
Abstract
Despite academic, policy and charity commissioned research giving considerable attention to the health of imprisoned women, significantly less research has considered the reproductive health and rights of this group. This shortfall is noteworthy since women who are imprisoned are often in very vulnerable positions, and so their ongoing healthcare in relation to gynaecology, obstetrics and sexual health and wellbeing, as well as access to such rights, should be a priority. These issues are exacerbated for the high number of women who are repeatedly imprisoned for short sentences. Presenting findings of a rapid evidence assessment, this article highlights the lack of attention to this aspect of imprisoned women’s health and rights, using the limited information available. The article argues that suitable reproductive healthcare needs to be seen as an essential aspect of women’s rights. Furthermore, the current nature of imprisonment in England and Wales results in multiple and frequent rights violations.
Despite academic, policy and charity commissioned research giving considerable attention to the health of imprisoned women, significantly less research has considered the reproductive health and rights of this group. This shortfall is noteworthy since women who are imprisoned are often in very vulnerable positions (Bartlett and Hollins, 2018), and so their ongoing healthcare in relation to gynaecology, obstetrics and sexual health and wellbeing, as well as access to such rights, should be a priority. These issues are exacerbated for the high number of women who are repeatedly imprisoned for short sentences (Ministry of Justice (MoJ), 2020b), specifically concerning the continuity of care. This article highlights the lack of attention to this important aspect of imprisoned women’s health and rights, using the limited information available in academic, policy and charity commissioned research. In so doing, the article argues that adequate and suitable reproductive healthcare needs to be seen as an essential aspect of women’s rights. Furthermore, the current nature of imprisonment in England and Wales results in multiple and frequent rights violations.
Reproductive rights are an essential aspect of women’s rights. The Office of the High Commissioner for Human Rights (OHCHR, n.d.) identifies that sexual and reproductive rights are related to multiple human rights, including the right to life, the right to be free from torture, the right to privacy, the right to education, the prohibition of discrimination and the right to health, which includes sexual and reproductive health. Consequently, ‘States have obligations to respect, protect and fulfil rights related to women’s sexual and reproductive health’ (OHCHR, n.d.). Such rights encompass substantial aspects of women’s health, such as health and wellbeing connected to menstruation, including access to suitable sanitary items; gynaecological healthcare; experiences of and treatment for symptoms of menopause and perimenopause; decisions about whether, when and how often to become pregnant; ways to prevent pregnancy, including abortion; and care during pregnancy, including treatment and support for miscarriage or stillbirth. If taking a reproductive justice perspective, then far more is encompassed under the umbrella of women’s reproductive rights, including access to adequate housing, education and employment to assist women ‘to maintain personal bodily autonomy, have children, not have children, and parent the children [they] have in safe and sustainable communities’ (SisterSong, n.d.; see also, Luna and Luker, 2013; Nelson, 2003; West, 2009).
Prison has always been a right-limiting institution with one of the stated purposes to deliver ‘reform [of] offenders to prevent more crime from being committed’ (MoJ, 2016b: 20). However, the ability of the State to remove the rights of prisoners is not absolute and needs to be tempered with human rights law and other competing policies; this is specifically relevant to reproductive healthcare. Following an agreement based on a formal contract between HM Prison Service and the National Health Service (NHS) in 2000, there is a statutory recognition that prisons are required to provide the ‘same level of care and access to services’ as those in the wider community (North, n.d.). In addition, the United Nations General Assembly (2010) Rules for the Treatment of Women Prisoners and Non-Custodial Measures for Women Offenders, also referred to as the Bangkok Rules, state that women in prison should be given, and have access to, gender-specific care. This, in theory, means that women’s reproductive healthcare should be of equal standard to that provided in the community. Thus, this offers a foundational basis from which reproductive healthcare and connected rights for imprisoned women stem, with accompanying legal obligations for the State and State agents who operate in prisons. Nevertheless, as outlined in this article, the structures and conditions within prison and the inadequacies in policies have created barriers to delivering such adequate care for women (Birth Companions, 2016; Corston, 2007; North, n.d.). Consequently, prison can be identified as a site of reproductive rights violation for women – a theme which reoccurs throughout this article.
To assess current knowledge and understanding of women’s access to their reproductive rights while imprisoned, a rapid evidence assessment (REA) of academic and grey literature, including official policy documents and reports, was conducted. This article outlines the findings and the implications for current understandings of imprisoned women’s reproductive healthcare and rights. It does so in three parts: methodological explanation of the approach to the REA, reporting of the key findings and a discussion of what is currently known and unknown about these issues. This article concludes that there is not enough available research to comprehend the full nature of women’s experiences of accessing reproductive healthcare and their reproductive rights. Existing research does, however, indicate that prison is a site of multiple and frequent reproductive rights violations for women.
Methodology
A question-led adapted REA was conducted to determine what is currently known about women’s ability to access their reproductive rights while in prison in the United Kingdom and pinpoint significant omissions within the current literature – specifically, women’s access to/of reproductive healthcare in prison in the United Kingdom (research question 1); imprisoned women’s experiences of reproductive healthcare in the United Kingdom (research question 2); their experience of pregnancy (diagnosis of pregnancy, continued to term, non-intentional miscarriage/stillbirth and intentional miscarriage/abortion) in prison in the United Kingdom (research question 3). These research questions were devised to provide a holistic understanding of the core issues related to women’s reproductive health and rights. REAs allow for a systematic assessment of existing evidence on a topic in a fraction of the time it would take to conduct a systematic review. Thus, while not as exhaustive as a systematic review, an REA is nevertheless detailed and focused. The rigorous method allows for the locating, appraising and synthesising of evidence from previous research and official documentation (Burton et al., 2007; Thomas et al., 2013). From the research questions, search terms were devised relating to reproductive health (health care, healthcare, pregnan*, expecting, labour, abort, test) and imprisonment (e.g. prison*, gaol*, jail*, incarcerat*).
