
Abstract
Aim:
The aim of the study was to explore the value of debriefing to enhance learning within operating theatres.
Methods:
A sequential mixed method study was undertaken at a local District General Hospital Trust in 2020. A total of 106 surveys were distributed to all multidisciplinary team members based in the trauma and orthopaedic theatres. Following the survey stage, 11 in-depth semi-structured qualitative interviews were undertaken with volunteers from the survey stage which included a range of health care professionals.
Findings:
Participants identified debriefing as a valuable tool for learning and reflection. However, significant barriers were identified, including lack of time and conflicting priorities. Some interviewees referred to the current debriefing process as a ‘tick box’ and a ‘herding cats’ exercise, attributing it to a lack of structure, leadership and organisational buy-in.
Conclusions:
Debriefing in the operating theatre is a valuable tool for individual and team learning. However, formalising the structure of the debriefing, along with joint team and organisational commitment, was deemed vital in optimising the value of debriefings in the future.
Keywords
Introduction
Debriefing aims to improve the safety culture in operating theatres by promoting reflection and enabling improvement in team performance (AHRQ 2019). The value of the debrief for everyday reflection (Abatzis & Littlewood 2015), individual and team learning is, however, often overlooked (Arriaga et al 2020).
Across the literature, there is disparity in what constitutes debriefing in operating theatres. For example, Bartz-Kurycki et al (2017) have used debriefing consistently with the ‘Sign-out’ phase of the World Health Organization (WHO 2009) Safety Checklist. The focus of the post-surgical debrief varies from identifying process failures (Bandari et al 2012) to reflecting on non technical skills (Bethune et al 2011, Mundt et al 2020). The structure of the debrief (Leong et al 2017), training debrief facilitators (Marks et al 2014) and creating a positive atmosphere (Mundt et al 2020) have been deemed key to improve the efficacy of the debrief. Team engagement and organisational buy-in have been highlighted as crucial to effective implementation (Brindle et al 2018, Finch et al 2019, Hill et al 2015) and to manage resistance (Zuckerman et al 2012).
Despite the benefits, lack of time and the timing of the debrief are significant barriers to the effective implementation of debriefing in operating theatres (Ahmed et al 2012, Leong et al 2017, Mundt et al 2020). Some studies reported a decline in the debriefing process over time (Bethune et al 2011, Brindle et al 2018, Sacks et al 2015). Leong et al (2017) and Finch et al (2019) attributed this to loss of leadership, communication breakdown, disengagement, disillusion and perceived lack of value and feedback within the team.
There is an obvious lack of focus on the educational value of the debrief in operating theatres in the literature. Therefore, this study set out to explore the role of debriefing to enhance learning within operating theatres. The main objectives were to (1) identify individual attitudes towards debriefing, (2) identify the perceived barriers and facilitators of the debriefing process and (3) explore the role of debriefing in operating theatres for individual and team learning.
Methods
A sequential mixed method design (Creswell 2014) was adopted to establish patterns and explore attitudes and experiences of debriefing across multi-professional groups. A bespoke survey was designed and the findings were used to inform a semi-structured interview schedule.
Following a pilot survey, multidisciplinary members of the T&O operating theatre team (n=106) were invited to participate in this study. The online General Data Protection Regulations (GDPR) approved JISC platform was used to distribute and gather the survey results. Participants were requested to provide contact details if they were willing to participate in the interviews. Thematic analysis of the surveys was conducted initially using the NVivo 12 software followed by a further manual review by the researchers for triangulation and meaningful interpretation of the ideas within the context of the topic (Clarke & Braun 2013). An iterative process was used, and the overarching codes of barriers and facilitators of debriefing were expanded as further themes emerged.
Interviews (n=11) were scheduled at mutually convenient times and were conducted, recorded, transcribed and coded by the first author, a perioperative nurse undertaking Master’s in Clinical Education. The NVivo 12 software was used to code the interview data using a two-staged process, first inductively from the questions, and then deductively from the interview content. A sample was then reviewed to ensure consistency of coding.
Ethics approval
Approval was provided by a university ethics board for this study (Ref 19/20-536) and agreement was given by the trust involved. This study was also approved by the Health Research Authority via their Integrated Research Application System (IRAS ID 266011).
