between January 2018 and August 2022. Eligible procedures included abdominoplasty, breast reduction, and breast reconstruction with implants.
Inclusion and exclusion criteria
Inclusion criteria were: age ⩾18 years at the time of surgery, documented active smoking status prior to surgery, and documented receipt of verbal instructions from the surgical team regarding perioperative smoking cessation.
Exclusion criterion was: patients who were unable to give informed consent at the beginning of a telephone interview.
Study protocol
For each patient who met the inclusion criteria, a telephone interview was performed. Telephone interviews were performed between August 2024 and September 2024 by a single interviewer (Yanay Shaked). In the event of no answer, up to three calls were conducted on different days. After accepting oral informed consent, the interviewer asked the patient the following questions:
- What is your marital status?
- At what age did you start smoking?
- How many packs per day?
- Did you have prior attempts to quit smoking before the surgery?
- Was it your first surgery under general anaesthesia?
- Did you adhere to the preoperative smoking cessation recommendations?
- Did you smoke during the year after the surgery? If so, when did you start smoking again?
- Are you a current smoker? If so, when did you start smoking again?
Study outcomes
The primary outcome was long-term smoking abstinence, defined as continuous abstinence for at least 1 year following surgery. The secondary outcome was the time until the patient returned to smoking after surgery.
Statistical analyses
The primary goal of the statistical analyses was to compare the outcomes of patients who complied with smoking cessation recommendations against those who did not, and to determine which factors predicted the likelihood and duration of long-term smoking abstinence. Appropriate tests were utilised to compare patient groups, and modelling techniques were employed to predict the primary outcome and analyse the time until patients resumed smoking.
To this end, both non-parametric comparison tests and advanced regression modelling techniques were employed. Patients were grouped based on adherence to preoperative smoking cessation recommendations (Compliant vs Non-Compliant). Continuous variables were reported as medians with interquartile ranges and compared using the Mann–Whitney U test. Categorical variables were analysed using the Pearson chi-square or exact test. All analyses were two-sided with a significance level of p < 0.05. Univariate logistic regression identified predictors of long-term smoking abstinence, the primary outcome. A binomial test was used to compare smoking and cessation rates with published population data. Time to smoking resumption was analysed using Kaplan–Meier curves, the log-rank test, and Cox regression. Analyses were conducted using SPSS (version 29, IBM Corp., Armonk, NY, USA, 2022).
Sample size calculation
The required sample size was calculated based on the primary binary outcome using logistic regression. We assumed an abstinence rate of 10% in the non-compliant group and 40% in the compliant group, corresponding to an expected odds ratio of 6.0. To detect this difference with a power of 80% and a two-sided significance level of 0.05, a total of 62 participants (31 per group) were required. Sample size estimation was performed using the Statsmodels package version 0.13.0 (Python version 3.11).
Ethical approval
The study protocol was reviewed and approved by the Institutional Review Board (Approval No. HMO-0276-23). Oral informed consent was obtained at the beginning of the telephone interview. Written informed consent was waived due to the telephone-based design and the minimal risk associated with participation. All data was anonymised before analyses; no direct identifiers or protected health information was retained.
Results
During the study period, 732 patients underwent eligible surgery and were evaluated for eligibility. A total of 612 patients did not meet the inclusion criteria. A total of 112 patients were eligible for the study and included in the telephone survey. Twenty-four patients were excluded (either did not answer or did not give informed consent). A total of 88 patients completed the telephone interview and were included in the analyses (Figure 1).
