
Abstract
Female athletes are increasingly seeking knowledge and support from coaches regarding the menstrual cycle as it relates to health and performance in sport. Yet few coaches feel equipped to provide this support due to low levels of knowledge about female-specific physiology, communication barriers, and lack of access to female-specific health education. This study qualitatively examines how male and female coaches of female athletes aged 15 + responded to an online education series on supporting female athlete health and performance. Coaches were encouraged to actively apply their learning in their coaching by sharing supplemental handouts and discussing menstrual health with athletes. Coaches then shared their concerns and experiences through surveys (n = 21) and interviews (n = 5). Analysis revealed that: (1) coaches were surprised to learn that menstrual health and symptom management is a significant concern for female athletes, (2) coaches had concerns that discussing menstrual health might violate social norms, gender roles, and/or exceed the scope of their leadership responsibilities, and (3) coaches desire support in translating menstrual health learning into their work with female athletes. Additionally, female coaches (i.e., those with lived experience with the menstrual cycle) were more likely to implement menstrual health awareness in their coaching, as they were able to relate to female athletes’ concerns and experiences with the menstrual cycle in sport. This study concluded that coaches’ comfort in discussing menstrual health with athletes can be developed and that both male and female coaches need translational support to navigate the social stigma associated with the menstrual cycle.
Introduction
The menstrual cycle (MC) has been deemed a “vital sign” of female health 1 and a “navigational beacon” for healthy development of young female athletes. 2 In fact, athlete and coach literacy around menstrual health and symptom management is critical to supporting sport participation in girls and young women.3,4,5 Yet, menstrual health literacy remains low across all populations, including female athletes, coaches, and physicians,6,7 which leaves cases of menstrual dysfunction undetected, undiagnosed, and untreated.8,9
Even for healthy female athletes, the physiological changes associated with the hormonal cycle can significantly impact experiences in sport and in life.10,11,12,13,14 For example, female athletes report a myriad of MC-related symptoms that impact their availability to train and compete, including pain, stomach cramps, low mood state and anxiety, tiredness/fatigue, gastrointestinal distress, and slowed rate of recovery from training.15,16,17 Given these physical and psychological impacts, it is important that female athletes feel safe to openly discuss, and functionally address, MC-related symptoms and concerns with their coaches. 18 Yet, athletes are reluctant to seek help around MC-related concerns due to lack of knowledge on the topic, social discomfort, and lack of communication and support from coaches.19,20
Coaches, too, feel unprepared to discuss MC-related concerns with athletes due to social discomfort, coach-athlete communication barriers, 21 and low perceived knowledge around menstrual health.22,23 Studies also indicate discrepancies in coaches’ attitudes around implementing menstrual health awareness in sport. For example, Zipp and Hyde 24 and Clarke et al. 25 found that coaches want menstrual health education to better support female athletes. Yet, Majumder et al. 26 and Stratham 27 found that coaches underestimate or are entirely unaware of the impact that MC hormone fluctuations have on female athletes.
These findings suggest that coach education is needed not only to increase coaches’ knowledge about female physiology, but also to improve coach-athlete communication 28 and to “bridge the divide” between the perceptions of coaches and female athletes. 29 While several studies have pointed to the need for coach education around menstrual health,30,31,32,33 few have tested coaches’ knowledge acquisition after female athlete education (see Clarke et al. 34 and Larsen et al. 35 for exceptions), and no known studies have focused on coaches’ concerns about translating learning into practice.
In this study, I examine how coaches react to a female athlete physiology educational intervention, including the concerns coaches have about applying learning in practice by discussing menstrual health with athletes. I introduce a visual framework which uses the Stages of Concern diagnostic tool 36 alongside sensemaking theory 37 to describe coaches’ experiences in four stages. This information can be used to inform coach development for coaches of female athletes, as it highlights the concerns and challenges a coach may face as they progress from early learning about female physiology toward translating learning into practice.
Methods
Recruitment and participant sample
A combination of convenience and snowball sampling 38 was used to recruit coaches of female athletes aged 15 + . Coach recruitment is challenging because there is no centralized, efficient channel of communication for reaching coaches, as coaching in the United States, where this study was conducted, remains decentralized and ungoverned. 39 To overcome this challenge, recruitment began by inviting 30 known coaches and athletic administrators from the collegiate and high school athletics space throughout the Pacific Northwest. These initial contacts were then encouraged to share the invitation with colleagues in their networks.
Forty-one male and female coaches from a mix of sports opted into the intervention, which was approved by the host institution's Human Subjects division (STUDY00019697/ MOD00020307). Twenty-one participants completed Survey 1, ten completed Survey 2, and five volunteered to interview. The original aim was to recruit an equal mix of male and female coaches for interviews; however, only five female coaches volunteered to interview. Three interviewees were known to the researcher through prior foundational coach development courses.
Study and intervention design
The intervention was broken into two parts and spread over two weeks. Learning materials were available asynchronously, giving coaches flexibility to participate at their convenience. Parts 1 and 2 included an educational video (designed and hosted by the researcher); supplemental handouts to support transfer of learning; and a survey link to share reactions and concerns. In between Parts 1 and 2, I followed up with coaches via email to provide handouts, key reminders, and encouragement to support learning transfer. See Appendix A for intervention curriculum. Figure 1 illustrates the flow of intervention activities and data collection.