Results
A 29% survey response rate (n=31) was accomplished, which is within the expected range for health care professionals (Cunningham 2015). This was representative of the multi-professional groups within operating theatres, including surgeons, anaesthetists, nurses, operating department practitioners and health care assistants. This included both consultants and junior doctors within the medical group.
Eleven health care professionals were then interviewed: anaesthetists (n=3), surgeons (n=2), nurses (n=2), operating department practitioners (ODP, n=2), surgical care practitioner (SCP, n=1) and a health care assistant (HCA, n=1).
Value / purpose of debrief
Debriefing was consistently identified as a valuable learning opportunity to enhance teamwork and patient care by survey respondents and interviewees alike. It was valued as tool for both individual and team reflection (Table 1).
Survey respondents views on the purpose of the debrief
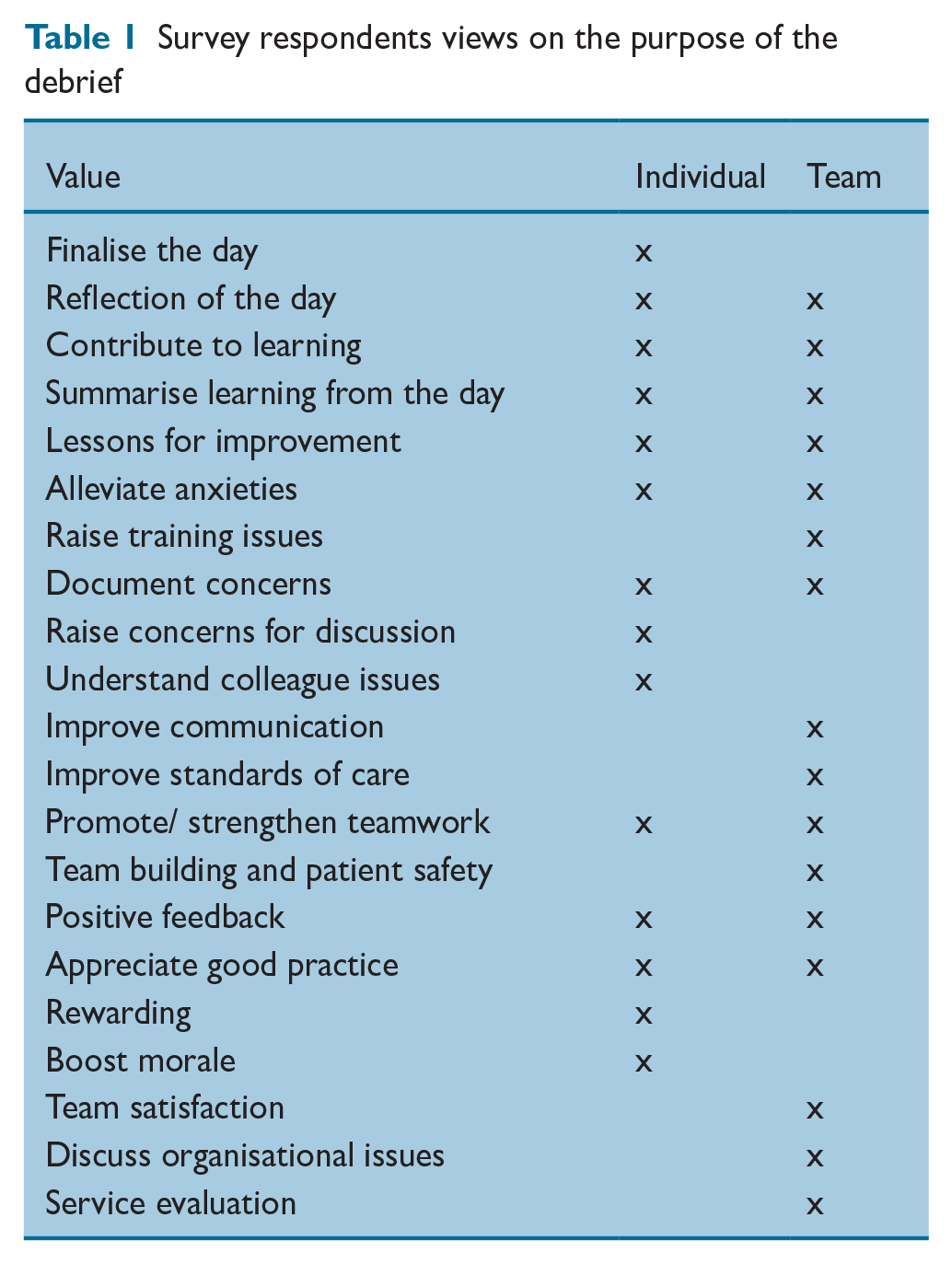
In addition, one survey participant clearly labelled a team that does not value debrief as a ‘dysfunctional team.’ The general consensus was that debriefs were most valuable when everyone was engaged in the process:
‘The surgeon said at the end, we could’ve planned our day better and we could have included the radiographer in our morning discussion. So, the following day, we got the radiographer up at the beginning of the day.’