The REA comprised three stages: identifying the literature, screening the search results and conducting a weight of evidence (WoE) of included literature and synthesising the results. To allow the search strategy to be reproducible, clear criteria for inclusion and exclusion of literature were devised (Table 1).
Inclusion and exclusion criteria.
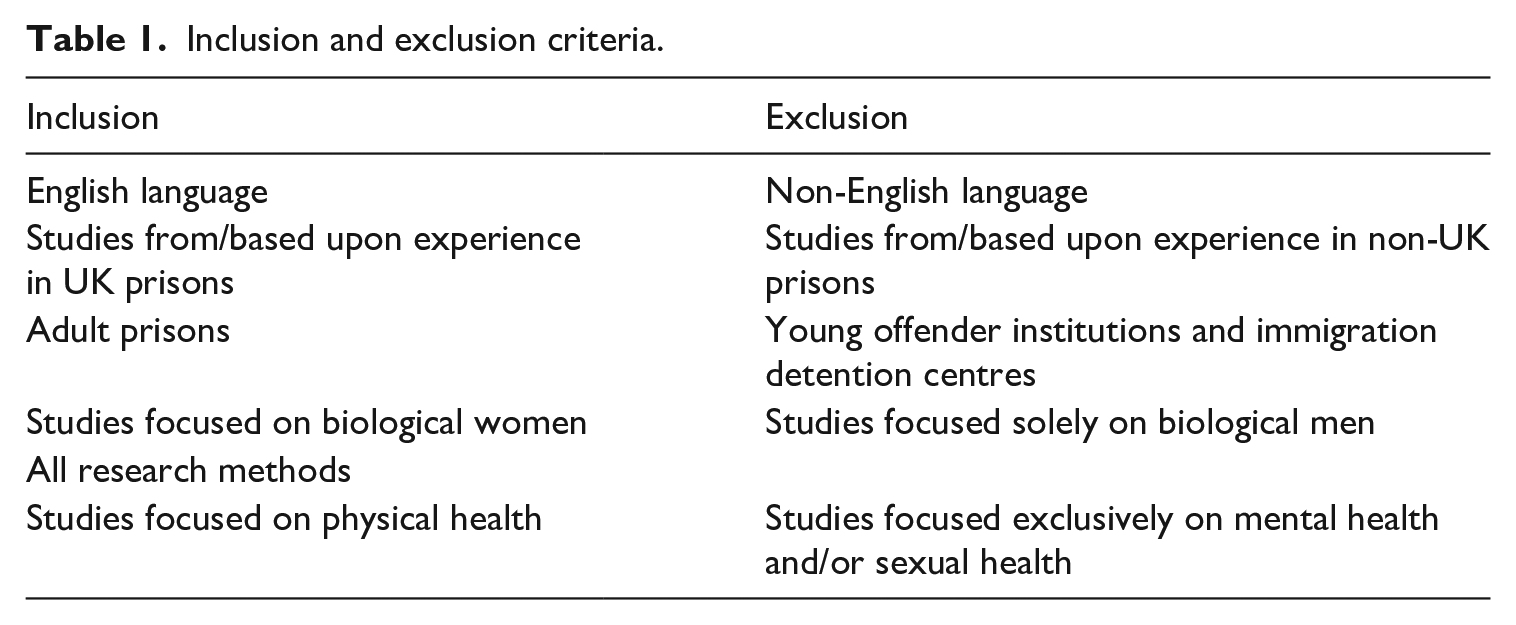
As prison systems around the world are different in nature, the study focused on the experiences of women imprisoned in the United Kingdom. Literature published prior to 1967 was excluded as this is the date that abortion became legal in Great Britain, thus having a significant impact on women’s reproductive rights. Included literature centred on women’s bodily health, rather than mental health (Dolan, 2016, 2020). Studies solely looking at women’s sexual health were omitted from the search criteria. While it is appreciated that sexual health is part of women’s reproductive health, the relevant sexual health literature largely focuses on the management and omission of AIDS (Chan et al., 2015) and sexually transmitted infections (Tang et al., 2010). The concern of these studies was therefore on ‘risky behaviour’, rather than on sexual health as an element of reproductive health.
To identify the literature (stage 1), researcher 1 used the devised key words to complete searches of academic databases (Web of Science, PsychINFO, Hein Online, Social Sciences Citation Index, Lexis Nexis and Medline), online sites (Google Scholar/Google) and repositories of grey literature (relevant UK and European Union (EU) government policy documents, regulations and guidance, and reports from non-governmental organisations (NGOs) and other interested parties). For the online and grey literature searches, only the first 50 items from each database were screened, which is in keeping with the rapid delivery of an REA. The searches for stage 1 identified literature published up to the end of July 2020. In all, 1,119 hits were identified. A subsequent search was conducted in June 2022 to update the findings prior to publication. A further 17 papers were included.
