
Abstract
Exercise physiologists, kinesiologists and coaches prescribe strength training to diverse populations with individual goals. Data-driven coaching is especially crucial with the rise of remote coaching, particularly in rural areas, to compensate for lack of direct supervision. Heart rate variability (HRV) has become a useful tool for measuring the effects of training stress on the autonomic nervous system and is easily accessible via wearables. The purpose of this study was to assess the effectiveness of using HRV to adjust strength training frequency in a remote coaching setting led by a group of recreationally trained participants. The participants completed a 6-week strength training program with pre- and post-lab testing (strength, body composition, blood pressure). HRV was collected daily by the participants, and an HRV threshold was calculated to determine whether they should train each day. Training data and a daily questionnaire were also completed and submitted to the leading researcher. The main findings showed that adherence to the protocol was high compared to other interventions in the general population and that the protocol led to significant strength gains without significantly impacting autonomic modulation. This study contributes to preliminary evidence supporting the effectiveness of HRV-guided strength training in remote settings.
Introduction
Exercise physiologists, kinesiologists, and coaches prescribe resistance- or strength-training (ST) programs to diverse populations seeking improvements in health, performance, and activities of daily living. Long-term benefits—from increases in lean mass and bone density to better metabolic and psychological health—depend on delivering an adequate workload while allowing sufficient recovery between sessions. 1 The balance between workload and recovery is difficult to achieve in practice: excessive loading or inadequate rest can lead to suboptimal results or unwanted effects such as injuries, loss of motivation for exercising, physical or mental fatigue, and, in extreme cases, precipitate adverse conditions such as exertional rhabdomyolysis.2,3 Recovery capacity varies widely among individuals 4 ; therefore, coaches require objective tools to monitor the balance between training workload and recovery. Chen et al. (2011) demonstrated that parasympathetic nervous system activity closely mirrors individual recovery capacity following exercise, highlighting that recovery varies substantially between athletes due to autonomic responsiveness, accumulated fatigue, and training load—therefore requiring coaches to rely on objective physiological tools (e.g., heart rate variability (HRV) monitoring) rather than subjective perception to accurately individualize training and optimize adaptation. 4 Therefore, recovery capacity is profoundly individualized, varying widely due to physiological factors such as genetics and training history, as well as lifestyle and psychological factors (e.g., sleep quality, stress levels).5–7 This inherent variability means that coaches cannot rely on generalized protocols or subjective assessments alone, as what promotes recovery for one athlete might lead to overtraining in another. 8 Consequently, coaches require objective tools, such as HRV monitoring, biological tests (salivary cortisol, immunoglobin A, testosterone,…), psychological and social monitoring as well as performance tests (isokinetic strength testing, jump test, grip strength, agility test…), to monitor the balance between training workload and individual recovery, thereby preventing overtraining and optimizing adaptation and performance.5,9–11 However, some testing can be more expensive or difficult to use, such as biological sample testing compared to others, like the HRV.
Heart rate variability (HRV)—an index of autonomic nervous system activity—has emerged as a promising measurement. HRV is an indirect measure of the autonomous nervous system's (ANS) activity, which regulates various automatic processes throughout the body (e.g., blood flow, breathing, digestion, temperature regulation). In the context of ST, previous studies have shown an acute decrease in HRV, (higher sympathetic activity, lower parasympathetic activity); following adequate recovery, HRV increased, indicating an increase in parasympathetic activity and a decrease in sympathetic activity, respectively. Furthermore, acute ST sessions typically suppress parasympathetic tone and reduce HRV; subsequent restoration or “rebound” signals that the athlete recovered.3,12 Parasympathetic responsiveness also appears to be sensitive in training volume, suggesting that HRV could guide day-to-day decisions about session frequency or load. While HRV-guided prescriptions are gaining popularity in endurance sports, 13 only a few studies have explored this approach in ST. Notably, De Oliveira et al. 14 demonstrated that adjusting session frequency to daily HRV yielded comparable strength and hypertrophy in fewer sessions than a fixed-frequency plan. However, their work was conducted face-to-face and used a fixed number of sessions rather than a fixed intervention duration.