A clear example of when debriefs were successful was provided by one participant in the quote above.
Team engagement and leadership in the debriefing process
Across the professional groups, lack of leadership and assertiveness were identified to be significant barriers to the implementation of debrief. A key observation was that unlike the team brief which is obligatory, there was no apparent formal requirement to attend a debrief at the end of the day.
Figure 1 shows that lack of engagement (n=17) and time pressures (n=16) were the most recurring themes in the survey. Other barriers to implementation of debriefs identified were overrunning lists (41%, n=13), conflicting priorities (35%, n=11) and team dispersion (38%, n=12). Any associated staff changes added further barriers to perform a meaningful debrief.
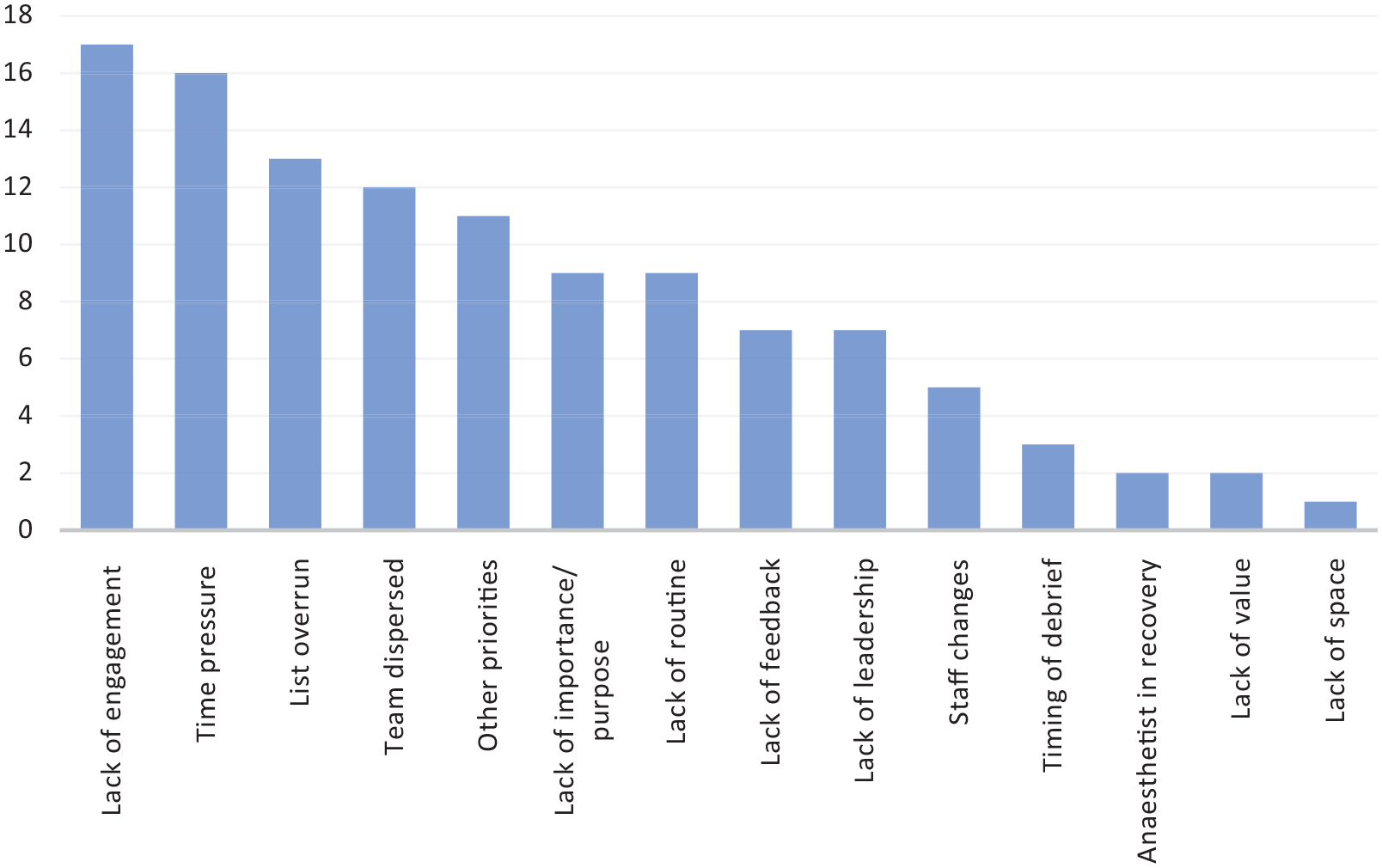
Frequency of themes recurring in the survey
Timing of debrief
Interviewees (n=10) deliberated the ideal time to perform the debrief. Typically, debriefs were conducted after the sign-out of the last patient on the list. However, this sometimes coincided or competed with critical activities such as extubating the patient. Other priorities affecting debriefs were identified as theatre staff tidying up, surgeons finishing operation notes and anaesthetists’ handover of patients to recovery. One participant highlighted that the various finishing times of the activities of the multidisciplinary team made debriefing a ‘herding cats exercise.’ During the study, this was further complicated by the COVID-19-related infection control requirements (PHE 2020). Doffing had to be performed in a designated area away from the main operating room and typically, unless there were pressing issues, staff did not return to theatre
‘. . . my experience of when the debrief is [sic] properly happened is on days we are finishing early.’ ‘it is probably something that is thought about more if . . . things have gone wrong’
Debriefs appeared to be more likely to happen when the lists finished on time or if substantial problems had occurred during the day. Across the survey and interview participants (n=9), lack of understanding of the importance of debrief and lack of feedback were thought to have resulted in a disinterest in the process.
Team and organisational culture
