
Abstract
Following the COVID-19 pandemic, National Health Service trusts nationwide are faced with a significant backlog of patients to clear, furthering the strain on the National Health Service. In an era where sustainability and efficient management of National Health Services is of paramount importance, the introduction of a Golden Theatre Initiative could alleviate day-to-day pressures and assist in the smooth running of a modern-day theatre department. Preoperative burdens on patients can be both physical and psychological, resulting in fears and anxiety surrounding the unknown. It is not uncommon for elective procedures to be cancelled last minute due to pressures; however, this can hugely impact the willingness of a patient to comply in the future, with a potential adverse effect on their health. Cost-effectiveness, reduction on waiting lists and overall negative patient impact, in addition to an improvement on first case start times following the introduction of the Golden Patient Initiative, have been observed nationally. It is believed with the introduction of a Golden Theatre Initiative; these improvements could greatly change the current running of elective waiting lists nationally.
Introduction
Delays to the start of operating theatre lists internationally have been a regular occurrence for several decades (Bridges 2017, Sharouf et al 2017, Tulloch et al 2020). Reasons for the delays appear to be numerous; however, the literature suggests that simple changes can improve start times, reduce delays and have a positive effect on overall efficiency with prompt finish times, reduced cancellations and improved patient satisfaction (Bridges 2017, Tulloch et al 2020). This article aims to examine these changes, with a view to improving attitudes, work ethic and compliance within the current National Health Service (NHS). The ‘Golden Patient’ Initiative (GPI), as first introduced by Javed et al (2013), enforced a prompt start time which minimised the risk of patient cancellation, thus generating greater theatre capacity. The GPI is a preselected first patient who has been medically optimised, consented, marked and prepared for surgery the previous night to reduce delays on the day of surgery and enhance efficiency. This initiative has been utilised, with success; however, the effectiveness halts at the end of the first procedure. Further patients listed may not be optimised, discussions regarding results pre-theatre may occur, and delays could be seen despite having started the day with the Golden Patient (GP).
The author, therefore, suggests the utilisation of a ‘Golden Theatre’, based on the ideology of the GPI, furthering the capacity of the operating list for that day. Understandably, the implementation of an initiative, such as this would be multifactorial, and initially complex in nature, requiring appropriate leadership and change management skills. Throughout this article, ideas for implementation of the Golden Theatre Initiative will be discussed, leadership techniques in health care examined and change management models reviewed.
The psychological needs of each patient should be considered in relation to effective utilisation of an operating theatre. Needing, and subsequently undergoing, a surgical procedure can place a huge burden both physically and psychologically on a patient and their family members (Sharouf et al 2017). As a result, any last-minute cancellation can result in significant distress and ultimately a lack of trust in the service itself (Bridges 2017). NHS trusts within the United Kingdom were instructed to suspend all elective, non-essential surgery for at least three months in April 2020 to facilitate redeployment of staff and repurposing of beds and operating theatres in anticipation of COVID-19 patients (Iacobucci 2020). As a direct result of this, many patients have already had to wait longer than usually necessary for procedures; therefore, maximising the available time and reducing any further wait for patient treatment is paramount (Howlett & Wood 2022).
Howlett & Wood (2022) state that an indirect result of the COVID-19 pandemic has been the rate of cancellation of elective surgery. An NHS waiting list of 4.4 million in February 2020 exponentially increased to 5.7 million by August 2021, as a result of the rapidly unfolding pandemic. The study conducted by Howlett & Wood (2022) aimed to predict the future size of the elective surgery waiting list up to December 2025, highlighting the volume of cancelled surgery would be in excess of 28 million elective operations worldwide. Carr et al (2021) affirm that the effect on planned surgery has become a significant issue and the number of patients awaiting treatment is the highest it has ever been within the UK NHS. As all surgical disciplines are experiencing similar backlogs, ultimately the patients are suffering delays to treatment, worry of the unknown and less choice of treatment options available to them, further causing health inequalities (Carr et al 2021, Howlett & Wood 2022).
Khan et al (2022) convey that operating theatres and associated resources take up a vast proportion of health care costs; more than 30% of all costs. It is thought that over one third of all NHS-operating lists experience a delay of more than 30 minutes. Therefore, any inefficiencies come at a cost to individual trusts and, ultimately, patients themselves. The number of patients on elective waiting lists has grown exponentially since the COVID-19 pandemic, demonstrating the pressing need for operating theatre utilisation to be effective and efficient, eliminating unnecessary delays and cancellations. Therefore, as many elective lists have already experienced cancellations due to the COVID-19 pandemic, it is imperative now, more than ever efficient running of operating lists ensue, requiring better management of time and prevention of unnecessary delays (Lucye et al 2024).