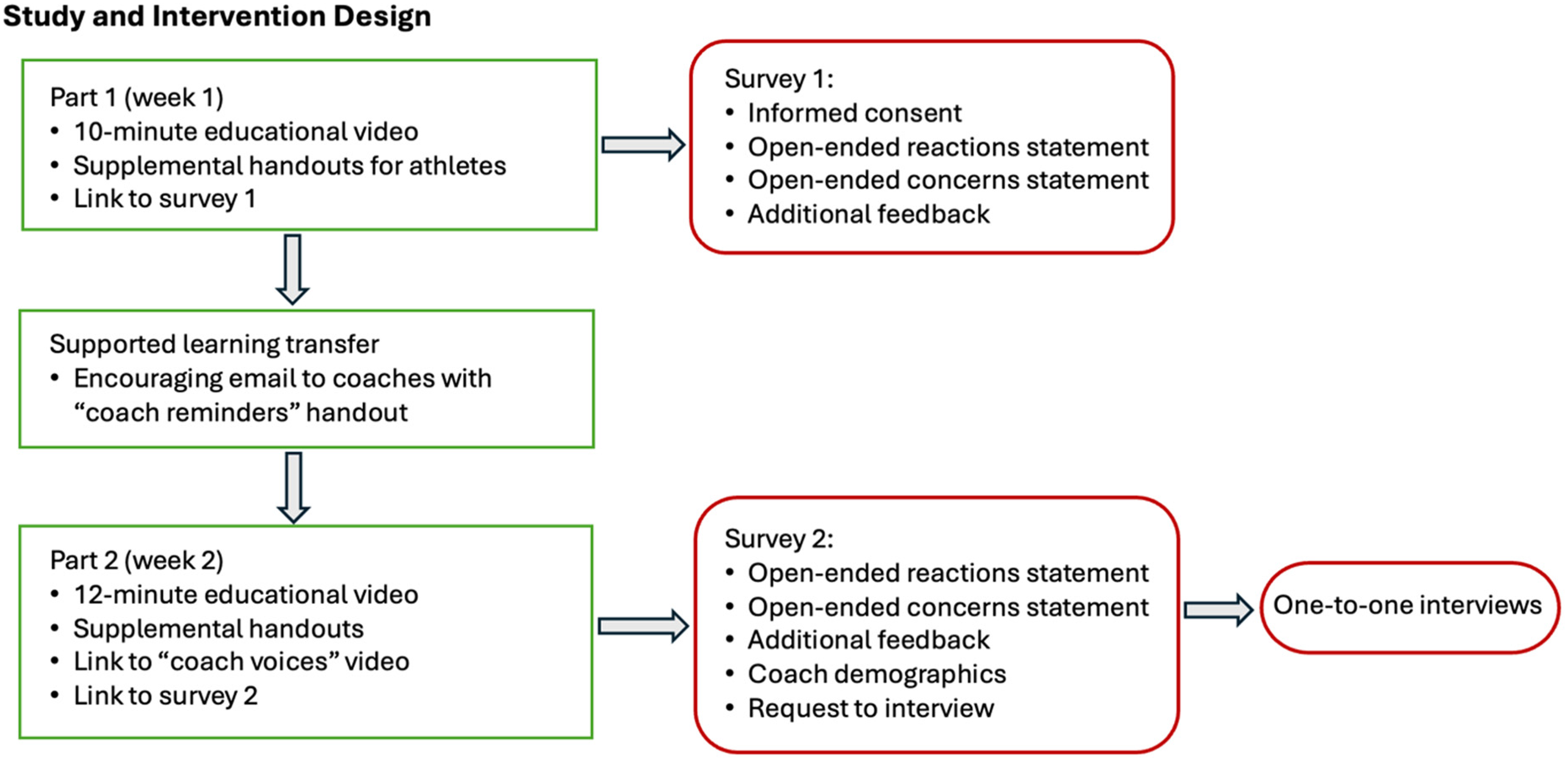
Study and intervention design. Intervention activities are outlined in green. Data collection is outlined in red.
Data collection
Coaches were invited to share their concerns and experiences through online surveys during the intervention and through a one-to-one interview at the end of the education series. Surveys were conducted with Qualtrics software. 40 Each survey included an open-ended reactions and open-ended concerns question. 41 See Appendix B for survey questions. To improve participation rates, each survey was designed to be completed in under five minutes; for this reason, coach demographics were collected only in Survey 2. However, coaches often self-disclosed demographic information in Survey 1 as part of their concerns statement. Demographic information from surveys is shared in the findings when it is known.
Interviews were conducted via Zoom videoconferencing software 42 audio recorded, and transcribed verbatim. Interviews used a semi-structured, open-ended format to allow participants to self-navigate 43 toward topics most significant to their concerns. Pilot interviews were conducted to test and refine interview protocol. 44 See Appendix C for sample interview questions.
Analysis
Thematic analysis 43 was used to summarize findings. Drawing from Charmaz’ constructivist grounded theory, 45 analysis was iterative and interpretive through my identities as a physiologist, female athlete, coach, and educator. Additionally, the voices, concerns, and experiences of the coach participants were centered; thus, findings and meaning were co-constructed between researcher and participants. To ensure reflexivity and rigor, data were reviewed with a “critical friend” 46 and member checks 47 were conducted with interview participants to check and challenge my interpretations of the data.
