
Abstract
Background:
Ineffective collaboration can increase adverse events in the operating theatre. When professionals work collaboratively, they are more likely to improve patient safety and outcomes.
Aim:
To identify interprofessional collaboration interventions involving operating theatre teams and describe their effect on facilitating communication, teamwork, and safety.
Methods:
A scoping review of four databases. Results were analysed by identifying interventions and mapping their related outcomes.
Results:
Twenty studies evaluated single or multi-faceted interventions. Despite low-quality study designs (no randomised controlled trials), four interventions (eg: briefings, checklists, team training, debriefing) improved communication and teamwork, and enhanced safety outcomes. Only one study, using team training, reported that organisational level interventions (eg: Standard Operating Procedures, Lean quality improvement management system) improved teamwork and safety outcomes.
Conclusion:
Several studies reported interventions enhanced interprofessional collaboration within operating theatre teams. Although findings were in favour of improved communication and teamwork, more rigorous research is required.
Introduction and literature review
Ineffective interprofessional collaboration can have adverse effects on health care especially in the operating theatre (Mazzocco et al 2009, Muller et al 2018, Schwendimann et al 2018, Zegers et al 2011). A large proportion of surgical adverse events are preventable, and their consequences are more severe compared to other types of adverse events in health care (Schwendimann et al 2018, Zegers et al 2011). Interprofessional collaboration (IPC) in the operating theatre (eg: communication, teamwork) improves respect among health care professionals and can lead to improved patient safety and outcomes (Muller et al 2018, Wauben et al 2011, WHO 2010).
IPC happens when multiple health care workers of different professions provide comprehensive services to patients, their families, and communities (WHO 2010). The Interprofessional Education for Collaborative Patient-centred Practice (IECPCP) framework is a structural model to facilitate and support the implementation of an approach to IECPCP across health care sectors (D’Amour et al 2008, D’Amour & Oandasan 2005). The IECPCP has 3 levels (micro, meso, and macro) with four interrelated core dimensions (internalisation, shared goals and vision, governance, and formalisation). IPC interventions can enhance IPC education and practice (Reeves et al 2011, 2018, WHO 2010, 2021).
An IPC intervention targets members of more than one health and/or social care profession with the explicit purpose of improving IPC (Zwarenstein et al 2009). A Cochrane systematic review of practice-based IPC interventions within health care conducted in five countries identified nine individual and cluster-randomised controlled trials evaluating four types of practice-based IPC interventions: (a) externally facilitated interprofessional activities, (b) interprofessional rounds, (c) interprofessional meetings, and (d) interprofessional checklists (Reeves et al 2017). Of nine studies, one conducted in the operating theatre evaluated a checklist based on a literature review of surgical practices and consensus of two surgeons, (Calland et al 2011). Findings showed no improvement on patient safety and little improvement on IPC (eg: situational awareness did not significantly differ) within the operating theatre teams (Calland et al 2011). More recent research reports that IPC can promote improved patient safety and outcomes, quality of work and work environment in the operating theatre (Holmes et al 2020). However, operating theatre nurses are known to rate IPC lower compared to other health care professionals within the IP team (Bowles et al 2016, Makary et al 2006, Muller et al 2018). Given this previous synthesis was limited to randomised controlled trials, and there is variability in findings based on the discipline reporting outcomes, there is little synthesised evidence on the use of interventions to improve IPC in the operating theatre.
The aim of this scoping review was to identify IPC interventions involving operating theatre interprofessional teams and describe their effect on facilitating communication within the IP team, teamwork, and safety outcomes.
Methods
Study design
A scoping review was guided by the Arksey and O’Malley (2005) framework. The five steps were (a) identifying research questions, (b) identifying relevant studies, (c) selecting relevant studies, (d) data charting, and (e) collating, summarising, and reporting of study results.
Identifying research questions
The research questions were: (a) What types of interventions are used to improve IPC in the operating theatre? (b) What IPC interventions are more likely to be adhered to by operating theatre health care professionals? and (c) What is the reported effect of IPC interventions in the operating theatre on communication, teamwork, and safety outcomes?
Selecting relevant studies
SPIDER (Sample, Phenomenon of Interest, Design, Evaluation, Research type) (Cooke et al 2012) (Table 1) was used to determine study eligibility. Given the extent of the literature, the focus of this study was on eligible quantitative studies that evaluated interventions to facilitate IPC within the operating theatre with teams that included nurses, surgeons, and anaesthetists.
