
Abstract
Youth sports development programs provide an opportunity to reach young people in diverse communities with mental health and wellbeing programs. However, ensuring that mental health and wellbeing programs can be integrated into sports programs in a sustainable and engaging format for young people can be challenging. Embedding mental health and wellbeing content within on-field sports activities that can be delivered by local volunteer coaches may overcome some of these barriers. This study examined the perceptions of volunteer coaches delivering on-field mental health and wellbeing workshops within a junior rugby league development program and whether more coaching experience influenced coaches’ perceptions. Of the 48 volunteer coaches recruited, 28 coaches completed the survey: 12 (43%) with more than 10 years coaching experience; 16 (57%) with less than 10 years coaching experience. Compared to less experienced coaches, those with more coaching experience reported significantly more benefit in terms of coaches learning, enjoyment, and engagement from delivering the on-field workshops and having more confidence in completing some online post-workshop protocols. All coaches, regardless of coaching experience, reported high levels of benefit, acceptability, and credibility of the workshops for players. Assessing volunteer coaches’ experience in coaching youth sports may be important for determining their understanding and engagement in delivering mental health and wellbeing programs within youth sports programs.
Introduction
Mental health concerns represent a substantial burden globally, particularly during youth and emerging adulthood. 1 Although many large-scale epidemiological studies have relied on population-level, cross-sectional self-report surveys rather than formal diagnoses that capture more stable and enduring patterns of mental ill-health, the available data suggests that the onset of elevated mental health symptoms commonly occurs during adolescence, with prevalence rates peaking around 14 years of age. Moreover, national surveys indicate that more than 70% of young people experiencing mental health difficulties do not access or receive appropriate support. 2 Numerous barriers impede help-seeking, including service affordability and availability, geographical constraints, family burden, stigma, and confidentiality concerns, particularly in regional communities, 3 alongside broader societal stressors such as social media exposure, climate anxiety, and lifestyle changes. 4
Although studies of youth mental health within sporting contexts have similarly relied on cross-sectional self-report measures that may not capture fluctuations in youth mental health with the highs and lows of sport, these studies have reported elevated levels of self-reported stress and anxiety among youths engaged in organised sports. 5 Moreover, given that 33% of 12–14-year-olds participate in organised sports outside of school at least three times or more per week on average, and 21% of 15–17-year-olds engage in more than one active session a day across 3.5 different activities, 6 organised sports programs represent an ideal context in which to embed mental health and wellbeing programs in order to reach more young people and harness the benefits of sports participation and physical activity on mental health Indeed, participation in organised sports is related to several positive life outcomes including feelings of independence and connection to others, 7 physical and mental well-being8,9 and improved self-esteem.10–12 Due to these positive outcomes, organised sports have been identified as a valuable context to promote and educate youth about physical and mental well-being.13,14
Despite the potential for organised sport to serve as a critical access point for receiving mental health interventions, such programs have not been targeted in a coordinated or broad manner. For example, a report from Liddle et al. 15 found that only 11% of sports organisations in Australia have engaged in campaigns that target player mental health, and those that did primarily focused on boosting personal strengths and stress management, did not target mental health problems,16,17 and often lacked robust evaluation. 18 More recently, researchers have begun to focus on mental health literacy and enhancing help seeking within the context of community sports programs.19,20 For example, Vella et al. 20 examined a four-component intervention (Ahead of the Game Program) to compare sports participants (males aged 12–17 years) in two regional communities. All workshops in the intervention group were delivered by a member of the research team or a registered sport psychology practitioner employed as a research assistant. At 1-month post-assessment, compared to the comparison group (N = 466), the intervention group (N = 350) showed significant improvements in depression and anxiety literacy, intentions to seek help from formal sources, confidence to seek mental health information, resilience, and wellbeing. Similarly, Liddle et al. 19 examined the effects of a mental health literacy program among 102 males aged 12–18 years from a community football club. The intervention group received one 45-min group-based workshop that was delivered at the sports clubhouse by two male undergraduate university volunteer presenters with lived experience of mental illness. At 1-month post-assessment, they found an increase in anxiety literacy and a reduction in stigmatising attitudes in the intervention group. Similar to Vella et al., 20 the intervention had no effect on actual psychological distress reported by players. More recently, Petersen et al. 21 conducted a systematic review including 15 papers (three of our studies were included in the review) aimed at evaluating interventions targeted at the promotion of mental health and wellbeing among males in organised sporting contexts. Most interventions were conducted in-person by health professionals, registered clinical psychologists, accredited facilitators, research personnel, and sporting club stakeholders, and one intervention was delivered entirely online via digital technologies. Of the studies that assessed mental health literacy outcomes, 85.7% reported improvements in anxiety and depression literacy, help-seeking and help provision, and mental health knowledge. Among studies that measured mental health and wellbeing outcomes, 63.6% reported improvements in such outcomes, including anxiety, resilience, and coping self-efficacy. However, the findings do suggest that in relation to many of the mental health and wellbeing outcomes, there were either inconsistent effects (e.g., one of four studies reported positive change in depression), or no effects (e.g., psychological distress, grit, perceived stress).