Analytical lenses: concerns and sensemaking theory
To examine coaches’ concerns, I utilized the Concerns Based Adoption Model's Stages of Concern (SoC) diagnostic tool (Figure 2). SoC is used in education to “describe, explain, and predict probable behaviors throughout the change process” 41 p.46], including teachers’ readiness to adopt new technologies and teaching strategies. 48
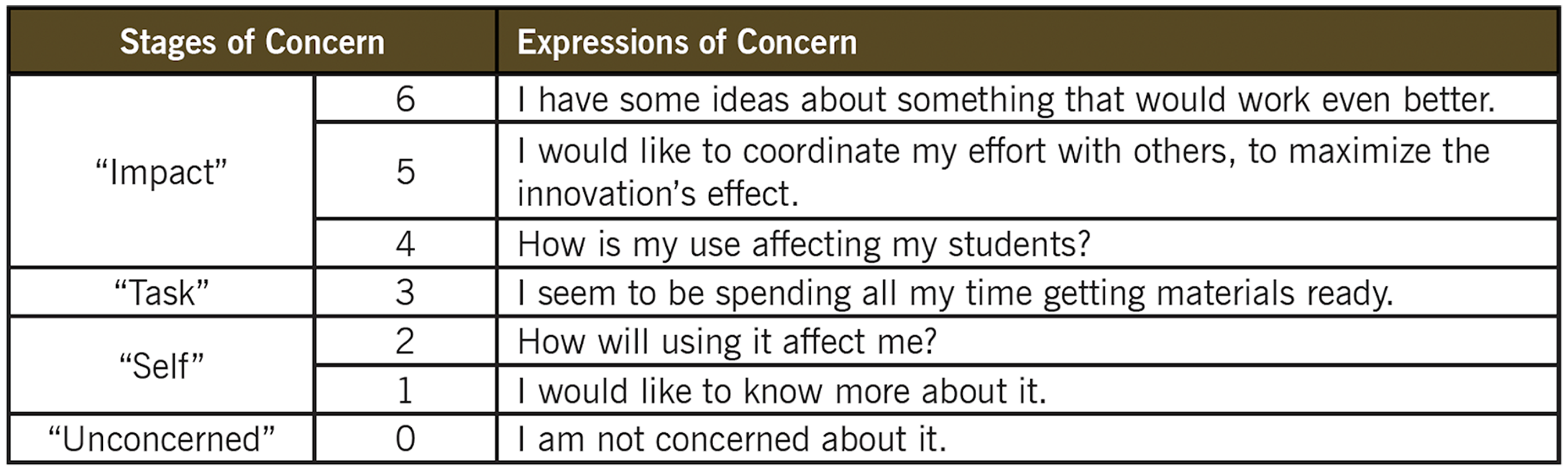
The Stages of Concern diagnostic tool. 49
SoC assumes that: (1) change is a process, not an event, and (2) an individual's readiness to apply new learning will depend on their stage of concern.
In addition to identifying coaches’ concerns, sensemaking theory was incorporated to examine how each coach's identity, sport, and social context influenced their concerns. Sensemaking is used to analyze and describe how individuals filter, interpret, and act upon new information and events.37,50,51,52,53 Klein and colleagues54,55,56 note three core tenets to sensemaking salient to this study: (1) sensemaking is driven by an individual's goals and concerns, (2) individuals filter new information through existing knowledge and beliefs, and (3) when making sense of new information, individuals are in a vigilant state of “problem detection” 55 p.117].
Drawing heavily from this work of Klein et al., I designed a visual framework to analyze and describe how coaches make sense of applying female-specific health awareness in sport.
A visual framework for analyzing and describing a coach's sensemaking process
This framework (Figure 3)—which emerged iteratively during data analysis—integrates SoC and sensemaking theory with literature in health literacy, adult learning, and neuroscience. The framework breaks a coach's sensemaking into four stages to highlight the challenges a coach may face as they progress from early learning about female-specific physiology toward translating learning into practice. I explain these four sensemaking stages below.
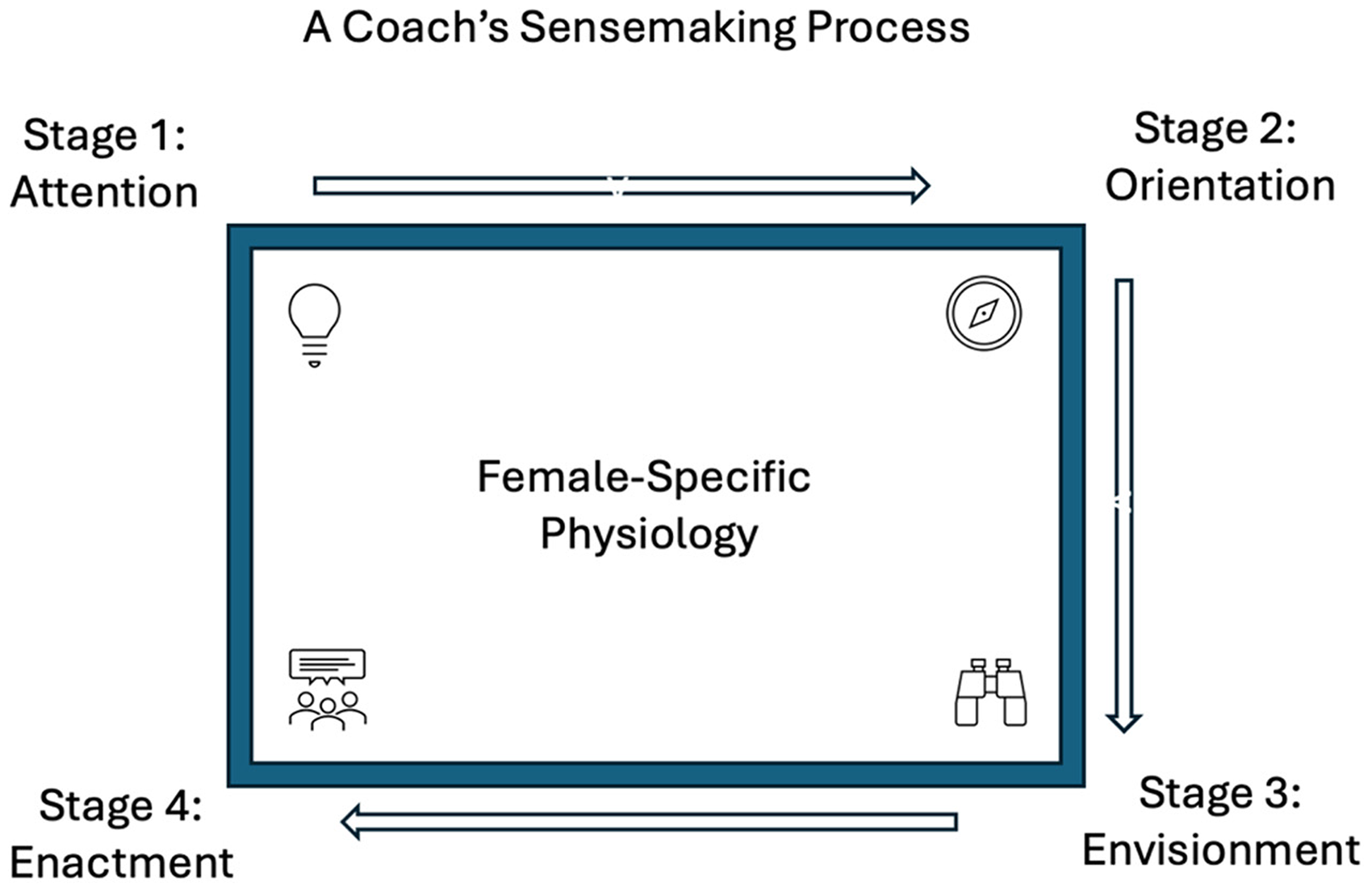
A framework for analyzing and describing how a coach makes sense of implementing female-specific physiology awareness in sport.
