
Abstract
Rugby tackles can cause head acceleration events (HAEs) which may acutely and chronically affect brain health. This study aimed to investigate the varying proportions, impact forces and rugby-specific factors of tackles from different directions relative to the ball carrier which may illuminate strategies to reduce injury and health risks. Boys from four youth boys’ teams in New Zealand (one U13 club: n = 19 players, 13 matches; two U16 club: n = 41, mean of 31.5 matches; one U16 representative: n = 26, 8 matches) wore instrumented mouthguards and all matches were videoed and analyzed to verify the collisions resulting in a tackle and code them based on rugby-specific and biomechanical factors (anticipation, falling, head position, face position). Of the 2539 tackles resulting in HAEs, most were front-on (56–64%). Tackle direction had no significant effect on either mean peak linear or rotational acceleration, however significantly fewer tackles from the rear resulted in impacts that would trigger an elite rugby head injury assessment than tackles from the front and side. The older and more skilled players more often had correct head positioning in front and side-on tackles, whereas almost none of the tackles from the rear had incorrect head positioning. Additional training focus should be given to tackles from the side and rear with younger players as they have poorer anticipation in these directions often resulting in higher HAE magnitude. Face up tackling seems to be best for reducing impact forces in tackles from behind, while face down tackling appears to be safest for front-on tackles.
Keywords
Introduction
Rugby union is among the most popular contact sports worldwide with 8.4 million players in 132 countries, an 11% increase from 2022. 1 Despite rugby's potential physical fitness, mental health and social benefits for players2–5 and cultural importance,6–8 potential safety concerns, notably its resultant head acceleration events (HAEs: rapid change in velocity of the head resulting from direct or indirect contact with the head, which may or may not result in injury) and their effects on rugby player health, merit further investigation. There is currently relatively little literature on youth rugby despite knowledge that they may be at greater injury risk than adult rugby players. 9
Relatively novel instrumented mouthguard (iMG) technology has permitted more accurate and reliable laboratory and field measurement of head kinematics10–12 that has allowed researchers to begin accumulating HAE exposure datasets in various rugby populations from elite adults to children.13–15 This may provide important information into the potential relationships between training and match rugby head loading and acute and chronic injury etiology.
Tackling is a key rugby skill used to compete for ball possession and territory which results in frequent contact and can cause injury,16,17 is the most common form of physical engagement in the sport, 18 occurring on average 99.4 times per game in youth players 19 and is an important determinant in performance outcomes.20–22 Studies in elite, adult rugby have found its intense and competitive nature can cause anticipated and unanticipated collisions which may result in a concussion,23–25 brain injuries in general 26 and all injuries. 27 Across all age groups, rugby has been found to be the contact sport with the highest rate of concussion incidence: 28.25 per 10,000 athlete-exposures. 