One approach that has produced beneficial effects on youth mental health outcomes, is the integration of a three-step system (i.e., Life-Fit-Learning) within a junior rugby league development program (i.e., the RISE program) that assesses the mental health and wellbeing of young people (Assess step), provides timely feedback (Reflect step), and connects them to interventions and resources proportionate to their needs and the services available in their communities (Connect step).22–27 In an initial pilot study, 22 we examined the feasibility, acceptability, and preliminary outcomes of Life-Fit within RISE for 74 adolescent boys between 12–15 years of age living in urban and rural communities. The Assess and Reflect steps were conducted online or by telephone, while the Connect step involved activities targeting rugby league skills, physical fitness, and mental health and wellbeing knowledge and strategies (i.e., the Life-Fit component). The Life-Fit component involved four in-person workshops with players and their coaches delivered by two co-facilitators on the research team (i.e., a clinical psychologist and a provisionally registered psychologist) in a room at the training grounds. Findings showed that the Life-Fit-Learning system was feasible to implement, acceptable to players, and efficacious in reducing anxiety and depression symptoms, along with improving personal strengths.
A subsequent study 25 examined the efficacy of Life-Fit within RISE via a community-matched, non-randomised design with 251 male junior rugby league players aged between 12–15 years who did versus did not complete the RISE program in regional communities. High-risk RISE players’ depression and behavioural problems improved from pre- to post-program relative to no change among comparison players. Additionally, of players who were not at high-risk, RISE players’ anxiety, depression, and behavioural problems did not change, whereas comparison players’ behavioural problems increased from pre- to post-program. A third study conducted during the COVID-19 pandemic 24 demonstrated delivering Life-Fit within RISE with 66 male junior rugby league players aged 12–15 years via computer, telephone, and teleconference modalities by Masters-level clinical psychology facilitators was feasible to implement, rated as highly beneficial and enjoyable by players, and reach was high.
Moreover, in an effort to reach more young people in a wider range of communities, we evaluated outcomes following Life-Fit delivered within RISE as per prior studies, but with the four Connect Step workshops delivered via one of four combinations depending on the geographical location, trained personnel, and technology available in each location: (a) In-person Delivery Only, (b) In-person + Remote Real-Time Delivery (video-conferenced), (c) In-person + Remote Prerecorded Delivery (video-recorded), and (d) Remote Delivery Only (video-conferenced or video recorded), 26 among 671 boys aged between 12–15 years in 21 metropolitan, regional, and rural locations. In-person delivered workshops were delivered by local rugby league wellbeing personnel and remote delivered workshops were facilitated by psychologists from the mental health research team with prior training and ongoing supervision sessions. Regardless of delivery condition, players with elevated anxiety, depression, and behavioural problems reported significant declines in symptoms from pre- to post-program, and those within healthy ranges did not change from pre- to post-program. Notably, player workshop enjoyment ratings were higher in the In-person + Remote Real-Time condition and the Remote Delivery Only condition than the In-person Delivery Only condition. The findings highlighted the potential value of non-classroom-like delivery formats that still maintain in-person facilitation for enhancing player engagement. Furthermore, given the challenges in sustaining training and supervision of local sports wellbeing personnel and high workforce turnover, delivery formats that involve online and on-field mental health and wellbeing workshops delivered by volunteer coaches from within the sports community may overcome these barriers.
In our most recent study, 27 we examined mental health outcomes of Life-Fit within RISE among 503 adolescent boys (N = 416) and girls (N = 87) 12–16 years of age across 42 metropolitan, regional and rural locations across Australia. We also examined whether partial or full completion of the Life-Fit program produced different outcomes among the larger sample of boys within healthy and high-risk ranges for anxiety, depression, and behavioural concerns. The Assess and Reflect steps were delivered as per our prior studies, however given the upscaling of the project reaching a wider range of communities, the Connect step was delivered as four online modules completed at home by players, in addition to four on-field workshops delivered in groups by volunteer coaches during RISE training sessions. From pre- to post-program, anxiety and depression symptoms reduced for boys in high-risk ranges, but not to within healthy ranges, but did reduce to healthy ranges for behavioural concerns regardless of whether they partially or fully completed the Life-Fit program. Improvements for depression in boys within the healthy range, and improvements for boys’ self-satisfaction overall, required full compared to partial completion of the Life-Fit program. For girls in high-risk ranges, improvements in anxiety symptoms were observed, but there were no improvements in symptoms for depression, behavioural concerns, or self-satisfaction. Findings from this study suggest that mental health and wellbeing programs embedded in a sporting context may need to be tailored specifically for girls to improve their outcomes, and boys in high-risk ranges may need more focused program content on anxiety and depression to strengthen their outcomes.
