
Abstract
Despite growing participation of young females in Australian football (AF), literature on concussion knowledge (CK), attitudes (CA), and reporting intentions (CRI) has focused on male athletes and adult populations. Understanding how female AF athletes perceive concussion risk, their willingness to report symptoms, and their knowledge about concussion, is essential for designing targeted injury prevention and education initiatives. This cross-sectional survey study utilised the Rosenbaum Concussion Knowledge and Attitude Survey Student version (RoCKAS-ST) to examine the CK, CA, and CRI of female AF players. Descriptive statistics, multiple one-way ANOVA, and multiple regression analyses were utilised to profile survey results, examine competition level differences, and explore associations between athlete / demographic variables and survey domains (CK, CA, and CRI). Overall, 132 Tier 3 (highly trained) female AF players from two youth and one open-age (OA) team/s on the eastern coast of Australia participated in the study. Mean scores for CK and CA increased by competition level, CK; Under-16 (U16) 18.66 ± 2.29, 95% CI [17.87–19.44], Under-19 (U19) 19.08 ± 2.12, 95% CI [18.47–19.69], OA 20.06 ± 1.83, 95% CI [19.53–20.59] and CA; U16 59.26 ± 7.20, 95% CI [56.78–61.73], U19 62.12 ± 7.42, 95% CI [59.99–64.26], OA 65.94 ± 5.50, 95% CI [64.34–67.53]. Significant differences in CK, CA, and CRI scores were observed between the U16 and OA cohorts (p < 0.05). Differences were also observed in the U19 and OA CA scores and the U16 and U19 CRI scores (p < 0.05). Across all competition levels combined, CA was strongly related to CRI (r(132) = .557, p < 0.001), however, there was no significant relationship between CK and CRI. Multiple regression analysis revealed age was significantly and positively associated with CK and CA scores in female AF players (β = 0.31, p < 0.01) and in the presence of CK, age, and other demographic variables, CA had a strong association with CRI (R 2 = 0.386, p < 0.001). Future research should explore potential barriers to SRC reporting using robust methods of CRI evaluation, explore competition level differences in RoCKAS-ST domain across a broader range of AF competitions, further explore variables that may influence CA and CRI, and determine if targeted CA initiatives post-SRC in female AF players are effective.
Introduction
In the last two decades, participation in contact and collision sports (CCS) among female athletes has grown considerably.1–3 Australian football (AF) is one of many CCS that has seen a marked rise in female participants, witnessing a staggering 790% growth in female participation in the past decade. 4 As a result, organised competitions and development pathways have expanded rapidly, particularly since the inception of the Australian Football League Women's (AFLW) competition in 2017.5–7 While this growth has provided expanding opportunities for female athletes to participate from grass-roots to the national level of AF, it has also brought increased exposure to injuries commonly associated with CCS such as sport-related concussion (SRC).7,8
At the 2022 International Conference on Concussion in Sport, SRC was defined as, “a traumatic brain injury caused by a direct blow to the head, neck or body resulting in an impulsive force being transmitted to the brain that occurs in sports and exercise-related activities.” 9 (p697) Over the last decade, SRC has gained growing attention in the fields of sport science and medicine due to its potential short- and long-term health consequences.10,11 Timely and appropriate reporting of SRC symptoms has been identified as a critical component for effective management and recovery of SRC. 12 However, underreporting remains a concern, especially in youth athletes, where players may lack knowledge to recognise SRC symptoms or may downplay or conceal injuries due to social, consequential, or competitive pressures. 13
Despite growing participation of young females in AF, literature on concussion knowledge (CK), concussion attitudes (CA), and concussion reporting intentions (CRI) has focused on male athletes or adult populations.14,15 This gap in research is particularly concerning given that established research demonstrates female athletes experience different SRC outcomes compared to their male counterparts, 16 and that recovery from SRC may be longer for youth athletes than adults. 17 Understanding how female athletes, and moreover female youth athletes, perceive SRC risk, their willingness to report symptoms, and their level of CK, is therefore essential for designing targeted, sex- and age-appropriate injury prevention and education initiatives.
Further to this, identifying factors associated with CK, CA, and CRI plays a pivotal role in assisting researchers in their efforts to design targeted SRC initiatives that specifically address the needs of unique cohorts. 18 A systematic review published in 2022 revealed there were no known studies that have explored factors associated with CK, CA, and CRI in AF athletes. 18 Exploration into factors associated with individual demographic and athlete profile variables and SRC domain outcomes in AF athletes is warranted to inform developments in SRC prevention and education, and guide future research in this area.
Therefore, the primary aims of this study were to: (i) profile CK, CA, and CRI of female AF players across three competition levels, (ii) evaluate competition level differences in these SRC domains, and (iii) analyse the overall relationships between these SRC domains. The secondary aims of this study were to explore: (iv) associations between demographic / athletic profile variables on CK, CA and CRI, and (v) associations between CK, CA and CRI.
Through exploration of CK, CA, and CRI, this research seeks to inform the development of evidence-based strategies to improve SRC safety and health outcomes for female athletes in AF and similar CCS.
Methods
Setting and study design
Utilising an observational cross-sectional survey study design, CK, CA, and CRI were investigated administering the Rosenbaum Concussion Knowledge and Attitude Survey Student version (RoCKAS-ST) 19 amongst Tier 3 (highly trained) Under 16 years (U16) and Under 19 years (U19) youth female AF players and Tier 3 (highly trained) open-age (OA) female AF players during the 2025 season. Classification of competition level was informed utilising the definition of training and performance calibre outlined by McKay et al. 20 This study was conducted in accordance with the ethical approval granted by Bond University Human Research Ethics Committee (LE00041) and the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelines were utilised to guide the reporting of study methods and results. 21
Recruitment and study participants
Two Tier 3 youth female AF programs and one Tier 3 OA women's AF club on the eastern coast of Australia were approached prior to the 2025 pre-season to participate in the study. All three programs / clubs agreed to participate. Parents of youth players and players from each program / club were invited to attend an information session during the 2025 pre-season and were provided with a participant information package prior to obtaining consent. The participant information package described the study objectives, outcome measures, potential risks and benefits, and information relating to confidentiality and consent. To be eligible for the study, participants were required to meet the following inclusion criteria: be an active player in a Tier 3 youth female AF program or Tier 3 OA female AF club throughout the 2025 season and be 13 years or older. Participants were excluded if they had any injury at the time of data collection that impacted their ability to participate in the study.
Procedures & outcome measures
Participants that provided consent to participate were invited to complete a paper-based version of the RoCKAS-ST survey during the 2025 pre-season. Surveys were administered under the direction and supervision of a trained research team member. Participants were instructed to complete the survey in silence, without input from peers or electronic sources. Participants were permitted to ask the supervising research member questions if required. Only context was provided where necessary; no information pertaining to CK or advice towards CA were provided. Completed surveys were collected by the research team and securely stored prior to manual input of results and scanned copies of original surveys were linked to a unique identifier code (UIC) for each participant and uploaded to a secure data store.
The RoCKAS-ST is comprised of five sections to capture CK, CA, and CRI. 19 Three sections assess CK and consist of 17 true or false statements, and a symptom recognition list (16 symptoms are listed; eight are legitimate SRC symptoms and eight are distractor symptoms). 19 In total, CK is tallied out of 25 (0–25 as a possible score); higher scores indicating higher SRC knowledge. Two sections contain 15 statements and scenarios to assess CA scored on a Likert scale (1 = strongly disagree and 5 = strongly agree). 19 The CA section was tallied out of 15 statements and scenarios (15–75 as a possible score), higher scores indicating safer attitudes toward SRC. As has been employed in previous studies, a single question in the CA section (question 3.1) was used to measure CRI: “I would continue playing a sport while also having a headache that resulted from a minor concussion”.19,22,23 A lower Likert scale score (1 = strongly disagree, 2 = disagree) indicated a higher and therefore ‘safer’ CRI score of ‘5’ and ‘4’ respectively. Whereas a higher Likert scale score (4 = agree, 5 = strongly agree) indicated a lower and therefore ‘unsafe’ CRI score of ‘2’ and ‘1’ respectively. An additional three validity scale questions and 12 distractor questions (not tallied in the final score) make up the 55-item survey. 19 Where necessary throughout the RoCKAS-ST, modifications were made to align with suitable vocabulary for an Australian context.
In addition, demographic / athlete profile variables were collected for each athlete, including: years of playing experience, preferred playing position, use of mouthguard when playing, use of headgear when playing, and participation in any previous SRC education programs. Participants that provided consent were provided a QR code to complete the online baseline demographic / athlete profile survey created and administered via Qualtrics (Qualtrics, Provo, UT) prior to the 2025 season commencing. This QR code was distributed to participants at the conclusion of information sessions, via email correspondence from participating programs / clubs, and via flyers during pre-season testing sessions. Participants were required to provide their names when completing the online baseline demographic / athlete profile survey to allow researchers to link exported results to participants assigned UIC and match to RoCKAS-ST data in a secure data store.