28 Though no significant neurological changes have been found after one season of boys rugby, 29 long-term rugby exposure may have pathological brain health outcomes later in life.30,31 Additionally, there has been concern regarding learning outcomes and school performance from contact sport exposure and concussion/mild traumatic brain injury in youth athletes with developing brains.32–34 Tacklers have been reported to have higher concussion risk and be subject to more head injury assessments (HIAs) than ball carriers being tackled in professional rugby 35 and twice the concussions in professional American football. 36 Examining and enhancing understanding of the incidence, magnitude, biomechanics and sport-specific elements of tackles can help improve player safety.37–41
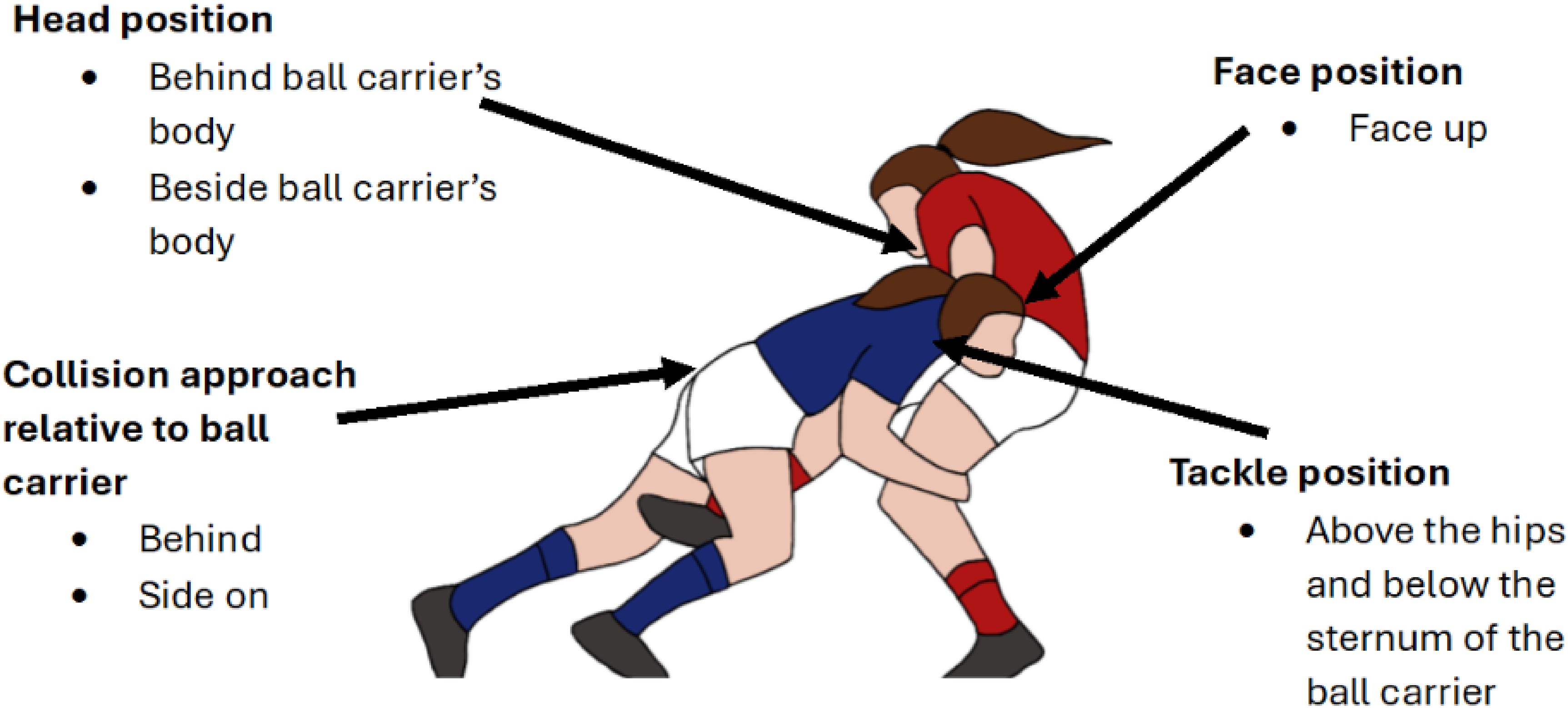
Coaching initiatives from national governing bodies like New Zealand Rugby's Rugby Smart 42 and the South African Rugby Union's Bok Smart43,44 recommend specific tackling technique for a safer, more effective tackle (see Figure 1). These recommendations include the tackler keep their face up, approach the tackle from the side or rear, contact the ball carrier's torso and/or hip and position their head beside or behind the ball carrier. Previous research has found equivocal evidence for tackle direction given that increased injury risk has been associated with tackling from behind 45 or front 46 but other studies showed no significant differences in PLA (peak linear acceleration, g)/PRA (peak rotational acceleration, radians/s2), 19 velocity of the tackler approaching side or front-on tackles 47 or injury risk48,49 for front on tackles versus those from the side/rear. In laboratory testing involving a human participant tackling a tackle simulator (moving 40 kg punching bag), front-on tackles resulted in higher biomechanical load to the tackler than tackles at 45° and 90°. 50 Other elements of recommended tackle technique (face position, tackle and body location) showed no significant differences in PLA/PRA versus unrecommended techniques. 19 The tackle technique that has the strongest support is head position,51,52 with studies showing the tackler's head being in front of the ball carrier's body rather than beside/behind increases injury risk 25× 53 and increases PLA (Cohen's d = 0.64) and PRA (Cohen's d = 0.74) forces to the head. 19
Tackling has also been examined through a performance lens, with tackling from the front reducing the likelihood of the ball carrier successfully offloading the ball and breaking tackles 22 and an American football study found head up tackles were 16.6% more likely to be successful than head down tackles and tackles with the head in front of the body were 33.2% less effective. 55 These performance based strategies, including the tackler avoiding making initial contact with their head by using an active shoulder tackle, 48 have also been linked with reduced injury risk. 41
Previous rugby tackle direction research has had conflicting results. No previous youth studies have directly measured HAE forces using field data and rugby-specific/biomechanical descriptors. The aim of this study was to investigate how the proportions, HAE PLA/PRA and rugby-specific factors differed among tackles from the front, side and rear of the ball carrier in boys rugby union.