The author has worked as a scrub nurse across multiple settings, latterly within a tertiary specialist neurosurgical hospital. There are seven elective operating theatres, in use from the hours of 08:00–18:00 Monday to Friday, with the addition of one emergency theatre, in use 24 hours a day. More than 25 consultant neurosurgeons cover procedures, including spine, complex spine, trauma, hydrocephalus, oncology, skull base and vascular. In addition to this, there are five consultant pain specialists who utilise the theatres regularly. Theatre over-runs and delays for various reasons are a regular occurrence, affecting patient treatment, theatre efficiency and staff morale as experienced in practice. NHS trusts nationwide have expectations to populate operating theatre lists to, what can only be described as unrealistic levels at times, despite the identification of potential over-runs due to, list over-scheduling, inadequate combination of perioperative staff due to skill mix and knowledge and availability of equipment. As a result, over-runs and patient cancellations occur daily, diminishing an already low staff morale and increasing patient dissatisfaction. With the ‘Golden Theatre Initiative’ suggested throughout this assignment, the author hopes to address some of the current issues, with an aim to improve the service, efficiency and overall staff assurance.
Aims
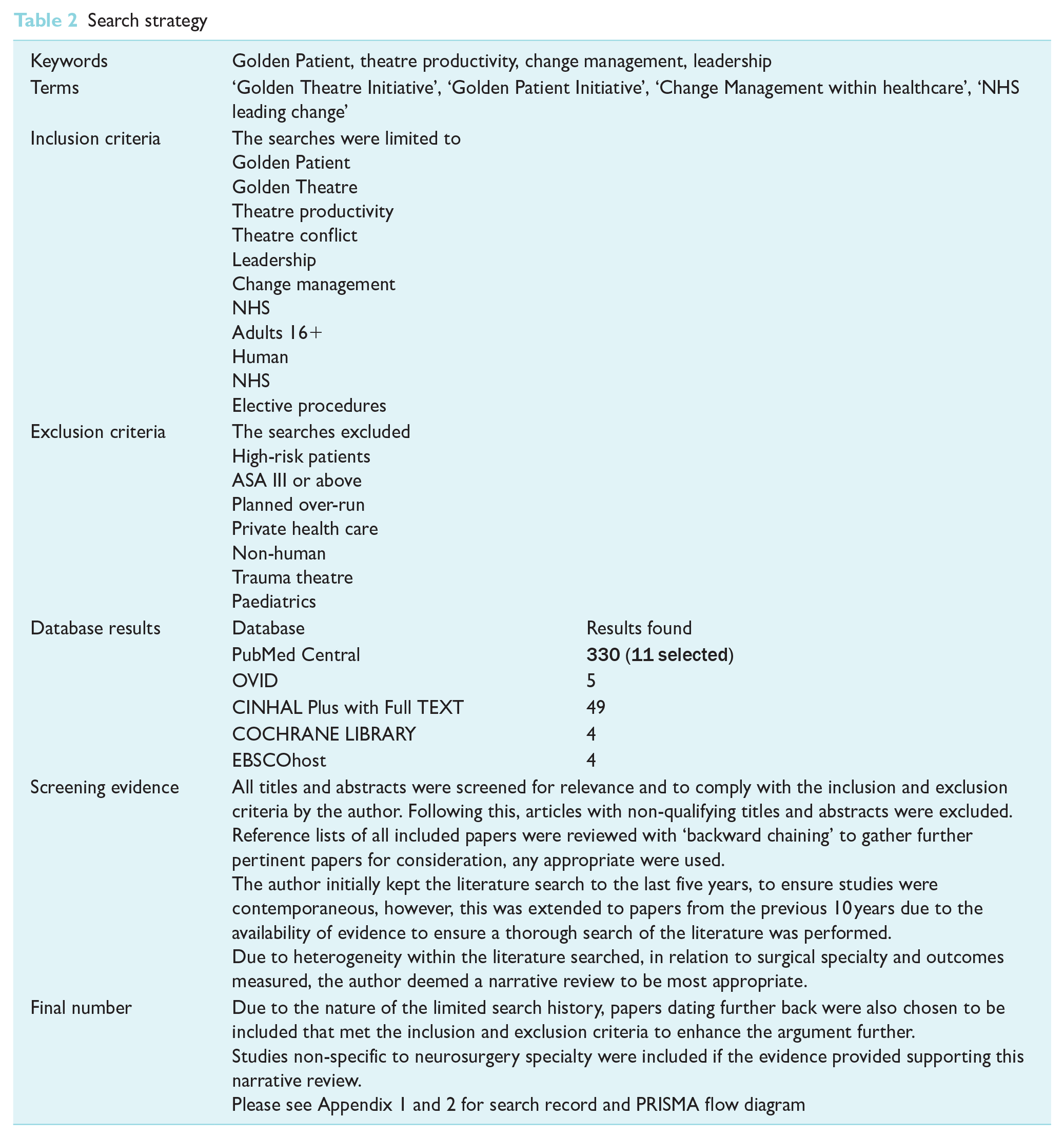
The primary aim of this article is to highlight the requirement of a large-scale initiative to address the current backlog of elective surgery within the NHS. Following a review of pertinent literature, a proposal for implementation of the initiative will be put forward. Tables 1 and 2 show literature search and search strategy.