A recent study by Petersen et al. 28 examined the willingness of 275 youth sporting club stakeholders (e.g., sportspersons, parents/guardians, support staff, coaches) to engage in mental health initiatives (e.g., perceptions pertaining to youth mental health promotion in sporting clubs) conducted by sporting clubs. Findings indicated that stakeholders were willing to support mental health initiatives conducted by sporting clubs, with key predictors of stakeholders’ support of implementing these initiatives including age (>25 years), and perceptions pertaining to the promotion of mental health (e.g., mental health attitudes about the importance of youth mental health).
To date, very little research has examined outcomes from coach-led and on-field approaches to enhancing mental health and wellbeing in young people within organised sports programs. O’Connor et al. 29 evaluated a community sport mental health literacy program that was delivered to coaches or community sport leaders. They sampled 25 community Australian Rules Football clubs from metropolitan and regional centres and randomised 265 coaches or sports leaders to either the intervention group or a waitlist control group. All 265 coaches/sport leaders completed surveys between 1 and 2 weeks prior to the intervention group receiving the Tackle Your Feelings (TYF) program (i.e., a mental health literacy program) delivered to coaches in each community clubhouse by a qualified local psychologist. Findings revealed that participants in the TYF program reported improved outcomes compared to controls on leader confidence to support and refer, knowledge of resources to support mental health, general help-seeking, and stigmatizing attitudes. Although a nine-month comparison group follow-up indicated some decay in scores over time, the results indicated that community coaches may be an important resource for reaching more young people to address mental health concerns within community sporting contexts.
Nevertheless, the workload and responsibility of formal coaches and officials is a major barrier to sustainable implementation of mental health and wellbeing programs within organised sport. 30 Therefore, the engagement of volunteer coaches interested in assisting young people more broadly provides an opportunity to overcome formal coach workloads as well as offer unique benefits to organisations, players, and the volunteers themselves. 31 Previous research shows that volunteering is associated with several positive outcomes including volunteers’ health, psychological wellbeing, and sense of self-worth.32,33 Furthermore, volunteering is vital not only for stimulating regional economies, but also for fostering community resilience. 34 Busser and Carruthers 35 examined the motivations of 141 youth sport coaches who were volunteering for a youth soccer program. They found that almost 90% of youth coaches had children on their team, however they also cited wanting to make a positive contribution to the lives of young people by instilling positive values in youth as a major motivation for volunteering as a youth coach. Thus, volunteer coaches interested in positive youth development may be ideal for delivering mental health and wellbeing content within the context of a youth sporting program.
Coach-related factors, such as years of coaching experience, may also influence volunteer coaches’ readiness and engagement as well as youths’ sporting experiences. While there is little research that has examined coaches’ readiness, Shull et al. 36 examined how coaching behaviours, coaching experience, and coach training relate to physical activity levels of children aged 6–11 years during their participation in a youth sport program. They found that coaching behaviours, including watching participants perform activities with or without feedback, were associated with coaches’ higher physical activity intensities during their participation in youth sport practice, and that teams with coaches who had more coaching experience, particularly those with five or more prior seasons coached, had higher team physical activity levels compared with coaches who had less experience. These findings demonstrate that years of coaching experience should be considered when assessing volunteer coaches’ perceptions of delivering mental health and wellbeing programs within a sports context for both coaches and players.
The aim of this study was to conduct a preliminary examination of the perceptions of volunteer coaches delivering on-field mental health and wellbeing workshops within a junior rugby league development program. Based on Shull et al.'s 36 findings of the benefits of coaching experience on participation and activity levels, it was hypothesised that volunteer coaches with more years of coaching experience would perceive greater benefits for players and themselves. We also aimed to conduct exploratory analyses relating to volunteer coaches’ evaluations of the acceptability and credibility of the on-field activities and their confidence delivering these activities.