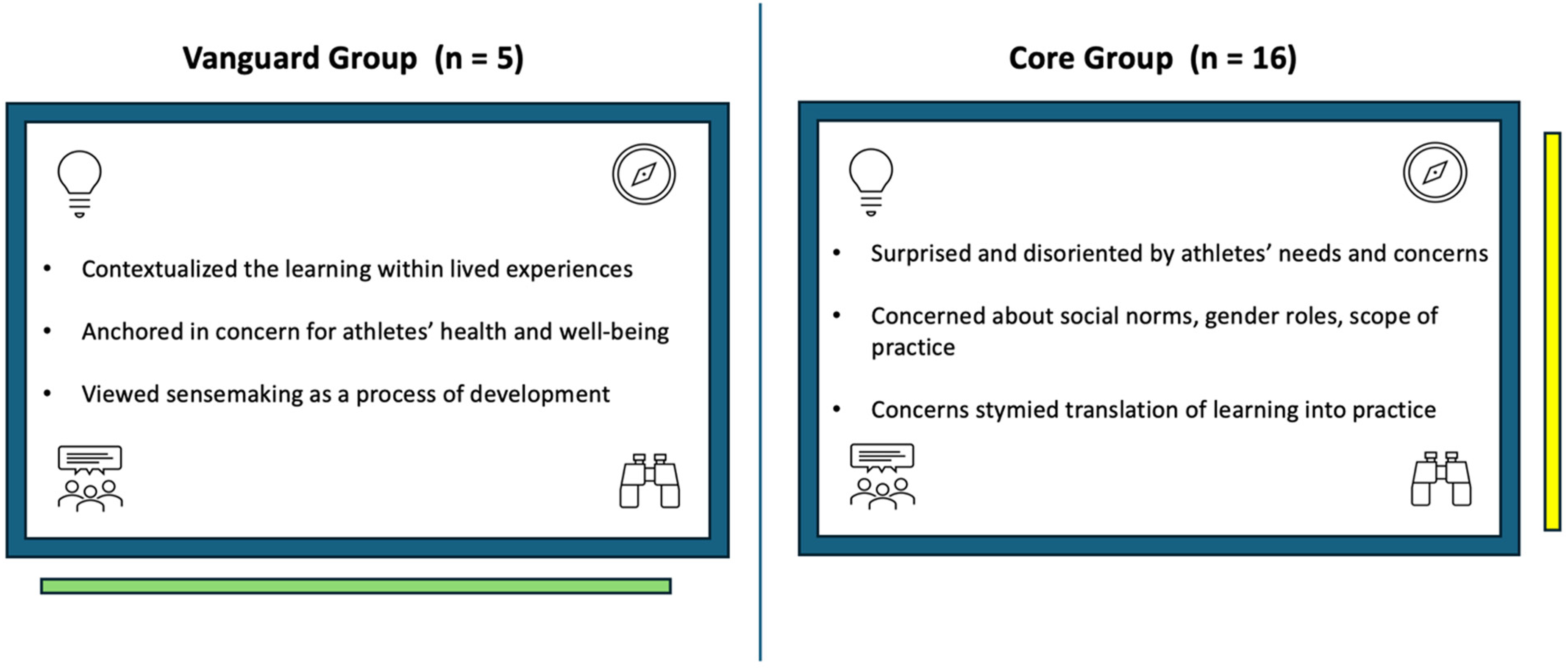
Group comparison of coach participants. The Vanguard coaches (left) were the only study participants to report translating learning into practice during the intervention; this enactment of their learning is indicated by the green line. The Core Group coaches (right) struggled to envision translating the learning into practice; this disruption in their sensemaking process is indicated by the yellow line.