Literature search and search strategy
Inclusion and exclusion criteria for literature search
Search strategy
Literature review
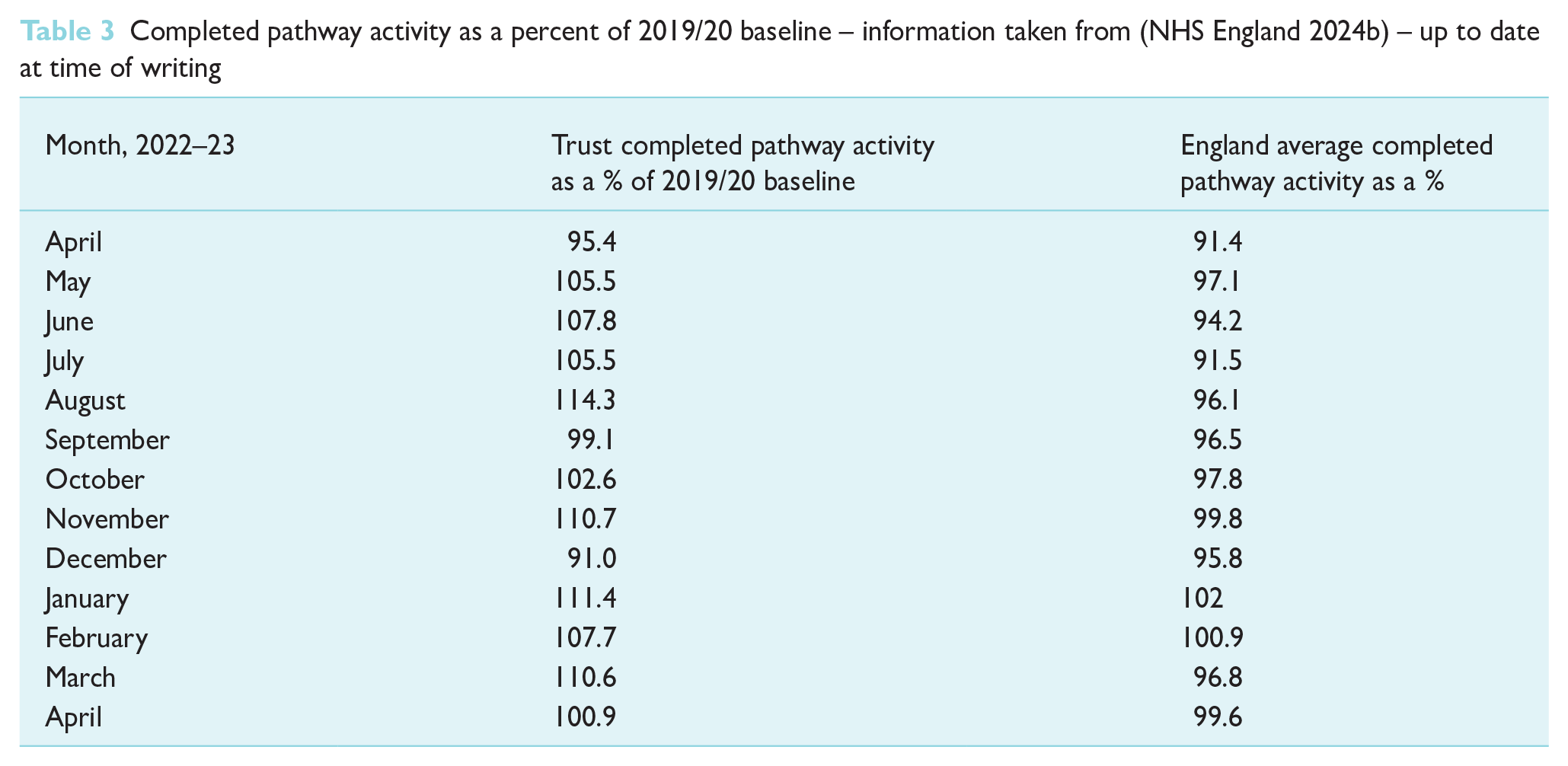
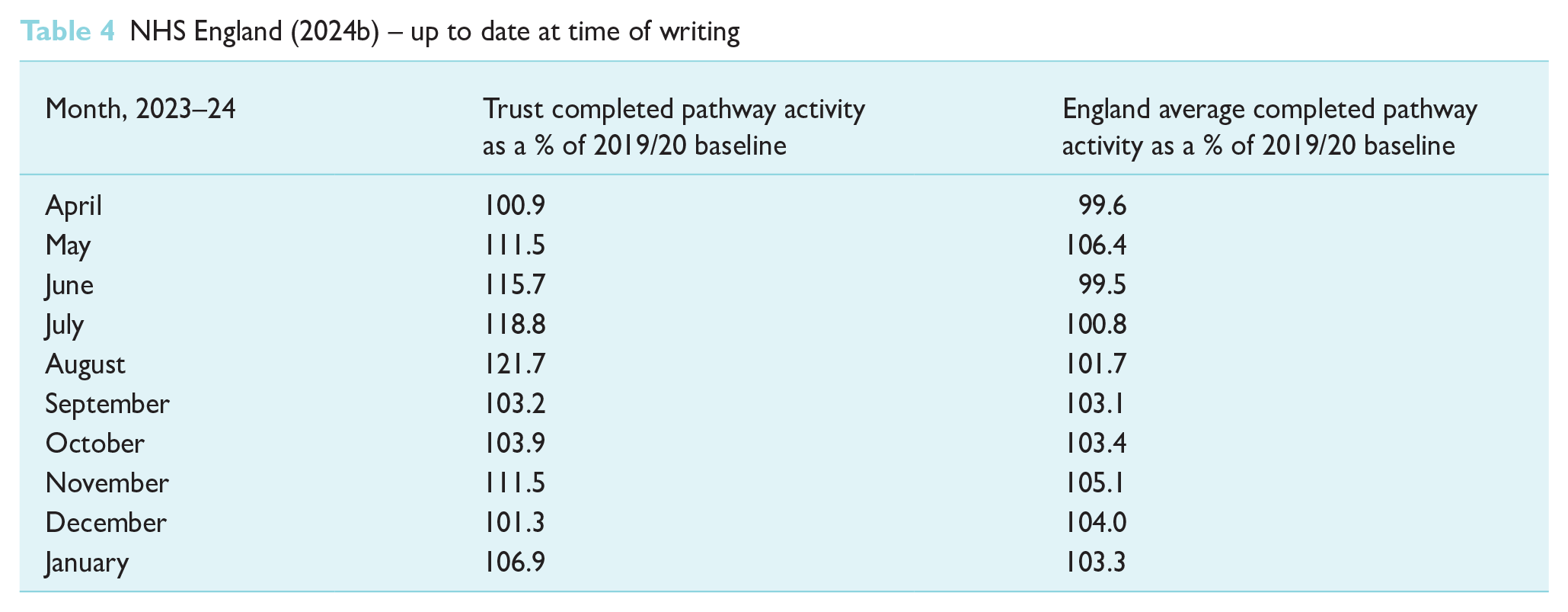
Following an examination of the recovery of elective activity by NHS England (2024b), it is apparent elective surgery is gradually increasing in the aftermath of the COVID-19 pandemic. Elective activity recovery as a percentage of the 2019/20 baseline is illustrated in Table 3. The aim set out by NHS England (2024b) was to recover elective activity to 110% of the baseline in previous years over the course of 2022 and 2023. Table 3 demonstrates the gradual increase of elective activity over the previous 12 months, however, it also highlights the length of time it has taken to reach over 100% of elective activity. Column 2 highlights the individual trust the author works within, as a comparison to the average of England as whole in column 3. Table 4 demonstrates that the England average has yet to reach the desired 110% of baseline activity; four years on from the pandemic; and, at the time of writing, there are still many trusts that have not achieved activity to 100% of the average from 2019/20; demonstrating the pertinent requirement for positive changes to be made to enhance this recovery of elective services.
Completed pathway activity as a percent of 2019/20 baseline – information taken from (NHS England 2024b) – up to date at time of writing
NHS England (2024b) – up to date at time of writing