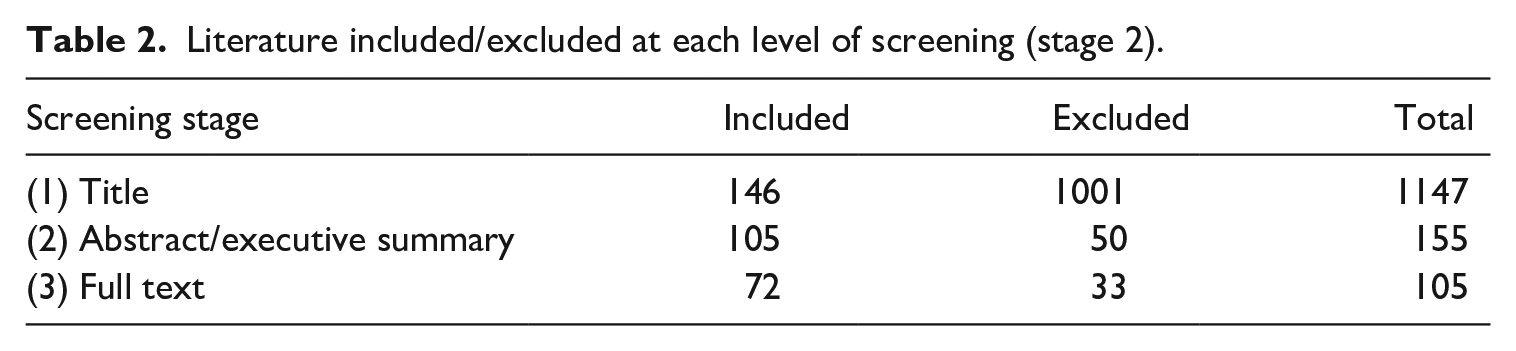
Screening of the search results and literature (stage 2) to confirm included results met the research criteria was conducted by researcher 1. Screening consisted of three levels: (1) based on the title of the piece, (2) the abstract or executive summary and, finally, (3) reading of the full piece. To ensure quality assessment and transparency of decision-making (Varker et al., 2015), 10% of the titles and abstracts/executive summaries, and all full texts were reviewed by the second researcher. Table 2 shows the number of pieces included and excluded at each point in the screening process.
Literature included/excluded at each level of screening (stage 2).
At stage 3, researchers 1 and 2 independently conducted a WoE to evaluate the quality and relevance of the results in line with the research questions. Results were given a strength rating (high, medium or low), an approach derived from David Gough (2007), thus ensuring consistency. Divergence in ranking between the researchers was discussed and agreed upon, in line with the research questions and strength of the piece. Table 3 shows the results of the WoE by research question.
Summary of the papers included by research question and WoE category.
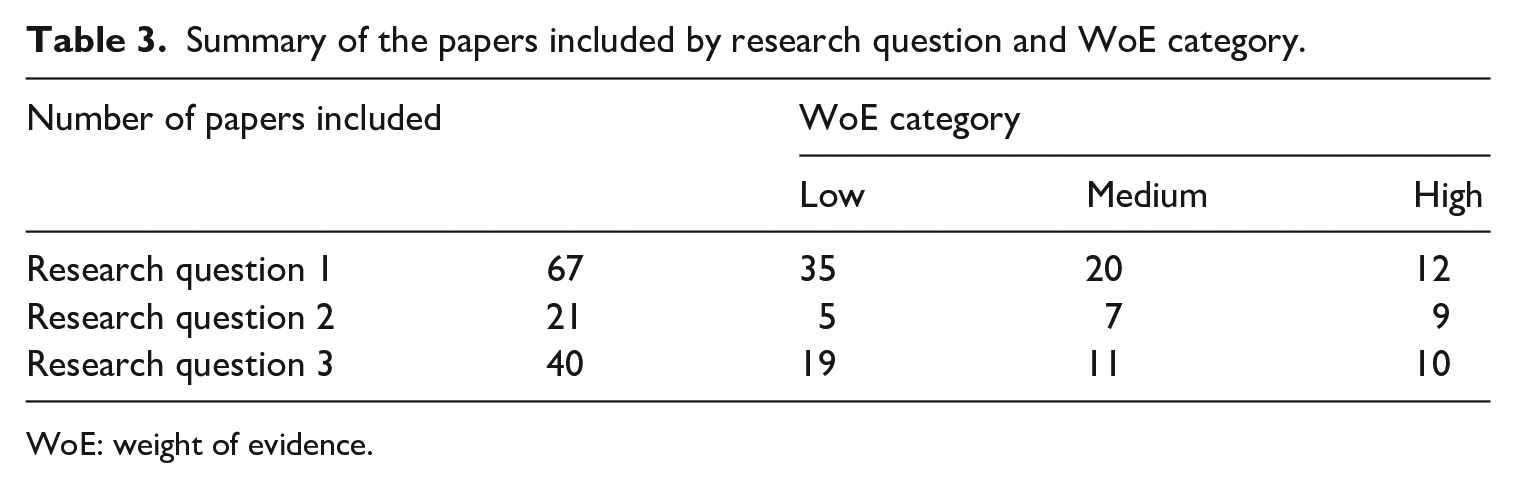
WoE: weight of evidence.
At stage 3 of the REA, the data collected for each of the research questions were synthesised to form a critical assessment of the current state of knowledge for this key aspect of women’s rights and health. See Supplemental Appendix A for a full breakdown of the 72 papers included in the final study, the research questions they related to and the WoE given.