Stage 1: Attention 
First, a coach's attention must be activated and their concern for female-specific health and performance registered. This can be challenging because: (1) coach education is not required of American sport coaches,57,58 and (2) the physiological needs and experiences of female athletes is a topic that has been deemed “invisible” 59 and neglected in exercise and sport science research60,61; therefore, many coaches are never made aware of the topic. Additionally, within today's fiercely competitive “attention economy”, human attention is pulled in all directions. 62 Therefore, to activate and retain a coach's attention, the coach must feel that the education is relevant to their interests, goals, and concerns. 63
Stage 2: Orientation 
Once a coach's attention is activated, they will begin orienting themselves to see how, or if, they fit within the social and cultural context of the learning content. Orientation occurs rapidly and intuitively
64
and is driven by self-focused concerns, as the coach may be asking themselves:
Is it safe for me to engage in this socially stigmatized
20
topic? Is it my role to discuss menstrual health with female athletes? Do I have the time, energy, and interest to commit to this learning?
Stage 3: Envisionment 
In Stage 3, the coach begins to engage the “slow thinking” 65 regions of their brain to “envision” how their learning might look and feel in their real-world coaching context. 66 This highly cognitive stage allows the coach to “anticipate difficulties and muster resources” 54 p.72], which is essential, as the challenges a coach faces, and the support resources they have available, will vary depending on their sport and social context.
Stage 4: Enactment 
By Stage 4, the coach has anticipated difficulties, devised strategies and support for mitigating challenges, and is ready to apply their learning in their work with female athletes.
In summary, this framework assumes that: (1) sensemaking is a process, (2) the challenges and barriers a coach faces will depend on their concerns and sensemaking stage, and, therefore, (3) as coaches work to translate their learning into practice, they will benefit from strategies and support that correspond with their concerns and sensemaking stage.
Findings
Two groups emerged in the data, the Vanguard Group and the Core Group (Figure 4). Lived experiences and challenges with menstrual health in sport differentiated the groups. The all-female Vanguard Group were the only coaches to report discussing menstrual health with their athletes during the intervention. In contrast, the Core Group, a mix of male and female coaches, expressed various concerns which they felt acted as barriers to discussing menstrual health with athletes.
Survey themes from the Core Group coaches are shared first, followed by themes from the Vanguard Group, who shared their experiences through a combination of surveys and interviews.
The Core Group (n = 16): surprised and disoriented
Three themes emerged within the Core Group's survey responses: (1) surprise that menstrual health and symptom management is a concern for female athletes (2) concerns that discussing menstrual health with athletes might violate social norms, gender roles, or leadership scope, and (3) a desire for support around implementing menstrual health awareness in their coaching.
Theme 1: Surprise: this is important to female athletes?
The Core Group coaches were surprised to learn that the impacts of the MC are a primary concern for female athletes. Many responded specifically to results shared from the Female Athlete Voice Project study,
66
which revealed that Team USA female athletes from a range of sports ranked education and support around the menstrual cycle as the number one sport science topic about which they most want to learn. Coaches expressed surprise with athletes’ high level of interest in the topic (e.g., “I was surprised that female athletes most want to know about menstrual health”) as well as surprise that athletes feel significantly impacted by MC symptoms (e.g., “I was surprised to learn that so many athletes are experiencing these symptoms” and “I was surprised to know that many female athletes want to know about how to cope with their menstrual cycle”). Another coach was particularly surprised that low menstrual health literacy extends into elite (Olympic) sport settings, as elite sport environments often have higher levels of education and support resources for athletes: What stood out to me was that Olympic athletes listed learning about the impact of the menstrual cycle on their performance as the highest priority. I think that demonstrates the lack of information that has been available to even the best female athletes. It surprised me because so much performance data is collected on top tier athletes and so you would expect that the data about the impact of their menstrual cycles would be available to them. I am surprised that I hadn't engaged with this information more as a coach. There have been moments in my career where it has come up and I can recall telling my teams that loss of MC is not normal and can be a red flag. However, I really didn't seek out more information about the impact of the MC on other areas of sport performance. I was surprised to know that so many athletes are experiencing these symptoms. I coach a sport that is not an endurance sport, and I wonder if less of the players I interact with deal with this or if it's because they aren't sharing it with me.
Theme 2: Social norms, gender roles, and scope of practice: is this my role?
The Core Group coaches expressed concerns that openly discussing menstrual health might violate social norms, gender roles, or the boundaries of their leadership responsibilities. Here, a male ultimate frisbee coach shared how he felt “anxious” that discussing menstrual health might negatively impact his relationship with his female athletes: I am a man and while I am becoming more comfortable with this subject, through education and consumption of resources, I am anxious about how comfortable my team would be with discussing the subject with me. I am close with the players I coach, we commonly discuss other health issues like more traditional injuries, again though, I am unsure how they would feel discussing this with me. My main concern is that I will get pushback from parents and other community members. I will be teaching this content in health and PE classes where there are many genders present. I anticipate some resistance from the male members of the cohort. Many of the female athletes in our sport play on mixed gender teams. I wonder how to best present this information. While it could be beneficial for the boys to be aware, a mixed setting might be too embarrassing for the girls at their current ages.
Theme 3: Applying learning in practice: coaches’ need to feel “less alone”
Finally, the Core Group coaches expressed a desire for support in communicating about menstrual health with their teams. For example, coaches appreciated the intervention's handouts guiding healthy communication with female athletes (e.g., “I’m looking forward to more handouts to share with athletes” and “I appreciate the handouts”). Coaches also expressed a desire to connect with and learn from fellow coaches, especially around overcoming fears of violating social norms. For example, several coaches responded to a component of the intervention's videos in which a male coach shared his experiences learning about and discussing menstrual health with his athletes. One survey respondent shared, “I liked seeing another coach and how he feels about this information and his approach”. Another coach stated, “It's helpful to see somebody else struggling through those same points”. Other study participants shared that seeing and hearing another coach's “struggle” helped them to feel “less alone” in the challenges and discomforts that accompany implementing menstrual health awareness in sport.