A blueprint set out by NHS England in 2022 hoped to address backlogs built up during the COVID-19 pandemic; known as the elective care recovery plan (NHS England 2024c). Delivering more procedures and scans in each of the three years following this, to achieve nine million more by 2025 was one of the primary aims. As part of this blueprint, new surgical hubs will be added with a view that patients, by March 2025, will not have to wait more than a year for surgery. This, however, can only be achieved through appropriate and continuous management of current elective and emergency operating lists. NHS England (2024a) further designed a national programme aimed at improving patient care and treatment while reducing unwarranted variations across patient care. Methods exist to track implementation of recommendations and outcomes on the delivery of care, ensuring change is being driven in the most appropriate and evidence-based manner. Through collaborative working and partnerships with local trusts, the gathering of these data reduces variations in clinical treatment of patients also.
A review into elective orthopaedic surgery was undertaken to address the variations observed (NHS England 2024b). At a 12-month point, over £30 m savings were witnessed, primarily through changes reducing the average length of stay of patients. As a result of this, a similar model has been implemented across 40 different specialities (NHS England 2024c). Changes to reduce the hospital stay can only occur if changes at earlier points in the patient journey facilitate effective and efficient delivery of care. The author strongly feels that, with the introduction of a golden theatre initiative to reduce unnecessary delays within the perioperative environment, patient care can be enhanced even further.