The rationale for remote data-informed coaching is particularly strong in rural and geographically dispersed regions, where limited access to qualified exercise professionals and training facilities constrains structured supervision and long-term adherence. Rural populations report reduced access to exercise services and greater logistical barriers, including travel burden and limited facility availability, which are associated with lower participation and higher adherence rates in structured programs.15–18 Telehealth and remote supervision models have emerged as viable strategies to mitigate these disparities, demonstrating comparable effectiveness to in-person interventions in several rehabilitation and chronic disease contexts.19,20 Parallel advances in wearable sensor technology and mobile health platforms now enable continuous, non-invasive physiological monitoring outside laboratory settings, increasing the feasibility of scalable remote coaching systems.21–23 Within this technological framework, heart rate variability (HRV) provides a validated marker of autonomic nervous system activity and recovery capacity, reflecting the dynamic balance between sympathetic stress and parasympathetic restoration following training stimuli.24,25 As explained previously, individualized recovery capacity is known to vary substantially between and within individuals due to accumulated fatigue, sleep quality, psychosocial stress, and training load.26–28 Without objective monitoring, coaches relying solely on subjective feedback risk misaligning training frequency with physiological readiness, potentially impairing adaptation or increasing injury risk. Integrating HRV monitoring into remote coaching models, allows practitioners to individualize training frequency and adjust load based on objective recovery status, thereby partially compensating for the absence of direct supervision and supporting adherence through tailored, data-driven feedback mechanisms. Therefore, incorporating HRV monitoring into a remote program could help fill the supervisory gap by customizing the frequency to individualize training and ensure adequate supervision and support, based on observations of a sedentary population. 29
The main objective of this study was to evaluate the effectiveness of an HRV-based, individualized frequency ST program implemented through remote coaching over 6 weeks. We hypothesize that integrating daily HRV monitoring into our 6-week remote ST program, will lead to higher participant adherence compared to a program without direct supervision, as reported by Yuki Arikawa et al., 15 by tailoring training frequency to each participant's actual recovery status, we believe the program will be more effective and better aligned with their perceived energy levels and recovery. This alignment could provide a form of supervision and support needed without direct supervision. 29 The secondary objective was to investigate the effect of an HRV-based program on gains in muscle mass and strength for squat and bench exercises over a 6-week period. We also aim to document digital tools and protocols for remote coaches in rural regions, where coaches must support clients across large geographic areas and cannot provide constant in-person supervision. 30
Methods
Participants
This study used 9 participants (7 males and 2 females) with a mean age of 29.7 ± 8.8 years (estimated squat 1-RM: 100.2 ± 49.7 kg (220.9 ± 109.5 lbs.), estimated bench press 1-RM: 77.6 ± 39.9 kg (171.1 ± 88.0 lbs.) Participants were recruited through voluntary response to advertisements (posters, email, and social media), constituting a non-probabilistic convenience sample. Participants were excluded if they did not have at least 24 months of reported strength training experience, had limitations to train such as chronic health or psychosocial issues (e.g., diabetes, cardiovascular disease, musculoskeletal issues, depression, anxiety disorders, alcoholism), used anabolic steroids or anabolic substances in the past 24 months, had symptoms of overtraining or have had rhabdomyolysis in the past or had any prescription medication that could affect HRV. Menstrual cycle details and oral contraceptive use were not included in the demographic data questionnaire. All participants were informed verbally and in writing of all procedures, risks, benefits, and their rights during the study before signing a consent form approved by the Research Ethics Board of Université du Québec à Rimouski (CER-122-995).
Study Design
This free-living single-group interventional study followed the study design illustrated in Fig. 1.
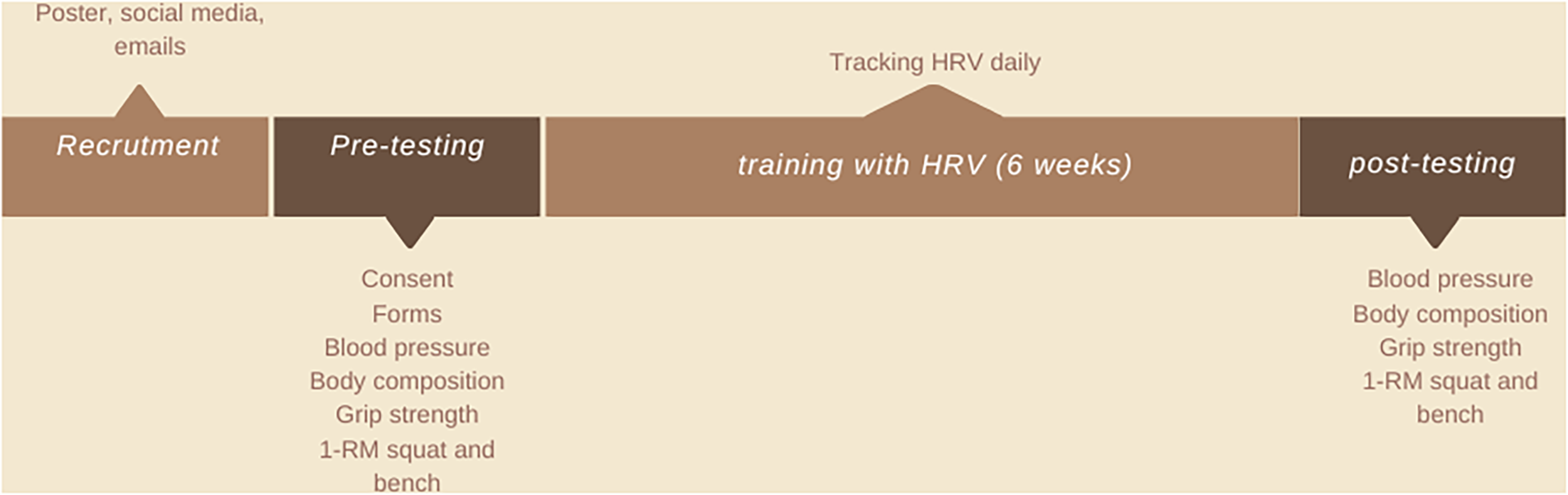
Study design.
Pre- and post-testing
At the pre-test appointment, participants received detailed instructions on the testing procedures, the detraining period, methods for collecting heart rate variability (HRV), training data collection protocols, and how to complete an online self-assessment questionnaire. Following this briefing, informed consent was obtained, and participants completed the Get Active Questionnaire 31 and the Nordic musculoskeletal Questionnaire 32 as screening tools.
Assessments were conducted in the morning or early afternoon in a temperature-controlled environment. Both pre- and post-testing included measurements of resting blood pressure, seated grip strength, body composition via bioimpedance and ultrasound, and one-repetition maximum (1-RM) estimations for barbell squats and bench press.