Method
Participants
Participants were volunteer coaches from New South Wales and Queensland delivering the Life-Fit-Learning program within the RISE junior rugby league program across 42 locations with junior rugby league players varying from Under 13's to Under 15's. Volunteer coaches were recruited at each location by the program head coach. A total of 32 of 48 volunteer coaches (hereafter referred to as ‘Life-Fit’ coaches) attempted the survey. However, only 28 (58%) completed the survey. Based on years of coaching experience, there were 12 Life-Fit coaches with more than ten years of experience and 16 Life-Fit coaches with up to ten years of experience.
Materials
The Life-Fit-Learning coaches survey. The research team developed a study-specific evaluation survey to explore Life-Fit coaches’ perceptions of delivering the on-field activities in the absence of suitable published measures. The survey drew on items from acceptability and credibility measures used in previous implementation and acceptability research, including measures used in prior evaluations of child and parent perceptions of Life-Fit reported by Dowell et al. 22 and Waters et al., 37 and the broader literature examining coach's perceptions..38–40 Initial questions asked Life-Fit coaches about their age (e.g., under 18, 18–24 years, 25–34 years, 35–44 years, 45–54 years, and over 55), gender (e.g., male, female, prefer not to answer), ethnicity (e.g., Australian, Indigenous or Torres Strait Islander, New Zealander, Asian, Indian, Middle Eastern, European, North American, South American, African, African American, Other), location delivering the Life-Fit on-field workshops, years of Rugby League (RL) coaching experience (e.g., less than 1 year, 1 year to less than 2 years, 2 years to less than 5 years, 5 years to less than 10 years, 10 years or more), Life-Fit coach experience (e.g., I have not been a Life-Fit coach before, less than 1 year, 1 year to less than 2 years, 2 years to less than 3 years, 3 years to less than 4 years, 4 years or more), and RL playing experience (e.g., never played rugby league, less than 1 year, 1 year to less than 2 years, 2 years to less than 5 years, 5 years to less than 10 years, 10 years or more).
The remaining questions were divided into five sections related to the Life-Fit on-field workshops which focused on coaches’ perceptions of player benefit (e.g., Overall, players enjoyed the Life-Fit on-field workshops), Life-Fit coach benefit (e.g., Overall, I enjoyed delivering the Life-Fit on-field workshops), acceptability (e.g., The Life-Fit on-field workshops are acceptable to deliver to young people), credibility (e.g., I would recommend being a Life-Fit coach to my colleagues), and implementation self-efficacy such as accessing, understanding, and using the Life-Fit Coaches Handbook, completing the online training, using the QR codes, delivering the workshops, and contacting the research team if needed (e.g., How confident were you in your ability to implement the Life-Fit on-field activities effectively?). Participants responded on a 9-point scale ranging from 0 = not at all to 8 = very much for each item.
Procedure
The study had human research ethics approval (GU Ref No: 2018:426). The Life-Fit-Learning program included three steps: Assess, Reflect, and Connect. The first step, Assess, consisted of players completing an online assessment that included questions about players’ health and well-being (e.g., anxiety, negative feelings, grit, gratitude). In the Reflect step, the Life-Fit-Learning system scored the responses, and members of the Life-Fit-Learning team contacted the parents of any players scoring in high-risk ranges for negative feelings, anxiety, and behavioural concerns to provide assistance and referral suggestions where appropriate. Players completed four online modules at home and four associated on-field workshops during the Connect step. The online modules and on-field workshops included content on: (1) Healthy Habits such as sleep and social media usage, (2) Strong Minds, such as grit and optimism, (3) Keep Cool, focusing on management of emotions, and (4) Stay Connected, focusing on gratitude and acts of kindness.22–25
The on-field workshops were delivered by the Life-Fit coaches participating in this study. The Life-Fit coaches completed training for delivering Life-Fit-Learning through four online modules and an online workshop with the research team. They also used the Life-Fit-Learning Coaches Handbook to deliver all components of the on-field workshops, which contained step-by-step instructions and visual examples of all on-field workshop activities accessed via QR codes in the handbook. Additionally, there was a QR code for Life-Fit coaches to click on after each workshop to check-in on how the workshop went for them (e.g., How confident did you feel facilitating the session; How engaged were the players; How well do you feel the session went overall). Their responses to the check-in survey were automatically sent to the research team.
An online survey link was sent to all Life-Fit coaches after delivering the Life-Fit-Learning program across QLD and NSW, requesting their consent to and participation in the survey. Life-Fit coaches who completed the survey were reimbursed a $20 e-voucher as a gesture of thanks for their time in completing the survey (not for volunteering as a Life-Fit coach). Life-Fit coaches had three weeks to consent and complete the survey after delivering the program.