The Vanguard Group (n = 5): applying learning in practice
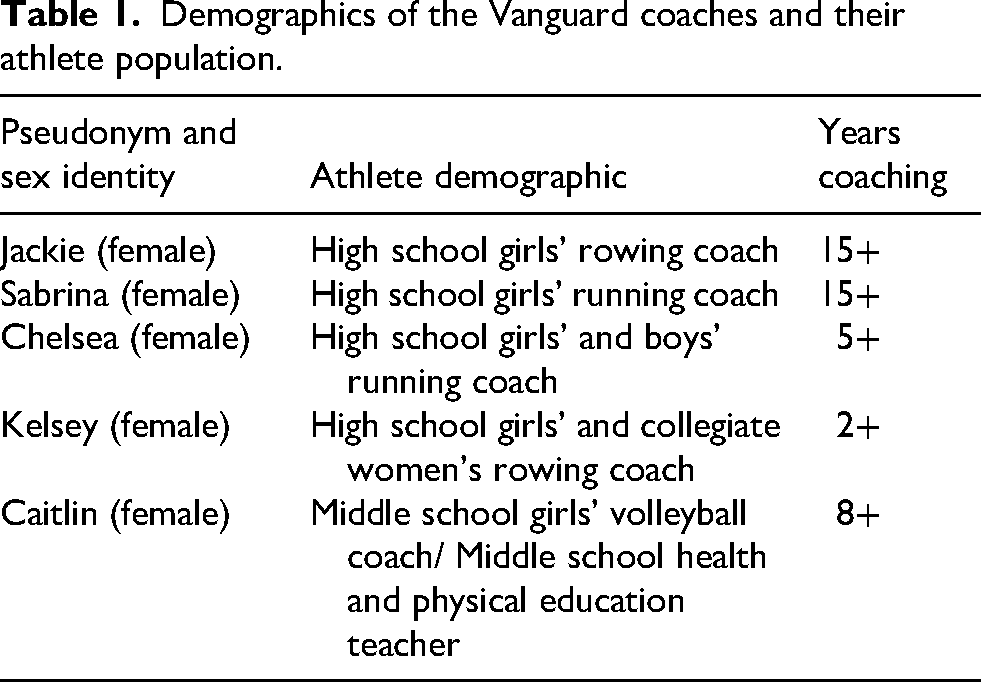
The Vanguard coaches stood apart in this study as they were the only participants to report applying their learning in practice during the intervention. Additionally, these coaches were the only participants to volunteer to interview and discuss their experiences. See Table 1 for Vanguard coach demographics.
Demographics of the Vanguard coaches and their athlete population.
Three themes emerged within the Vanguard coaches’ surveys and interviews: (1) These coaches all made sense of the intervention through former lived experiences—and challenges—with menstrual health as female athletes, (2) these coaches were all driven by concern for the holistic health and well-being of their athletes, and (3) these coaches viewed sensemaking around menstrual health as a process of development.
Theme 1: Contextualized the learning within lived experience
The Vanguard coaches all made sense of this intervention through their former experiences—and challenges—with menstrual health as female athletes. They shared about confusion, frustration, and/or physical and psychological distress they experienced as a result of being uninformed about menstrual health when they were athletes. Here, Coach Jackie expressed frustration that her doctors and coaches never taught her “what regular menstruation looked like” when she was a rower: No one taught me about this. Doctors… coaches… they never talked about it. No education on menstruation or what regular menstruation looked like. When I went through an eating disorder, I had no idea. And when I was doing lightweight rowing, I had no idea of the problems, of what was happening to my body as a result of those…you know…that time period. In high school, I had lost my menstrual cycle for a year or two. And at the time it really wasn’t … it was like … oh, well, you know, your body is trying to learn its routine. I wasn't aware. I didn't know. I just thought my injuries were because I pushed myself so hard. I had some shin splints that got so bad. We went into the doctors. I had stress fractures in both of my legs. I lost my junior year of cross country because of my stress fractures. And so even today that's hurtful.
Chelsea's mention of “these things” was in reference to eating disorders, stress fractures, and overuse injuries, all of which she said were common on her team. Yet, Chelsea had not understood the connections between menstrual health, bone health, and nutrition. Here, Chelsea shared how she began seeking answers at the end of her running career to better understand the root of her and her teammates’ health problems: I just kind of sought out a lot of answers on my own to figure out what was happening. Like, why was I getting stress fractures? And why my teammates had eating disorders. And like, what was the right way to eat? So, I just kind of started like listening to podcasts and finding answers on my own. I remember distinctly, one of my coaches actually talked to us about it. And she shared a podcast from the US women's soccer team where an athlete was under fueling, and then ended up like breaking a bone or something. And she spoke to us about it. And I think at the time I didn't realize how important that was.
Theme 2: Sensemaking driven by concern for athlete health and well-being
The Vanguard coaches were all grounded in concern for the holistic health and well-being of their athletes, which motivated them to work through the challenges and discomfort associated with discussing the menstrual cycle. For example, Coach Sabrina was clear that she was not yet comfortable discussing menstrual health with her athletes (e.g., “I was nervous and they could tell that I was nervous”). Yet, she was determined to develop strategies to manage her discomfort (e.g., “I have to practice. I have to have my script. I want to become more comfortable”). When I asked Coach Sabrina why she wanted to become more comfortable discussing menstrual health, she responded that her athletes “need to know” about their bodies: “The athletes, they need to know their body. They need to know eating properly, sleeping … everything that affects them”.
