
Abstract
Major bleeding represents a critical scenario that can quickly evolve into life threatening, thereby compromising patient safety. A Validated Intraoperative Bleeding Scale called VIBe Scale was introduced and studied as part of a quality improvement initiative. This study evaluated the clinical implementation of the VIBe Scale in perioperative patient management and team communication from the nurses’ perspectives. A descriptive study was undertaken, incorporating introductory lecture, simulation of major bleeding event and post-lecture questionnaire with 33 operating room nurses. Despite many participants not previously having experience of the VIBe Scale in practice, over two-thirds reported the scale could improve situational awareness. Furthermore, nearly two-thirds reported they could see the utility of the VIBe Scale as a tool to improve communication. Our study shows that the VIBe Scale is an easily understood concept, has the potential to increase situational awareness and can support team communication around intraoperative bleeding events.
Keywords
Introduction
During a critical haemorrhage event, a patient’s life mainly depends on a skilled surgical team and the availability of blood products. Managing such an event may involve many aspects of human factors (Irita 2011). Haemorrhagic mortality and morbidity in the operating room (OR) can be reduced by a systemic, not an individual, approach. Establishment of hospital processes to manage critical haemorrhage depends upon the overall capability of risk and crisis management of a hospital (Irita et al 2005). Therefore, it is recommended that the local clinical quality and safety management systems include processes to assess the haemorrhage control measures and outcomes (Spahn et al 2019).
Failure to achieve haemostasis quickly after bleeding onset during surgery is associated with increased mortality, higher care costs and increased likelihood of blood transfusion requirement (Marietta et al 2006, Shander 2007, Stokes et al 2011). A retrospective analysis showed that bleeding-related complications occur in one in three patients undergoing inpatient surgical procedures. Such complications include blood transfusion, renal failure and stroke, all of which can increase length of stay, mortality and resource utilisation (Shander 2007). Optimal patient blood management, although crucial, is not always achieved (Meybohm et al 2017).
Lewis et al (2017) described the development of a clinician-reported Validated Intraoperative Bleeding scale (VIBe Scale) to describe bleeding severity for use in clinical studies of haemostatic agents. The VIBe Scale was used by surgeons (N = 144) from 11 surgical specialties, recruited to test the scale across three study phases: concept (N = 9), feasibility (N = 33) and validation (N = 102). They concluded that the VIBe Scale was usable, clear and clinically relevant with excellent reliability.
There is a lack of standardised language or consensus in the definitions of intraoperative bleeding severity in both clinical and research settings, with a knowledge gap as to how this can relate to human factors and to effective team communication during a bleeding event. The VIBe Scale, designed for consistent and reliable assessment of intraoperative bleeding severity, could provide a common language for surgical teams to assess and manage intraoperative bleeding, potentially improving the response to bleeding events, leading to improved patient outcomes.
The objective of this service improvement was to evaluate the clinical implementation of the VIBe Scale in the perioperative patient management and team communication from the nurses’ perspective.
Driving force for change
Rationale for the desired improvement
A recent major haemorrhage simulation was performed as part of a quality improvement initiative in a urological cancer service in Scotland, where it was identified that effective communication was a key aspect for the surgical team to improve upon. This quality improvement project was centred on the evaluation of the VIBe Scale’s potential to assess intraoperative bleeding and act as a communication tool during these events.
Although the dissemination of clinical guidelines is necessary, it is rarely sufficient alone, to ensure reliable acceptance of evidence-based practice. Clinical guideline recommendations can be sustainably integrated within current clinical systems, if linked with ‘high-impact’ quality indicators to show where a measurable change in clinical practice can improve patient outcomes (Foy et al 2020).
Therefore, the process of adopting the VIBe Scale as a clinical tool in clinical practice was structured based on three pillars: (1) Professional and practice-based knowledge, (2) Team management and effective communication and (3) Patient safety, clinical practice and quality improvement.
Team management and effective communication are important factors in consolidating a clinical practice and improving professional performance. A qualitative study of 16 members of the surgical team suggested that education and increasing the knowledge base of all surgical team members can change cultures, improve communication and increase professional understanding (Gillespie et al 2010).
A study investigated how much distractions in the OR are associated with increased mental workload and stress, and how much it affects teamworking (Wheelock et al 2015). This study followed 90 cases of general surgery in real time, using validated tools for behavioural assessment. Irrelevant conversations initiated by surgeons and anaesthestists, equipment-related distractions and acoustic distractions correlated with higher stress and lower teamworking. Wheelock et al (2015) also argue for the idea that distractions may be managed by the implementation of standard operating procedures such as the ‘sterile cockpit’ or ensuring a comprehensive preoperative surgical brief and debrief. The use of these structured communication procedures enables the surgical team to develop shared mental models of the clinical task, thereby optimising teamworking (Gillespie et al 2010).
According to Ben-Yehuda and Redfors (2016), the use of clinical scales, such as the VIBe Scale, may reduce distractions, improve communication between the OR team and facilitate higher quality decision-making with the potential to improve teamwork in surgery and, thus, increase patient safety.