Leadership
Leadership is a process by which a leader influences an individual, or group, to achieve a common goal (Cummings et al 2021, Curtis & Cullen 2017, Gauly et al 2023). Leaders should create a shared purpose and vision, with common values among a diverse workforce, understanding how different teams within an organisation interact and connect (Curtis & Cullen 2017). Lynas (2015) focussed on the impact the Francis Report has had on leadership, identifying meagre leadership as an immediate risk to patient safety (Mid Staffordshire NHS Foundation Trust Public Enquiry 2013). Poor-quality leadership was highlighted and demonstrated the historical hierarchy of a top-down performance driven culture within health care had failed to promote a motivational way of working. Harrison et al (2021) stipulate good leadership is essential to patient centred care and leaders must guide, motivate, and set standards, while simultaneously delegate power and authority. Inter-personal relationships are fundamental to excellent leadership within health care and, as such, a respectable leader can greatly influence the care and compassion provided by an organisation (Cummings et al 2021).
The sentinel work of Bass & Steidlmeir (1999) suggested that an effective transformational leader should set examples, which are then mirrored by others, to permit motivation and growth among teams due to a genuine commitment, and without coercion. Effective and inspirational leadership can be demonstrated through personal values and individual characteristics, motivating and developing individuals via a transformational style of leadership (Atkins et al 2023). Appropriate engagement and empowerment of staff is necessary; removing any barriers that may impede open and honest communication, to ensure motivated and invested staff (Atkins et al 2023, Fisher 2017).
Empowering staff to ensure they feel recognised and appreciated, in addition to caring for their psychological needs is paramount for a good leader (Cummings et al 2021, Giddens 2018). The wellbeing of NHS staff is fundamental to the provision of patient care; therefore, leaders must enable individuals to provide care and compassion in an unpredictable and rapid changing health care environment through reducing the unnecessary impact of stress on the workforce (Alban-Metcalfe & Alimo-Metcalfe 2018, Fisher 2017, Robins & Davidhizar 2020) encourages all good leaders to have a secure and trusting relationship with their team, to inspire and motivate. Encouraging staff to share the same vision results in more committed, invested and motivated workforce (Atkins et al 2023, Giddens 2018).
Appropriate leadership styles can play a pivotal role in health care, enhancing and transforming the care provided to patients; while simultaneously positively affecting staff mentality (Cummings et al 2021). Rossum et al (2016) suggest that a hierarchical structure is expected to impede successful change and foster that the coherence and ability of a team to work effectively, requires open, clear and structured communication, with visible leadership. The author believes that this can be clinician dependent, and some areas of health care experience significant conflict due to the hierarchical, autocratic leadership styles. To change current practice and create a ‘Golden Theatre Initiative’ in elective settings, leadership must be enhanced to diminish a negative cultural network within the perioperative environment and reduce the hierarchical leadership styles.
More recently, a study by Atkins et al (2023) addresses issues surrounding leadership within the surgical setting, affirming high-quality patient care is only achieved through collaborative team leadership. Gauly et al (2023) further this notion, stating that leadership development used in surgical settings should be a shared process across a group of individuals with a collective goal. Leadership of this sort encourages individual opinions and recognises the contribution these can make to the overall outcome. Individual leaders must also focus on their strengths and weaknesses, in addition to leadership style, as these factors can greatly influence the success of a change process; feeling equally valued and with a sense of engagement will encourage staff to drive a change forward (Atkins et al 2023).
Change management
Although change management is a recognised core requirement of health care managers and leaders, efforts to alter practice and introduce new methods of working often fail (Harrison et al 2021). Harrison et al (2021) reason that the multiple variables within health care can be unpredictable and uncertain, and this must be acknowledged when trying to introduce any change process. Individuals have variable learning experiences, attitudes and beliefs; all of which need to be considered to facilitate progression and change. Change, within any institution, is a multifaceted process requiring leadership to direct, guide, transform and fulfil goals set (Rossum et al 2016). Planned change within health care is fundamental to continually improve service provision, however, can be difficult to implement. Unstructured approaches to change often fail; therefore, it is imperative to identify a framework to work within, ensuring change is implemented, managed and evaluated successfully (NHS England 2024a).
A specific need for change is necessary prior to developing shared visions and beliefs; by holding a team responsible for the implementation of change, they may be able to provide greater insight into where the change is required; assuming a bottom-up approach to change management (Rossum et al 2016). Through the systematic review conducted by Harrison et al (2021), it was deemed Kotter’s eight-step model was preferred, with Lewin’s three-stage model also commonly employed. The study highlighted that the models do provide a framework to support and sustain change, and with clinician involvement, change projects were more successful. Lewin’s three-stage model of change has been implemented historically, with success; however, can be argued to be outdated, and not applicable to big organisational change, such as those that occur in health care (Campbell 2020, Mitchell 2013).