Inclusion and exclusion for criteria for search strategy tool SPIDER
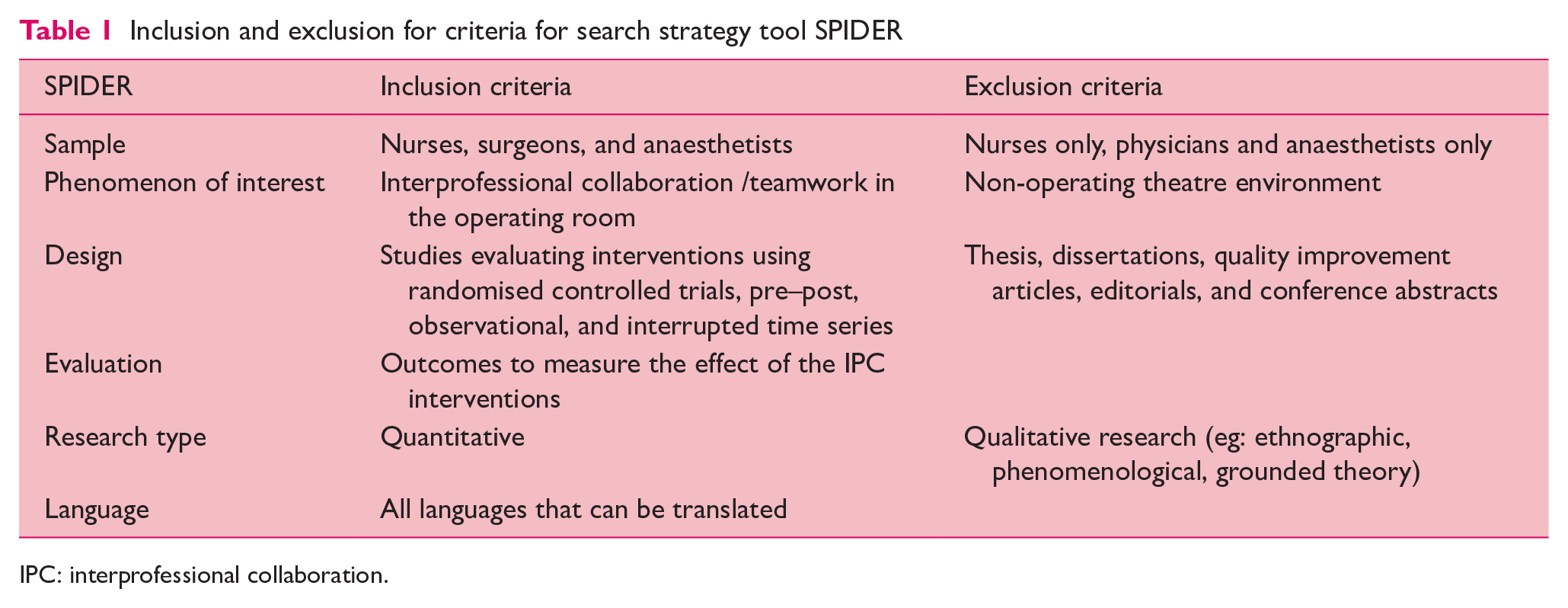
IPC: interprofessional collaboration.
Information sources
Medline (via OVID), CINAHL (via EBSCOHost), PsycINFO (via OVID), and Embase (via OVID) were searched between 1 January 2005 to 6 November 2020. The start date of 2005 reflects the publication date for the IECPCP framework.
Search strategy
With the assistance of research librarian (LS), the research team designed the search strategy. Subject headings and keywords included: Interprofessional, Interprofessional relations, Interdisciplinary, Multidisciplinary, Collaboration, Teamwork, Operating room, Nursing. The searches were performed by MJL and validated by LS (Appendix A).
Selecting relevant studies
The search findings were uploaded into Covidence (2020). Title and abstract screening were conducted by two independent authors (MJL, NM). Titles and abstracts were excluded only if both reviewers agreed. Studies that appeared to meet the inclusion criteria were retrieved in full and assessed independently by two reviewers (MJL, NM, DS). Disagreements were resolved through discussion and consensus.
Data charting
Three authors independently pilot tested the data extraction sheet (DS, MJL, NM) with two studies and extracted data compared to ensure consistency. Guided by the Arksey and O’Malley (2005) framework, data extraction included (a) study characteristics, (b) intervention characteristics, (c) instruments, and (d) outcomes (eg: communication, teamwork, safety).
Collating, summarising, and reporting of study results
Extracted data were mapped against the research questions (Arksey & O’Malley 2005). The research team analysed findings to respond to the research questions with results summarised in tables and described narratively. Results are reported using the PRISMA-ScR checklist (Tricco et al 2018).
Results
Of 1840 citations after removing duplicates, 20 studies were eligible to be included. Reasons for excluded full text were documented. See the PRISMA flow diagram (Figure 1) for details (Tricco et al 2018).