Data screening, response definitions and statistical analysis
Correlation matrices were inspected to examine coherence among items within each section of the survey. Items demonstrated moderate to strong associations (.390–.847), and mean scores were computed for descriptive and comparative purposes. Cronbach's alpha values were calculated to provide an indicative, descriptive estimate of internal consistency for each section (.917–.931), rather than evidence of psychometric validation or inferential reliability, and should be interpreted cautiously given the small sample size and exploratory design.
Categorial variables included gender for male and female (the ‘prefer not to answer’ option was not included in any analyses), ethnicity as Australian or Other (all ethnicity options that were endorsed other than Australian were categorised as ‘Other’ and included Indigenous Australian or Torres Strait Islander, N = 3; New Zealander, N = 1; European, N = 2; and Australian/Dutch, N = 1), age was categorised as under 55 or 55 years and over, coaching experience was categorised as either ten or more years of RL coaching experience or less than ten years of RL coaching experience, Life-Fit coach experience was categorised as either having been a Life-Fit coach or having not been a Life-Fit coach, and RL playing experience was categorised as either played before or not played before. All other survey items were continuous variables, including coaches’ perceptions of player benefit, Life-Fit coach benefit, acceptability, credibility, and implementation self-efficacy.
Chi-square analyses were used to examine any differences in categorical variables between RL coaching experience groups including gender, ethnicity, age, Life-Fit coach experience, and RL playing experience. Independent samples t-tests were performed to examine differences between RL coaching experience groups in continuous variables including coaches’ perceptions of player benefit, Life-Fit coach benefit, acceptability, credibility, and implementation self-efficacy.
Results
Control analyses