Further demographic / athlete profile variables were extracted from baseline Sport Concussion Assessment Tool 6 (SCAT6) completed during the pre-season, including: previous history of SRC (self-reported or diagnosed), previous diagnosis of attention deficit hyperactivity disorder (ADHD), previous diagnosis or treatment for headache or migraine disorders, previous diagnosis of a learning disability / dyslexia, previous diagnosis of depression, anxiety or other psychological disorder, previous hospitalisation for a head injury, and baseline SCAT6 symptomology score. 24 The baseline SCAT6 assessments were administered by trained physiotherapists or physiotherapy students, sports and exercise students, and athletic trainers under the supervision of a trained and accredited physiotherapist. The SCAT6 baseline screening assessments were completed according to the previously published protocol. 24
Statistical analysis
To analyse data collected, IBM SPSS Statistics software (version 28, Armonk, NY, IBM Corp.) was utilised, and the α value was defined at 0.05. 25 Survey validity was evaluated via participant responses to three validity scale questions; where scores of 0 or 1 were interpreted as invalid, and scores of 2 or 3 were interpreted as valid. 19 All participant surveys were deemed valid and therefore included in analysis.
Data analysis included descriptive statistics reported for demographic / athlete profile characteristics of participants, including the mean, standard deviation (SD), and range, or frequency and percentages. Descriptive statistics were also reported for CK, CA, and CRI for each playing level: U16, U19, and OA. Overall RoCKAS-ST and RoCKAS-ST domain results were presented as mean, SD, 95% confidence interval (CI), and range. Itemised results for each section of the RoCKAS-ST were presented as frequencies and percentages.
Multiple one-way ANOVA were performed to assess differences between competition levels (U16, U19, and OA) for RoCKAS-ST domains. Assumptions of normality and homogeneity of variances were evaluated prior to conducting the ANOVA. Normality of residuals was assessed visually using Q-Q plots and histograms. Homogeneity of variance was tested using Levene's test. Bonferroni post hoc tests were applied to determine pairwise differences.
Consistent with previously published criteria, ten outcome events (cases) per demographic / athletic profile variable were deemed necessary to conduct multivariate analyses.26,27 To satisfy this criterion, several post hoc variable groupings were implemented. Specifically, responses indicating; prior hospitalisation for head injury, diagnosis / treatment for headache disorders or migraine, diagnosis of ADHD, diagnosis of anxiety, depression or other psychological disorder, and diagnosis of a learning disability / dyslexia were combined into a single dichotomous predictor “previous medical history”. Likert responses associated with mouthguard use were grouped into ‘safe’ for answers ‘always’ and ‘most of the time’, and ‘unsafe’ for answers ‘never’, ‘rarely’, and ‘sometimes’ to the question “do you wear a mouthguard when playing in AF matches?”. Preferred playing positions were grouped together according to the three main areas of the AF field; ‘forward’, ‘midfield’, and ‘back’.
To explore relationships between RoCKAS-ST domains, associations between CK, CA, and CRI were evaluated via Pearson's correlation. Prior to analyses, all variables were tested for normality via visual inspection of histograms and Q-Q plots. Strength of association was interpreted as follows: |r| < 0.1 to < 0.3: weak correlation, 0.3 ≤ |r| < 0.5: moderate correlation, |r| ≥ 0.5: strong correlation. 28
Finally, multivariate regression analyses were performed to explore associations between demographic / athletic profile variables and RoCKAS-ST domains, and associations between CK, CA, and CRI, in female AF players combined. Prior to analysis, assumptions of linearity, independence, homoscedasticity, and normality of residuals were assessed. Multicollinearity was assessed by tolerance values greater than 0.1. Casewise Diagnostics were utilised to assess standardised residuals greater than ±3 SD. Normality of residuals was assessed visually using Q-Q plots and histograms. Unstandardised regression coefficients (B), regression coefficients (β), standard error of the coefficient, 95% CIs, R2 values, adjusted R2, and p values were reported. Percentage of variance uniquely associated with an independent variable was calculated by the first author utilising the squared semi-partial correlation (sr2) formula. 29
Analyses were based on a sample size of n = 132 for the ANOVAs, multiple regression, and Pearson's correlation tests for overall RoCKAS-ST results. To address missing data points in the secondary analysis of demographic / athletic profile variables, Little's missing completely at random (MCAR) test and a visual inspection of patterns of missing variables (PMV) was completed. 30 Visual inspection of PMV revealed no single missingness pattern exceeded 5% of cases. This was supported by Little's MCAR test which was non-significant, χ2(11) = 7.976, p = .715. Therefore, complete case analysis (listwise deletion), n = 106, was utilised for the multiple regression analyses of associations between demographic / athletic profile variables and RoCKAS-ST domains. For the ANOVAs, three groups were compared (U16, U19, and OA), and effect sizes (f) were calculated from the partial η2 values obtained. For multiple regression analyses, eight predictor variables were included, and effect sizes (f2) were calculated using the formula: f2 = R2 / (1 – R2) based on the observed R2 values and interpreted as follows: f2 = 0.02 equates to a small effect size, f2 = 0.15 equates to a medium effect size, and f2 = 0.35 equates to a large effect size. 28 For Pearson's correlations, effect sizes were based on the observed r values. All post hoc analyses were conducted using a two-tailed test and an α level of 0.05.
Results
Female AF players (n = 181) were invited to participate in the study. Of these, 133 were Tier 3 female youth AF players (U16 & U19) and 48 were Tier 3 female AF players (OA). In total, 132 players consented to participate; 35 U16 (55%) and 49 U19 (70%) players, and all 48 (100%) OA players completed the RoCKAS-ST survey. Participant demographic characteristics can be found in Table 1.
Summary of demographic / athlete profile characteristics for female Australian football players across three playing levels.
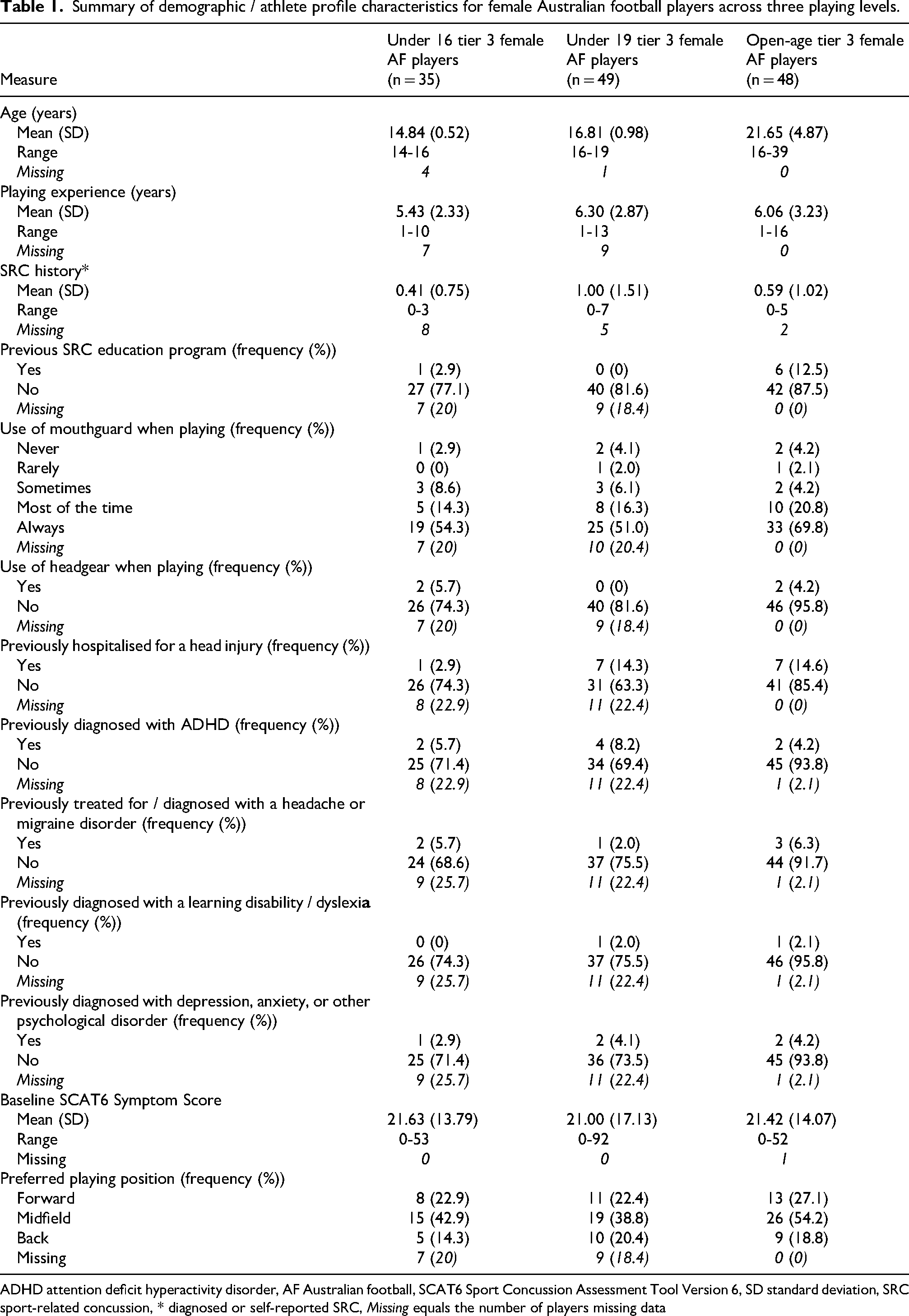
ADHD attention deficit hyperactivity disorder, AF Australian football, SCAT6 Sport Concussion Assessment Tool Version 6, SD standard deviation, SRC sport-related concussion, * diagnosed or self-reported SRC, Missing equals the number of players missing data
Overall RoCKAS-ST results
RoCKAS-ST results can be found in Table 2. Overall RoCKAS-ST scores were significantly different between competition levels (p < 0.001); U16 had the lowest RoCKAS-ST scores (77.91 ± 8.32, 95% CI [75.06 to 80.77]), and OA had the highest scores (86 ± 6, 95% CI [84.26 to 87.74]). Bonferroni post hoc analysis revealed differences in mean RoCKAS-ST scores were significant between U16 and OA (p < 0.001), and U19 and OA (p = 0.007), but were not significant between U16 and U19 (p = 0.124).