Results: What is currently known
Synthesising the 72 included papers across the three research questions illustrates that the picture of imprisoned women’s access to their reproductive rights is fragmented, fractured and uneven in terms of areas that have received coverage and focus in academic literature, government and official sources, and research and reporting by NGOs and charities. Pregnancy and childcare in prison is the area of women’s reproductive healthcare about which the greatest level of information is known. Most of the literature in the broad area of women’s reproductive healthcare while in prison focuses on pregnancy and the antenatal and postnatal care women have received (56 papers: academic = 17, grey = 39). Most of this literature is focused on maternity care provision, particularly discussions surrounding parenting support: how women access Mother and Baby Units (MBU), the overall condition of these units within and across prison sites, and women’s experiences of separation from their babies (total 39 papers: academic = 11, grey = 28). A smaller number of studies have considered women’s experience of pregnancy while in prison. Nine of those studies (academic = 4, grey = 5) utilised scoping exercises and/or have drawn on the views of prison staff and healthcare professionals to reach their conclusions. A further 15 studies (academic = 11, grey = 4) considered women’s views on/experiences of pregnancy.
Very little has been written about women’s experiences of ending a pregnancy while in prison. There is little to no research focused on abortion, miscarriage or stillbirth experienced by imprisoned women (9 papers: academic = 6, grey = 3). Policies and guidance related to ending a pregnancy within prison are also sparse (3 papers). Knowledge is also limited in other key areas of women’s reproductive health. There are a small number of reports and research papers that report findings on the health issues of incontinence, cervical screening, fertility services and menstruation (7 papers: academic = 5, grey = 2).
Discussion
From the papers identified for inclusion to answer the three research questions, five key themes were identified: reproductive healthcare as an ‘issue’ to be ‘managed’; inconsistencies across and between prisons and policy; a focus on pregnancy; limited information about the ending of a pregnancy in prison; and the large gaps in current knowledge, including that women’s experiences are predominantly missing. Together, this information and data point to the conclusion that prison is repeatedly and consistently a site of reproductive rights violation. As will be discussed below, this aspect of rights violation raises further questions about the suitability of prison as a form of punishment for women who are criminalised.
‘Managing’ reproductive health and capacity
Within the official literature included in the REA (guidance, policy documents and reports produced by State agencies), the reproductive health of imprisoned women is viewed as an ‘issue’ that needs to be ‘managed’ as an aspect of their imprisonment. A clear example is Prison Service Order (PSO) 4800, ‘Women Prisoners’, which was introduced in 2008 into the canon of standards of ‘best practice’ for prison staff in England and Wales. PSO 4800 was initiated ‘to provide regimes and conditions for women prisoners that meet their needs’ (HM Prison and Probation Service (HMPPS), 2008: 1). While providing little in the way of specific guidance relating to women’s reproductive health, the document did advise that women should be provided with the necessary means and provisions to maintain their own hygiene and personal care – specifically, to have easy access to a choice of sanitary provision. It also recommended that antenatal and postnatal services include specific provisions for pregnant drug users. With reference to pregnant women, it specified that suitable nutrition and rest are required but that staff should be mindful that perceived ‘special treatment’ may leave a woman open to becoming a target for bullies. The PSO also states that handcuffs should not be used after arrival at hospital or clinic appointments, and women should not travel in cellular vans, due to potential risks inherent in being locked in a confined space. The PSO also directs the Prison Service in making adequate provisions for women wishing to breastfeed their babies and suggests that careful planning should take place when women are being separated from their babies, due to the risk to their mental health. It is noted that procedures for managing women who have experienced miscarriage, termination of pregnancy, stillbirth or neonatal health issues need to be adhered to. For mothers who enter prison, PSO 4800 stated that support is also given with respect to how women can maintain contact with children throughout their sentence, as well as directives on resettlement processes.
From this PSO, we can see that standards of best practice have been provided to prison staff regarding aspects of women’s reproductive health. However, the framing and phrasing of the PSO was such as to make it clear that the points raised were seen as ‘issues’ in the lives of imprisoned women that needed to be addressed. Reproductive healthcare and wider rights (including the ability to care for their children) were not considered holistically in terms of women’s lives, nor as essential elements of women’s experiences that originate from their bodies, but as factors that need to be ‘managed’. As Abbott (2018) argues, the language is ‘cloaked in benign paternalism’ (p. 164).
The detrimental impact of this approach to women’s reproductive health and rights was exasperated in 2018 when PSO 4800 was cancelled and replaced by the Women’s Policy Framework (MoJ and HMPPS, 2018). This new document offered a far less detailed set of expectations, reducing the level of specificity that prison staff need to follow, with standards framed as a requirement to ‘assess and address’ the needs of women concerning aspects of reproductive health, such as pregnancy. The reduced level of specific information has the potential consequence of allowing greater variability across the prison estate in terms of how women’s reproductive health and rights are approached and responded to. The concept of what should occur for a woman’s needs to be addressed is left to the discretion of staff in individual prisons.
Similar framing can be seen in official documents relating to pregnancy and the care of infants in the postpartum period. These ‘issues’ are ‘tagged in’ wider health policy and documentation (National Institute for Health and Care Excellence (NICE), 2016; Public Health England, 2018), in recommendations for pregnancy and childbearing care (Corston, 2007) and, as noted above, in various prison frameworks and policy and guidance documents (HMPPS, 2000a, 2000b; 2008; MoJ, 2020a; MoJ and HMPPS, 2018, 2021). National health standards and guidance for women in prison have been published by Public Health England (2018) and HM Chief Inspector of Prisons (HMCIP, 2014a); these also do include wider considerations of reproductive health, pregnancy and parenting. Yet, Public Health England (2018) is the only document that provides guidance on the gender-specific standards pregnant women should receive. The standards include support on all aspects of antenatal and postnatal care (such as accessing abortion services, or experiences of ectopic pregnancy, miscarriage or stillbirth).