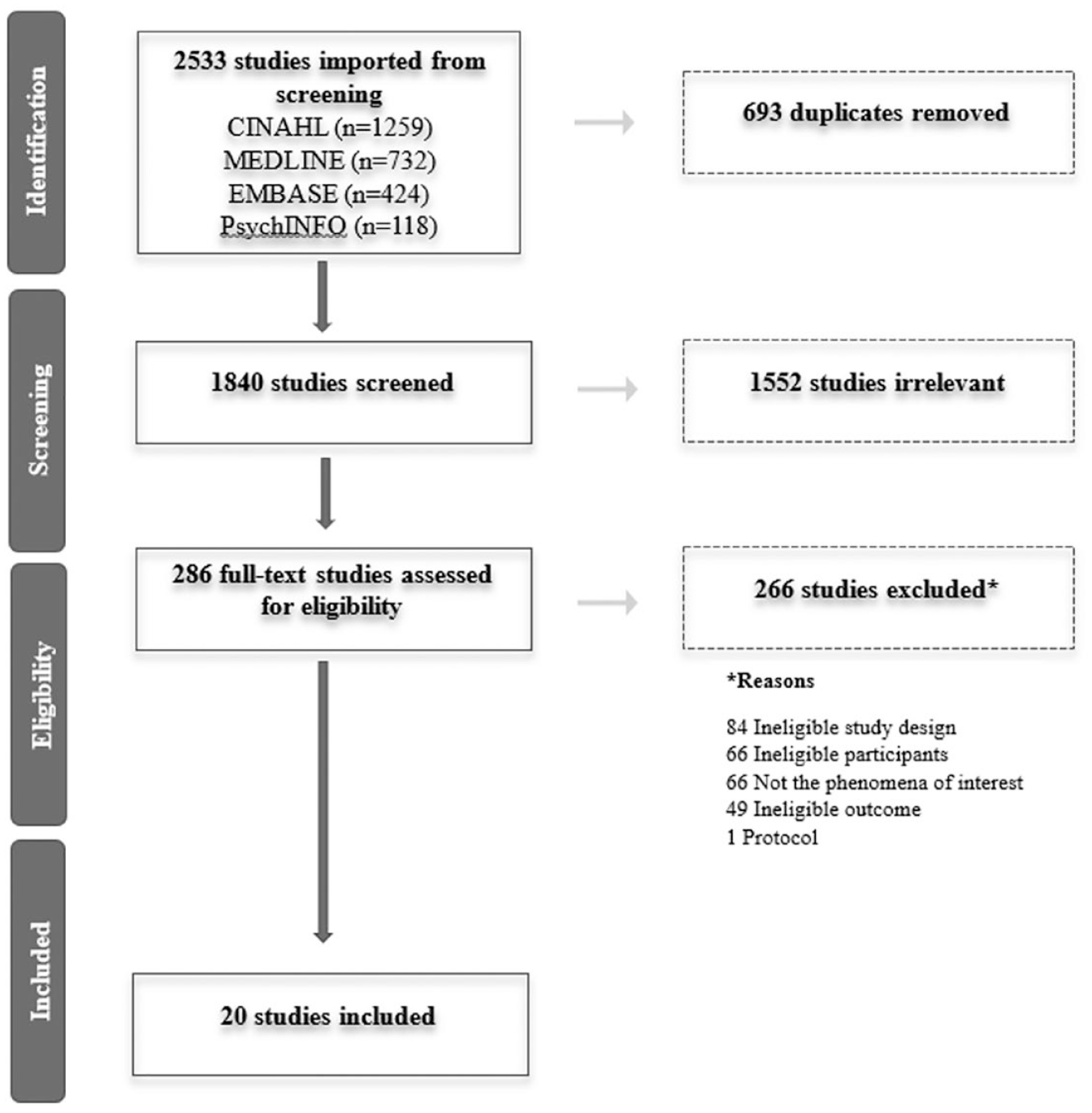
Selection of sources of evidence PRISMA flow diagram
Characteristics of sources of evidence
Studies, conducted in eight countries; United States (n = 10), United Kingdom (n = 4), Brazil (n = 1), Canada (n = 1), France (n = 1), Finland (n = 1), Israel (n = 1), and New Zealand (n = 1) (Table 2), were mostly in academic hospitals (75%; n = 15). Studies were (a) non-randomised intervention with controlled group or interrupted time series (10%; n = 2) (McCulloch et al 2017, Morgan et al 2015), (b) pre–post using observations or survey (55%; n = 11), and (c) mixed method using observation and survey (35%; n = 7). Studies’ participants were members of the operating theatre team including: (a) surgeons and often residents, (b) anaesthetists and often residents, and (c) nurses (90%; n = 18). The other two studies did not describe the team members (Cabral et al 2016, Hinde et al 2016). The median number of participants who responded to surveys was 129.5 (range = 32–929) and median of 86 observations of surgical cases (range = 34–37,133) (see Table 2).