Rosenbaum Concussion Knowledge and Attitude Survey (student version) descriptive results and analysis of differences between three playing levels of female Australian football players.
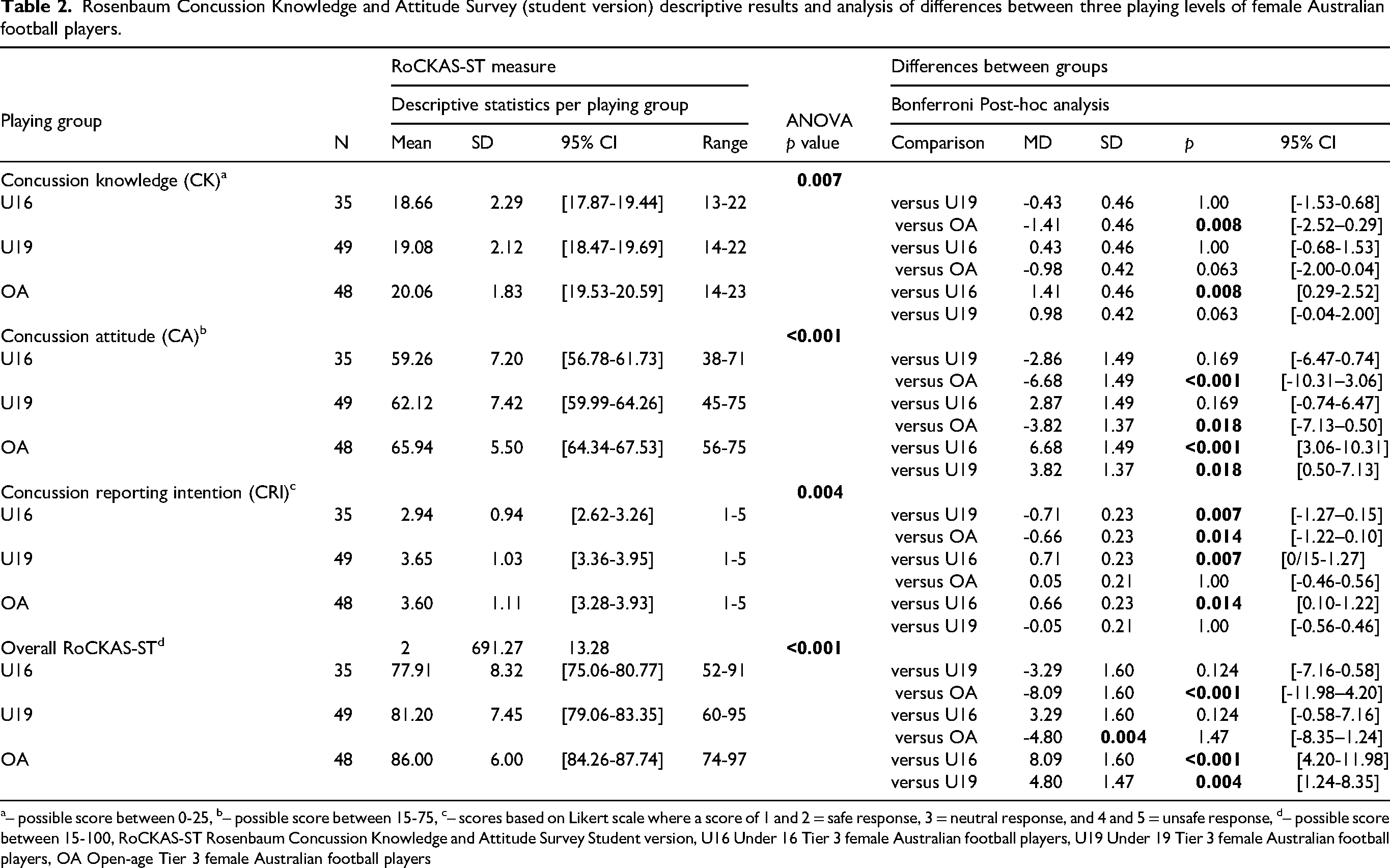
– possible score between 0-25, b– possible score between 15-75, c– scores based on Likert scale where a score of 1 and 2 = safe response, 3 = neutral response, and 4 and 5 = unsafe response, d– possible score between 15-100, RoCKAS-ST Rosenbaum Concussion Knowledge and Attitude Survey Student version, U16 Under 16 Tier 3 female Australian football players, U19 Under 19 Tier 3 female Australian football players, OA Open-age Tier 3 female Australian football players
In the true / false section of the CK evaluation, the most frequent correct responses were: Q5 – “In order to be diagnosed with a concussion, you have to be knocked out.” (false), and Q12 – “If you receive one concussion and have never had a concussion before, you will become less intelligent.” (false). Conversely, the most common incorrectly answered items included: Q17 – “An athlete who gets knocked out after a concussion is experiencing a coma,” (correct response ‘true’), and Q11 – “After a concussion, brain imaging (e.g., CAT scan, MRI, X-ray) typically shows visible physical damage (e.g., bruise, blood clot),” (correct response ‘false’) (Table 3).
Results for Rosenbaum Concussion Knowledge and Attitude Survey (student version) statements evaluating concussion knowledge across three playing levels of female Australian football players.
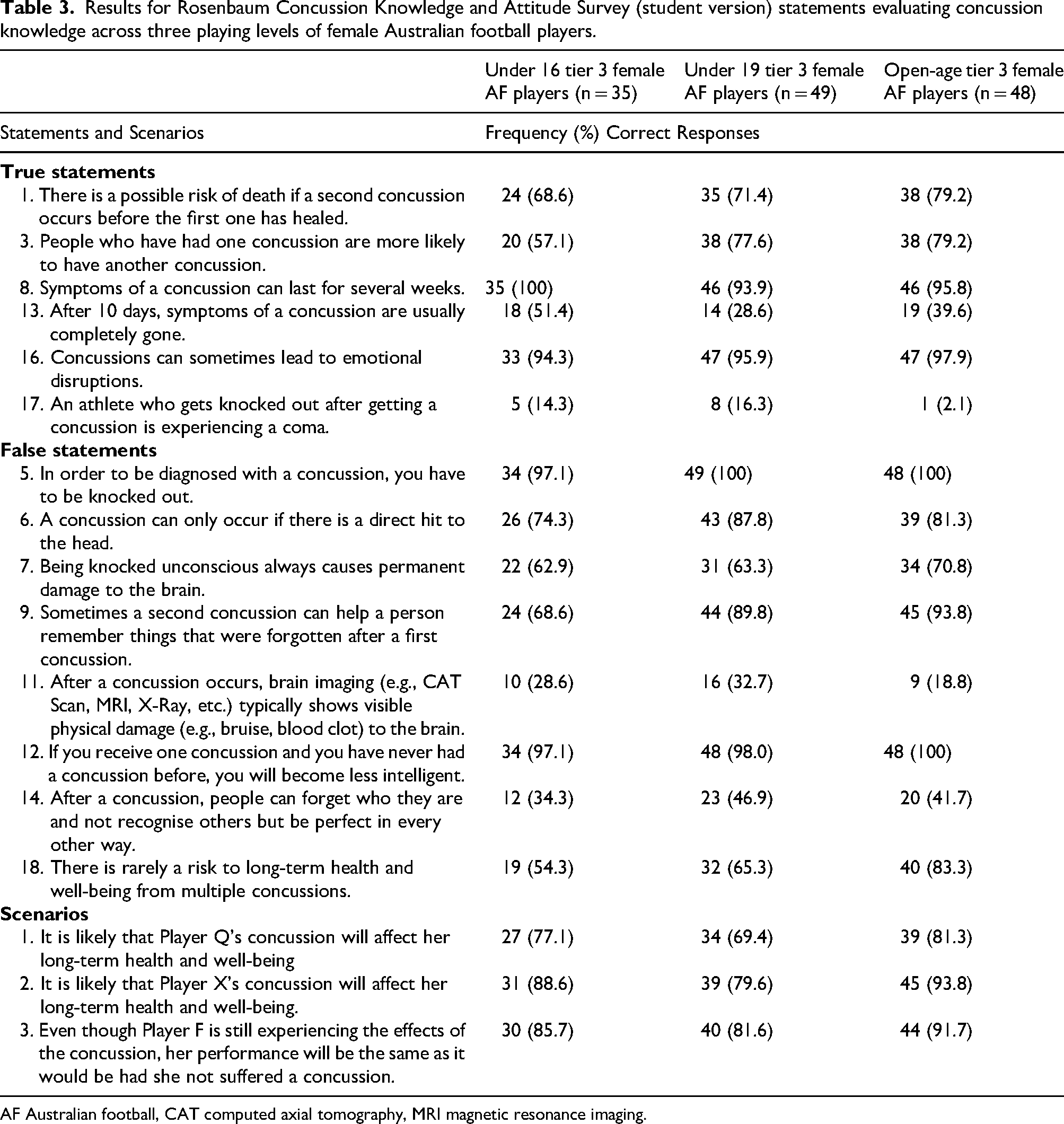
AF Australian football, CAT computed axial tomography, MRI magnetic resonance imaging.