Inconsistencies between prisons and policy and across prisons
One of the major challenges to women receiving sufficient reproductive healthcare and thus accessing their reproductive rights that emerge from the literature is the inconsistencies that exist between the standard of care outlined in policy documents and what occurs on the ground.
As most of the research identified in the REA focuses on pregnant and postpartum imprisoned women, it is in this area that inconsistencies between policy and practice are most apparent. Maternity services are provided by the NHS, and the standard of care should be equivalent to that provided in the community (Codd, 2012; North, n.d.; Price, 2005). Research has consistently shown that the care of imprisoned women during and after pregnancy and childbirth has been grossly inadequate (Abbott, 2018, 2021; Abbott et al., 2020; Baldwin, 2021; Epstein et al., 2021; Ginn, 2013; North, n.d.; Parliament et al., 2019; Price, 2005), with persisting gaps between policy development and consistent implementation. It has also been argued that there is a need for further guidance and consistency across prison estates, and the sharing of good practice (The Fawcett Society, 2009) – an aim also outlined in current policy documents (MoJ, 2020a; MoJ and HMPPS, 2021).
A further inconsistency raised by academics and researchers is the variation of care across the prison estate and between different prisons. Research with midwives unearthed that many felt frustrated in their efforts to deliver an antenatal service comparable to that on offer ‘outside’. Midwives cited the nature of prisons, and the Prison Service, as causing these variations (North, n.d.; Price, 2005). Individual prisons tend to run to their own rules, which results in healthcare for pregnant women often being provided in an inconsistent and ad hoc manner. In one Category C prison, for example, it was stated that a woman may have her partner attend an ultrasound appointment with her, and in another, she cannot (North, n.d.). Prisoner relocation or release at short notice was also cited by midwives as a barrier to delivering quality services. Midwives are neither promptly nor routinely informed of imprisoned women’s movements, and there is no established network of contacts between prison midwifery teams (North, n.d.).
The research literature also highlights that new mothers residing in MBUs have widely divergent experiences, both between and within prisons. Some women have positive experiences, recognising the support provided by individual officers and outside agencies. For example, Maya Sikand (2017), in her discussions with 15 women, noted that once in a MBU, women and babies can flourish (see also, Birth Companions, 2016). For others, experiences on MBUs were extremely difficult and stressful (Birth Companions, 2016; Gardiner et al., 2016). In interviews with imprisoned mothers and professionals involved in the support of mothers and babies, Adelle Gardiner et al. (2016) found that ‘arrangements do not adequately account for the often-complex needs of imprisoned mothers’ (p. 4). Mothers often felt isolated, and it was deemed there was a lack of access to appropriately trained skilled professionals. Arguably, the lack of a specific PSO focused on the needs of pregnant women and women with infants is exacerbating the inconsistencies in services provided for women and their infants. As argued by Jenny North (n.d.), a specific PSO could set mandatory minimum national standards that prisons should adhere to. Adequate funding for prison antenatal care is also of utmost importance to ensure that minimum standards are upheld across all prison establishments (North, n.d.; Royal College of Midwives (RCM), 2019).
Focus on pregnancy and MBUs
As already noted, research focused on pregnancy, postpartum care and MBUs dominates the literature on imprisoned women’s reproductive health (Abbott, 2015, 2018, 2021; Abbott et al., 2020, 2021; Baldwin, 2021; Birth Companions, 2016; Corston, 2007; Elton, 1988; Gardiner et al., 2016; Ginn, 2013; Gullberg, 2013; North, n.d.; Plugge et al., 2006; RCM, 2008; Sikand, 2017). Accurate numbers of pregnant women held in UK prisons are not recorded, although it is estimated that 6%–7% of the female prison population are at varying stages of pregnancy at any one time, and that around 100 babies are born in prison each year (Abbott, 2018; Birth Companions, 2016; Prison Reform Trust, 2017). However, not every woman will choose to have a pregnancy test on arrival, and some women may pass through prison without their pregnancies being recorded (Ginn, 2013). Thus, we have very little knowledge of how many pregnant women are imprisoned each year. Furthermore, the records of birth weights of babies born in prison are not kept, nor are the incidences of miscarriage, birth complications or stillbirths (North, n.d.). As Jenny North (n.d.) argues, the collation of these statistics would indicate a commitment to the welfare of imprisoned women and their foetuses/babies. Availability of such data would allow an analysis of any significant discrepancies between the statistics for imprisoned women compared to women from similar social backgrounds in the general population, so supporting the delivery of services. The MoJ (2020a) have stated they intend to publish national data providing a snapshot of the women in prison who are pregnant and the annual number of births that occur.