Demographic information for Life-Fit coaches as a function of less and more years of RL coaching experience can be found in Table 1. There were no significant differences between Life-Fit coaches with more and less RL coaching experience in proportion of those younger and older than 55 years X2 (1, N = 28) = 2.054, p = .152, males relative to females X2 (2, N = 28) = 4.083, p = .130 (For gender, only the categories for male and female were included in the analyses. The ‘prefer not to answer’ category for gender was not included in the final analyses.), and whether or not they had been a Life-Fit coach before X2 (1, N = 28) = 0.608, p = .436. However, Life-Fit coaches with more years of RL coaching experience had more years of RL playing experience than Life-Fit coaches with fewer years of RL coaching experience X2 (1, N = 28) = 9.333, p = .002. Furthermore, there was a significant difference between ethnicity and coaching experience X2 (1, N = 28) = 7.000, p = .008, whereby a greater proportion of Life-Fit coaches with less than 10 years of RL coaching experience identified as Australian.
Demographic details for life-fit coaches as a function of less and more years of rl coaching experience.
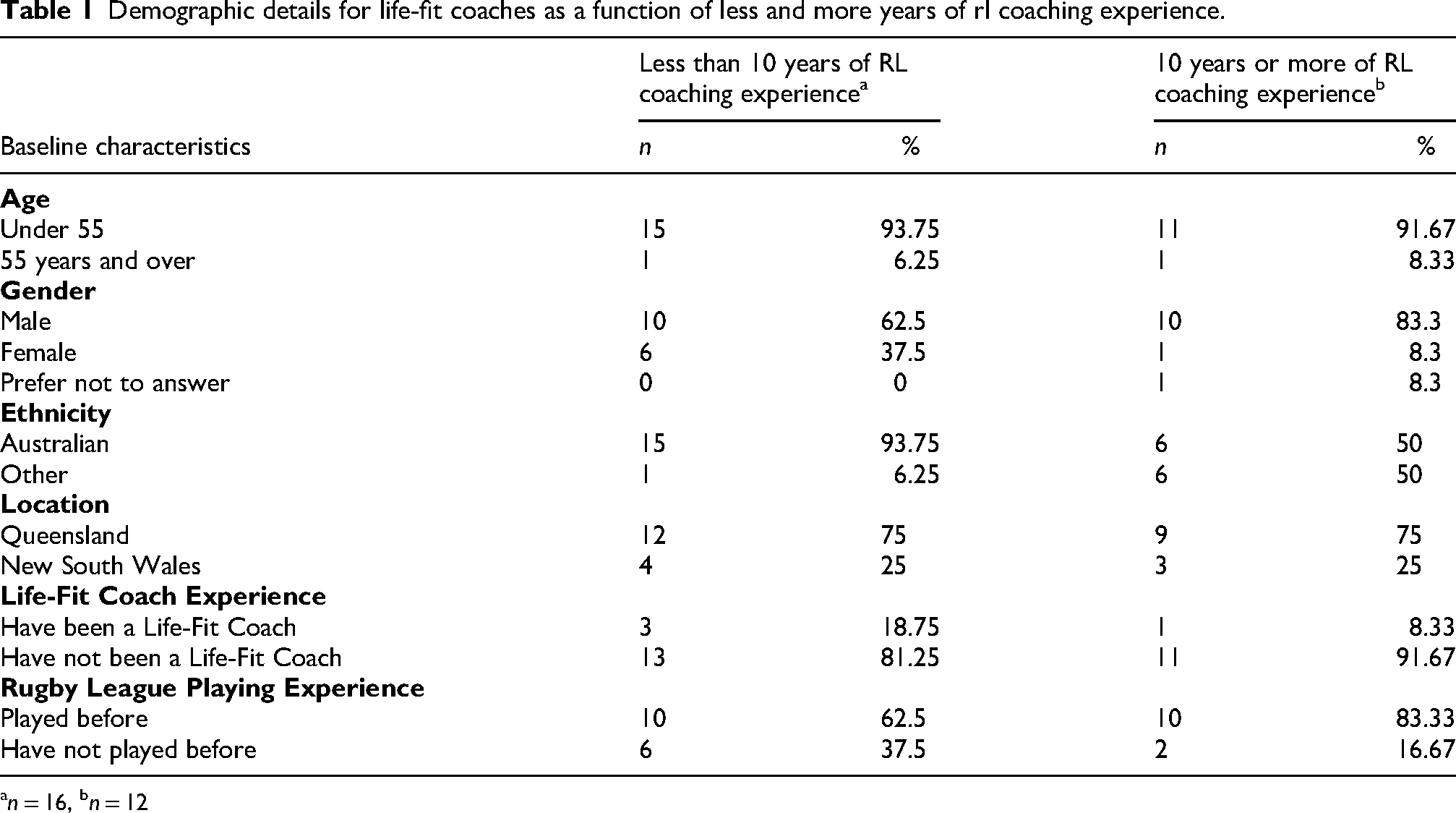
n = 16, bn = 12
Life-Fit coaches’ perceptions of players experience
The results for Life-Fit coaches’ perceptions of players experience of the Life-Fit program as a function of less or more years of RL coaching experience can be found in Table 2. There were no significant effects of years of RL coaching experience on player benefit t(26) = - 1.114, p = 0.138, acceptability t(26) = - 0.717, p = 0.24, or credibility of the program t(26) = - 0.657, p = 0.258, with all Life-Fit coaches providing high ratings in general (see Means and SD scores in Table 2, response scales ranged from 0–8 for each item).
Analyses of life-fit coaches’ perceptions of players and coaches experience of the life-fit program as a function of less and more years of rl coaching experience.
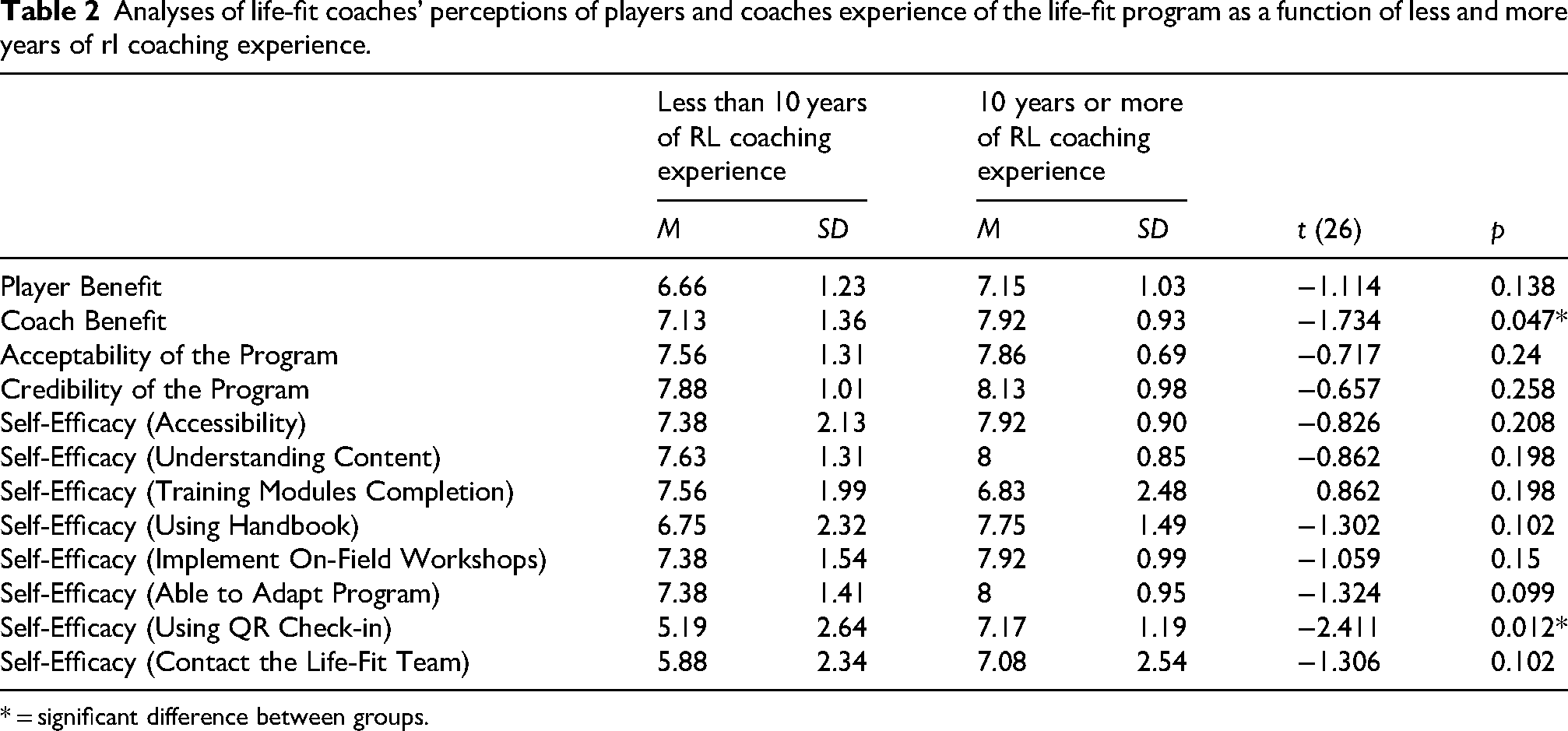
* = significant difference between groups.
Life-Fit coaches’ perceptions of coaches’ experience
The results for Life-Fit coaches’ perceptions of coaches’ experience of the Life-Fit program as a function of less or more years of RL coaching experience can be found in Table 2 (the mean scores for the self-efficacy subscales were calculated individually). Life-Fit coaches with more years of RL coaching experience perceived participation as a Life-Fit coach as significantly more beneficial for themselves compared to Life-Fit coaches with less years of RL coaching experience, t(26) = - 1.734, p = 0.04. Life-Fit coaches with more years of RL coaching experience also reported greater confidence in completing the QR check-ins post-workshop than Life-Fit coaches with less years of RL coaching experience, t(26) = -2.411, p = 0.012.