Resting blood pressure was measured first to ensure the participant's safety. Following by the bioimpedance assessment of body composition, verbal instructions were provided according to the manufacturer's protocol (Inbody770, South Korea). 33 The body composition analysis also included an ultrasound scan using the BodyMetrix system (IntelaMetrix, USA). The ultrasound algorithm was based on the right side of the seven-site skinfold method of Jackson & Pollock (i.e., triceps, biceps, subscapularis, suprailiac, abdomen, thigh, and calf). 34 This measurement was performed by the same staff who received company training.
For strength evaluation, grip strength was assessed with participants seated, their arms at their sides, and their elbows flexed at 90 degrees using a hand dynamometer (Jamar, USA). Participants maintained a neutral wrist position throughout the test. Three trials were conducted for each hand, and the average of the three trials was calculated. Furthermore, a 1-RM test was performed and was estimated for both barbell squat and bench press using a six-repetition maximum (6-RM) test. Foot position during squats was not standardized, but the distance between participants’ heels was recorded to ensure consistency across the pre- and post-tests. A squat wedge was used, and squats were required to reach minimum depth consistent with International Powerlifting Federation (IPF) technical rules. 35 Spotting was provided by the research team to ensure that the anterosuperior iliac crest dropped below the top of the knee. For the bench press, the procedure followed the American Council on Exercise (ACE) guidelines. 36 Two submaximal warm-up sets (initial load determined by participants) were performed for each exercise, followed by incremental increases in weight (determined by participants between trials). Participants were allowed four minutes of rest between trials. Testing was conducted to assess volitional failure, defined as the participant's decision that they could not perform more than 6 repetitions. In some cases, participants were unable to complete the last repetition, indicating a momentary failure. The number of attempts was between 2–4 after the warm-up. Final 1-RM estimations were calculated using the NSCA 1-RM prediction chart. 37 The NSCA prediction chart was based on previously published regression equations derived from empirical strength-testing datasets, primarily those reported by Brzycki 38 and Epley, 39 which modelled the relationship between load and number of repetitions performed to failure. 40 Minimum squat depth was standardized to ensure consistency across participants. A repetition was considered valid when the iliac crest descended below the superior border of the patella (i.e., achieving at least parallel squat depth). Depth was visually monitored in real time by a trained member of the research team positioned laterally to the participant. All assessors were trained prior to data collection to ensure consistency in depth determination. If a repetition did not meet the minimum depth criteria, participants were verbally cued to adjust subsequent repetitions.
Heart Rate Variability baseline
After initial testing, participants were asked to refrain from intense exercise for 5 days before the 6 weeks of continuous ST. HRV data was collected every morning to establish a baseline. The participants were required to collect HRV for 10 min under the same conditions (upon waking up, after urinating, in the supine position in bed, and before ingesting food or drink) using a heart rate monitor (H10, Polar, Fi). The mean and standard deviation for the 5 days were calculated. The baseline was defined as the average of the five detraining days. The HRV floor value was calculated as the baseline value minus 1 standard deviation.
Strength-training program
After baseline testing, participants underwent a 6-week ST program. The program consisted of a rotation between 6 sessions using a push-pull-legs split (supplemental material is available for details). The training program consisted of 3–4 sets of 5 exercises per session, with 6–10 repetitions per exercise. The intensity was set at 1–3 repetitions in reserve, so the last working sets were carried close to momentary failure. The rest periods between sets were 90 to 120 s. The sessions started with compound exercises and followed by isolation movements. The participants were instructed to train on a flexible schedule determined by their daily HRV. The program was available on the remote coaching tool TrainHeroic (Mobile application software, USA). The participants had access to detailed daily sessions on the mobile application, which included tutorial videos for each exercise. The participants were instructed to refrain from intense exercise outside of the prescribed training protocol for the duration of the experiment.
Participants’ self-reported measures and HRV during training
The HRV data was recorded on each participant's mobile phone using an application (Heart Rate Variability Logger by A.S.MA B.V.). Each morning, participants emailed the data to the team for analysis using the export function. HRV data were analyzed using computer software (KubiosHRV V 2.2, Finland), and ectopic beats were removed using the same software. A 5-min sample of the clearest signal was used for analysis. The root-mean-square of successive differences between normal heartbeats (RMSSD) was used to determine training status. It was communicated to the participant, indicating whether to train or not that day. If the RMSSD for the day was below the RMSSD at baseline minus one standard deviation (HRV floor), the participant was instructed not to train that day. 14
Data analysis
The training conditions were reported and numerically coded as such: 1. Could not train, did not train, 2. Could train, did not train, 3. Could train and trained, 4. Could not train, but trained, and 5. HRV data missing. Two groups were formed from this adherence data: more adherent participants were those who respected training conditions 1 and 3 at least 75% of the time and had omitted HRV tracking no more than 25% of the time (condition 5). At the same time, less adherent participants did not meet these criteria. The term ‘adherence’ was used in this paper to describe a participant's active choice to use the prescribed intervention for their well-being in an ecological environment. 41
The HRV variables analyzed were the RMSSD (HRV) and HRV floor to determine the training days. The RMSSD difference daily compared to baseline (HRVdiff), the average RMSSD per week (HRVavg), the ratio of HRVdiff to HRV floor (HRV floor ratio), and the average of HRV floor ratio were used to observe fluctuations during the 6-week training program. Also, the square root of the summation of the square roots of the different previous variables was calculated and divided by the number of variables obtained during the week (RMS) to assess variance.