Characteristics of included studies
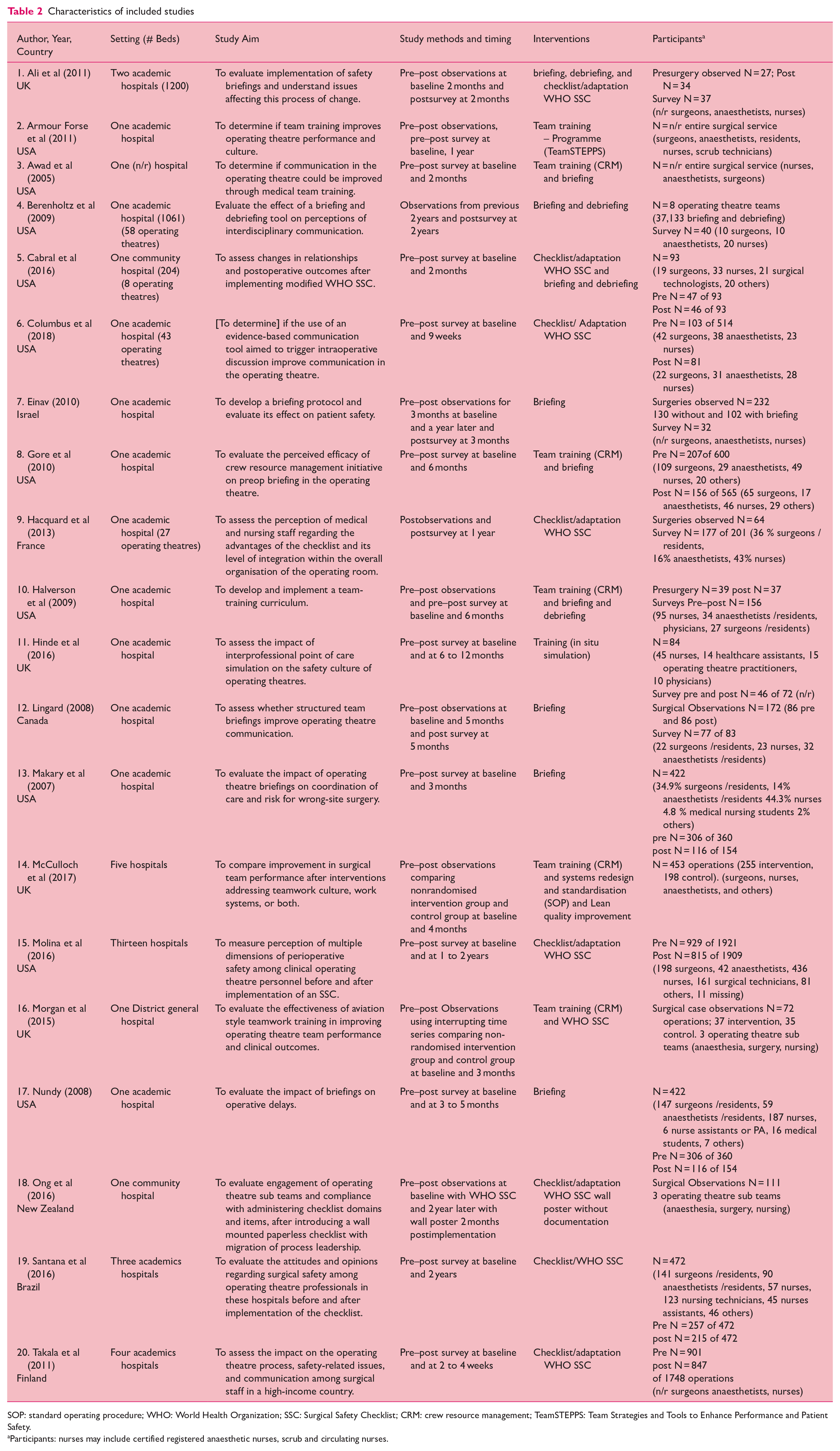
SOP: standard operating procedure; WHO: World Health Organization; SSC: Surgical Safety Checklist; CRM: crew resource management; TeamSTEPPS: Team Strategies and Tools to Enhance Performance and Patient Safety.
Participants: nurses may include certified registered anaesthetic nurses, scrub and circulating nurses.