In the symptom identification section, correct identification rates of legitimate SRC symptoms were high across all groups: 89% for both U16 and U19, and 95% for OA. “Headache” was universally identified as a concussion symptom by all participants. Other frequently recognised symptoms included “blurred vision” and “dizziness”. The most commonly selected distractor (i.e., incorrect) symptoms were “weakness of neck range of motion” and “sharp burning pain in the neck” (Table 4).
Results for Rosenbaum Concussion Knowledge and Attitude Survey (student version) concussion symptom identification evaluating concussion knowledge across three playing levels of female Australian football players.
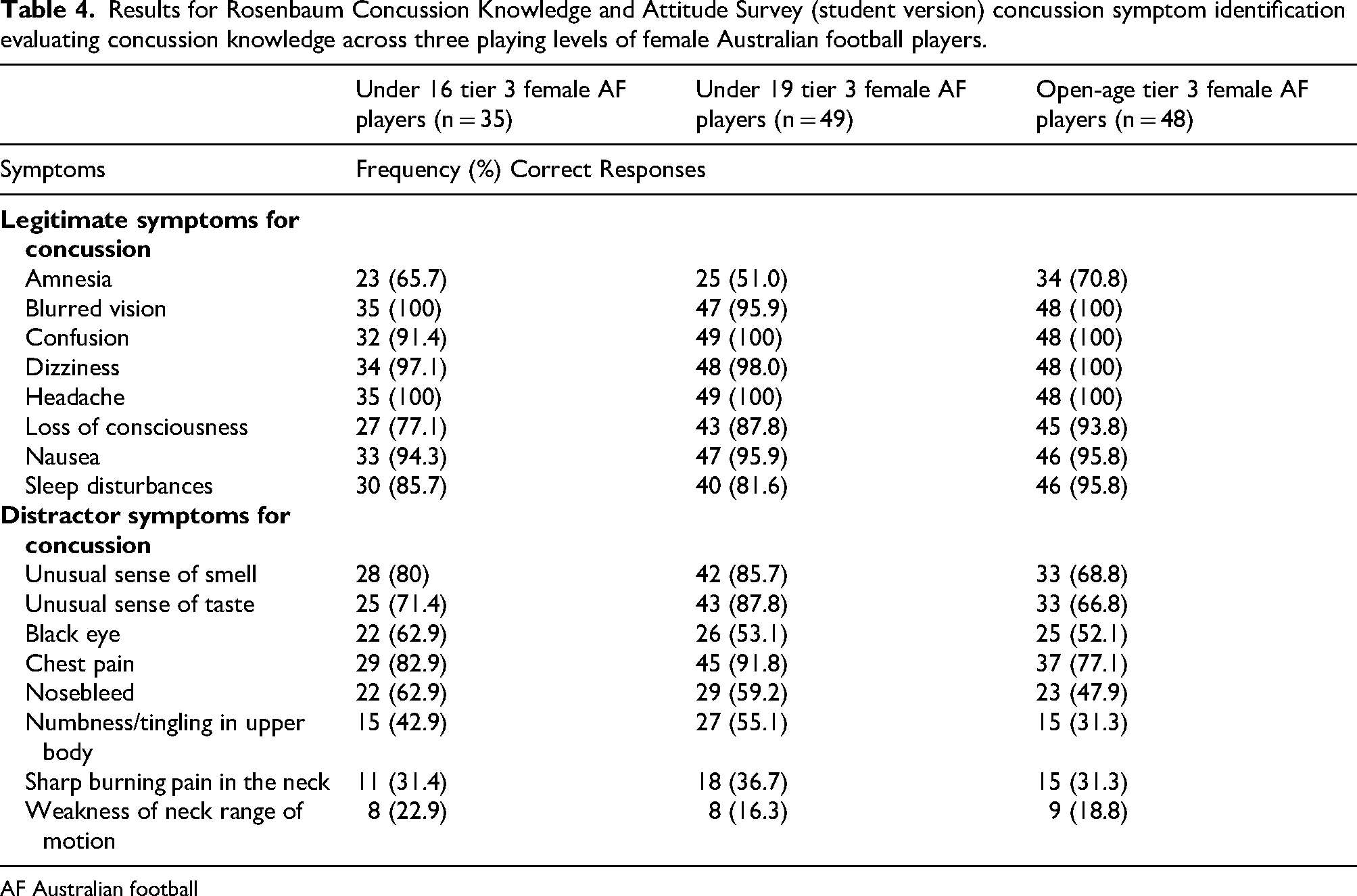
AF Australian football
In the CA statements and scenarios section, a high proportion of players indicated ‘safe’ responses to disclosing SRC symptoms to coaches despite knowing that disclosure will mean the athlete will miss a game (scenario 9) and coaches making decisions to keep athletes out of games when they have suffered a SRC (scenario 1). Conversely, there were fewer ‘safe’ responses towards the perceived attitude of other athletes (i.e., teammates) with relation to feeling that an athlete should disclose symptoms of SRC to a coach (scenario 10), and that an athlete should return to play after suffering an SRC during a semi-final game (scenario 6). Full CA results are detailed in Table 5. Regarding ‘unsafe’ responses to CRI, the U16 players demonstrated the highest frequency of ‘unsafe’ responses, followed by OA, and then U19 (Table 5).
Results for Rosenbaum Concussion Knowledge and Attitude Survey (student version) Statements and Scenarios Evaluating Concussion Attitude across three playing levels of female Australian football players.
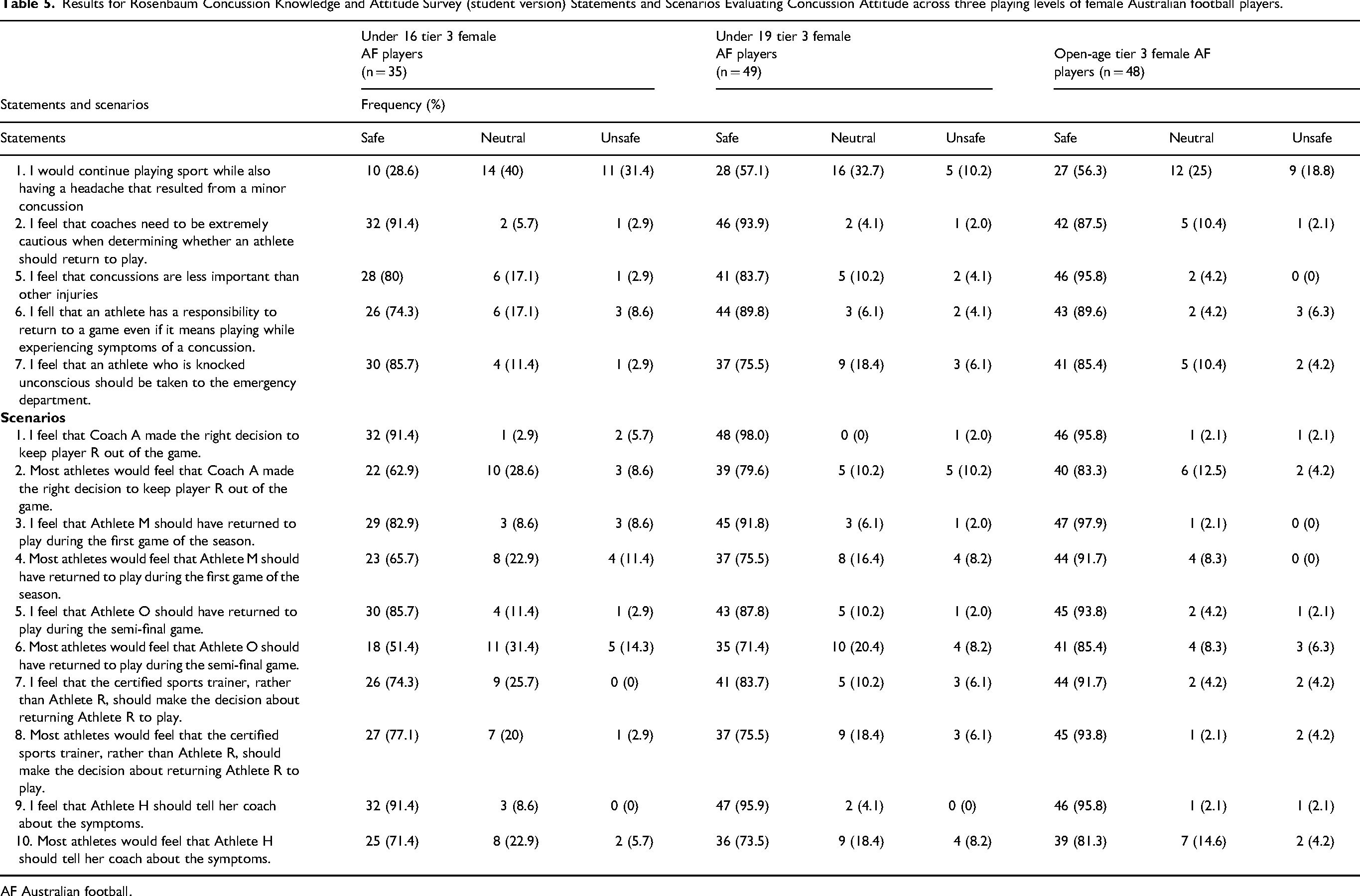
AF Australian football.