Statistical testing was performed using JASP v.0.18.3 (Apple Silicon, USA) software. After visual inspection, the Shapiro-Wilk test was used to test the normality. Paired T-tests were performed to analyze the results of pre-post testing. RMANOVA (Friedman tests) and Conover post hoc testing were performed for the HRV and training load variables to evaluate changes from week to week. Compliance was added as a moderating factor. The alpha criterion for significance was set at 0.05. Cohen's d-effect sizes were also reported to observe the magnitude of mean differences (small=0.2; medium=0.5; large=0.8; very large=1.3). 42
Training quantification
The training volume load (TVL) was calculated as tonnage (number of repetitions multiplied by the load (in lb)) extracted from the training mobile application. An average was calculated each week to minimize daily fluctuations, and summation of these TVLs (total TVL) was performed to evaluate workload changes between weeks. The variance in training volume for each week was calculated using the square root of the summation of the total volume load (TVL) of the week, divided by the number of training sessions during the week (RMS TVL).
Results
Eight participants completed the 6-week protocol and underwent both pre- and post-testing. One participant requested to drop out before the final week of the experiment. Participants completed 20.6 ± 5.5 sessions, as recorded in training logs.
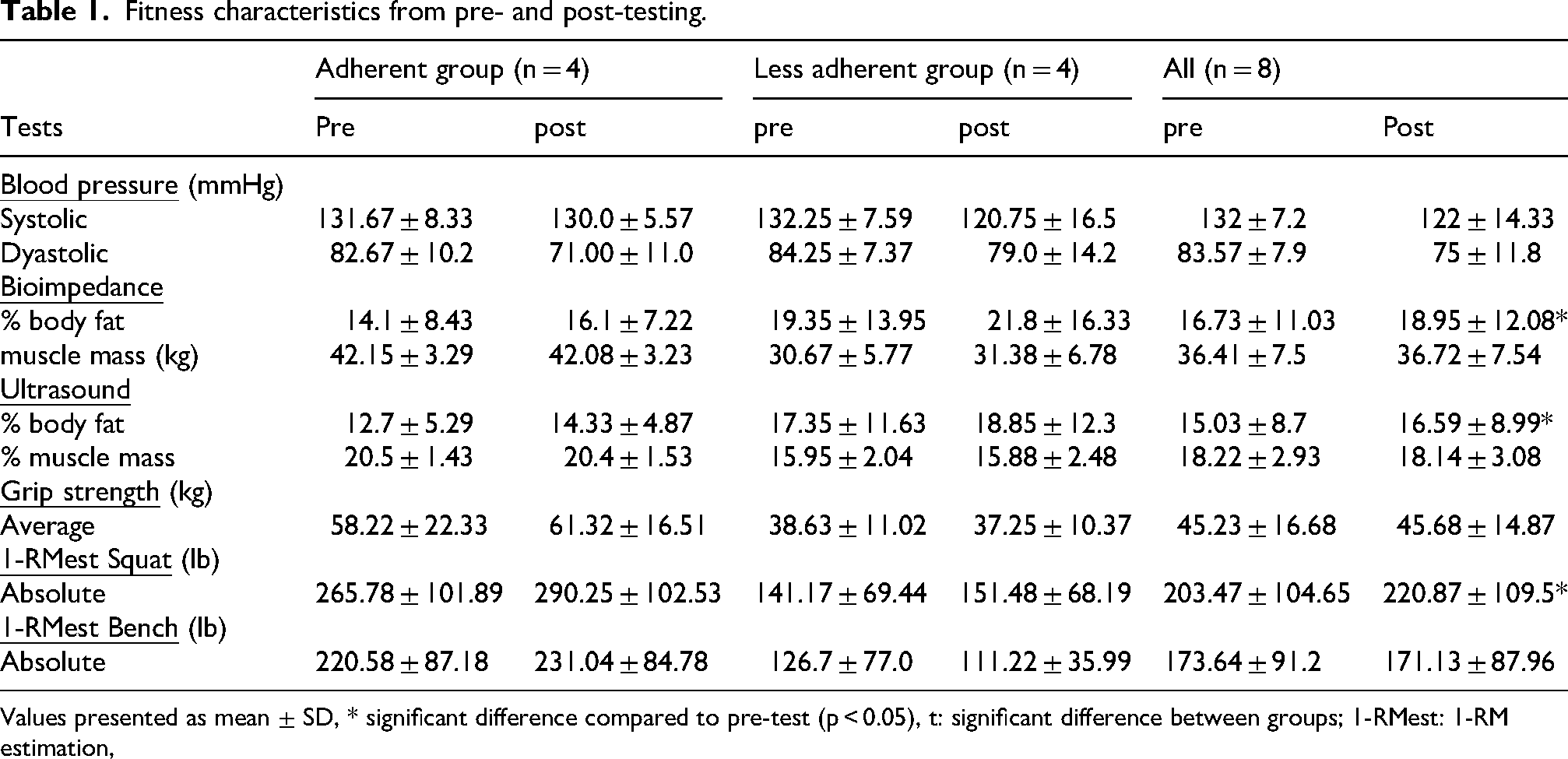
The pre- and post-testing data are presented in Table 1. The comparison of pre- and post-for systolic (t(6) = 1.628, p = .155, d = 0.615) and diastolic blood pressure (t(6) = 2.018, p = .090, d = 0.763) was insignificant. For both variables, pre-data was missing for 1 participant.
Fitness characteristics from pre- and post-testing.
Fitness characteristics from pre- and post-testing.