Characteristics of interventions to improve IPC in the operating theatre and their use
Four IPC interventions evaluated were (a) briefings (50%; n = 10 studies), (b) checklists (45%; n = 9), (c) team training (35%; n = 7), and (d) debriefings (20%; n = 4). Studies evaluated an individual intervention (50%, n = 10) or a multi-faceted intervention (50%, n = 10) (Table 3).
Outcomes for IPC interventions
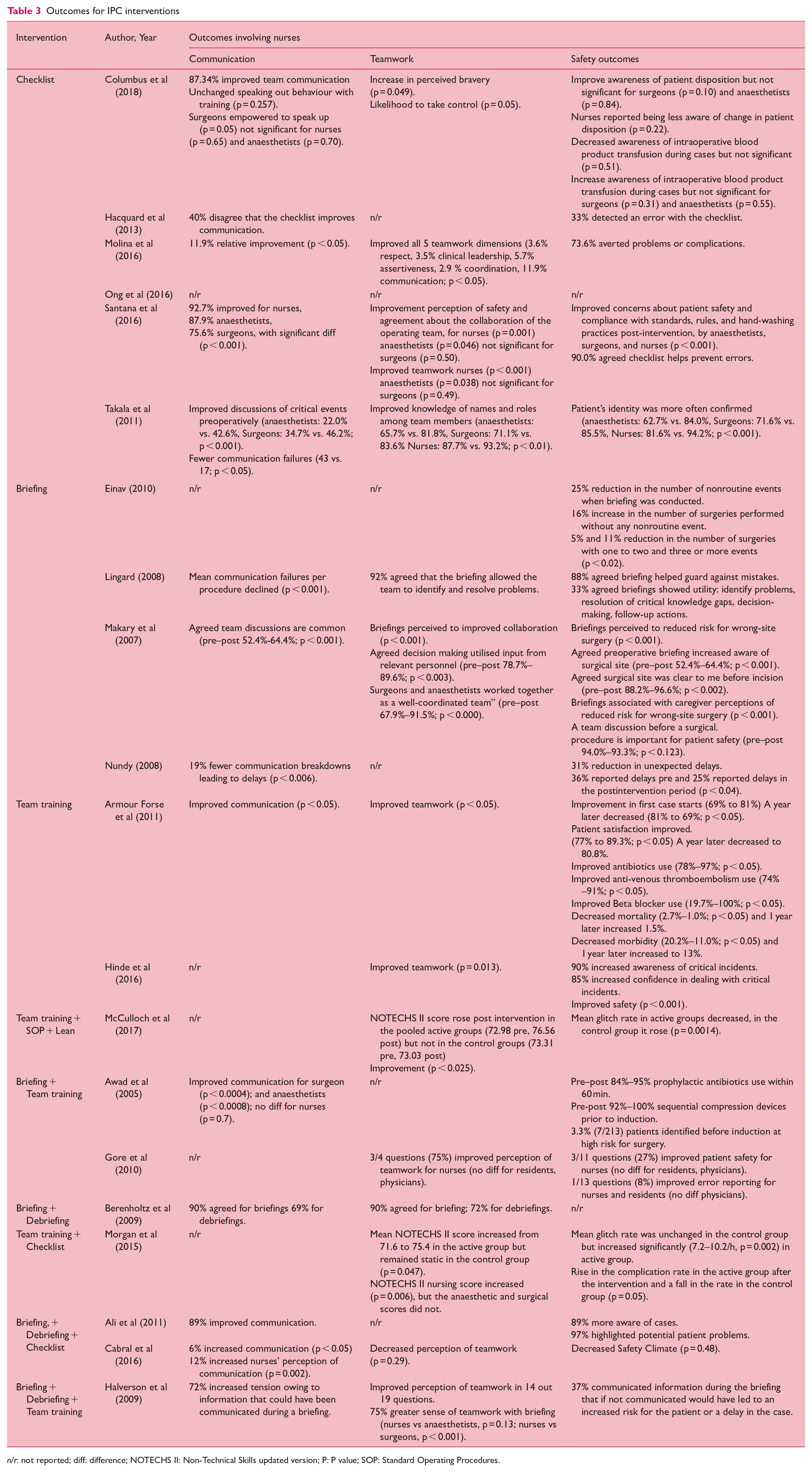
n/r: not reported; diff: difference; NOTECHS II: Non-Technical Skills updated version; P: P value; SOP: Standard Operating Procedures.
Briefings
Ten studies evaluated a briefing intervention (Table 3). A briefing refers to a communication practice among the surgical team members before the surgical procedure to help enhance knowledge, purposeful action, quality, and safety of collaborative care (eg: team briefing, perioperative briefing). Briefings were applied in various formats (eg: list of structured items or poster) with some documented and others verbal only.