Description of the change process
The use of the VIBe Scale was piloted as part of a quality improvement initiative within a major urological cancer service in Scotland, specifically in renal cancer surgery. Both the lead nurse and the surgeon had independently identified the VIBe Scale as a potential tool to enhance communication after being exposed to it during a training event. The aim was to explore whether the VIBe Scale can be used to describe bleeding and to communicate this effectively between team members (Figure 1). Utilising a Plan Do Study Act approach, the VIBe Scale was taught, discussed and incorporated into clinical practice. Listening to staff feedback was a vital part of the process to harness ideas of how to utilise the VIBe as an effective trigger tool (see section ‘Project design and approach to improvement’ for further details).

Quality improvement process of incorporating VIBe as a tool for use in managing bleeding and communicating blood loss
Evaluation of the use of the VIBe Scale was through a questionnaire. At the surgical debrief, a further questionnaire captured the intraoperative use of the VIBe Scale.
The VIBe Scale and the measurement techniques for quality improvement
The VIBe Scale was developed to address the lack of a validated, clinician-reported scale sought by the United States Food and Drug Administration (FDA) to standardise the definitions of intraoperative bleeding (Lewis et al 2017) (Figure 2).
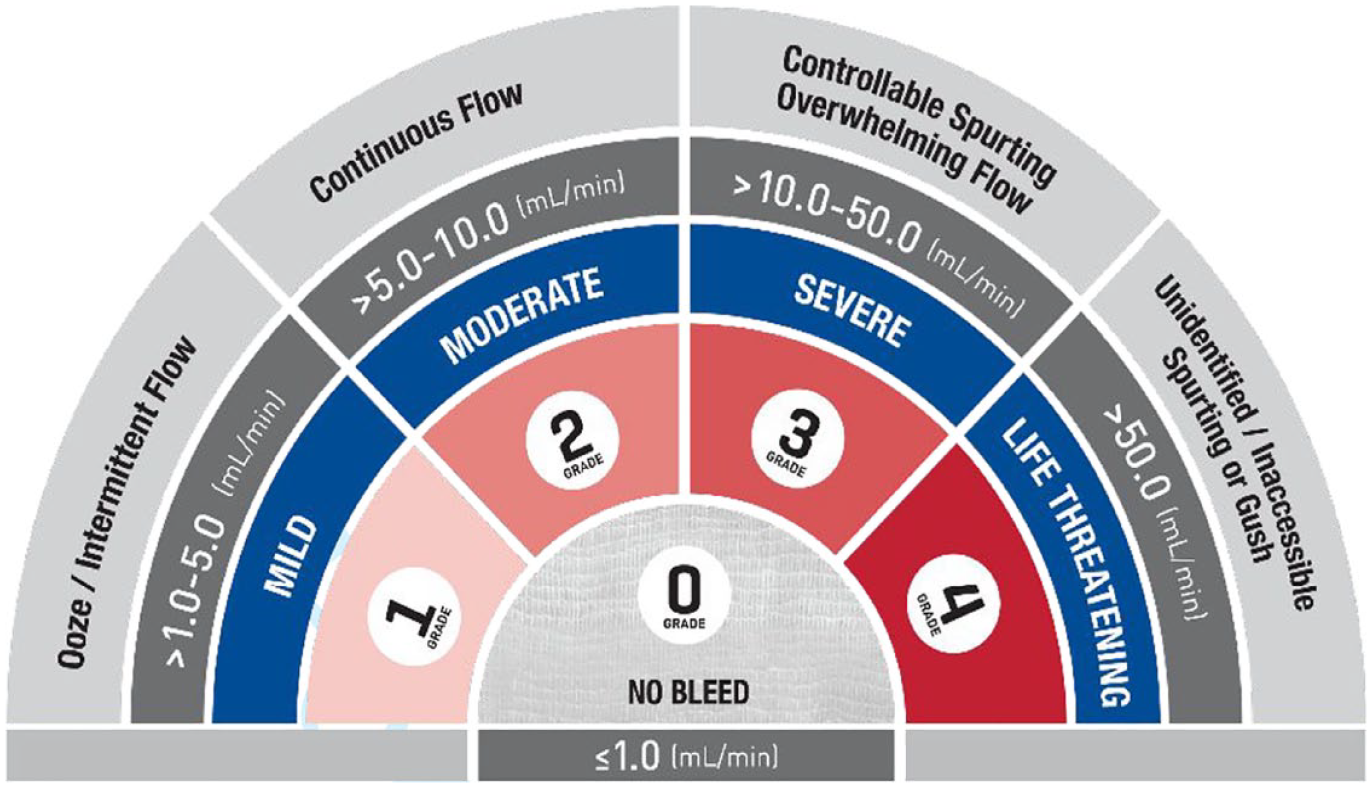
The VIBe Scale: Classifying severity into five distinct grades (Lewis et al 2017)
The VIBe Scale fulfils all FDA criteria for a clinician-reported scale: ability to detect change, clarity, construct validity, relevance, repeatability, reproducibility, response range and usability. The VIBe Scale is the first surgeon-validated scale designed for consistent and reliable assessment of intraoperative bleeding severity. The scale classifies bleeding severity into five distinct grades – Grade 0 (‘no bleeding’), Grade 1 (‘mild’), Grade 2 (‘moderate’), Grade 3 (‘severe’) and Grade 4 (‘life threatening’) – the distinct visual presentation, anatomic appearance, qualitative description and visually estimated rate of blood loss to five grades of severity (Figure 3). This is a simple tool that can be integrated into surgical practice and encompasses visual, descriptive and data-driven elements (Lewis et al 2017).