Relationships between RoCKAS-ST domains
There was a strong, significant relationship between CA and CRI, (r(132) = .557, p < 0.001, 95% CI [0.43 to 0.67]), and a weak, significant relationship between CK and CA (r(132) = .183, p = 0.035, 95% CI [0.01 to 0.34]). There was no significant relationship between CK and CRI (r(132) = .109, p = 0.211, 95% CI [-0.06 to 0.28]).
Competition level analysis of concussion knowledge (CK)
Mean CK scores increased by competition level, with U16 demonstrating the lowest CK level (Table 2). One-way ANOVA revealed a statistically significant difference in CK scores across competition levels, with Bonferroni post hoc demonstrating differences in CK scores existed between U16 and OA, but not between U16 and U19 or U19 and OA (Table 2).
Competition level analysis of concussion attitudes (CA)
Mean CA scores increased by competition level with U16 players demonstrating the lowest CA scores and OA the highest (Table 2). One-way ANOVA revealed a statistically significant difference in CA scores across competition levels and Bonferroni post hoc analysis revealed significant differences between U16 and OA, U19 and OA, but not between U16 and U19 players (Table 2).
Competition level analysis of concussion reporting intention (CRI)
Mean CRI scores increased from U16 to U19, but decreased between the U19 and the OA group. One-way ANOVA demonstrated CRI scores were significantly different between playing levels with Bonferroni post hoc analysis revealing significant increases in CRI score between U16 and OA, and between U16 and U19 players, but no significant differences in CRI score were noted between U19 and OA players (Table 2).
Associations between demographic / athlete profile variables and RoCKAS-ST domains
Multivariate regression analyses were performed to explore associations between demographic / athletic profile variables and RoCKAS-ST domains. The f2 value for the overall CK, CA, and CRI models were 0.215, 0.239, and 0.138, respectively; indicating medium effect size for the CK and CA models and small effect size for the CRI model. 28 Age, years of playing experience, history of SRC, use of mouthguard while playing, medical history associated with SRC, baseline SCAT6 symptom severity score, and preferred playing position were significantly associated with CK and CA; F(8,97) = 2.612, p = 0.012, and F(8,97) = 2.891, p = 0.006. However, the associations between the aforementioned variables and CRI was not significant; F(8,97) = 1.938, p = 0.116.
In the presence of all other demographic and player variables, age was significantly associated CK, CA, and CRI, whilst SRC history was significantly associated with CK and CA (Tables 6, 7, and 8). For every previous history of SRC recorded there was a 0.41 point increase in CK (p = 0.035, 95% CI [0.03 to 0.79]) (Table 6). Conversely, for every previous history of SRC recorded there was a 1.35 point decrease in CA (p = 0.047, 95% CI [-2.69 to −0.02]) (Table 7).
Association between demographic / player profile variables and concussion knowledge results in female Australian football players.
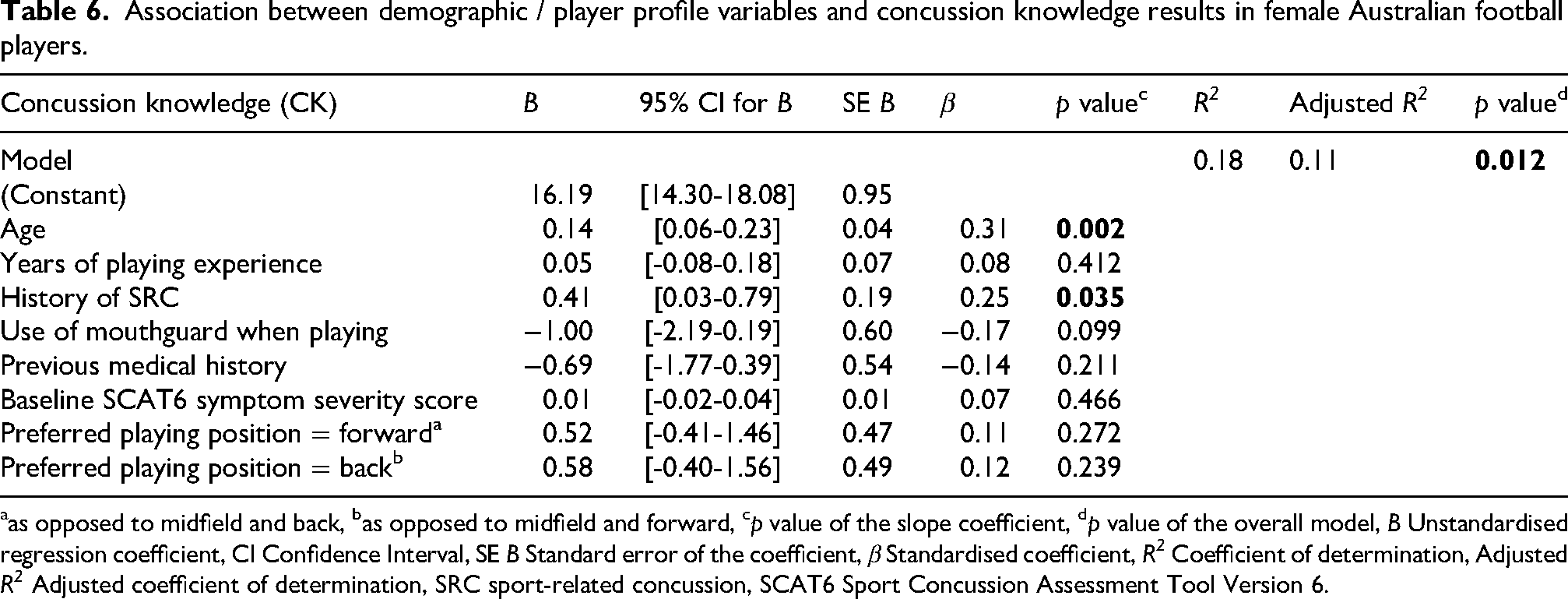
as opposed to midfield and back, bas opposed to midfield and forward, cp value of the slope coefficient, dp value of the overall model, B Unstandardised regression coefficient, CI Confidence Interval, SE B Standard error of the coefficient, β Standardised coefficient, R2 Coefficient of determination, Adjusted R2 Adjusted coefficient of determination, SRC sport-related concussion, SCAT6 Sport Concussion Assessment Tool Version 6.
Association between demographic / player profile variables and concussion attitude results in female Australian football players.