Discussion
This study aimed to investigate Life-Fit coach perceptions of delivering the on-field workshops as part of the Life-Fit-Learning component of the NRL RISE program. Overall, findings suggest that Life-Fit coaches perceived that both players and themselves benefited from the workshops and found the program to be acceptable and credible as indicated by high ratings in general, regardless of having less or more years of RL coaching experience. Positive evaluations may not be surprising, given that Life-Fit Coaches were volunteers who had invested their time to assist with program delivery. This pattern may partly reflect an ‘advocacy effect’, whereby individuals who are personally invested in a program are more likely to evaluate it favourably. Nevertheless, Life-Fit coaches with 10 or more years of RL coaching experience did perceive greater personal benefit from delivering the program and more confidence in completing the QR check-ins after each workshop than Life-Fit coaches with less than 10 years of RL coaching experience. Greater perceived benefit from delivering in the Life-Fit-Learning program align with those of Shull et al. 36 who found that coaches who had five or more years of coaching experience, observed greater benefits, such as higher physical activity levels of their players, compared with coaches who had less coaching experience.
The findings may reflect that by commencing training some 10 + years ago when the integration of mental health and wellbeing programs within sports was far less likely,39–42 Life-Fit coaches with more years of RL coaching experience may have had fewer prior opportunities for engagement in mental health and wellbeing programs and therefore found the experience more worthwhile and a welcome addition to community sports programs. They may also have a greater understanding of the challenges of coaching young people and the value of mental health and wellbeing workshops for improving their coaching knowledge and ability to engage with youth players in a meaningful way. Additionally, Life-Fit coaches were specifically tasked with focusing their time and attention on the mental health content of the Life-Fit program, rather than coaching RL, and thus, may have derived greater perceived personal benefit given the nature of the experience.