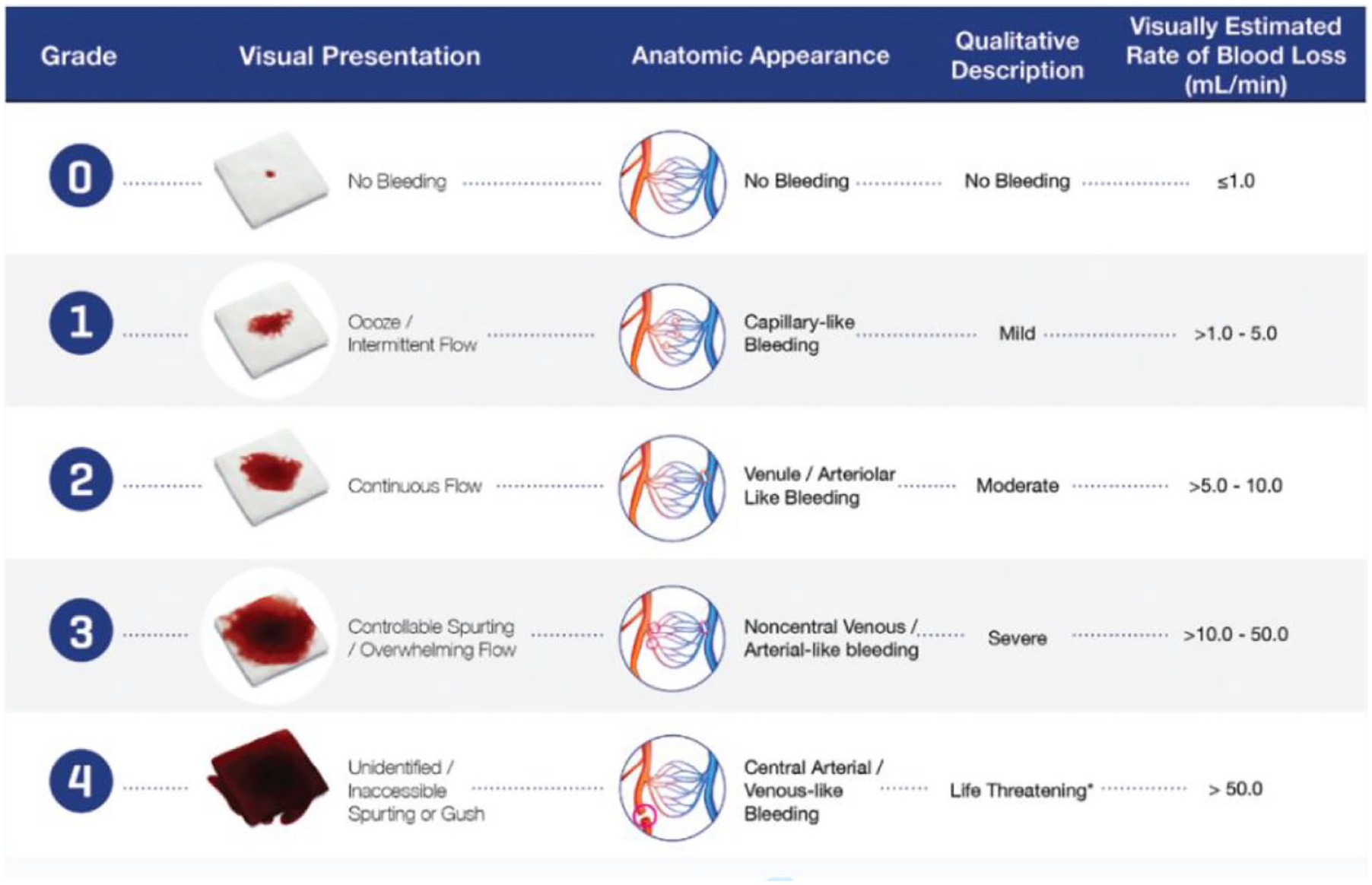
Alternate representation of the VIBe Scale: Streamlining Visual Presentation to Anatomy, Qualitative Descriptions and Estimated Blood Loss. This is a useful representation for scrub staff due to the incorporation of swab images (Lewis et al 2017)
Recent studies have described the utility of the VIBe Scale across a variety of surgical specialties (Ramia et al 2022, Sciubba et al 2022, Siebert et al 2019, Tan et al 2023), and a recent global observational study also provides human factors verification of the VIBe Scale across multiple additional surgical specialties (Smith et al 2024, Tibi et al 2023).
Project methods
Project design and approach to improvement
A descriptive quality improvement study was carried out. The target audience was invited to take part in the study and the participants received a hard copy of a questionnaire to complete (see Supplemental files 1 and 2).
A multidisciplinary event with several themes was the first opportunity to introduce the VIBe Scale. Outcomes of the major haemorrhage simulation event and human factors in the OR setting were discussed by an anaesthetist. The surgeon led a discussion on renal anatomy, surgical procedures and risks of haemorrhage. Finally, the introduction of the VIBe Scale was presented, along with an introduction to an amended surgical brief.
The bleeding scale was introduced, including its background and visual representations. It was discussed how this scale could be used as a communication tool between team members to describe blood loss, and as a trigger to take action.
As well as incorporating the VIBe Scale and anticipated blood loss events, the amended surgical brief also used height and weight to calculate the estimated blood volume (EBV), 10% EBV loss and 20% EBV loss (Nagelhout et al 2014).