Values presented as mean ± SD, * significant difference compared to pre-test (p < 0.05), t: significant difference between groups; 1-RMest: 1-RM estimation,
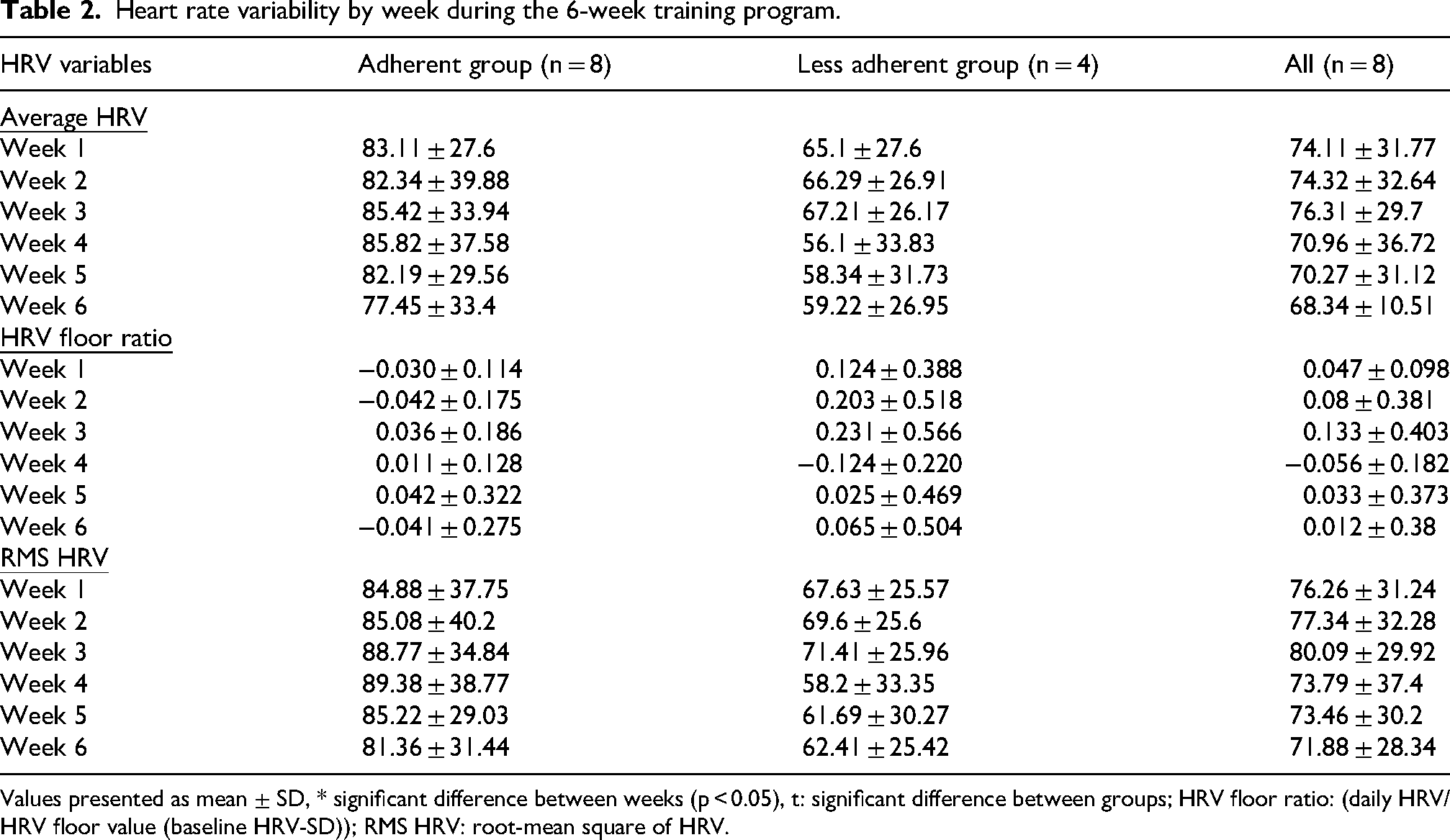
The different HRV variables are presented by week in Table 2. Average HRV per week showed no significant changes (χ2(5) = 8.43, p = .134). HRV floor ratio changes were not significant (χ2(5) = 8.43, p = .134). Root-mean square HRV (RMS HRV) was not significant (χ2(5) = 7.36, p = .195). Pre-post comparisons for root mean square difference HRV (RMSD HRV) were not significant (χ2(5) = 7.429, p = .191).
Heart rate variability by week during the 6-week training program.
Heart rate variability by week during the 6-week training program.
Values presented as mean ± SD, * significant difference between weeks (p < 0.05), t: significant difference between groups; HRV floor ratio: (daily HRV/HRV floor value (baseline HRV-SD)); RMS HRV: root-mean square of HRV.
The TVL is illustrated in Figure 2. Average TVL per week almost reached significance (χ2(5) = 10.67, p = .058) (fig 2.a). Total TVL per week changes were not significant (χ2(5) = 4.39, p = .495). Total TVL increased from weeks 1 through 3 and decreased in week 4. This decrease was followed by an increase in week 5 and a decrease in the last week (fig 2.b). Repeated measures ANOVA showed no effect of compliance for average TVL (F(5, 1) = 1.16, p = .355) and total TVL (F(5, 1) = 0.541, p = 0.744) for weeks 1 through 6 (fig 2(b)). The root-mean-square of total weekly TVL (RMS TVL) was significant (χ2(5) = 12.88, p = .025). Conover's post hoc test was run to observe differences between specific weeks. The plot showed a linear increase in total weekly TVL variance for weeks 4 to 6 (2c).