Coach Jackie shared that she wanted her athletes to “feel knowledgeable so they can feel powerful”. Here, she connected her concern for her athletes’ well-being with her beliefs around her role as a coach: My role is to provide them with the information so that they can feel more powerful in their own bodies. I want them to feel knowledgeable so that they could feel powerful. If I coached males, and I found out there was something in their health profile that I needed to tell them so that they could have some agency and awareness, I would 100% teach that. Give them the information. This is about giving the athletes power, knowledge, agency over all of this. I've really worked hard to create a good support system for my athletes. We have a registered dietitian. There's a runner that comes and talks to our team every year. So they hear the same presentation every year. But they need to hear it every single time.
Theme 3: Knowledge and comfort develops over time
The Vanguard coaches agreed that gaining knowledge and comfort in discussing menstrual health was a process of development for them and for their athletes. For example, Coach Jackie shared her learning that developing coach-athlete trust was essential before discussing the menstrual cycle: I learned that this is not the topic I'm bringing out in week one. I need to build trust with the athletes. I need to feel that I have enough social capital with whoever I'm coaching. And they need to know that I am coming from a place of compassionate concern. They need to know I care first. I learned that it can’t just be one time, like, here's the information, and then never talk about it again. It's better if it's smaller doses of information shared more frequently. The more we can get other people to talk about it rather than just one person on the staff it's helpful, because then the girls start talking about it. I really feel for male colleagues, because there's this fear that you'll be seen as creepy, or invasive, or meddling too much with female athletes. As teachers and coaches, it's kind of drilled into you, like, don't overstep your boundaries. You’ve got to be really careful. And I think for male colleagues especially, there can be a fear that they will be considered crossing a boundary if they talk about menstruation. It's the small things I learned, like just opening channels of communication so they can express a little bit about how they're feeling. Or when you're going to an away game, tell them where the bathrooms are going to be, or when the bathroom breaks will be. Really simple stuff that's not that hard.
Discussion
This study examined how coaches responded to an educational intervention on supporting female athlete health and performance, including their concerns about applying the learning by discussing menstrual health with athletes. Findings revealed that coaches face several barriers to translating female athlete education into practice, including: (1) misperceptions about athletes’ needs and experiences related to the MC, (2) questions about how (or if) MC-related concerns apply to athletes in their sport, and (3) concerns about how to navigate menstrual health conversations with athletes. Findings also revealed that female coaches (i.e., those with lived experience with the menstrual cycle) were more likely to implement menstrual health awareness in their coaching, as they were able to relate to the concerns and experiences female athletes had related to the menstrual cycle in sport.
Narrowing coach-athlete perception gaps
The Core Group's sense of surprise that MC symptom management is a primary concern for female athletes highlights a disconnect between the concerns of athletes and the awareness that coaches have of those concerns. Perception gaps between coaches and athletes, in fact, are common in sport. 68 These gaps strain coach-athlete relationships, as they create a divide between athletes’ needs and experiences and coaches’ perceptions and behaviors. 69 Indeed, Höök et al. 28 found that coach-athlete perception gaps around the MC “hinder” female athletes’ experiences in sport, and thus need attention in coach education. One example of the behaviors of coaches misaligning with the needs of athletes has been noted in elite sport settings, where coaches often collect athletes’ MC-tracking data while failing to communicate with athletes about how, or if, that data will be used to adapt training.70,71 This practice fails to acknowledge athletes’ needs, including their desire for increased access to education about menstrual health and symptom management,16,67,15 support from coaches,20,21,22,29 and team environments where athletes feel safe to openly discuss and functionally address-related symptoms and concerns.24,18
The need to contextualize physiology learning
In addition to their surprise, the Core Group coaches also questioned the relevance of menstrual health in their context—e.g., “I wonder if this is a problem for athletes in my sport”. This finding suggests that coaches need opportunities to contextualize their learning to consider how the science of female physiology applies to their sport and athlete demographic. Contextualization can be supported by pairing physiology content with athlete stories, narratives, and case studies within varying sport contexts, as use of case studies has been shown to facilitate learning application. 72 This need for learners to connect science learning to human stories was noted by Roux et al. 73 who found that teachers, nurses, and students found a school-based menstrual health intervention to be overly scientific and thus unrelatable and of limited value. Inviting learners to contextualize their learning also heightens attention and engagement, as learners feel they are part of the learning experience.74,75
In contrast to the Core Group, the Vanguard coaches contextualized the intervention's content within their lived experiences as female athletes. By connecting to their “lived expertise”, 76 the Vanguard coaches were able to relate to the concerns and experiences of their female athletes, and, importantly, to apply their learning in ways that fit the unique needs of their athlete population. For example, Coach Caitlin discussed how, for athletes in early adolescence, “the small things” coaches do make a big difference, such as ensuring athletes know the bathroom locations during away games and field trips and keeping “open channels of communication” so girls feel safe seeking help when struggling with MC symptoms. Coach Chelsea, on the other hand, applied the content in the context of competitive high school running, where athletes face the body-related pressure of achieving an optimal power-to-weight ratio. In her coaching context, Chelsea felt that athletes needed to hear the voices of outside experts such as nutritionists and fellow female athletes who were navigating similar performance pressures.
Social norms as barriers to implementation: mitigating the threat response
The Core Group coaches expressed reluctance to discuss the MC with athletes due to concerns about violating gender roles, social norms, or exceeding the scope of their leadership responsibility. Male coaches in particular shared concerns that violating gender norms might negatively impact coach-athlete relations—e.g., “I don’t want my athletes to have a changed perspective of me”. Even female coaches expressed concern for their male coach colleagues, indicating that male coaches may be viewed as “creepy” for discussing menstrual health. These findings align with those of Höök et al. 28 who found that male coaches feel that discussing the MC is outside their comfort zone.