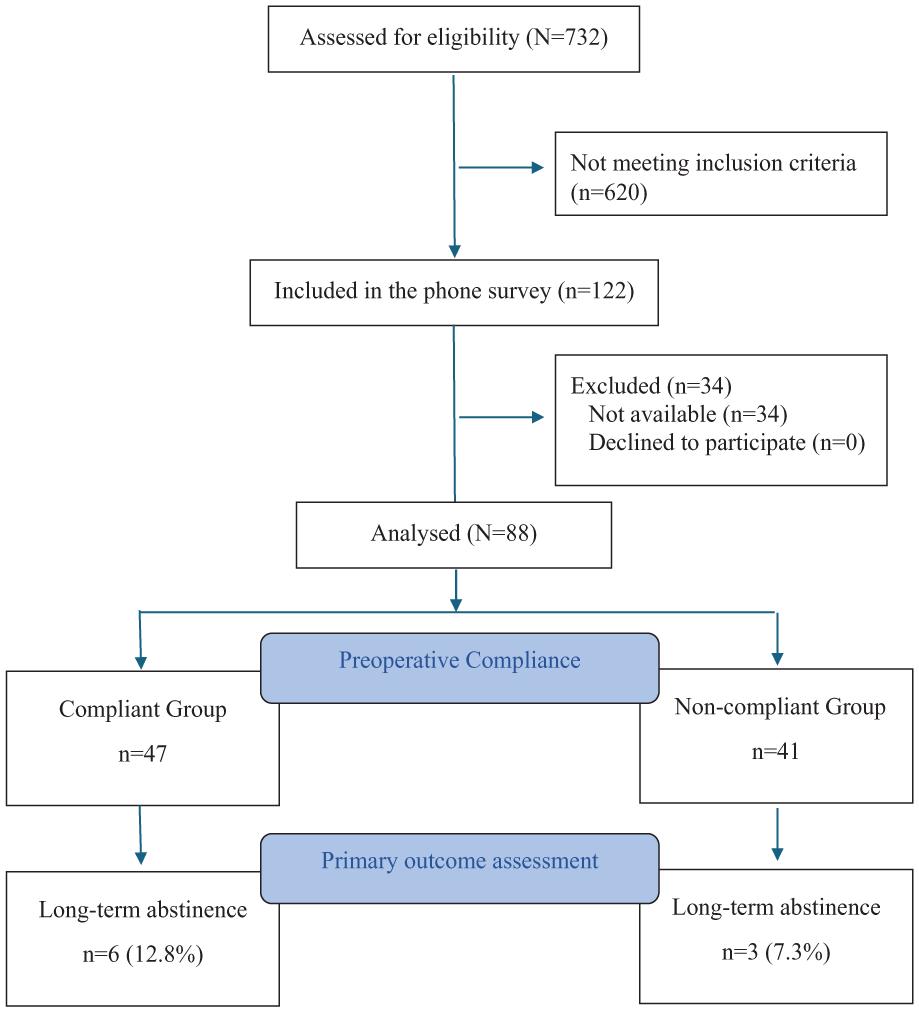
Participant flow diagram
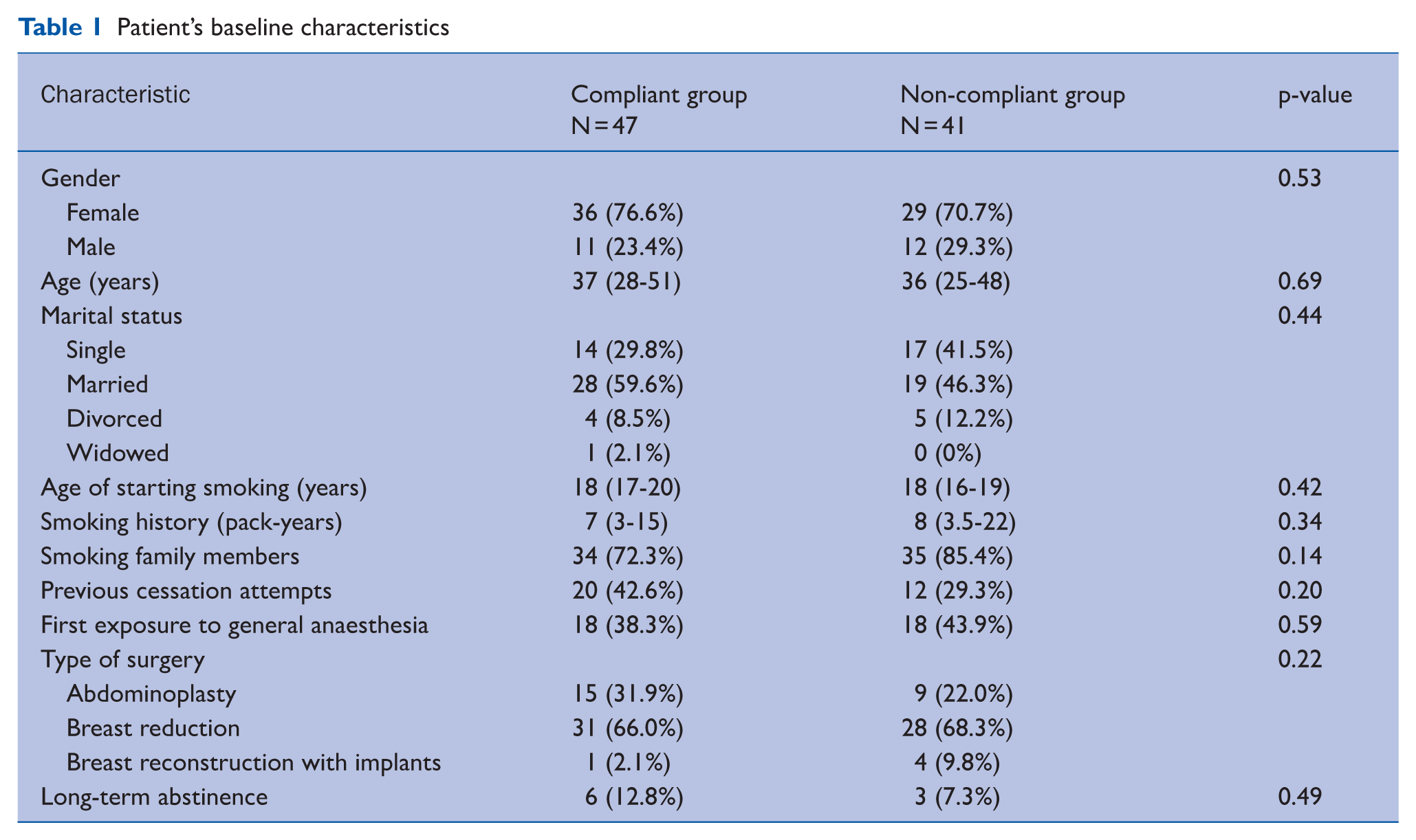
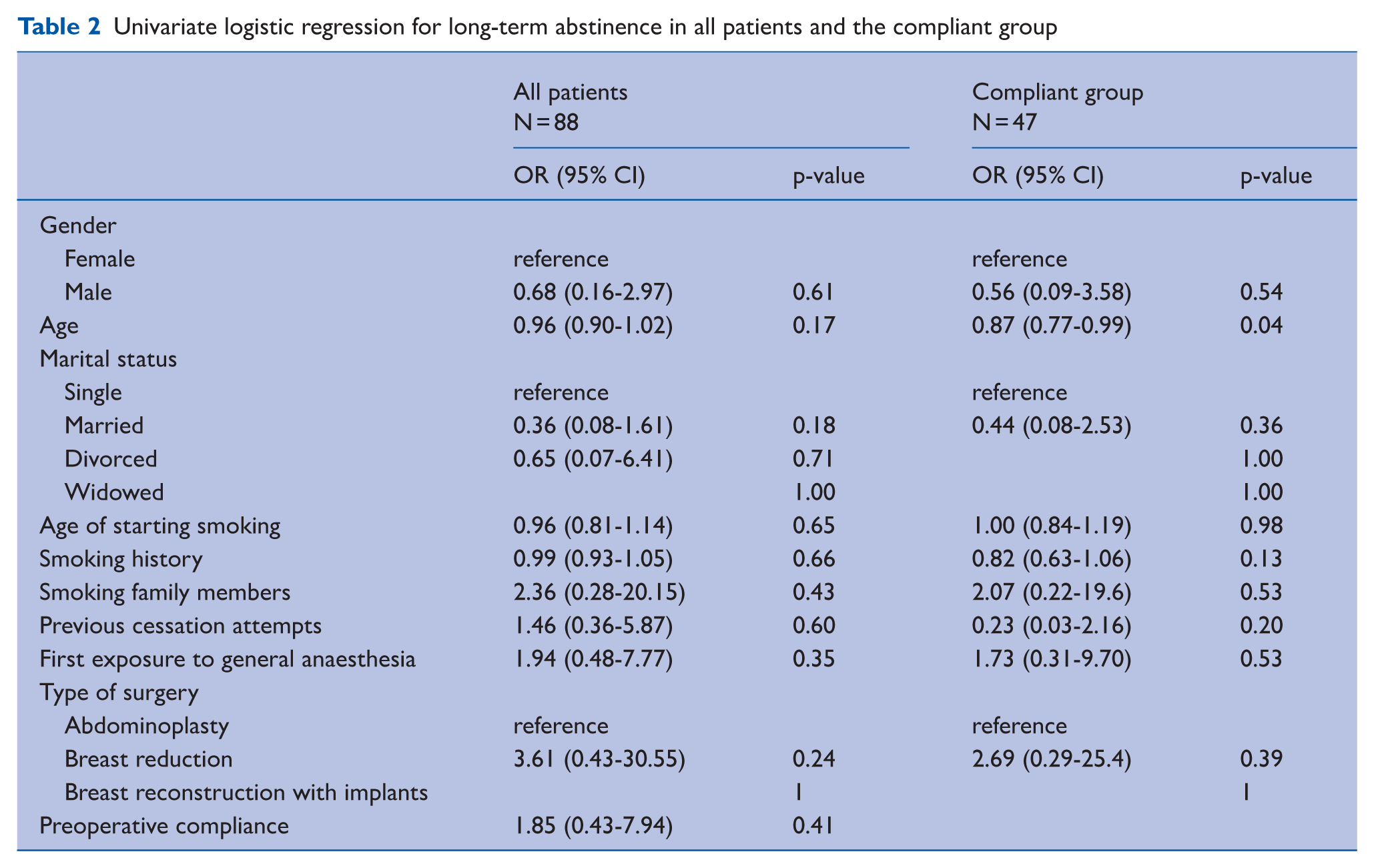
The median age was 36 years (IQR = 27–49), with a gender distribution of 23 men and 65 women. Forty-seven (53.4%) patients were in the compliant group, while 41 (46.6%) were in the non-compliant group. No significant differences were observed between the groups’ baseline characteristics (Table 1). The primary outcome of long-term abstinence was achieved by 6 of 47 (12.8%) patients in the compliant group and 3 of 41 (7.3%) in the non-compliant group (p = 0.49). In univariate binary logistic regression, no predictors were identified for long-term abstinence (Table 2). Subgroup analyses of the compliant group identified age as a predictor for long-term abstinence with an OR of 0.87 (95% CI = 0.77–0.99), p = 0.04.
Patient’s baseline characteristics
Univariate logistic regression for long-term abstinence in all patients and the compliant group
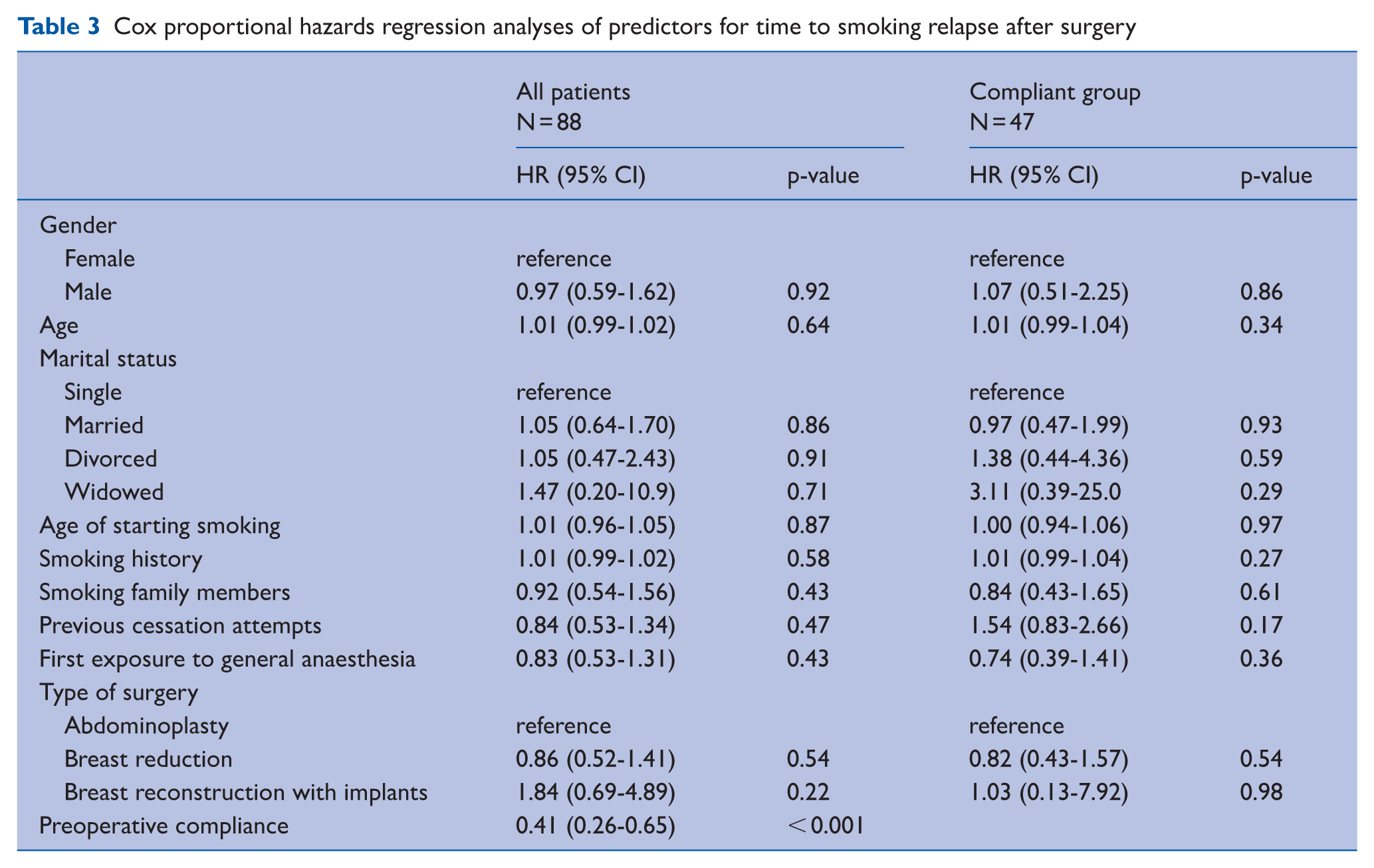