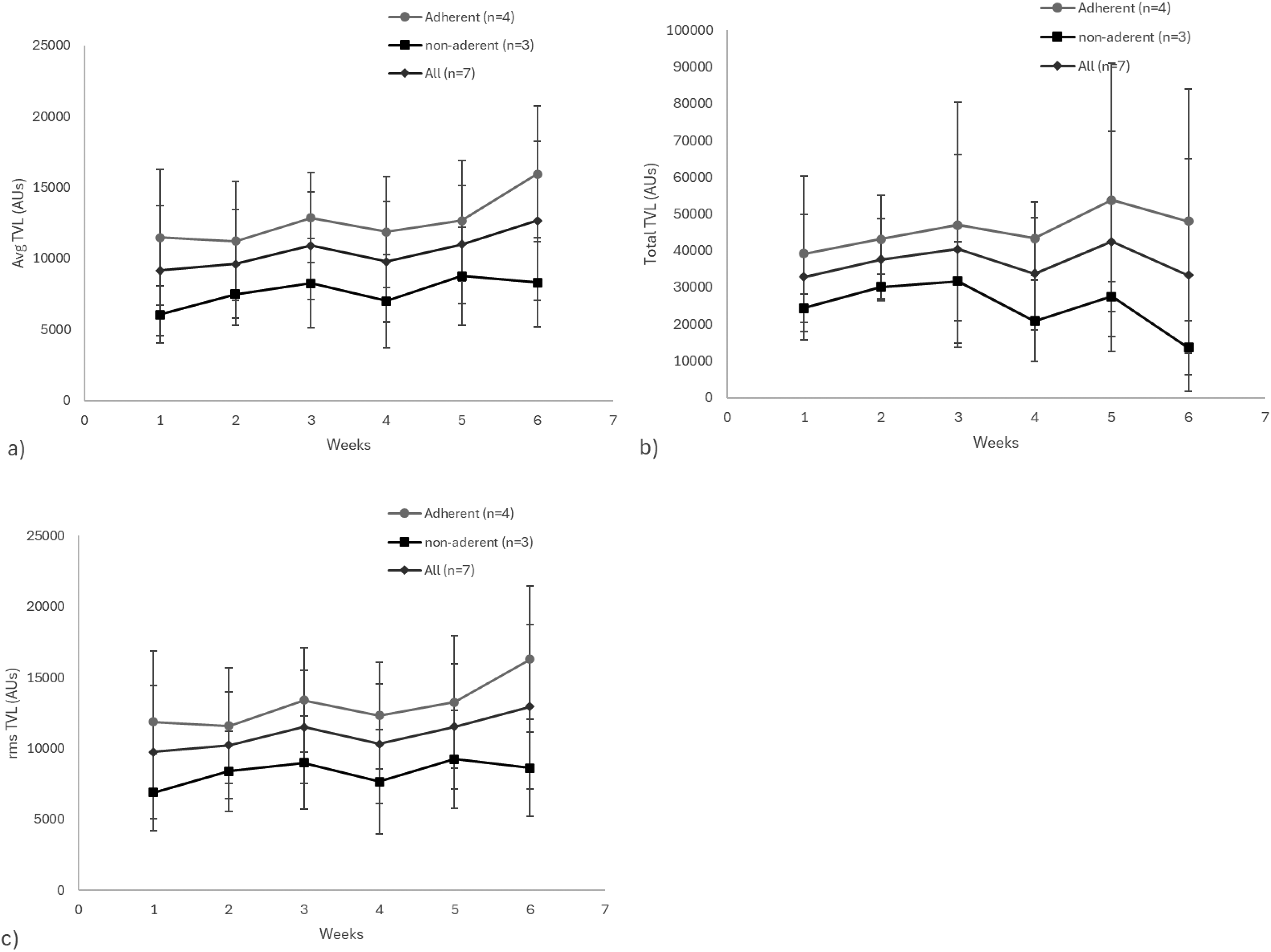
Training volume load variable for each week: a) Average TVL for both group together and separately per week, b) Total TVL both group together and separately per week, c) the root-mean-square of TVL (RMS TVL) for both group and separately per week. AUs means for arbitrary units.
Overall, participants adhered to the training conditions on average 78% of the time. Approximately 13% of the time, participants did not train when instructed, whereas 5% of the time, they trained when instructed to rest. 4% of the time, the research team was unable to determine the participants’ status due to missing data.
Discussion
This study aimed to evaluate the effectiveness of a 6-week HRV-based, remotely supervised strength-training (ST) program with individualized frequency. The main hypothesis was that integrating daily HRV monitoring would enhance adherence to the training frequency by optimizing the alignment between training demands and recovery status. This remote framework was designed to address known adherence challenges in unsupervised programs 15 by offering a personalized structure that can mimic supervision through objective recovery monitoring. 29 The average adherence (78%) to the protocol was superior to most unsupervised training interventions within the general population16,29; in sedentary populations, a similar intervention using a mobile application and training guided by HRV by Casanova-Lizón et al. 29 had an average compliance of 70.5%, which is almost identical to what we observed. A secondary aim was to explore the effects of this intervention on muscle mass and strength (bench press and squat). Our hypothesis that muscle mass and strength would be higher in adherent people than in nonadherent people was partially confirmed. The 6-week intervention significantly increased the estimated 1-RM squat for all participants. However, muscle mass and 1-RM bench press estimates did not differ significantly after the intervention, whereas body fat measurements increased significantly. The observed significant increase in body fat percentage should be interpreted cautiously. Although statistically significant, this magnitude of change approaches the known reliability limits of the assessment devices used.33,34 Part of this variation may reflect measurement variability rather than a true physiological increase in adiposity. Also, it is important to note that 1-RM values were estimated from 6-RM testing, which carries a reported prediction error of approximately 0.03–0.05% for squat and approximately 1–4% for the bench press. 43 Although the magnitude of changes suggests a possible physiological adaptation or not, part of the improvement or maintenance may reflect methodological variability. However, the findings could guide the creation of remote coaching tools suitable for rural areas where in-person coaching is limited.