Combined, these findings suggest that coaches may be experiencing a threat response in the brain as they consider discussing the MC, which is recognized as a universally taboo topic. 77 This is of crucial significance when considering female athlete coach education, because a threat response will impair executive function in the brain, and thus impact coaches’ willingness to engage and their capacity to learn. 78 In fact, even perceived social disconnection (e.g., through violating gender norms) can impair executive function and evoke behaviors of avoidance. 79 In this study, for example, no male coaches reported having discussed menstrual health with female athletes. These findings suggest that male coaches may need unique support to translate female athlete education into their coaching, as their lack of lived experience with the menstrual cycle may heighten feelings of social disconnection. 30
For both male and female coaches, mitigating any threat response and establishing a sense of psychological safety is an essential first step to engaging coaches in learning about menstrual health.80,81 One step toward establishing psychological safety with learners is for educators to explicitly name—and thus begin to normalize—the discomfort associated with the menstrual cycle. This technique, known as “affect labeling”, 82 can reduce the intensity of unpleasant emotions, support emotion regulation, and help coaches feel less alone in their emotions. 83
Sensemaking as a process of development
The Vanguard coaches’ experiences illustrate how developing knowledge and comfort discussing the MC is a process, even for female coaches. The Vanguard coaches were not immune to the social discomfort associated with discussing the MC (“I was nervous and they could tell that I was nervous”). However, by connecting to their former lived experiences as athletes, the Vanguard coaches felt anchored in concern for the well-being of their athletes (“This is about giving the athletes power, knowledge, agency over all of this”). Though male coaches will not have personal lived experience to support their sensemaking around menstrual health in sport, coach educators can support male coaches in contextualizing the learning by pairing physiology content with athletes’ stories and case studies. 84 Additionally, male coaches in particular may benefit from hearing the voices of fellow male coaches who have implemented menstrual health awareness into their work with female athletes. Seeing and hearing fellow coaches may support male coaches in feeling less alone in this work.
Implications for practice: coaches’ need for translational support
A key takeaway from this study is that coaches need support to translate female physiology learning into practice. This finding is well documented in adult learning literature, which emphasizes that learners require ongoing support to overcome barriers to change and to sustain the difficult work of transferring new learning into practice.84,85,86,87 What is becoming increasingly clear is that the support needs of coaches exist on multiple levels. Several studies, for example, illustrated that coaches want guidance on how to communicate with athletes about the MC.18,22,24,25,28,29 Perhaps the more difficult problem to address is coaches’ need for higher-level support6,7,20 to navigate scope-of-practice concerns (“I’m concerned about pushback” and, “You’ve got to be really careful”). Clarke et al. 25 also found that coaches desire policy-level support to know the scope of their roles and guidance to determine how and when to refer athletes to specialized care.
Limitations and future work
This study had important limitations. First, the intervention was offered over a short period of time (two weeks); given the social stigma associated with the MC, most coaches will need a longer period of time to process content, develop comfort, and envision how to apply their learning within their coaching context. Additionally, this intervention having been hosted by a female coach/educator may have influenced coaches’ experiences with the learning either positively or negatively. Efforts were made to address this limitation by including a male coach's voice and experiences in the intervention's curriculum; however, male coaches may need opportunities to process and discuss menstrual health learning with peers who share challenges and experiences similar to their own.
Future work is needed to understand not only how to increase coaches’ knowledge about female physiology, but also how to strengthen their comfort and skill in translating their learning in ways that align with the needs of their athletes. Looking ahead, it is important to acknowledge that most American sport coaches lack any sort of coach education 88 ; thus, coaches may need foundational training in order to fully benefit from female physiology education. For example, given the concerns coaches have about discussing the menstrual cycle, precursory coach training in healthy communication and cultivation of trust with athletes may be necessary for coaches to feel prepared to discuss menstrual health with athletes. In fact, all five of the Vanguard coaches reported having participated in foundational coach or teacher education, which likely supported their comfort in applying the intervention's learning in their coaching. Coach Jackie, for example, shared that she needed to “build trust with the athletes” before discussing the MC. Indeed, recent studies agree that coach-athlete trust is essential for coaches and athletes to feel safe discussing menstrual health and, crucially, to support participation of women and girls in sport.30,89
Conclusion
Coaches serve a crucial role in supporting the health and performance of female athletes. This study provided evidence that coaches’ sensemaking around implementing female-specific health awareness in sport is a process that can be developed. Coach education must go beyond simply supplying coaches with the science of female athlete physiology—coaches also need support in navigating concerns around social norms, gender roles, and scope of practice. Additionally, coach education must be designed with awareness of the vast variation in individuals’ lived experiences with the menstrual cycle; it is expected that coaches who have not lived with the MC may need additional time and support to gain familiarity and comfort with female physiology content. Finally, this study benefitted from a co-constructivist research approach: Coaches both with and without lived experience with the MC offered valuable insight into coaches’ learning and support needs as they translate female athlete physiology learning into practice.
Footnotes
Acknowledgements
Thank you to the coaches who made this work possible by participating in this study. Additionally, thank you to the University of Washington Center for Leadership in Athletics for funding this research; to my doctoral committee for your feedback and support; and to this paper's reviewers for your constructive feedback that strengthened this work.
Ethical considerations
This study was approved by the University of Washington Human Subjects Division: STUDY00019697/ MOD00020307. No AI-assisted technologies were used in the composition of this manuscript.
Consent to participate
Informed consent was collected from study participants electronically via Qualtrics software in Part 1 of this intervention prior to all data collection.
Consent for publication
Not applicable.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the University of Washington Center for Leadership in Athletics.
Declaration of conflicting interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability
Due to informed consent protocols and participant anonymity concerns raw data cannot be made available.
Appendix A: Educational Intervention Design and Curriculum
Appendix B: Open-Ended Survey Questions
Appendix C: Sample Interviews Questions