From the limited research that focuses on women’s experiences of pregnancy, the findings provide a very troubling picture of the situation faced by women. Unfit conditions within and the regimes of prison have been reported to have a negative impact on pregnant women’s health and wellbeing, specifically in terms of nutrition, issues with bathing and showering, fresh air and lack of comfort (Abbott, 2015; Abbott et al., 2020; Corston, 2007; Gullberg, 2013; North, n.d.). Evidence from studies paints a grim picture for women. In her ethnographic observations, Laura Abbott (2018) noted the strong smell of tobacco that circulated within the prison she visited and the lack of fresh air. From her discussions with midwives, Jenny North (n.d.) was told about one case where a midwife asked for extra pillows so that a pregnant woman with swollen ankles could sleep with her legs raised. This request was turned down, with no explanation of what operational or security problems the extra pillows would pose. Such difficulties were also highlighted in consultation with imprisoned women and prison staff, with pregnant women being afforded no special treatment: women did not, for example, receive healthy snacks, breast pads, maternity bras or suitable bedding (Abbott et al., 2020). The lack of availability of such items occurs despite entitlements of pregnant women being outlined in numerous policy documentation (HMPPS, 2000a, 2000b: F35, cited in Abbott, 2018). Bodily suffering during pregnancy was thus often exacerbated by regimes and conditions in prison; for example, Abbott et al. (2020) describe the experience of ‘Abi’, who was so unwell due to her pregnancy that she was unable to work which led to a loss of possessions and privileges.
The care imprisoned pregnant women receive when outside of the prison was also noted to be highly problematic. Women must be accompanied by prison officers to appointments held outside the prison; however, prison officers are often unavailable as escorts due to staff shortages. The consequence is that outpatient appointments may be cancelled at the last minute, so preventing timely scans or other investigations, and thus potentially detecting serious conditions (Ginn, 2013; North, n.d.). Abbott et al. (2020) also note that women experience being handcuffed and placed in chains during hospital appointments and being strip-searched by female officers upon return from hospital. Despite numerous campaigns from the 1990s to date vigorously calling for a prohibition on the shackling of pregnant women (see Kitzinger, 1994, 1997), an interview with one prison governor by Stephen Ginn (2013) reveals that while shackling during labour is ‘extremely unlikely’, it is not forbidden.
There are countless cases of difficult pregnancy and birthing experiences being exacerbated by institutional neglect within prison (Corston, 2007). Plugge et al. (2006) report that one woman experienced a life-threatening 2-hour delay in being transported to hospital following an ectopic pregnancy. The delay was due to the nurse misdiagnosing her symptoms, which occurred despite the woman informing the medical team that she had previously suffered from the condition (see also Plugge et al., 2008). Tragically, three babies born to imprisoned women have died after the women delivered while in prison or in an ambulance travelling to hospital (Baldwin, 2021; Baldwin and Epstein, 2017; Prisons & Probation Ombudsman, 2021, 2022). Fear of the possible delay in receiving care and transport to the hospital upon the commencement of labour has reportedly resulted in women choosing medicalised models of childbirth, such as an elective caesarean section (Abbott et al., 2020). Such decisions call into question the notion of ‘choice’ for women and once again illustrates that the standard of medical care is not equivalent to that experienced by women in the community. The story of ‘Layla’, provided by Abbott et al. (2020), reminds us that women are being forced to give birth in their cells without the help of a midwife or medical practitioner due to prison staff not responding to their calls for assistance (p. 669). The conflict between caring and custodial duties, and between the need to protect women while also punishing, becomes apparent in light of such examples.
Of the literature relating to pregnancy and childbirth, the majority is focused on women’s experience after giving birth – specifically the conditions of and experiences on MBUs. Of the 12 women’s prisons in the United Kingdom, six have MBUs, with 64 places available nationally. The MOJ and HMPPS policy document, Pregnancy, Mother and Baby Units (MBUs), and Maternal Separation from Children up to the Age of Two in Women’s Prisons, outlines the role of MBUs, the application process, mother-baby separations and management of MBUs (MoJ and HMPPS, 2021; supported by MoJ, 2020a; replacing National Offender Management Service (NOMS), 2014; supported by MoJ, 2016a). However, reports from NGOs have noted the lack of transparency in guidance (11 Million, 2008; Prisoner Advice Service, n.d.). HMCIP (2006, 2007, 2010, 2012, 2013, 2014b, 2015, 2016, 2017) reports give insights into conditions within MBUs. Reports are, in general, positive and comment on improvements made in recent years. In particular, reports about the quality of childcare and staff attitudes have been encouraging (HMCIP, 2015, 2017). Academic research supports these positive evaluations of experience-based programmes for mothers and infants (Baradon et al., 2008; Sleed et al., 2013). Nevertheless, HMCIP (2014b, 2015, 2016, 2017) have also reported limitations of MBUs. One challenge of using these inspector reports to assess women’s access to their reproductive rights is that the observations reported are often vague, with limited detail. When detail is provided, either by drawing on examples at specific prisons or via the use of individual policies and/or procedures, the practices in prisons are seemingly at odds with gender-specific health guidance. For example, the Annual Report for 2015–2016 noted that women in the MBU in New Hall were expected to remain in their rooms with their babies after 7:30 p.m. (HMCIP, 2016). This restriction contrasts with the standards that were set by HMCIP (2014a: section 2.25) in their ‘Expectations’ report, which states, ‘mothers are able to freely leave their rooms at night’. This example from official reports provides further evidence of the limits placed on women and thus raises concerns about violations of their access to their rights in conjunction with MBUs.