The 10% and 20% EBV loss limits were set as blood loss triggers for actions among the surgical team, such as notifying the anaesthetist, preparing additional equipment and so on.
A surgical debrief was introduced, which included a questionnaire to evaluate the intraoperative application of the VIBe Scale. The debrief also allowed the team to reconvene and discuss any issues noted during the operating day.
Population
Thirty-three nurses from the OR participated in the study. Questionnaires were offered to all staff. No inclusion or exclusion criteria were applied; however, participants had the option to opt out of the study at any time.
Ethical aspects
The study was approved by the hospital as a quality improvement project and therefore did not require Institutional Review Board approval. Informed consent was obtained from all participants, and confidentiality and anonymity were guaranteed. Participants were given the option to withdraw consent at any time.
Implementation process
A multidisciplinary approach to the review of outcomes and an open and inclusive discussion around potential improvements to team communication paved the way for the introduction of a change to the preoperative surgical brief, the postoperative debrief but also introduction of the VIBe Scale (Figure 4).
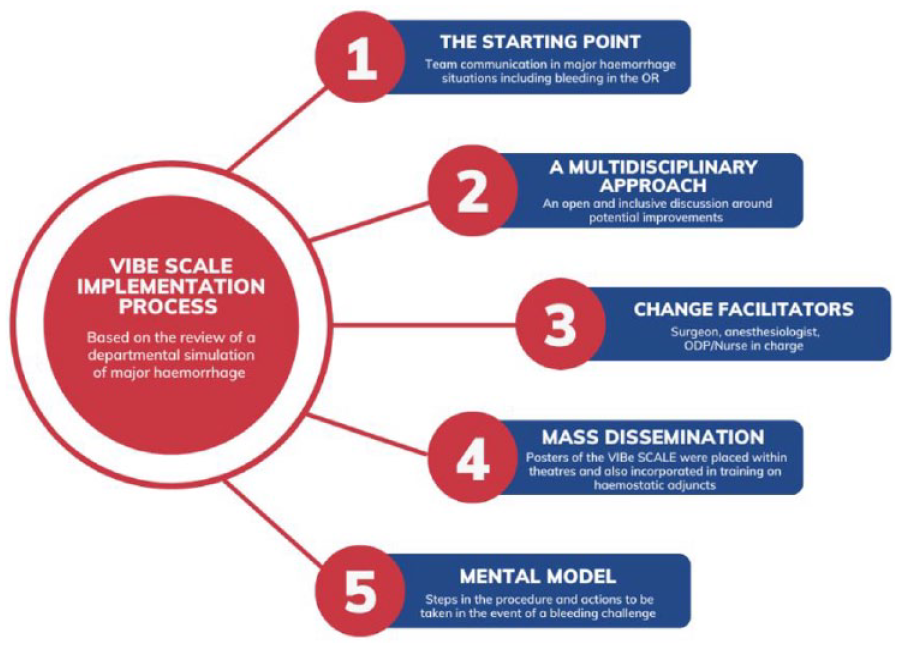
VIBe Scale implementation process
Facilitators of change were from a multidisciplinary background – surgeon, anaesthetist, operating department practitioner (ODP) or charge nurse. This allowed dissemination of information to many groups. This multidisciplinary approach demonstrated strong leadership among the facilitators and encouraged participation from team members.
Posters and information folders discussing the VIBe Scale were placed in the OR. The VIBe Scale was incorporated in the training on haemostatic adjuncts, to ensure team members were confident in their understanding of the correct type of passive and active haemostat for the grade and type of bleeding (Table 1), thereby allowing for preparedness and a common mental model on actions to be taken in the event of a bleeding challenge.
Variables and hypotheses
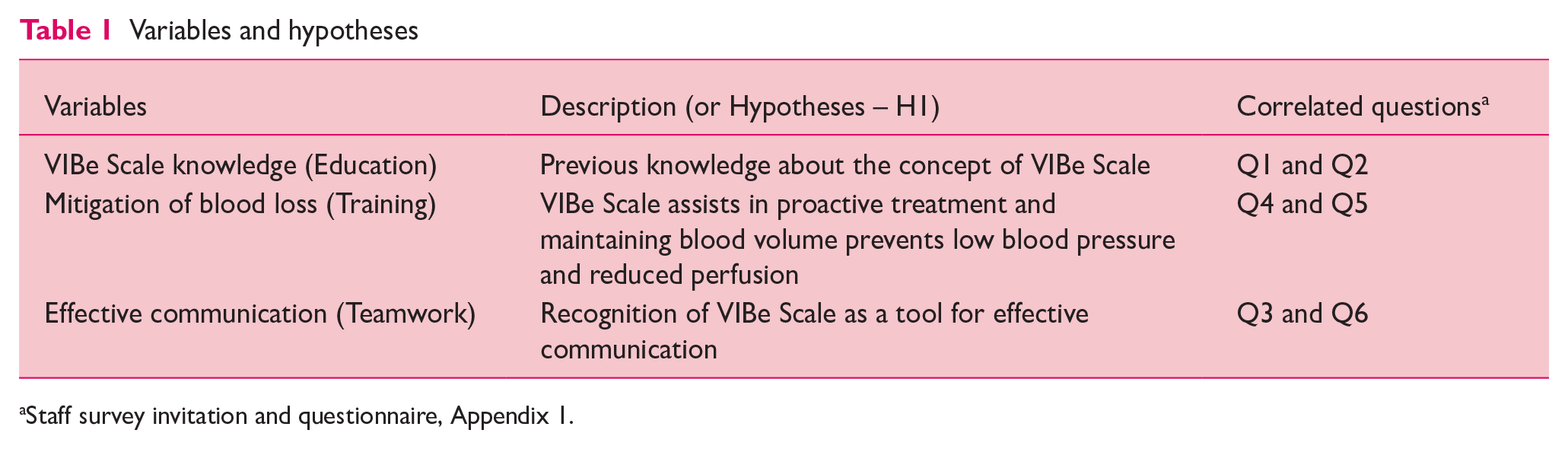
Staff survey invitation and questionnaire, Appendix 1.