The median time to smoking relapse after surgery was 2 months in the compliant group and < 1 month in the non-compliant group (p < 0.001) (Figure 2). Cox regression analyses showed that preoperative compliance was independently associated with time to smoking relapse, with a hazard ratio of 0.41 (95% CI: 0.26–0.65, p < 0.001). No other variables were significantly associated with the time to smoking relapse (Table 3).
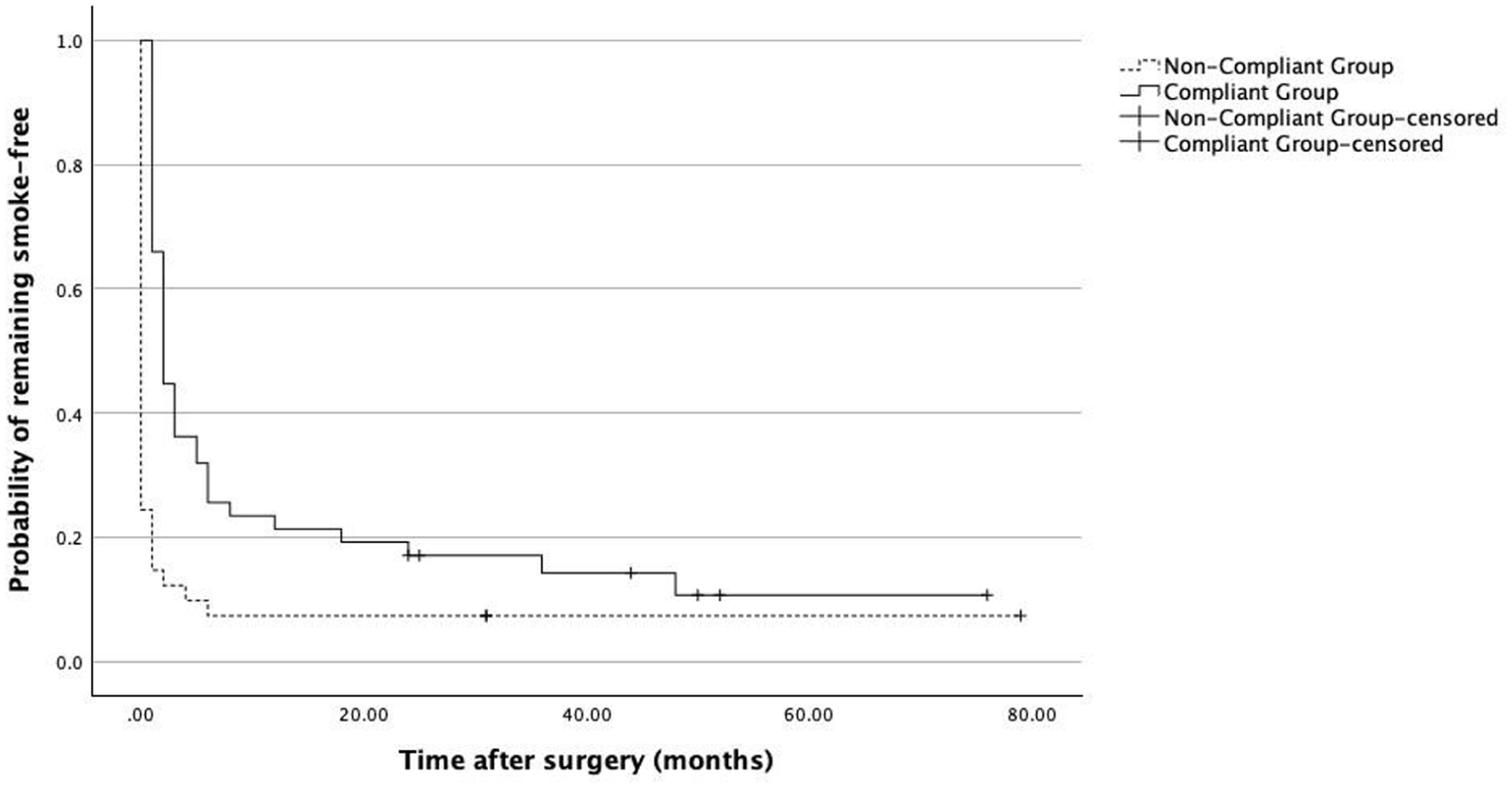
Kaplan–Meier curves for relapse-free survival after elective plastic surgery in smokers, stratified by preoperative compliance with smoking-cessation instructions
Cox proportional hazards regression analyses of predictors for time to smoking relapse after surgery
Discussion
In this study of patients undergoing elective plastic surgery, we found a smoking prevalence of 15.3%, similar to the published smoking prevalence in the adult population (15.9%, p = 0.69) (Organisation for Economic Co-operation and Development (OECD) 2023). We chose to check the long-term abstinence at 1 year after surgery. Previous studies showed that the risk of smoking relapse reduces dramatically after 1 year of abstinence.