HMCIP Annual Reports have also detailed how, in various prisons, MBUs are underused (see HMCIP, 2012, 2013). Regardless of this underutilisation, recent statistics demonstrate that since 2012 there has been a steady rise in the rejection rates of women who have applied for a place in a MBU. Furthermore, women’s appeals against these decisions to reject their application are often unsuccessful, with only 24% of appeals resulting in a successful outcome in 2015 (Sikand, 2017). Recent research has described the complications involved in gaining a place on a MBU and the complexities of the appeal process when denied a place (Abbott, 2015, 2018; Abbott et al., 2021; Baldwin, 2021; Sikand, 2017). Maya Sikand’s (2017) study with women and staff across multiple prison sites focused on women’s experiences of the MBU decision-making process. She concluded that the process is unclear and women find it obscure: applicants are given minimal information and are effectively prevented from taking any meaningful part in the admissions process. Sikand observed that there is little prospect of admission if women have a custodial history. Navigating the bureaucratic layers when applying for MBU places is therefore difficult. The uncertainty of, and delays during, this process creates high levels of stress and anxiety (Abbott, 2015, 2021; Baldwin, 2021; Birth Companions, 2016; Codd, 2012). Delays can mean that newborn babies are placed in foster care after birth, and even if mother and baby are subsequently reunited in an MBU a few weeks later, the separation can interfere with the bonding process and can have a profound and negative effect on the mother’s health and wellbeing (Codd, 2012; North, n.d.). Furthermore, the death of Michelle Barnes from suicide shortly after her child was removed from her care post-birth and she was returned to prison highlights the trauma and distress that women experience (Prisons & Probation Ombudsman, 2015; see also Abbott et al., 2021).
The spectre of ending a pregnancy: Miscarriage, stillbirth and abortion
While there has been a reasonable level of research on women’s experiences of continuing a pregnancy in prison, there is very little written about women’s experiences of ending a pregnancy while in prison, with little to no research focused on abortion, miscarriage or stillbirth experienced by imprisoned women. The report by Maternity Alliance, a UK maternity rights charity (North, n.d.), offers one of the few examples of published research that includes a focus on women’s access to termination of pregnancies, concluding that it is difficult to determine how easily women are able to access abortion or what support women are given in relation to decisions to terminate a pregnancy. While knowledge and understanding in this area are limited by the lack of research, available data would suggest that women are not being supported to terminate their pregnancies while in prison (Abbott, 2018; Codd, 2012). Research indicates that it is likely that women who are confirmed to be pregnant on arrival in prison are offered little advice about their options for the outcome of their pregnancy for the duration of their imprisonment (Birth Companions, 2016; North, n.d.). The potential consequence is that women who wish to terminate the pregnancy would need to remain pregnant until their release, accessing a later abortion. Unsurprisingly, there is no empirical research that has focused on women’s experiences of accessing abortion services from prison. More needs to be known about women’s experiences of accessing abortion while in prison, as without this information we have very limited means to assess this aspect of reproductive healthcare provision and women’s reproductive rights. For example, what, if any, impact has the decision to make telemedical abortion permanent in England had on imprisoned women (Royal College of Obstetricians and Gynecologists, 2022)?
Even less information is known about women’s experiences of their pregnancies ending due to miscarriage or stillbirth. Figures as to the number of miscarriages or stillbirths are not currently kept by HMPPS. Poor pregnancy health and inadequate antenatal care in prison may be contributing to rates of miscarriage or stillbirth, another unknown. As Codd (2012) outlines, it is valuable to understand what support is available in prison for women who miscarry. She further notes that without a better understanding of how easy it is for a woman to obtain an abortion, we are unable to determine what proportion of miscarriages may, in fact, be self-administered terminations. This point is significant, as self-administered abortions remain illegal in England and Wales, punishable by up to life imprisonment (Offences Against the Person Act 1861, s. 58).
Where are the women?
As the above discussion suggests, very little is known about women’s experiences of and ability to access their reproductive rights while imprisoned. Existing research generally focuses on the impact on a baby who is born to an imprisoned woman (see Elton, 1985). When women are included in the research, it is often not to further our understanding of their experiences, but has other concerns, such as the impact on the baby caused by separation from its mother (Baradon et al., 2008); how women’s health and wellbeing will impact the child (Codd, 2012; North, n.d.); breastfeeding outcomes (Abbott and Scott, 2017; Tremarco et al., 2020); or to evaluate programmes designed to ‘teach’ women how to be ‘better’ mothers (Baradon et al., 2008; Sleed et al., 2013).
Existing academic literature that is women-centred (Abbott, 2015, 2018; Abbott et al., 2020; Birth Companions, 2016; Gardiner et al., 2016; Plugge et al., 2006; Sikand, 2017) conveys the stress, fear and anxiety caused by prison conditions, notably in relation to pregnancy. Findings suggest that prison life continues with little thought to the unique physical needs of pregnant women. Abbott et al. (2020) note that to navigate feelings of a loss of control, disempowerment, shame and humiliation, women employ various coping mechanisms; for example, fearing for the safety of their unborn child, women often wear baggy clothes as a means to hide or not draw attention to their growing bumps. Furthermore, women are reported to anticipate the grief of separation from their baby, pre-empting the actual removal of their child; such grief is further compounded when separation actually occurs (Gardiner et al., 2016).