‘unfortunately it is the classic human factor thing of you know the organisational hierarchy influences the benefit that people may feel or the ability to contribute.’ ‘it is harder for me to say something when there is a consultant in the room’ ‘Grades have nothing to do with it . . .’ debrief could ‘hurt staff feelings if they have not been praised for their hard work despite some failings.’
There seemed to be a difference in opinion as to whether hierarchy influenced the debriefs. Most interviewees (n=9) identified that due to the transient nature of theatre teams, leadership varied from day-to-day as did the capacity of team members to initiate the debrief. One participant alluded that dominant characters within the team could either enable or disable the implementation of the debriefs. In this environment, team members felt vulnerable and less empowered to participate. Conversations during debrief were sometimes thought to be dominated by the lead surgeon, anaesthetist and team leader. This was attributed to a ‘top down’ culture and if the aforementioned members of the team didn’t advocate for a debrief, it did not happen. On occasion, debrief was perceived to be a punitive process.
Familiarity between team members and lack of assertiveness and confidence, especially where junior staff or staff from different ethnic backgrounds were involved, were identified as additional contributing factors to the effectiveness of the debrief. A formalised structure was proposed to help people speak up, as the focus then shifts from individuals to roles.
Impact of structure and training on debriefing
‘(debriefs) should be short and succinct like the . . . AAR.’ ‘. . . we are not receptive enough to pick up some of the more subtle things at the moment because it’s not structured and not, perhaps valued as much as it should be.’
Mostly, participants acknowledged that a lack of structure and routine for ‘how’ and ‘when’ the debriefs were performed potentially made debriefs a ‘tick box exercise.’ Interviewees also acknowledged that apart from the debrief discussions as part of human factors training, they were not trained to formally lead a post-surgery debrief. Most debriefs were reported to be verbal in nature and there was uncertainty on how this information was dealt with.