Adherence to Protocol
Adherence was assessed using daily HRV data submissions and compliance with personalized training prescriptions. Participants who submitted HRV data and followed the training prescriptions at least 75% of the time were considered more adherent. Using this standard, half of the participants were classified as more adherent for analysis, with an average adherence to the training conditions of 78%. Literature indicates notable differences in adherence between supervised and unsupervised training. Supervised programs show higher adherence rates: 95% for supervised versus 65% for non-supervised programs in Arikawa et al.; 15 and 76% for the supervised ST program in Davis et al., 44 among women with obesity. Our study more closely aligns with an HRV-guided intervention by Casanova-Lizón et al. 29 in a sedentary population. We recorded an average adherence rate of 78% and a dropout rate of 11% (i.e., one participant withdrew before the end of data collection). These findings align with their observed average adherence rate of 71%. This suggests that HRV tracking and flexible frequency may have enhanced motivation and accountability. To our knowledge, very few studies explored adherence to remote ST interventions in recreationally trained individuals, making it challenging to compare adherence to the protocol with that of equivalent interventions and populations. It is also noteworthy that adherence may be defined differently in supervised studies.
Effects on Physical Fitness
The 6-week HRV-based, remotely supervised ST program with an individualized frequency significantly improved estimated squat 1-RM but not bench press strength. This outcome corroborates findings from De Oliveira et al., 14 who also observed significant improvements in lower body strength in a similar HRV-based intervention. Overall, the training volume of their intervention was superior to ours (8 exercises versus 5). They observed a significant increase in leg extension and estimated 1-RM following 20 sessions of ST intervention modulated by HRV, with similar strength gains observed in the traditional ST group (3 sessions per week). The absence of bench press strength gains compared to the De Oliveira et al. 14 may be attributed to participants’ training experience—many had more than two years of ST before the intervention—and the well-established principle that strength gains are more rapid in novices due to neural adaptations. 45 The mechanisms explaining strength gains are still being studied, but include motor learning (more efficient contraction of agonist muscles), increased excitability of motor units, and reduced cortical inhibition. 45 Moreover, it is also still possible that, for strength gain outcomes, direct supervision by professionals remains superior. 29 Additionally, the 6-week intervention period may have been too short to elicit visible hypertrophy, especially in trained individuals. 46 Our study also used moderate loads (6–10 repetitions per set). According to the general literature, high loads tend to be slightly more effective than moderate loads for strength outcomes, in line with the specificity principle. However, significant strength gains are also seen with moderate loads. 47 Muscle growth is possible with light, moderate, or high loads, if sets are performed close to failure.48–50 A similar outcome was found in a 6-week study conducted on 14 untrained men by Heffernan et al., 51 which used a similar training frequency and weekly training volume. Our participants underwent training in 15 to 29 sessions over a 6-week period, averaging 20.6 sessions per participant. The study by Heffernan et al. 51 involved a 3-session-per-week supervised ST intervention with three sets of 5 exercises (8 to 15 repetitions) aimed at momentarily fatiguing the muscles. Our intervention involved similar volumes, consisting of 3 to 4 sets of 5 different exercises (6 to 10 repetitions) with increasing proximity to failure. Given the flexible training frequency, it is plausible that some participants trained too little to produce adaptations over 6 weeks, as progressive overload is necessary to prevent stagnation and training volume is a key factor in muscle gains.52,53 This could be because, in trained lifters, training history (defined by their usual training volume) influences hypertrophy outcomes, meaning the protocol might not have been a significant enough increase in workload from their typical routine to induce muscle adaptations over 6 weeks. 54 There can also be variance in the definition of trained participants across studies, with some studies considering 6 months of ST experience sufficient. 46 Our participants reported varying levels of training experience, with one participant reporting 15 years or more of continuous ST experience. Other factors, such as genetics and lifestyle, can influence the rate of muscle growth. Our results differed from those of a study by De Oliveira et al., 14 which showed a significant increase in quadriceps cross-sectional area in untrained participants after 20 training sessions. This was further compounded by the lack of control over caloric intake, which could have contributed to the observed increase in fat mass. Participants may have been in a caloric surplus, as ST without dietary control has a limited effect on reducing fat mass. 55
Effect of training parameters on HRV
Using daily HRV to guide training decisions offered an objective “green-light/amber-light” cue that replaced in-person supervision and likely supported the high adherence observed: trainees could skip a session without guilt when HRV indicated incomplete recovery, yet they also had clear permission to train once their autonomic status improved. This flexible approach mirrors the design of De Oliveira et al. 14 while adapting it to a real-world six-week setting. It seems to have stabilized parasympathetic tone, with weekly HRV metrics remaining consistent despite increasing ST volume and proximity to failure, thereby reducing fatigue and supporting proper recovery. We monitored workload primarily through two metrics: tonnage, recorded via training journals on the mobile app, and repetitions in reserve (perceived intensity by participants). We expected tonnage to change significantly during the six-week period, reflecting increased training intensity. Additionally, we hypothesized that workload increases would result in a significant decrease in HRV over time, because medium-to-high volumes are reported to cause a larger short-term reduction in HRV. 56 The average change in training volume nearly reached significance (p = .058), though total weekly volume did not (p = .495), possibly due to significant variance in training load (p = .025). Despite non-significant changes in total weekly training load, our data suggest that autoregulated intensity using repetitions in reserve effectively helped recreationally trained participants increase effort, resulting in significant strength gains. This aligns with existing research, which shows that autoregulating sets near failure allows repetitions in reserve to serve as accurate indicators of intensity, 57 especially as trainees gain more strength training experience. 