On the one hand, we found that the overall rate of long-term smoking cessation at 1 year was low (12.8% in the compliant group and 7.3% in the non-compliant group) and that the difference between the groups was not statistically significant. The overall quit rate in our study population was 10.2%, whereas the overall quit rate in the general population is approximately 8.8% (p = 0.37) (VanFrank et al 2024).
On the other hand, we found that preoperative compliance with smoking cessation instructions is associated with a significantly longer duration of postoperative smoking abstinence (2 months in the compliant group versus < 1 month in the non-compliant group, p < 0.001). This meaningful delay is not without clinical importance, particularly for surgeries with high sensitivity to smoking-related complications. A temporary cessation, even if it does not achieve long-term success, may still reduce short-term surgical risks (Sørensen 2012).
Previous studies have suggested that elective surgery may present a teachable moment for behavioural change; our results partially support this hypothesis. This is consistent with previous studies that reported similar short-term abstinence benefits, though long-term success often required formal cessation programmes (Kim et al 2024, Shi & Warner 2010).
Limitations of the study
Although our study has a well-defined cohort, standardised perioperative instructions, and direct follow-up interviews, which allowed for individualised data on relapse timing, several limitations must be acknowledged. First, the retrospective design introduces potential recall bias, particularly regarding the timing of smoking relapse. Second, we relied on self-reported smoking status without biochemical validation (e.g. cotinine testing). Third, the sample size was limited, and the study may have been underpowered to detect modest differences in long-term abstinence. Finally, the lack of a formal cessation intervention limits the generalisability of the findings to programmes involving counselling or pharmacotherapy.
Conclusion and suggestions for further research
The perioperative period may offer a unique opportunity to promote smoking cessation, particularly among individuals motivated by upcoming elective procedures. While long-term abstinence was limited, the observed behavioural shifts suggest potential for brief interventions. Incorporating structured cessation support into routine surgical pathways could enhance public health efforts to reduce tobacco use.
Future studies should examine whether combining perioperative instructions with structured support, such as nicotine replacement therapy or behavioural counselling, could increase long-term abstinence rates. Randomised trials could evaluate whether integrating cessation programmes into surgical workflows improves outcomes.
Footnotes
Authors’ note
This work was performed in partial fulfilment of the Master of Public Health (MPH) thesis requirements of Yanay Shaked at the Faculty of Medical and Health Sciences at Tel-Aviv University.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
The study protocol was reviewed and approved by the Institutional Review Board (Approval No HMO-0276-23). Verbal informed consent was obtained from all patients.
Data availability statement
The data will be available on reasonable request from the corresponding author.
AI statement
No generative artificial intelligence (AI) tools were used in the writing or editing of this manuscript. Standard AI-based software (e.g. for grammar and spelling correction) may have been used to improve readability, and the authors take full responsibility for the content of the published study.