Checklists
Nine studies evaluated the WHO Surgical Safety Checklist (SSC) or a version adapted for their setting (Table 3). The WHO SSC is a 19-item checklist where the entire team stops at three critical points: (a) pre-anaesthesia (Sign In), (b) pre-incision (Time Out), and (c) before patient leaves the operating theatre (Sign Out) to enhance communication between the surgical team members, improve outcomes, decrease complications, and improve patient safety (WHO 2009). The WHO SSC has a designated area of responsibility for each of the three operating theatre sub teams (eg: surgery, anaesthesia, nursing). Nurses frequently contributed to the initiation and systematic verification of the checklist, but the checklist is not always used completely (Hacquard et al 2013, Molina et al 2016). The SSC significantly improved Sign Out compliance and team engagement by all operating theatre sub teams (Ong et al 2016).
Team training
Seven studies used a variety of team training interventions (Table 3). Team training in health care refers to an educational programme provided to a group of health care professionals to build overall team performance by increasing their procedural knowledge, proficiency in their roles, and skills in functioning as part of a team. Of seven studies, five used the Crew Resource Management (CRM) approach (Awad et al 2005, Gore et al 2010, Halverson et al 2009, McCulloch et al 2017, Morgan et al 2015). This approach is based on the aviation-style CRM communication techniques and consists of a body of basic patient safety behaviours, including leadership, assertiveness with respect, and effective communication techniques (Awad et al 2005, Gore et al 2010). One study used CRM with systematic multi-organisational level team training approaches such as Standard Operating Procedures (SOP) and the Lean quality improvement management system (Lean) (McCulloch et al 2017). Another study used the TeamSTEPPS programme (Armour Forse et al 2011); a government sponsored programme composed of 12 modules that provides a rich resource-based, evidence-based approach for training groups of health professionals to improve institutional collaboration and communication relating to patient safety (Canadian Patient Safety Institute 2021). The final study used point of care (in situ) simulation on safety culture in the operating theatre (Hinde et al 2016). Most studies used team training as a multi-faceted intervention (Table 3). Team training was described as significantly improving compliance with briefings and debriefings (Halverson et al 2009).
Debriefings
Four studies specifically mentioned the use of debriefing as part of a multi-faceted intervention (Table 3). Debriefing refers to a structured communication among the surgical team members after the surgical procedure to review any concerns or deficits identified during the procedure. Some studies refer to debriefing as a ‘sign-out’ from a surgical safety checklist. A high percentage (70%) of the operating theatre team members agreed that the debriefing tool is feasible considering their workload (Berenholtz et al 2009).
Reported effects of IPC interventions on communication, teamwork, and safety outcomes
The IPC interventions are presented as a single or a multi-faceted intervention and in order of frequency (Table 3).
Single-interventions
Checklist intervention (n = 6 studies)
Five of six studies used an adapted version of the WHO SCC and one study using the original WHO SSC (Table 3). Four out of six studies that measured team communication reported improved team communication. Although one study reported improved team communication, the authors also reported that the checklist did not improve the ability to raise patient safety concerns (ie: ‘speaking out behaviour’) by the nurses and anaesthetists (Columbus et al 2018). All four studies that measured teamwork reported improvements as indicated by enhanced assertiveness, respect, clinical leadership, coordination, and collaboration (Columbus et al 2018, Molina et al 2016, Santana et al 2016, Takala et al 2011). Of the five studies that measured safety outcomes, four reported the checklist helped prevent errors and improved compliance with standards of practices (Hacquard et al 2013, Molina et al 2016, Santana et al 2016, Takala et al 2011) and one study showed no differences (Columbus et al 2018).
Briefing intervention (n = 4)
Three of four studies that measured communication reported significant improvements by reducing communication failures, increasing teamwork discussions, or reducing communication breakdown leading to delays (Table 3). For two studies, teamwork was significantly enhanced by improving the perception of collaboration, decision making used, or allowing the team to identify and resolve problems. Patient safety was improved in all four studies by either reducing non-routine events (eg: near misses), resolving critical knowledge gaps, helping prevent mistakes, augmenting surgical awareness, and reducing risk of wrong-site surgery.
Team training intervention (n = 3)
Of three studies, one measured and reported significant improvement in communication following the TeamSTEPPS programme (Table 3). All three studies showed improvements in teamwork and in safety outcomes. For example, the study using simulation training revealed statistically significant perceived improvements in both teamwork (p = 0.013) and safety climate scores (p < 0.001) and improved awareness of and confidence in dealing with critical incidents six and 12 months after implementation of interprofessional point of care simulation sessions (Hinde et al 2016). The study that used the TeamSTEPPS programme showed increased use in antibiotics, beta blockers, and venous thromboembolism treatment with a decrease in mortality and morbidity rates and persistency one year after implementation (Armour Forse et al 2011). The final study showed decreased mean glitch rate compared to increased mean glitch rate for controls (McCulloch et al 2017).