Campbell (2020) discusses John Kotter and William Bridges as two leading individuals in the field of change theory and how their theories can be utilised. Once a change process has been successfully implemented, it needs to be anchored in place to instil normal practice (Kotter 2014). Organisations wish to reduce costs, improve quality and increase productivity through change; however, leaders can often underestimate the difficulty of driving people out of their comfort zones; therefore, establishing a sense of urgency to change can reduce any potential complacency (Kotter 2014). Human factors in relation to skill mix, culture and psychological safety within the environment should be considered and teams selected according to comparable attitudes and common goals; as a more effective team-working mind set can have greater results for change and therefore delivery of patient care (NHS England 2024c).
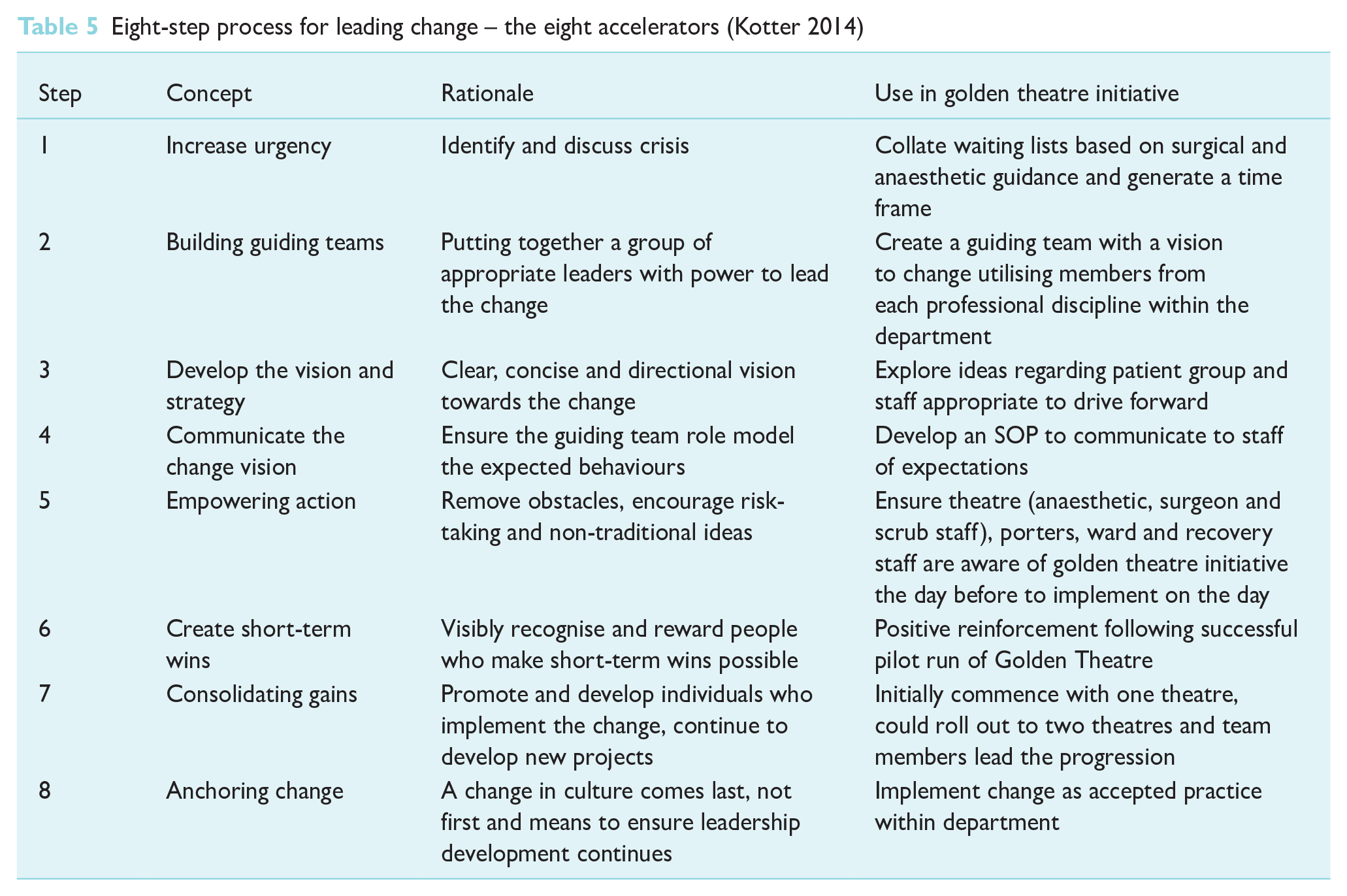
The eight-step model as designed by Kotter (2014) incorporates change and focuses on three main stages: creating a climate for change, engaging and enabling the workforce, and finally, implementing and sustaining the change. Kotter (2014) centres on the concept that emotional consideration must be given to employees, as these can impede the success of alteration; negative feelings must be transformed into positive ones that can promote change. It is also emphasised that when behaviour change is fuelled by emotion, it is more likely to be longer lasting then when analysis is the primary focus. Kotter (2014) stresses that this framework is not a step-by-step approach and encourages that one step may be used to achieve another; Table 5 demonstrates the eight steps and identifies the concepts within each.