Beyond pregnancy and the ending of a pregnancy, considerable gaps in our knowledge remain. The REA found only a small number of reports and research papers that discuss findings on reproductive-related health issues such as incontinence (Drennan et al., 2010), menopause (Baldwin and Epstein, 2017) and cervical screening (Harris et al., 2007; Plugge et al., 2006; Plugge and Fitzpatrick, 2004). The lack of attention given and data available on these issues are surprising considering that studies regularly find that women in prison are either at the same or greater risk of ill health in these areas, compared to the wider female population. A small number of studies suggest that prison contributes to issues women face with menstruation. For example, Baroness Corston (2007) noted in her report on women’s experiences of prison that women had limited access to personal hygiene products, clean and hygienic sanitary conditions and suitable nutrition. Toilet facilities were cited as being inadequate, particularly for women during menstruation. Similarly, Gullberg (2013) reported that women’s sanitary needs were not always remembered or respected by prison staff.
There are substantial aspects of imprisoned women’s reproductive health that simply seem to be missing from the literature, for example, diagnosis and treatment of health conditions such as endometriosis, fibroids and heavy and painful periods. There is no discussion of contraception for imprisoned women. While they may not need to prevent birth and/or protection against sexually transmitted infections or diseases while in prison, most women serve very short sentences, meaning that if, for example, they use long active reversible contraception (LARC), then they may need assistance with this form of birth control during their custodial sentence. Similarly, there is an absence of discussion of women’s ability to access assisted reproductive technologies such as in vitro fertilisation in prison; this is despite the European Court of Human Rights ruling that the United Kingdom’s blanket ban on prisoners’ access to artificial insemination facilities was incompatible with Article 8 of the European Convention on Human Right (Codd, 2015).
One of the further challenges limiting our understanding of women’s access to reproductive rights lies in the lack of intersectional analysis of women’s experiences. Imprisoned women are not a homogeneous group who experience reproductive healthcare uninformedly. The prison population is diverse; women’s health outcomes and experiences are dependent on their age, class, ethnic and racial background, as well as their geographical location. Yet studies identified within the REA often treat these markers as separate, independent categories. An intersectional understanding, therefore, seems to be absent in most studies, despite findings highlighting the need for such an approach to improve health outcomes and experience (Epstein et al., 2021; Harris et al., 2007). Thus, current research is limited in terms of what it can tell us about structural concerns that might be harming women or the approaches that might work to improve women’s reproductive health outcomes and rights in the context of differing experiences.
Conclusion: Prison as a site of reproductive rights violation
This article has reviewed current policies, guidance and research relating to women’s ability to access their reproductive healthcare and rights while imprisoned in England and Wales. The findings from this REA provide a patchy picture of women’s experiences. Of significance, the importance of women’s reproductive rights as a concept and lived reality is very much missing from most of the existing literature, demonstrating that women’s reproductive rights appear to be of low priority for the government, the prison system, and many academics and charities who work in this area.
The little available research that is women-centred suggests that women face multiple rights violations across all aspects of reproductive healthcare and rights. Studies reveal the difficulties women face when navigating within a prison system, where the approach to reproductive health seems to be trying to ‘manage’ these aspects of women’s lives as ‘problems’ to be solved. It appears that women who are imprisoned are consequently not supported to access and maintain their reproductive rights, but that the prison system is consistently and readily a sight of reproductive rights violation – women’s reproductive rights are both damaged and limited directly due to being imprisoned. Lack of access to suitable support and care during menstruation and to contraception counselling and services (including abortion), lack of specific care relating to gynaecological issues (including endometriosis, fibroids and heavy and painful periods, as well as cervical and ovarian cancer) and lack of consideration of the impact of menopause and perimenopause all indicate that the institution of prison is a site of State-perpetrated violence against women due to multiple rights violations. Furthermore, the evidence of the impact of imprisonment on experiences of pregnancy and childcare is so stark and damming that it raises questions as to whether pregnant women and mothers should face imprisonment at all (Baldwin, 2015; Lockwood, 2020; O’Malley and Baldwin, 2019). The fact that pregnant women were temporarily released from custody during the COVID pandemic due to the risk posed by the virus demonstrates that the State can take action to protect the welfare of pregnant women when it chooses to do so (MoJ, HMPPS and The Rt Hon Robert Buckland QC MP, 2020).
More research is needed into women’s experiences of reproductive healthcare and rights while in prison. We are unable to truly assess the extent to which prison is a site of reproductive rights violation without this research. Future research needs to be woman-centred, considering women’s experiences of reproductive health, as opposed to those of prison staff, or from a perspective of health assessment. Future research also needs to focus on the intersections of women’s identities and how these have an impact on women’s access to reproductive healthcare. Without this research, we are unable to conclude whether the punishment of prison is going far beyond the government’s mandate of ‘reform [of] offenders to prevent more crime from being committed’ (MoJ, 2016b: 20). Many would argue that prison should be hard. However, considering the evidence of significant, multiple and far-reaching reproductive rights violations, it is, perhaps, too hard.
Supplemental Material
sj-docx-1-crj-10.1177_17488958221117925 – Supplemental material for Reproductive rights on the inside: A rapid evidence assessment of women’s experiences of reproductive healthcare and rights while in prison in England and Wales
Supplemental material, sj-docx-1-crj-10.1177_17488958221117925 for Reproductive rights on the inside: A rapid evidence assessment of women’s experiences of reproductive healthcare and rights while in prison in England and Wales by Vicki Dabrowski and Emma Milne in Criminology & Criminal Justice
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Dr Emma Milne received financial support from Middlesex University, School of Law, ‘Small Grants’ funding scheme for the research published in this article.
Supplemental material
Supplemental material for this article is available online.
Author biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.