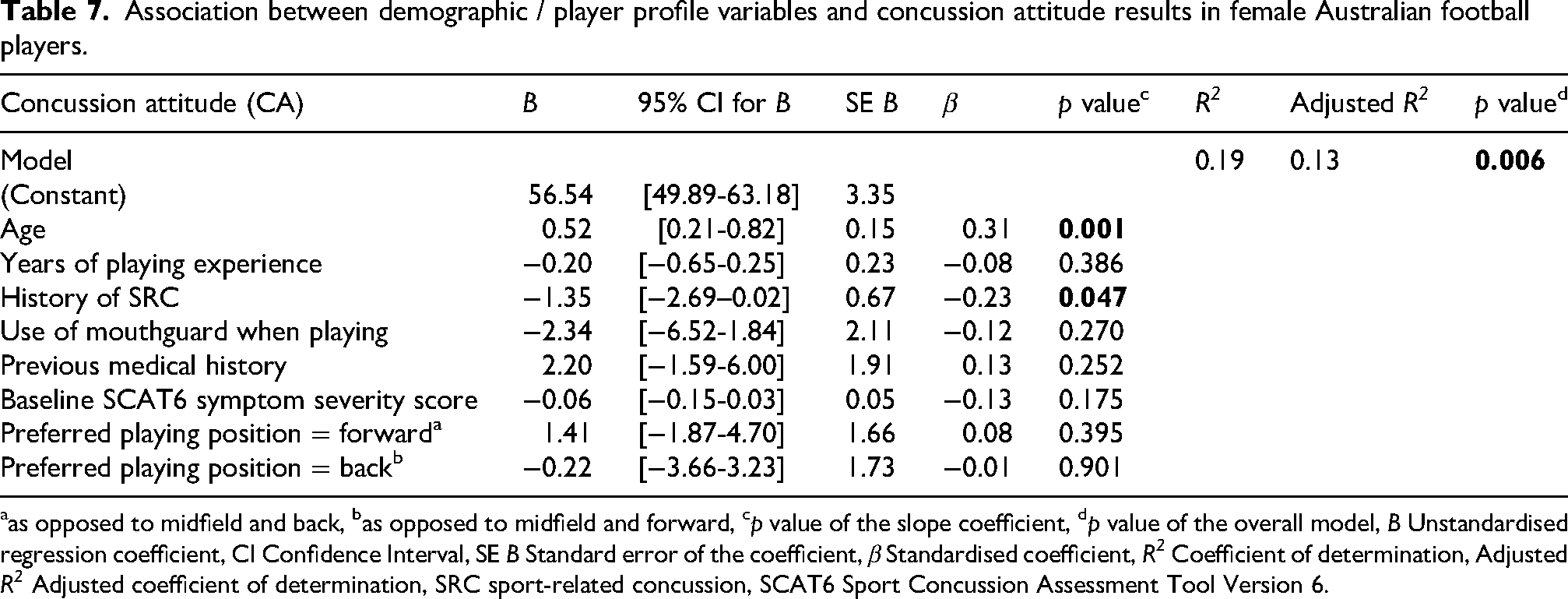
as opposed to midfield and back, bas opposed to midfield and forward, cp value of the slope coefficient, dp value of the overall model, B Unstandardised regression coefficient, CI Confidence Interval, SE B Standard error of the coefficient, β Standardised coefficient, R2 Coefficient of determination, Adjusted R2 Adjusted coefficient of determination, SRC sport-related concussion, SCAT6 Sport Concussion Assessment Tool Version 6.
Association between demographic / player profile variables and concussion reporting intention results in female Australian football players.
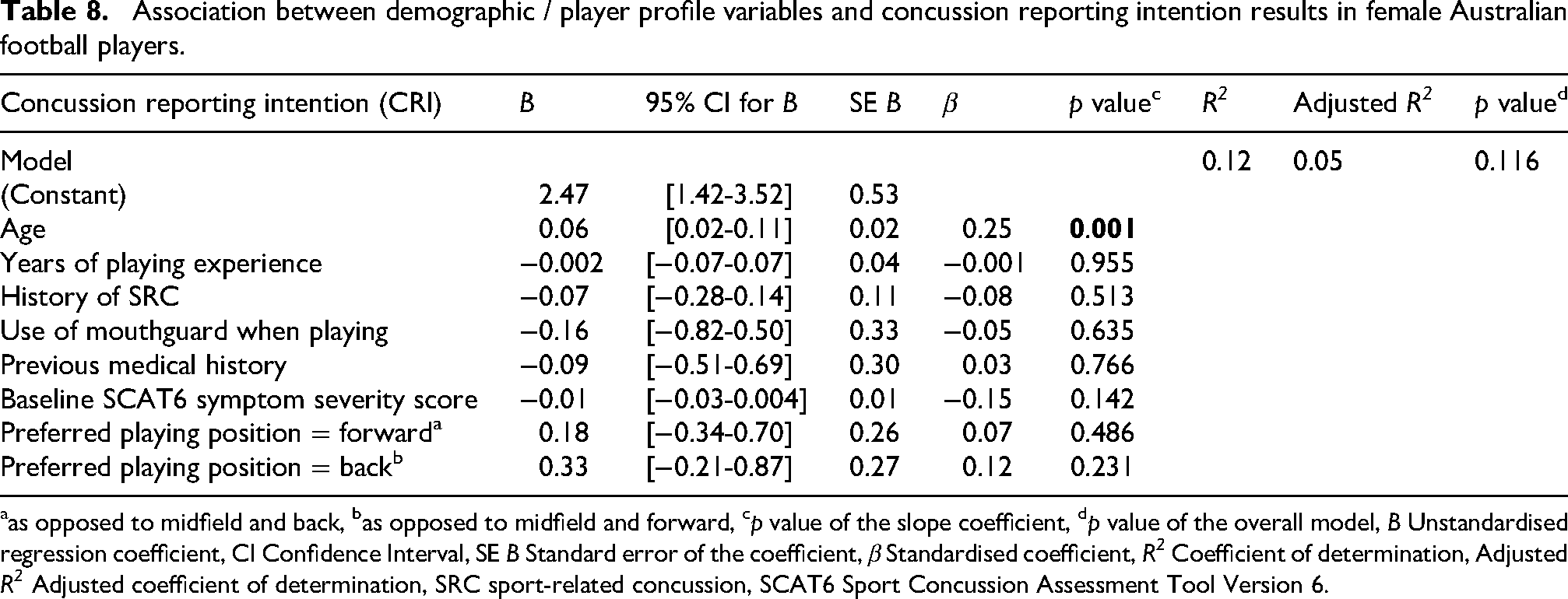
as opposed to midfield and back, bas opposed to midfield and forward, cp value of the slope coefficient, dp value of the overall model, B Unstandardised regression coefficient, CI Confidence Interval, SE B Standard error of the coefficient, β Standardised coefficient, R2 Coefficient of determination, Adjusted R2 Adjusted coefficient of determination, SRC sport-related concussion, SCAT6 Sport Concussion Assessment Tool Version 6.
Associations between RoCKAS-ST domains
Multivariate regression analysis was performed to explore associations between CK, CA, and CRI. The f2 value for the model was 0.672, indicating a large effect size. 28 The multivariate regression model revealed that in the presence of CK, CA was significantly associated with CRI scores (β = 0.556, p < 0.001) (Table 9) and when controlling for CK and athlete profile / demographic variables, CA uniquely accounted for 26% of the variance of CRI (Table 10).
Association between concussion knowledge and concussion attitude with concussion reporting intention results in female Australian football players.
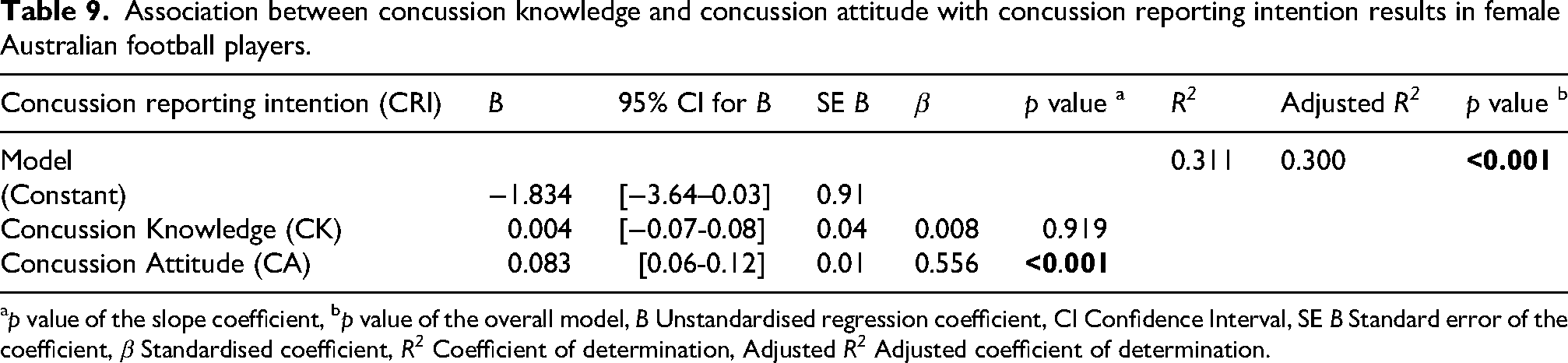
p value of the slope coefficient, bp value of the overall model, B Unstandardised regression coefficient, CI Confidence Interval, SE B Standard error of the coefficient, β Standardised coefficient, R2 Coefficient of determination, Adjusted R2 Adjusted coefficient of determination.
Association between concussion knowledge, concussion attitude, and athlete profile / demographic variables with concussion reporting intention results in female Australian football players.