Data collection methods
Questionnaires were handed out or made available for participants to complete.
Questionnaire design:
The questionnaire was designed to create a snapshot of how many theatre nurses had attended the introductory lecture on the VIBe Scale and what they thought of the VIBe Scale as a communication tool and whether they had used the scale.
Training session:
A folder with the resources pertaining to the amended surgical brief incorporating the VIBe Scale was used. Each theatre team was then briefed on the contents and discussed the VIBe Scale and how this could be used in communication relating to a bleeding event.
Measured variables
Three main categories were used: Education, Training and Teamwork. For each of these categories, a measure was defined (Table 2).
Types and indications of surgical haemostats and tissue sealants
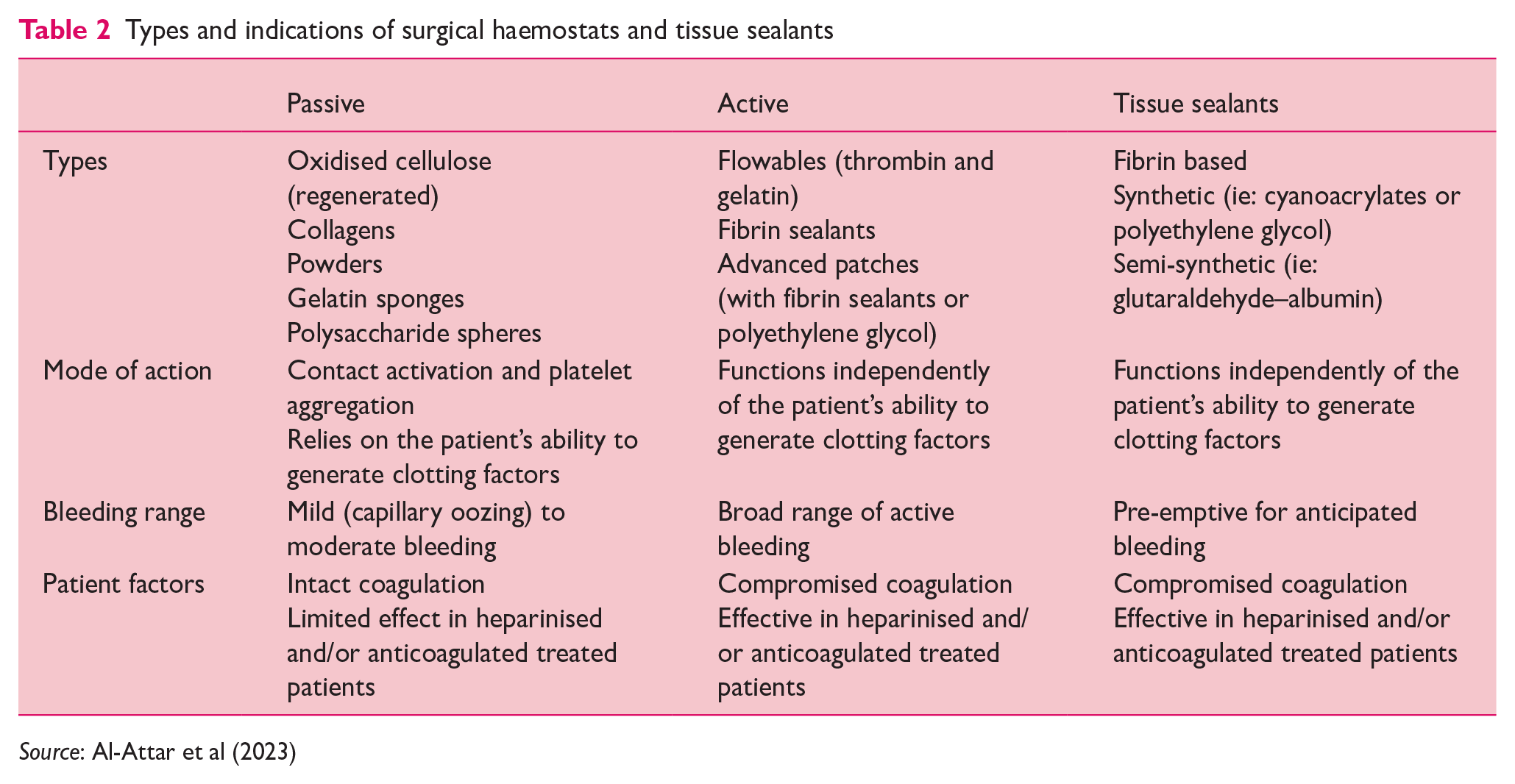
Source: Al-Attar et al (2023)
Data analysis methods
The data were collected and transposed to a spreadsheet (Microsoft Office Excel® 2008) and tabulated for descriptive analysis.