In terms of Life-Fit coaches’ perceived benefit with 10 or more years of RL coaching experience, as there were no significant differences in Life-Fit coaches’ age, and differences in having less or more years of RL playing experience did not relate to Life-Fit coaches’ perceptions of benefit, it is unlikely that the results reflect differences in personal life stages or playing history.
In relation to confidence in completing the post-workshop QR check-in, these findings could indicate that Life-Fit coaches with more years of RL coaching experience have likely had previous exposure to various programs with multiple reporting requirements. Specifically, Life-Fit coaches with more years of RL coaching experience may be more familiar with following similar processes for task completion and thus may have found the QR check-in process to be a similar routine to previous coaching roles. Additionally, they will likely have had greater exposure to many different programs throughout their coaching careers. If this one stood out to them as teaching something new or different, their perceived benefit would be higher than Life-Fit coaches with less RL coaching experience who have not been exposed to as many programs.
Another point of interest is Life-Fit coach participation in this study. In similar studies, coach participation is between 50–58%,43,44 while other studies had much lower with 6–20% of individual coaches participating.40–42 By comparison, the participation rate for this study is in the upper range similar to other studies, with a 58% participation rate (total of 28 Life-Fit coaches). It appears that coaches in previous studies43,44 were not incentivised for their time, however they were incentivised a small gift card amount in the current study. It may be that coaches may need to be incentivised from the outset to increase participation rates and ensure that the incentive is sufficient to entice participation, particularly if they are volunteers. However, further studies are needed to fully understand the barriers and enablers of Life-Fit coaches who did and did not complete the survey.
Although the present study revealed some interesting findings, several limitations should be acknowledged. First, the Life-Fit coaches’ survey relied exclusively on quantitative responses; the inclusion of open-ended questions may have allowed coaches to elaborate on their experiences and provide richer contextual insights. Future research would benefit from incorporating qualitative methods such as interviews and focus groups to more deeply explore coaches’ perceptions, including aspects of the program that were most effective and those that could be improved. Second, the current study utilised a study-specific survey with a small sample of coaches, which precluded formal psychometric validation. Future research with larger and more diverse samples should seek to further refine and validate measures assessing coach perceptions and implementation outcomes. Third, the absence of a formal measure of social desirability limits the extent to which the influence of response bias on the uniformly high scores can be determined. Given that participating coaches were volunteers who had invested time in program delivery, favourable evaluations may partly reflect an advocacy or social desirability effect. Future studies would benefit from incorporating a social desirability measure to better contextualise self-report responses. Fourth, participation was limited to a three-week data collection window, which may have contributed to the modest response rate. Extending the recruitment period in future studies may facilitate greater participation and reduce potential self-selection bias. Relatedly, future research would benefit from actively engaging coaches who were hesitant or did not participate in the current study to better understand barriers to involvement and to inform strategies for broader engagement. Fifth, the findings may have limited transferability beyond the specific sport and program context examined. While the Life-Fit program was delivered within a youth rugby league development program, implementation processes and coach perceptions may differ across sports with varying cultures, structures, and developmental pathways. Future studies should examine the applicability of similar interventions across a wider range of sporting contexts. Finally, while the present study focused on Life-Fit coaches’ experiences of program delivery, youth mental health outcomes have been reported in our previous studies.22–27 Building on this work, future research should prioritise (1) examining program implementation across different sports and settings, (2) refining strategies to engage less involved or initially hesitant coaches, and (3) exploring ways to embed mental health supportive practices within sport environments through developmentally appropriate, non-stigmatising approaches that do not rely on overt mental health framing.
Taken together, these preliminary findings suggest that perceptions of player and Life-Fit coach benefits and program acceptability and credibility were high overall. Furthermore, Life-Fit coaches with 10 years or more of RL coaching experience perceived more significant benefits from the program and greater confidence in completing QR check-ins than Life-Fit coaches with less than 10 years of RL coaching experience. Future research that examines barriers and enablers of Life-Fit coaches’ engagement in delivering these programs would provide more detailed information that could improve strategies to engage and support community coaches in delivering mental health and wellbeing programs for youth within junior sports programs.
Footnotes
Ethical approval
Human research ethical approval was obtained from the Griffith University Ethics Committee (GU Ref No: 2018/426).
Consent participant
All human subjects provided informed consent.
Author contributions
All authors contributed to various aspects of the study conception, design, material preparation, data collection or analysis. The manuscript was written by all authors who read and approved the final manuscript.
Funding
This research was supported by funding awarded to the authors from the Australian Sports Commission and the School of Applied Psychology, Griffith University.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
The data that support the findings of this study are available from the corresponding author, RS, upon reasonable request.