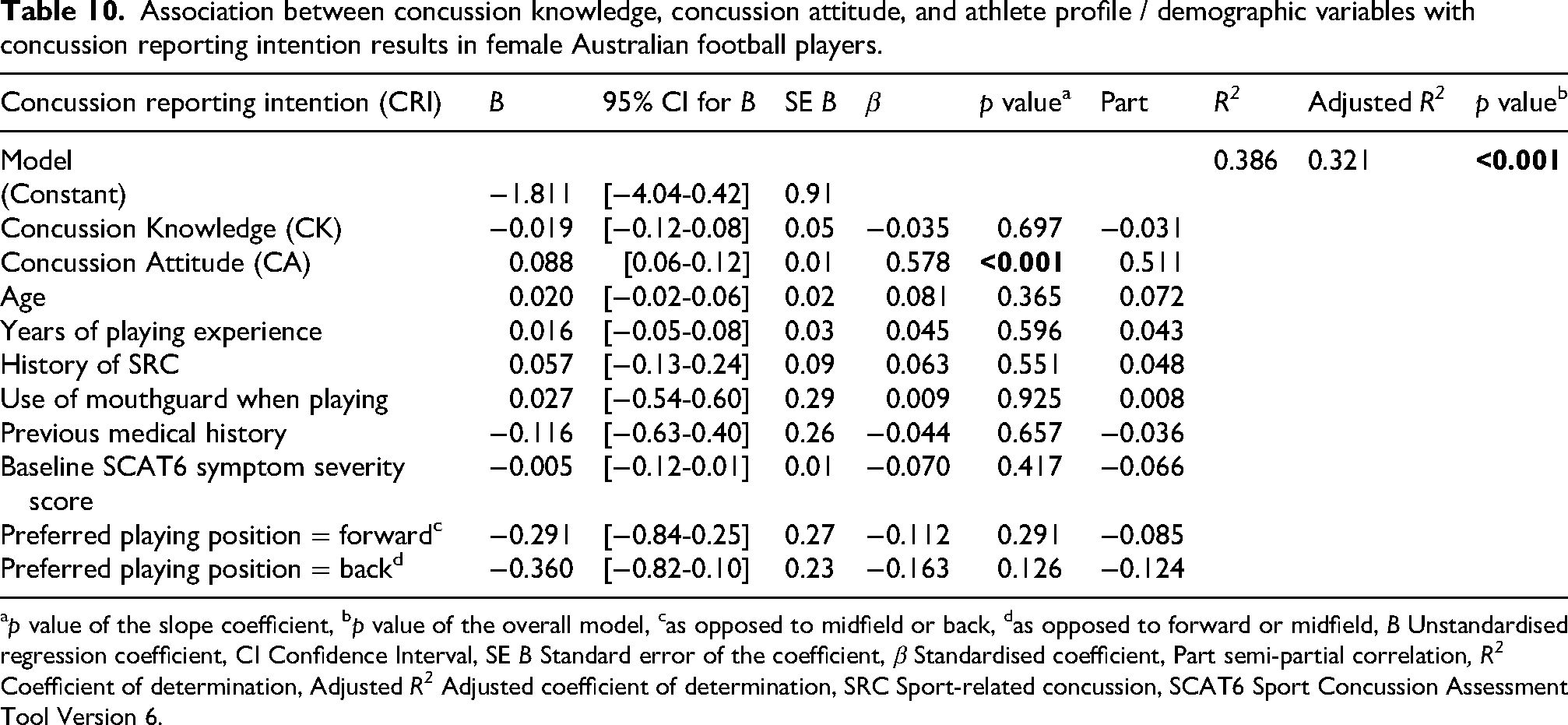
p value of the slope coefficient, bp value of the overall model, cas opposed to midfield or back, das opposed to forward or midfield, B Unstandardised regression coefficient, CI Confidence Interval, SE B Standard error of the coefficient, β Standardised coefficient, Part semi-partial correlation, R2 Coefficient of determination, Adjusted R2 Adjusted coefficient of determination, SRC Sport-related concussion, SCAT6 Sport Concussion Assessment Tool Version 6.
Discussion
The primary aims of this study were to: (i) profile concussion CK, CA, and CRI of female AF players across three competition levels, (ii) evaluate competition level differences in these SRC domains, and (iii) analyse the overall relationships between these SRC domains. The secondary aims were to explore: (iv) associations between demographic / athletic profile variables and CK, CA and CRI, and (v) associations between CK, CA and CRI.
This study is the first known to profile CK, CA, and CRI results for female AF players, therefore, providing a baseline for future research examining the RoCKAS-ST among female AF players. Whilst there were no comparative studies amongst female AF players, literature from other CCS examining female athletic cohorts were available for comparison. Findings from the U19 and OA groups, respectively, revealed similar mean CK (19.08 ± 2.12, and 20.06 ± 1.83) and CA (62.12 ± 7.42, and 65.94 ± 5.50) scores to community (CK 19.0 ± 2.2, CA 65.3 ± 5.3, age range 15–54 years), and ‘elite’ (national) (CK 20.53 ± 2.31, CA 63.28 ± 6.33, age not reported) female soccer players.31,32 Whereas, the U16 group appeared to have comparable mean CK (18.66 ± 2.29) and CA (59.26 ± 7.20) scores to female high school rugby union players (CK 18.9 ± 2.1, CA 60.2 ± 6.5, mean age 15.8 years). 22 Whilst reference data exists for a number CCS populations utilising the RoCKAS-ST, a universal normative index does not exist for the survey itself. Therefore, comparison simply provides a reference to demonstrate whether mean CK and CA scores differ largely from similar CCS populations in the interest of informing the potential need for targeted analysis within future research.
Literature relating to CRI measures associated with RoCKAS-ST results among athletic cohorts, however, appear scarce. This is likely due to the complex nature of examining CRI; including consideration of behavioural intent, attitudes, subjective norms, and perceived behavioural control; a problem previously described by Register-Mihalik et al. 33 Whilst the evaluation of CRI via responses to question 3.1 of the RoCKAS-ST has been utilised previously amongst literature, it has significant limitations in the subjective and singular nature of the question analysed.22,23 However, given the constraints of the current study, analysis of CRI via this method was utilised to guide and inform future research. In the study by Salmon et al. 22 in 2021, CRI results were reported relative to Likert scale scoring (rather than converting to the scoring system utilised to derive the overall CA result) therefore results could not be directly compared. Another study by Hardaker et al. 32 drew reference to the proportion of ‘safe’ CRI responses in female community soccer players, with over two thirds (68%) of players (age 15–54 years) providing a ‘safe’ response to the CRI assessed statement in the RoCKAS. The result published by Hardaker et al. 32 was considerably higher (safer) than the proportion of ‘safe’ responses provided by the AF cohorts in the present study. Notable, by comparison, the U16 cohort in the present study observed less than one third of players that provided a ‘safe’ CRI response (Table 5). Whilst it would be reasonable to hypothesise that younger age in the U16 cohort may be associated with decreased playing experience, SRC education, and SRC exposure potentially negatively impacting CRI responses, findings from other studies appear to negate this. In a study of male and female high school contact sport athletes by Kurowski et al., 34 younger age was associated with better SRC self-reporting behaviours. A finding reinforced by a 2019 review, which revealed younger age was a major facilitator in SRC reporting behaviours among high school and collegiate athletes. 35 Again, whilst no universal normative reference values exist for CRI using the RoCKAS-ST, comparison amongst similar populations suggests results of the present female AF cohort differ considerably. One notable difference between comparable studies for CRI however, was differences in competition level; with comparable studies examining community level athletes. Recent research among ‘elite’ (national and international) youth athletes revealed perceived threat to athlete performance or success is a key variable contributing to concussion under-reporting. 36 Given the present study examined Tier 3 athletes, it is reasonable to hypothesise that perceived threats to playing time and national draft prospects may have been a contributing factor to a higher degree of ‘unsafe’ CRI responses. However, it is important to note that any number of differing intrinsic and extrinsic variables between the studies may be responsible for the variance in CRI observed. Nonetheless, further research is warranted to ascertain reasons for the ‘unsafe’ CRI demonstrated in the present AF cohort, particularly in the U16 cohort, when compared to similar CCS cohorts.
When evaluating RoCKAS-ST domain results between competition levels, significant differences were observed in CK, CA, and CRI scores between the OA and the younger of the youth AF cohorts (U16). By comparison, significant differences between the OA and the older of the youth AF cohorts (U19) were only observed in CA scores, and significant differences between the older (U19) and younger (U16) cohorts were only observed in CRI scores. The authors were unable to find any literature that examined differences in CK, CA, or CRI relative to competition level among female athlete populations. Further research is required across a broader range of AF competition levels to establish an understanding of any association between competition level and CK, CA, and CRI to assist researchers and practitioners in informing future SRC injury prevention and education initiatives.