Descriptive statistical analysis was carried out to characterise the sample and the variables: (1) Professional knowledge, practice-based knowledge and awareness (self-perceived knowledge), (2) Team management and effective communication and (3) Patient safety, clinical practice and quality improvement.
Outcomes
The survey included 33 respondents, all nurses with experience in the surgical area and trained on management of severe perioperative bleeding.
Nurses’ professional knowledge of the VIBe Scale
Most participants (19/33, 58%) did not attend the introductory lecture, however, despite this, 42% of participants (8/19) understood the concept of VIBe Scale. All participants who attended the lecture (14/33, 42%) reported understanding the concept of the VIBe Scale. Overall, 22 of the 33 participants (67%) understood the use of the VIBe Scale (Figure 5).
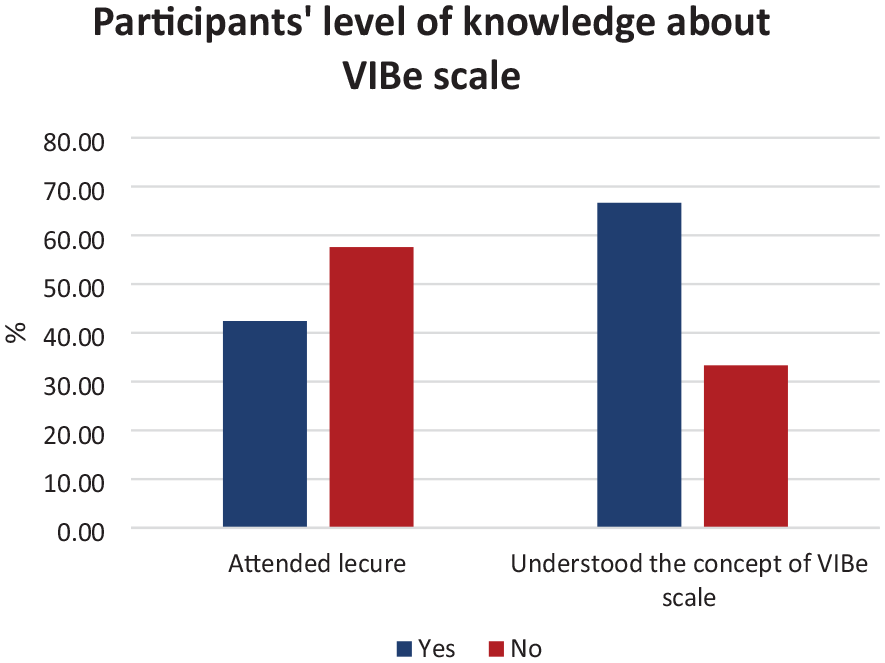
VIBe Scale knowledge
Patient safety, clinical practice and quality improvement
Majority of the participants (79%) did not have any experience or had not seen the VIBe Scale being used within the OR; however, they believed (67%) that the VIBe Scale could improve situational awareness.
Team management and effective communication
Although many participants (58%) mentioned that they did not witness the amended surgical briefing, most of them (64%) reported that they could see the VIBe Scale as a tool to improve communication.
Calculating and noting estimated blood loss levels at 10% and 20% of EBV as triggers on the OR display board, prior to the procedure commencing, made it easier for the participants to monitor the rate of blood loss, enhancing communication between team members when percentage blood loss triggers were met (Figure 6).
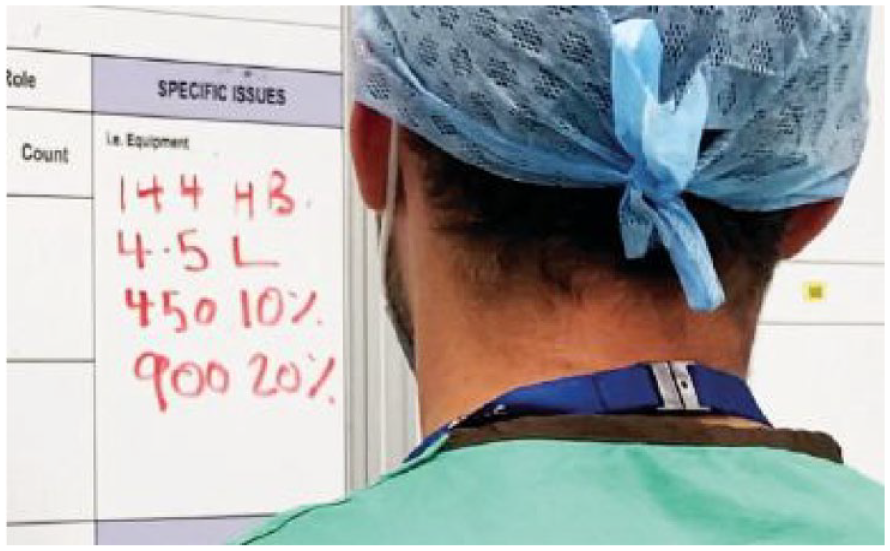
Including estimated blood loss levels at 10% and 20% as blood loss triggers on the operating room display board. Image shows Hb, and estimated blood volume for a 64.3 kg patient with calculation for 10% and 20% of EBV
Discussion
Substantial blood loss during surgery can result in increased patient morbidity and mortality, and clear and effective communication within the OR team can mitigate this (Bible et al 2018).