Multi-faceted intervention
Briefing and team training (n = 2)
Two studies employed briefing and CRM team training (Table 3). One study measured and reported improved communication for surgeons and anaesthetists, but no difference for nurses (Awad et al 2005). The other study measured and reported improved teamwork for nurses, but no difference for other team members (Gore et al 2010). Both studies reported overall improvement in patient safety with nurses increasing reporting of patient safety and errors (Gore et al 2010) and increased application of preventive measures during operating theatre procedures (eg: prophylactic antibiotics within 60 minutes and sequential compression devices prior to induction) (Awad et al 2005).
Briefing and debriefing (n = 1)
One study used briefing and debriefing interventions (Berenholtz et al 2009). Both briefing and debriefing were perceived to improve communication and teamwork, but the study did not measure safety outcomes.
Team training and checklist (n = 1)
One study used CRM team training and the WHO SSC (Morgan et al 2015). No communication or safety outcomes were measured. There was improved teamwork, such as situation awareness, decision making, leadership and cooperation. Concurrently, there was a rise in operative glitches such as interruptions, omissions and changes affecting outcomes of the procedure.
Briefing, checklist, and debriefing (n = 2)
Two studies used briefing, debriefing and the WHO SSC (Table 3). There was improved communication and perception of communication in both studies. One study reported no differences in teamwork and safety outcomes (Cabral et al 2016). The other study reported improved safety outcomes by increased awareness during cases and enlightenment of potential problems (Ali et al 2011).
Briefing, debriefing, and team training (n = 1)
One study applied briefing, debriefing, and CRM team training (Halverson et al 2009). The communication between team members was improved with the use of briefings by helping alleviate operating theatre team tensions. There was improved perception of teamwork and nurses reported better teamwork, more predominantly when briefings were used. Patient safety was improved by increased information exchanges, lessening the risks for patients and delay of care.
Discussion
This scoping review identified interventions for improving IPC in the operating theatre were briefings, checklists, team training, and debriefings. Most studies reported a significant improvement in communication, teamwork, and safety outcomes. Some of the studies reported that nurses indicated less improvements compared to surgeons, anaesthetists, and others on the operating theatre team, but these results were not significantly different (Awad et al 2005, Cabral et al 2016, Columbus et al 2018). Overall, the findings from this scoping review indicated favourable improvements in patient safety and outcomes. However, these results need to be considered within the context of weak study designs and the need for further rigorous mixed-methods studies (Reeves et al 2017). These findings lead to the following points of discussion.
There were different perceptions of positive outcomes among the various professions within the operating theatre team. For example, nurses rated communication and teamwork lower compared to surgeons and anaesthetists (Carney et al 2010). This is consistent with findings from previous research showing discrepancies between surgical team members concerning communication, teamwork, and situation awareness (Gillespie et al 2013, Wauben et al 2011). All team members should understand and be well informed about the surgical procedures and about patient-specific health issues such as allergies or comorbidities (Wauben et al 2011). A lack of consistent perceptions between surgical team members can translate into a lack of shared understanding, leading to increased adverse events (Haynes et al 2009, Sexton et al 2006).
Most studies reported outcomes immediately after exposure to the intervention. In fact, only six of the 20 studies measured outcomes one year and beyond (Armour Forse et al 2011, Berenholtz et al 2009, Hacquard et al 2013, Molina et al 2016, Ong et al 2016, Santana et al 2016) (Table 3). Although most studies were showing favourable improvements overall, one study showed that the improved communication and teamwork at one year was better than baseline, but not as strong as the earlier post intervention measurements (Armour Forse et al 2011). These findings reinforce the recommendation from the previous Cochrane systematic review, suggesting waiting a longer period of time (unspecified) after implementation of the intervention before evaluating outcomes (Reeves et al 2017).
The second most common intervention was the WHO SSC or an adapted version. The WHO SSC is used around the world and in Canada for enhancing organisational practices (Accreditation Canada 2020, Healthcare Excellence Canada 2021). The WHO SSC has shown significant reduction in morbidity and mortality (Haynes et al 2009). Interestingly, one study from Canada, reported mixed findings on the effectiveness of the WHO SSC, and found that the SSC was not associated with significant reductions in operative mortality or complications (Urbach et al 2014). Urbach et al (2014), question if the favourable effect indicates a Hawthorne Effect. This explication is consistent with findings of a recent Systemic Review of the Hawthorne Effect on surgical studies, showing that 63% of the 16 included studies used this effect to explain their improvements in results (Demetriou et al 2019).