58 Moreover, our findings offer preliminary evidence that tracking intensity with repetitions in reserve in a remote coaching context may help prevent overreaching. Other long-term observational studies, such as Williams et al., 2 found that activity in the peripheral nervous system decreases with higher training volume load quartiles, which we did not observe. The prescribed training volume may not have been enough to cause parasympathetic withdrawal in recreationally trained individuals. One limitation of this study was that the increase in weekly training volume was not statistically significant, possibly due to reporting errors. We noted some missing weekly data from one participant, which may have impacted the analysis given our small sample size. This suggests that, without direct supervision, there's a risk of incomplete or inaccurate training reporting. Our data suggest that chronic ST may not exert cumulative effects on HRV beyond 24 to 48 h post-exercise, consistent with previous studies.4,14 Few studies have examined HRV over periods longer than six weeks; thus, the long-term impact of progressively intensifying ST on HRV remains unclear. Overall, high adherence and avoiding autonomic overreach may have contributed to the observed increase in predicted 1-RM squat. These mechanisms demonstrate how HRV-guided training frequency can boost commitment and deliver targeted performance benefits in remote coaching.
Limitations
Small sample size (n = 9) limited statistical power and precluded the use of a control group and the analysis of sex differences. Findings should be viewed as preliminary and intended to generate hypotheses, rather than being considered definitive conclusions. Despite the recruitment challenges, the research team encountered other issues; participants were initially required to complete a five-item daily online survey on morning recovery perception. Because of the missing timestamps in the database, we could not analyze the correlation between HRV and perceived recovery.
It was important to note that neither facilitators nor barriers were evaluated for this project. Dietary intake was not controlled, which may have contributed to the observed increase in body fat mass and limited the interpretation of changes in muscle mass. The body composition was assessed using bioimpedance and ultrasound. Thus, small changes in body fat percentage should be interpreted cautiously, which may reflect measurement variability rather than physiological adaptations.
Practical Applications and Future Directions
This study provides preliminary evidence supporting the effectiveness of HRV-guided ST in remote settings. The data suggest that individualizing training frequency based on HRV does not impair recovery and may help maintain adherence in unsupervised environments. This approach is especially relevant in rural or remote areas where in-person coaching is limited. 30 We recommend that coaches implement a remote-monitoring framework where daily HRV readings serve as a readiness “gatekeeper.” In this system, green-light values indicate it's time for a training session, amber values suggest reducing the volume or intensity of the workout, and red values signal the need for active recovery. This approach is similar to programmed sports watches that utilize heart rate, HRV or other metrics; and should be combined with a daily perceived recovery survey. Further research should investigate longer interventions, control dietary intake, and include larger samples to explore the chronic effects of HRV-guided ST on performance, recovery, and hypertrophy. Improved tools for capturing both HRV and subjective recovery would allow a robust exploration of recovery relationships.
Supplemental Material
sj-pdf-1-spo-10.1177_17479541261436950 - Supplemental material for Individualized heart rate variability on a strength 6-week training program. A remote-coaching effectiveness study
Supplemental material, sj-pdf-1-spo-10.1177_17479541261436950 for Individualized heart rate variability on a strength 6-week training program. A remote-coaching effectiveness study by Jean-Philippe Morin, Andrée-Anne Parent and Mathieu Tremblay in International Journal of Sports Science & Coaching
Footnotes
Acknowledgements
Jean-Philippe Morin received a scholarship in 2022 from Réseau Intersectoriel de Recherche en Santé de l’Université du Québec (RISUQ).
Ethical considerations
Ethical approval was granted by the Research Ethics Board of Université du Québec à Rimouski (CER-122-995)
Consent to participate
Verbal informed consent was obtained from each participant, and all participants signed an ethics waiver.
Contribution statement
Idea of the article: Jean-Philippe Morin, Mathieu Tremblay; Data collection: Jean-Philippe Morin; Data analysis: Jean-Philippe Morin, Andrée-Anne Parent, Mathieu Tremblay; Writing the original draft: Jean-Philippe Morin; Review and editing: Andrée-Anne Parent, Mathieu Tremblay; Supervision: Andrée-Anne Parent, Mathieu Tremblay.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding statement
The authors declared no financial support was received for this work.
Data availability
Although the data supporting this study's findings are not publicly available, they can be made available upon reasonable request from the corresponding author. This is necessary to protect the privacy of research participants, and to ensure that confidential information is not compromised. The detailed training program is available in the supplementary materials.
Declaration AI
The authors of this paper utilized AI software to enhance grammar, sentence structure, and paragraph organization, thereby improving readability. All the content was created and reviewed by the authors. AI was also used to format the test results into proper text.
Supplemental material
Supplemental material for this article is available online.