Eight-step process for leading change – the eight accelerators (Kotter 2014)
In comparison to the above, Bridges (2017) focuses on change as an individual notion; stating that within health care, each member of staff is required to transition to new ideologies of change. Bridges theory of transitional management stipulates responsibility sits with the manager, ensuring these transitions are supported, otherwise the change will be likely to fail (Bridges 2017, Campbell 2020). Three independent stages exist: endings, the neutral zone and beginnings. The neutral zone comprises unfamiliar territory during the transitional period where individuals let go of old ways and learn to develop new ways of working. In the final stage of this model, new beginnings, individuals should feel committed to the new change. Resistance occurs as people experience loss for the previous way of working, however, with direct communication of their role to play in the change process, focus and compliance can be ensured, allowing individuals to feel part of a team and willing to anchor the change in place (Bridges 2017, Campbell 2020, Kotter 2014).
Although the theory by Bridges (2017) has potential to be applicable to the health care environment, and the author believes that it would be most useful for smaller changes; Kotter’s theory is far more relatable to larger organisational changes due to the extensive nature of the framework. The focus must be on the long-term goals and sustainable change process before any initiative is put forward. Fundamentally, leadership can either encourage or inhibit a successful change, demonstrating an argument for focussed, motivational leaders and demonstrating the requirement for whole team involvement throughout the process, to reduce any potential failure of the change (Rossum et al 2016).
If a vision is complex, failure to create adequate short-term wins and incentives can risk a loss of momentum; these can take the form of recognition, promotion or financial enticements (Kotter 2014). The study by Halim et al (2018) demonstrated the use of financial incentives to encourage the prompt start to operating theatre lists; however, the study highlighted this was only offered to anaesthetists. Khan et al (2022) affirm a similar use of tangible gains; with strategies deployed to attempt to encourage staff to work through these lengthy lists; including financial, introduction of new protocols, education and improvements in team motivation. These have demonstrated some results, however, change needs to happen at a faster rate to reduce the current issue more effectively. The author believes that these strategies could cause some conflict among operating theatre colleagues if treatment is not equivalent across the board. If used appropriately, and fairly, these methods could improve productivity and increase staff morale, resulting in a higher level of coordinated working; although in the current financial climate, the author does not believe that this approach would be viable and perhaps incentives relating to earlier finish times or time in lieu would yield the same effects upon staff.
An effective leader must understand, plan, implement and communicate any aspect of change; failure to do so may result in unsuccessful change and work force dissatisfaction. While the literature examined focuses on transformational leadership as fundamental and preferential in health care; the author believes that individual characteristics can also influence a good leader. Holistic approaches to change management are required; ensuring staff engagement, appropriate communication and, ultimately, an ability to adjust leadership traits as necessary. Following an evaluation of the literature surrounding change management and the theories, the author believes that an approach utilising the eight steps as suggested by Kotter would be best for larger changes; however, the author proposes that the theory of transition from old to new practice should also be strongly considered by managers to focus on over all staff wellbeing.
Golden theatre initiative and proposed change
Bridges (2017) examined how the introduction of a GPI following a review of delayed starting times could improve practice. Data collection for this study commenced six months after its introduction to allow a settling in period and adjustment for all staff involved in the change. This is aligned to the theory suggested by Bridges (2017) stating the transition of old ways to the new way of working must be supported by managers to ensure the change is successful. In the six months following the start of this study, patient cancellations were n = 49, the six months preceding the study n = 99; thus, demonstrating a significant impact on the identification of a GP, theatre efficiency and reduction in cancellations following the change.
Matthews et al (2015) conducted an operating room-focussed improvement project aimed at increasing the first case on time starts. The entire perioperative team was involved, which demonstrates a multidisciplinary approach to change, as recommended by Kotter (2014). Neurosurgical theatres were the focus of this project, identifying that any delay in starting the first case to have a cumulative effect on subsequent cases for the day. Prior to the improvement project, first case prompt start times were 33%. Following the engagement of the whole team for a shared goal to improved start times and the employment of a new service manager; the first performance analysis demonstrated an increase of 44% cases starting on time. At the second performance analysis, the rate of on-time starts was 68%, and significant predictors of delayed starts were identified to anchor the change in place and ensure success.