The least used intervention was debriefing, and it was always used in combination with one or more other interventions (eg: checklist, briefing, team training). The interchangeability of terminology of ‘debriefing’ and ‘sign-out’ of the surgical safety checklist in the literature may add confusion on the concept of debriefing. Hence, it is difficult to know the added effect of debriefing. The term ‘debriefing’ should refer to the additional communication (beyond acknowledgement of the tasks performed) at the end of the surgical case addressing safety, equipment and efficiency that arose, and identify opportunity for improvement (Brindle et al 2018). Compared to briefing at the start of operating theatre procedures, debriefing was shown to have less impact on communication and teamwork (Berenholtz et al 2009). Debriefing was less well implemented or accepted by IPC teams, and could be attributable to logistical challenges (eg: competing priorities of subsequent surgeries) and perceived lack of value (eg: not related to direct patient care, not valued by the institution, issues during debriefings not subsequently addressed) (Bergs et al 2015). To ensure meaningful debriefing, an atmosphere dedicated to open communication needs to be fostered with the commitment of resources (institutional and personnel) and leadership engagement (Brindle et al 2018).
Most team training within the operating theatre setting used CRM and identified that its application required more than just the micro IP operating theatre team involvement. For example, one study reported that when synthesising team training approaches at various levels (micro: CRM in operating theatre; meso: Lean and SOP adoption by the organisation), the effectiveness of the interventions to enhance safety was improved (McCulloch et al 2017). All the interventions targeted mostly the interactional processes of the IECPCP Framework (D’Amour & Oandasan 2005). It is important to recognise that collaboration does not only exist within the operating theatre team, but also in the context of a larger organisational setting within all dimensions of IPC (sense of belonging, shared goals, structure of care and governance) (D’Amour & Oandasan 2005). Therefore, strategies to improve IPC should consider interventions targeting micro (eg: operating theatre team), meso (eg: hospital policies and processes), and macro (eg: government and professional guidance). Furthermore, the IPC interventions should target organisation factors and systemic determinants (eg: strong leadership, human resource management, policies and governance supporting IPC) (D’Amour & Oandasan 2005, Reeves et al 2017, San Martin-Rodriguez et al 2005, Toh et al 2017).
Limitations of the study
There are four key limitations that need to be considered. First, out of 20 included studies, 18 used weak study designs such as pre–post observations and/or survey evaluations. Second, there is potential for self-reported bias. To overcome the potential for self-response bias, several studies used observations to measure outcomes such as compliance, non-routine events, glitch rates, and communication and teamwork interactions. Third, assessment of methodological quality within this scoping review was not performed. This is common practice for scoping reviews unless there is a specific requirement due to the nature of the aim of the scoping review (Munn et al 2018). Fourth, there is a need to consider the potential impact of the Hawthorne effect also referred as the ‘observer effect,’ in which participants change their behaviour when being observed (Nguyen et al 2018). Eight out of ten studies described the Hawthorne effect as an explanation for the improvements in outcomes in surgical studies (Demetriou et al 2019).
Conclusions and suggestions for further research
In the operating theatre, four IPC interventions have been evaluated in studies to measure their effect on enhancing communication, teamwork, and safety outcomes. The findings of this scoping review have focused mainly on the interpersonal processes for implementation of briefings, checklists, team training and debriefings. The included studies had low-quality designs and their outcomes reported improved IPC in the operating theatre. Therefore, there is not sufficient evidence to draw clear conclusions on the effects of IPC interventions in the operating theatres and more rigorous research using high-quality study designs is needed. Interestingly organisational factors influencing IPC were not reported, and it would be beneficial to better understand how the factors within the meso and macro levels influence the micro level IPC and outcomes. Other studies highlight the need to further improve the effectiveness of IPC multi-faceted interventions targeting individuals (eg: nurses, surgeons, anaesthetists), and systems-level factors within health care delivery (D’Amour & Oandasan 2005, Etherington et al 2021, Reeves et al 2017).
Supplemental Material
sj-docx-1-ppj-10.1177_17504589221137978 – Supplemental material for Interventions to facilitate interprofessional collaboration in the operating theatre: A scoping review
Supplemental material, sj-docx-1-ppj-10.1177_17504589221137978 for Interventions to facilitate interprofessional collaboration in the operating theatre: A scoping review by Marie-Julie Levesque, Cole Etherington, Michelle Lalonde, Narges Moradi, Lindsey Sikora and Dawn Stacey in Journal of Perioperative Practice
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the University of Ottawa Research Chair in Knowledge Translation to Patients held by Dawn Stacey.
Provenance and Peer review:
Unsolicited contribution; Peer reviewed; Accepted for publication 23 October 2022.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.