Regarding relationships between CK, CA, and CRI, results of the present study indicated a strong, statistically significant linear relationship between CA and CRI. Multiple regression analysis examining the associations between RoCKAS-ST domains also demonstrated CA was significantly and positively associated with CRI; when controlling for CK, every 1-unit increase in CA score was associated with a 0.08 increase in CRI score. However, in both analyses, CK was not found to have any statistically significant relationship or association with CRI. This finding is of particular importance to sports practitioners and researchers working in the area of SRC educational interventions given existing literature indicates that historically SRC education programs have largely placed emphasis of SRC knowledge as the primary measured outcome of interest. 37 In a 2022 systematic review examining SRC education interventions, only 21% of the interventions examined addressed all three domains (CK, CA, and CRI) as an outcome measure of interest. 37 Among the interventions within the review, 100% measured CK as an outcome measure of the intervention, yet fewer than 30% measured CA and CRI as an outcome measure of interest. 37 Hussain et al., 37 highlight amongst their key recommendations that a tailored approach specific to unique target audiences should be considered as a priority in future development of SRC education interventions. With this in mind, considering the significant relationship between CA and CRI for female AF players in the present study, the development of future SRC education and prevention initiatives that focus on improving CA for this cohort may be warranted. Further research that examines CA and CRI via more robust methods is required, to explore variables that may drive this relationship to best inform SRC initiatives.
Among the regression analyses of associations between demographic / athlete profile variables and RoCKAS-ST domains, age was found to have a weak but significant positive association with CK and CA in our study cohort. CK increasing with age has been noted in previous literature. For example, in a study by Kurowski et al., 34 older age was associated with increased CK in a cohort of 496 male and female high school athletes. Similarly, a study by Register Mihalik et al. 38 found higher CK scores were significantly associated with older age in a cohort of male and female CCS athletes aged 8–15 years. However, findings relating to CA in the present study have not been consistently reinforced across the literature. A systematic review by Beran et al. 18 examining factors related to CK, CA, and CRI in high school athletes in the United States of America found little evidence for age being significantly associated with CA. More research is required to thoroughly evaluate the association between age and CA. Finally, the CRI regression analysis in the present study was likely underpowered to detect small effects, therefore future research utilising larger cohorts is required when analysing association between age and CRI in female AF players.
History of SRC was the only remaining variable found to weakly but significantly be associated with RoCKAS-ST domains. While CK increased with SRC history, CA decreased with SRC history. There are mixed findings amongst the empirical literature with respect to these results. The previously mentioned review by Beran et al. 18 supports findings within the present study with history of SRC commonly being associated with decreased CA scores (i.e., poorer attitudes toward concussion). However, the same review noted ‘disturbingly’ that most studies evaluating high school athletes found history of SRC was not associated with increased CK. 18 The results of the present study relating to an increase in CK following SRC in female AF players are promising, optimistically highlighting potential benefits of recent advancements in SRC resources and protocols from AF league level. 39 However, the observed decrease in CA associated with SRC is concerning. Findings of the present study indicate that amongst female AF players there is a positive and strong association between CA and CRI, however, CA appears to decrease the more female AF players are exposed to SRC. Therefore, given the relationship and association between CA on CRI, this trend suggests that the more female AF players are subject to SRC injuries, the less likely they may be to report future SRC injuries. Whilst this association may not be the case for every athlete and certainly requires further research utilising large scale female AF samples, this trend is not unique amongst the literature - in a 2024 study of male and female university student-athletes, those with a history of SRC were more likely to report continuing to play sport whilst experiencing SRC symptoms. 40 Another study by Register-Mihalik et al. 41 found a positive history of SRC was negatively associated with CA and CRI in a cohort of 167 male and female high school athletes. This apparent cycle of SRC under-reporting associated with repeated SRC exposure has long been described in the literature among ‘cultural issues’ associated with SRC under-reporting in sport, and is extensively outlined in the 2023 Commonwealth of Australia Senate report on concussion and repeated head trauma in contact sports. 42 Importantly though, emerging evidence has unveiled a number of variables that may support increased CA and CRI among athlete populations. Fostering motivational team culture, building self-efficacy skills, and promoting optimal athlete well-being should be considered when designing future initiatives aimed at improving CA and CRI in athlete populations.35,43 Post-SRC specific interventions may also be appropriate to address the potential shift in players willingness to report SRC symptoms following SRC injuries.
Overall, given the significant relationship and association identified in the present study between CA and CRI, further research into associations between a broad range of intrinsic and extrinsic variables and these domains in female AF players is needed. When doing so, researchers should consider other validated measures that examine CRI via more robust methods such as those developed by Register-Mihalik et al., 33 Kroshus et al., 44 and Milroy et al. 45 If the findings of the present study are considered and recommendations suitably addressed in future research and SRC education and prevention strategies, a shift that aims to improve CA and CRI results could lead to improved belief systems and reporting outcomes associated with SRC. This, in turn, has the potential to have a meaningful impact on the health and longevity of female AF players in the future.
Practical implications
The RoCKAS-ST values from this study can be used by sporting researchers, practitioners, and coaches as a baseline reference for Tier 3 female AF players.
The findings of the present study suggest AF coaches and relevant club staff / stakeholders should;
Reflect on likely barriers that exist in CRI for female Tier 3 AF players, such as perceived threats to playing time and national draft prospects.
36
The present study revealed CRI in female Tier 3 AF players appear lower (more unsafe) than similar female contact and collision sporting cohorts.
32
Consideration should be given to initiatives that may target changes to systems, environment, culture, and broader athlete self-efficacy and well-being development that may enable athletes to report symptoms of a concussion in a supportive environment with reduced fear of repercussions.35,43 Consider reviewing and / or implementing post-SRC strategies and initiatives targeted at maintaining and / or improving CA (and in turn CRI) in female Tier 3 AF athletes following concussive injuries. The present study revealed previous history of SRC in female Tier 3 AF players was associated with a significant reduction in CA scores. Understand that a high CK score in female Tier 3 AF athletes does not necessarily translate to improved CA or CRI, given the present study demonstrated no significant relationship between CK and either CA or CRI. Historically, SRC initiatives have largely focused on SRC education (i.e., targeting CK).
37
AF coaches and clubs should review their use SRC initiatives and consider SRC programs that address all three domains.
Limitations
Whilst this study included a relatively large sample of female athletes within a specific sporting code, the cohort existed within a small geographical area and was not representative of all competition levels, therefore results may not be generalisable across the broader female AF athletic population. Given the nature of a survey instrument there were also several inherent limitations such as response bias, potential for misunderstanding or misinterpreting questions, and lack of longitudinal data. Results pertaining to CRI should also be interpreted with caution given limitations associated with the use of a single question to measure CRI, such as the risk of; limited content validity, vulnerability to random measurement error, interpretation variance, and direct measurement bias. Additionally, there were a number of athletic profile / demographic variables that could not be examined via multiple regression analysis due to a low number of incidences within specific variables (less than 10); such as participation in previous SRC education and use of headgear when playing. Finally, logistical constraints associated with pre-season data collection resulted in baseline demographic surveys only being captured via online methods, which resulted in a number of non-responses. These limitations should be considered when interpreting the findings of this study, and future research should consider examining a broader female AF population across all competition levels.
Conclusion
This study details the first known CK, CA, and CRI measures among female AF players and provides a baseline for Tier 3 female AF cohorts. Findings suggest lower CRI scores than similar CCS cohorts may be indicative of a need for further research to ascertain barriers to SRC reporting in Tier 3 female AF players. With respect to the examination of competition level differences, the results of this study should be used alongside future research across a broader range of AF competition levels to establish a clearer understanding of associations between competition level and CK, CA, and CRI. The present study identified just two variables (age and SRC history) that were significantly associated with one or more of the RoCKAS-ST domains, therefore, more research is needed to explore a greater range of intrinsic and extrinsic variables associated with CK, CA, and CRI. Trials are therein required to determine if variables identified as significant truly have any predictive relationship with RoCKAS-ST domains in female AF players. The significant association found between CA and CRI, and lack thereof between CK and either CA or CRI, is important. Where SRC education and prevention programs have largely concentrated on SRC knowledge in the past, there appears a need to adapt SRC curriculum to encompass strategies aimed at shifting CA and CRI. Variables highlighted within the research to date should be considered in efforts to improve CA and CRI in female AF players.35,43 Future research should focus on examining barriers to developing positive CA and CRI specific to female AF players and investigate strategies, including post-SRC initiatives, targeted at improving CA and in turn CRI.
Footnotes
Ethical consideration
This study was conducted in accordance with the ethical approval granted by Bond University Human Research Ethics Committee (LE00041).
Consent to participate
Written informed consent to participate was obtained from each participant in this study prior to study commencement. Where a participant was aged 17 years or younger, written informed consent was also obtained from a parent and / or guardian.
Author contributions
Laura Ernst: Conceptualisation, Methodology, Investigation, Visualisation, Writing – Original draft preparation. Jessica Farley: Conceptualisation, Methodology, Investigation, Supervision, Writing – Reviewing and Editing. Nikki Milne: Conceptualisation, Methodology, Investigation, Supervision, Writing – Reviewing and Editing.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Australian Government Research Training Program (RTP) Scholarship, (grant number doi.org/10.82133/C42F-K220).
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability
The datasets generated and/or analysed in the context of the current study cannot be made publicly available for ethical reasons; the public availability could compromise confidentiality and/or participant privacy as the data contain potentially identifying information.