Many factors can contribute to a risk of excess bleeding during surgical interventions; although not all complications can be prevented, a full working knowledge of most likely complications, haemostatic tools and adjuncts, and concise communication with team members can prevent significant blood loss (Herford & Lowe 2018).
In this study, most participants reported that they easily understood the concept of the VIBe Scale (67%) and that this tool could increase situational awareness (67%). In a previous study, this scale was found to be usable, clear and clinically relevant with excellent reliability (Lewis et al 2017).
Visual estimation has been the most used method of assessing bleeding and an accurate estimation of blood loss is crucial as it can substantially alter the timing of blood transfusion and direct interventions to control bleeding. Inaccurate estimation of blood loss can lead to either over or under transfusion (Anya et al 2019).
Many investigators have attempted to devise new methods for an accurate determination of blood loss. Ali Algadiem et al (2016) assessed blood loss using Gauze Visual Analogue tool and showed that the absorptive capacity of different gauze sizes was determined when fully soaked with blood. The authors concluded that the use of a visual analogue may increase the accuracy of blood loss estimation. However, if another type or size of gauze is used, this analogue may be inaccurate for use in all situations.
Some studies emphasise that teaching staff members on how to estimate blood loss is effective in increasing the accuracy of visual estimation (Dildy et al 2004, Schorn 2010, Toledo et al 2010, Zuckerwise et al 2014).
Recently, Smith et al (2024) showed that the VIBe Scale is an independent predictor of intraoperative, postoperative and overall blood transfusion, estimated blood loss (EBL) and postoperative day one drain output. The study evaluated the clinical relevance of the VIBe Scale in 121 patients under thoracolumbar spine surgery. VIBe scores were correlated with an increased likelihood of intraoperative blood transfusion (β = 2.46, p = 0.012), postoperative blood transfusion (β = 2.36, p = 0.015), any transfusion (β = 2.49, p < 0.001), total transfusion volume (β = 180.8, p = 0.020) and EBL (β = 409, p < 0.001). They concluded that the VIBe Scale is clinically relevant and has potential utility in both the clinical and research settings for improving haemostasis.
In a post-test survey, using a novel visual aid to improve estimation of blood loss, 90% of participants (n = 136) reported subjective improvement in estimation ability, and the accuracy of blood volume estimation was not correlated with years of experience (Zuckerwise et al 2014).
All participants who attended the lecture reported understanding the concept of the VIBe Scale, and even some of those who did not attend the lecture but saw the VIBe Scale in practice, understood the concept of the scale.
Based on evaluations, some improvement actions were considered and implemented:
Further training on surgical instruments for theatre staff was required;
Training folders were created as a resource on surgical instruments;
Redevelopment of an enhanced surgical brief;
Debrief end of each theatre session with a focus on communication and managing blood loss;
Further or regular updates on haemostatic agents required;
An escalation poster was developed (Figure 7).
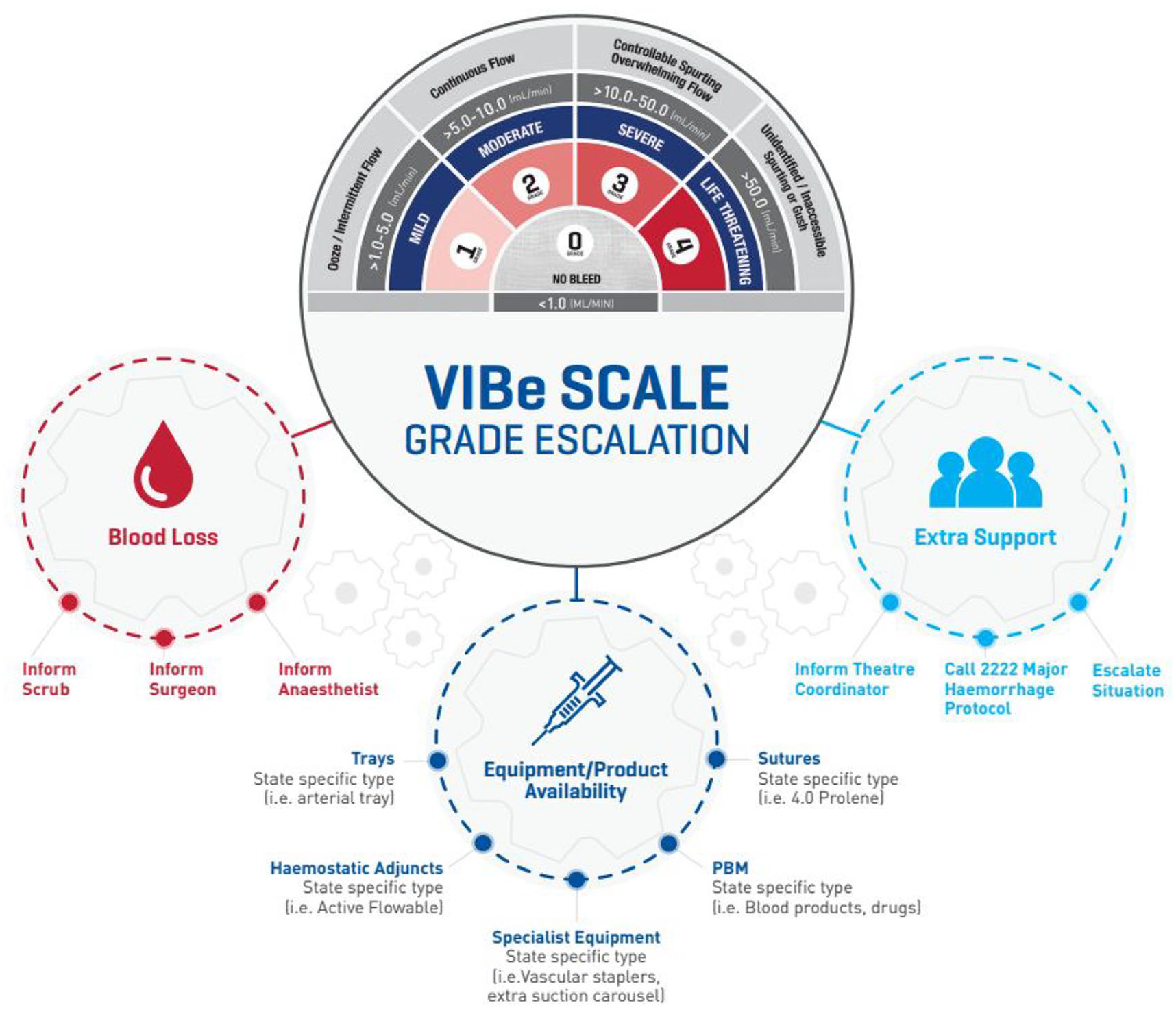
VIBe Scale Grade Escalation Poster – illustrates how the escalation process should be considered and actions taken. It also illustrates how content linked to the VIBe Scale was organised in posters and folders for equipment and made available for wider dissemination
A possible limitation to the study is the fact that the survey was carried out in a single geographical area; the practice and characteristics of the professional population may be different in other regions or institutions, although the authors believe this to be unlikely.
Conclusion
Teamwork, education and training through structured initiatives are the most effective mechanism to improve patient safety. Accepting the contributions of team members, reducing barriers to reporting errors and promoting a work environment, where all individuals work together, will have the most significant effect on improving patient and staff safety (Rodziewicz et al 2023). In this sense, effective teamwork and communication are crucial determinants of patient safety in the OR, and the VIBe Scale is potentially a tool to make clinical practice safer.