A further study by Tulloch et al (2020), focussed on reducing neurosurgical theatre start time delays. An observational retrospective service evaluation was conducted and acknowledged that 91.7% of cases (45 of 49) over a 12-week period were delayed, with 66% experiencing a delay greater than 60 minutes. Following implementation of the GPI, a delay of 66.7% was noted, and only 4% of cases were delayed beyond 60 minutes. This study demonstrates that the GPI had a positive effect on the start time of a theatre, and identified the main factors of delay, unavailability of surgeon and anaesthetist and the absence of senior clinician supervision.
Key et al (2019) performed a study focussing on the late start times of orthopaedic trauma lists, affecting total operating capacity. This study found the delay to commence a list was as a direct result of the patients not being suitably managed prior to their transfer to theatre. Patients were frequently deemed to be medically unfit at the point of sending for, causing avoidable delays and inefficiencies. Results over a timeframe demonstrated that mean procedure start time within the first month following implementation of GPI was 19 minutes, increasing to 26 minutes in the second month; demonstrating a positive implementation of this initiative. Key et al (2019) also affirm that the current perception of theatre efficiency is in line with the management of elective lists. However, in the case of this study, in addition to worldwide, the nature of a trauma list is significantly different, and can vary from moment to moment. Elective and emergency operating lists are two separate entities and should therefore be treated as such. Reducing elective waiting lists and ensuring patients receive treatment in a manageable timescale is an enormous focus from the NHS in their Getting it Right First-Time initiative (NHS England 2024c).
More recently, the systematic review of the implementation of the GPI by Khan et al (2022) sustains the argument that GPI when implemented does demonstrate favourable results and enhance efficiency. Organisational input is suggested to further implement this initiative and manage staff morale accordingly. Results of more recent studies demonstrate the delays experienced within the perioperative setting are not novel and have existed prior to the COVID-19 pandemic. NHS England (2024c) stipulates that an effective theatre flow relies upon patient and theatre preparation. Each aspect of the theatre pathway directly contributes to the overall aim of achieving staff and patient satisfaction, in addition to timely delivery of treatment. Therefore, any delay can have adverse effects on both patient and staff satisfaction.
The current delivery of elective care requires reimagining, to attempt to tackle the present demands on the service (Wall et al 2022). Evidence within the literature suggests that the GPI has been effectively rolled out across multiple disciplines, with success. The suggestion to extend this initiative to a whole theatre approach would tackle the same issues, but at an increased rate on an individual institutional level. In the proposed initiative, procedures should be precoded into major and minor, based on complexity, risks, and surgical time. Following this, only minor procedures with a low relative risk of having to convert into a major procedure, should be listed for the Golden Theatre. This proposed way of managing an elective list should insist upon a designated start time that all staff are aware of and comprehend the expectations of keeping to these timelines to ensure efficiency and appropriate theatre utilisation (NHS England 2021, 2024c).
Conclusion
Although operating theatre start times have a profound impact on the overall theatre efficiency, the author believes that there are several other areas that require addressing simultaneously; surgeon compliance to be present on time, theatre turnaround time and wards ensuring patients are ready for theatre promptly. The current literature available demonstrates a broad spectrum of specialities and highlights that each speciality has variable patient demographics. Therefore, what may work to enhance and improve surgical start times for one speciality, may very well cause further delays for another; there is no ‘one-size-fits-all’ approach. As such, under this initiative, individual trusts would work to determine their lowest risk of elective procedures and develop a ‘Golden Theatre’ list accordingly. The change would involve a specific theatre utilised each day to optimise patient throughput, with dedicated consultant surgeon, anaesthetist and appropriate skill set of staff. This would require the patients to be admitted the night before, medically optimised, consented and prepared fully for theatre.
While delays associated with the perioperative assessment and preparation of a patient are outside of the suggestions within this article, these also require streamlining. The ideas put forward within this article are specific to reducing cancellations on the day of surgery, enhancing operating theatres to be more efficient, and ensuring patients receive care in a timely manner. To further the ideas set out by this article, a pilot trial of a ‘Golden Theatre’ in an elective care setting would provide suitable evidence for the feasibility to commence a quality improvement project on a wider scale. Ultimately, the introduction of a golden theatre initiative is a low cost, simple method with the potential to reduce delays and allow surgical departments to tackle lengthy waiting lists.
Key points
Literature review presenting a balanced critical examination of how leadership during a change process can be utilised to implement a new perioperative initiative.
Delays to elective operating lists are multifactorial and long standing; however, simple changes can have a positive, overall effect on delays and proficiency.
Physical and psychological impacts of late elective cancellations can result in patient distress and lack of trust in NHSs.
Following a synthesis of the literature, recommendations for change in practice are made, suggesting a move to enhance sustainability and improve patient outcomes.
Footnotes
Appendix
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.