Suggestions for improvement
Across the survey and interview participants, suggestions to improve debriefs centred around three key issues: engagement, leadership and timely feedback from issues identified in the debrief to raise the profile and credibility of the debriefing process. Overall, re-engaging team members and organisational buy-in were identified as the way forward to embed debriefing:
‘it’s about translating some of the tools, techniques, tips, language from the educational debriefs – in simulation, for example.’ ‘it could be themed at the briefing at the beginning’ ‘recognise that debrief isn’t just picking up when things have gone wrong . . . I like the idea of AAR.’ ‘organisational sign up that will accept that you are going to spend 5 to 10 minutes doing this and it has to be factored into the length of the list.’
Raising awareness and expectations, involving the whole team, identifying the best time for a debrief as a team and challenging the difficult personalities were suggestions made for re-engaging team members. Allocated time within the scheduled sessions and feedback on issues arising from the debrief were identified as key for engagement in meaningful debriefs. Different approaches such as the After Action Review (AAR) (Sawyer & Deering 2013) and Learning for Excellence (LfE) (Cope et al 2019) for positive reinforcement, and adapting educational frameworks were proposed to structure the debriefs.
Other suggestions related to improving the value of the debriefs such as making notes throughout the day to feed into the process, training for debriefing and learning from positive events.
Discussion
This study has clearly highlighted that post-surgery debriefing is considered to be an important reflection and learning opportunity for both individuals and teams. It is not necessarily the lack of value, but the logistical challenges, and the lack of time and resources that influence the debriefing process in operating theatres. In this study, it was clear that where meaningful debriefs have been implemented, their value in identifying concerns and lessons for improvement, promoting teamwork and boosting morale was acknowledged. Nevertheless, psychological safety is key to enable participation.
A potential challenge to implementation highlighted in this study is due to the lack of a structured debrief form to complement the debriefs. Zuckerman et al (2012) reported an increase in their compliance from 47% to 90% with the use of a structured debrief form on an electronic whiteboard. This would also serve to be a visual reminder to the whole team in the operating theatre and potentially increase the chances of a debrief happening despite the logistical challenges.
While it is evident that staff engagement is crucial, the current debriefing model, widely used in operating theatres, fails to appreciate a fundamental principle of learning, which is exploring ‘why’ the session was successful or unsuccessful. In their seminal paper, Hollnagel et al (2015) challenge the traditional view of safety management, from understanding why things go wrong (Safety I) to why things go right (Safety II), particularly in complex health care systems, where flexible transient teams have to adapt to constantly changing situations. By focussing on learning from mistakes, other potentially valuable learning opportunities could be lost.
Despite the challenges over the years, a definite positive cultural shift has been reported in the perception of debriefings in the operating theatre (Leong et al 2017, Marks et al 2014). In this study, participants consistently identified feedback, scheduled time, staff engagement and positive reinforcement as key enablers to the implementation of debriefing in operating theatres. Moreover, while debriefs promote constructive criticism, they were sometimes perceived as punitive if team efforts were not appreciated. In the light of these views, embracing a model based on positive reinforcement principles of LfE (Cope et al 2019) would be useful to promote debriefs.
Conclusion
Evident lack of structure and motivation to complete a debrief have been identified as factors detrimental to implementing debriefings in the literature (Leong et al 2017, Marks et al 2014) and in this study. It is clear that the purpose of debriefing needs to be redefined before redesigning the current structure. Staff empowerment, hierarchy and staff engagement remain potential barriers to the implementation of debriefing. Leadership both from the wider organisation and within surgical teams is vital to rectify this and to raise the profile of debriefing and its role in organisational learning. At the same time, efforts should be made to improve the debriefing process through better structure and team training while acknowledging that further research is required to understand the impact of these on the efficacy of debriefing in operating theatres.
Although time is perceived as an obstacle, only one study to date (Mundt et al 2020) has measured the time required for a debrief. Quantifying the actual time required for a routine post session debrief would have significant benefits, not least to highlight that, if carried out effectively, a debrief could be meaningfully incorporated within surgical sessions without becoming ‘herding cats’ or ‘tick box’ exercises. With well designed structures and facilitative leadership, these opportunities could also be leveraged to optimise organisational learning.