The introduction of the VIBe Scale through a quality improvement project into clinical practice has been facilitated by the multidisciplinary membership of the implementation team. The multidisciplinary team approach allowed all stakeholders to be educated, trained and conduct the test of change.
Feedback demonstrates that discussing potential bleeding scenarios for the procedure utilising the VIBe Scale at the surgical brief increases the situational awareness of the nursing and broader OR team. The enhanced brief should include the following:
A description of the potential types of bleeding utilising the VIBe Scale;
Incorporation of potential actions to be taken and haemostatic adjuncts to be utilised or available;
Along with having a focus on blood loss by calculating the estimate blood volume for the individual patient, with 10% and 20% as blood loss triggers.
A significant number of nurses found that the VIBe Scale was an effective communication tool during bleeding events, by offering a shared mental model between nursing, anaesthetic and surgical team members.
The introduction of a formal surgical debrief at the end of the day allowed the team to discuss and reflect on their performance that day. It also allowed capture of important metrics such as need for blood products, equipment issues, staffing issues and any educational or development issues related to patient blood management.
In summary, the VIBe Scale is an incredibly useful tool in the communication of bleeding pre, during and after an operative procedure. It allows team communication throughout the case. It breaks down barriers, including hierarchy, between team members and professionals to allow a singular focus on blood loss, potentially minimising the requirement for further interventions and mitigating the associated postoperative complications of blood loss. Incorporating the VIBe Scale allows the nursing and support team to be more focused on blood loss and, crucially, empowers nurses to speak up and convey and discuss blood loss not just to the surgeon but to the anaesthetist and other members of the surgical team.
Key points
VIBe Scale is a simple tool that can be readily integrated into everyday surgical practice and encompasses visual, descriptive and data-driven elements.
VIBe Scale is an effective communication tool during bleeding events, offering a shared mental model between nursing, anaesthetic and surgical team members.
VIBe Scale has the potential to improve situational awareness of intraoperative bleeding events and how to describe them.
VIBe Scale empowers nurses to speak up and convey and discuss blood loss with the whole surgical team.
Supplemental Material
sj-docx-1-ppj-10.1177_17504589241287744 – Supplemental material for Clinical implementation of the Validated Intraoperative Bleeding Scale: Perioperative patient management and effective team communication from the nurses’ perspective
Supplemental material, sj-docx-1-ppj-10.1177_17504589241287744 for Clinical implementation of the Validated Intraoperative Bleeding Scale: Perioperative patient management and effective team communication from the nurses’ perspective by Clare Sewell, Becky L Whiteman, Flavia C Morone Pinto and Steve Leung in Journal of Perioperative Practice
Footnotes
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Disclosures: CS have not personally received any payment in relation to this manuscript. He have received honoraria for presentations from Baxter Healthcare and Olympus Medical. BLW have not personally received any payment in relation to this manuscript. He is an employee of Baxter Healthcare Limited. SL have not personally received any payment in relation to this manuscript. He have received honoraria for presentations from Baxter Healthcare and Olympus Medical. FCMP is an employee of Baxter Healthcare Limited and writing manuscripts is part of my role. General: Open access fees was supported from a grant within Baxter Healthcare.
Funding
The author(s) received no financial support for the research, authorship and publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.