Methods
Participants
Ethical approval for all procedures and experimental design was obtained in full from the University of Canterbury Human Ethics Committee prior to undertaking the study. Ethics approval for the study was initially obtained on 13 July 2021 (Ref: HEC 2021/26). The study was approved by New Zealand Rugby's (NZR) Medical Science and Advisory Panel (18 July 2019).
Participants were recruited via an informational meeting with the players and their parents from four specific boys teams within the greater Ōtautahi Christchurch region of Aotearoa New Zealand during the 2022–2024 seasons: a year 8 (under 13) club team (n = 19, 10 forwards, 9 backs; age: 13.26 years ± 0.47; height: 164.70 cm ± 8.96; weight: 54.79 kg ± 9.42; rugby experience: 5.84 years ± 2.41), two junior (under 16) club teams (n = 41, 26 forwards, 15 backs; age: 15.02 years ± 0.76; height: 178.41 cm ± 7.59; weight: 73.67kg ± 13.56; rugby experience: 7.44 years ± 2.74) and a U16 representative (reps) side (n = 26; 12 forwards, 14 backs; age: 16.08 years ± 0.28; height: 178.84 cm ± 5.96; weight: 78.84 kg ± 10.30; rugby experience: 9.45 years ± 2.50), a higher ability team than the U16 club consisting of players that were selected to play on and represent their sub-union as they distinguished themselves in their sub-union based on their play during the club rugby season. All participants provided informed written assent and their parent/guardian provided written consent before participating in the study.
Procedure
This study used a prospective observational cohort design and iMGs. Before the season, participants received dental scans from an orthodontist which were digitally sent to HitIQ who manufactured custom-fitted Nexus A9 mouthguards (HitIQ Ltd, South Melbourne, VIC, Australia) for each participant. The iMGs used in this study contained a gyroscope (Bosch, Germany, BMG250, ±2000 dps range, 16-bit), three triaxial accelerometers (Analog Devices, USA, ADXL372, range: ±200 g, 12-bit) and had sampling rates of 800 Hz/3200 Hz (linear/rotational). An independent validation study found them to have high accuracy (R2 = 0.996 for PLA and 0.994 for PRA). 11 During manufacture, HitIQ set the recording threshold at the World Rugby (WR) standard of 8 g. 56 PLA values below 8 g were not recorded, both to exclude recording of accelerations resulting from non-contact movement, such as running or jumping and to decrease the amount of noise in the data.57,58 HAEs were recorded when a single accelerometer sample was ≥8 g on any of the three axes. 15 A higher recording threshold may omit many valid HAEs, as most HAEs in rugby have been found in the 10–15 g range. 59 The IMGs recorded 20 ms before and 80 ms after each recorded event, allowing for events with multiple impacts to be recorded. Recorded HAEs were stored in the iMG's onboard memory.
All matches were video recorded from the highest midfield location using a Canon HFG50 digital video camera (Canon Inc., Japan) and/or Panasonic HC-X1500 (Panasonic, Japan) affixed to a Manfrotto MK290LTA3-V 290 tripod (Manfrotto, Italy). Additionally, a referee-mounted camera (GoPro Hero10 camera, GoPro Inc., USA) was used. The iMG data exported from HitIQ's servers and video footage were uploaded to Catapult Focus (Catapult Sports Technology Ltd, Australia) and synced via New Zealand standard time displays at the start and end of each video. Rugby exposure was calculated from the video for how many minutes of match play in which each player participated.
HAEs were video verified by a trained researcher with reliability being assessed by a second researcher. The analysts were trained on the video coding by experts from Catapult and experienced rugby players and coaches. The data analysis process (see Figures 2 and 3) began with video verification to rule out mouthguard false positives, determining whether the imported tags recorded by the iMGs were a real contact event (‘yes’) or not (‘no’). Additional descriptors were added to each HAE. If the event was tagged ‘no’ (false positive), a reason was given (such as mouthguard removal), and the tag was completed. If the event was tagged ‘yes’, then as much more detail as could be visualized about the event was provided: direct (head location and the surface the head contacted were both noted) or indirect (whiplash, jarring, etc.), falling (controlled, uncontrolled or unknown), match action (tackler, ball carrier, breakdown, ruck, etc.) and impact anticipation (good, poor, none or unknown). Though this is part of a larger research project measuring all rugby match actions, only HAEs coded as ‘tackle’ were included for analysis in this tackle-specific study. Where possible, detailed analysis of each event using zoom, slow-motion, and frame-by-frame scrolling were utilized. 24 To aid in the verification process, players’ presence in game-play action was confirmed by an expert reviewer and cross-referenced with each session's field diary. Where possible, players’ jersey numbers were used to confirm identity. For HAEs that were verified ‘yes’ but lacked clear visuals, descriptors such as being ‘obstructed’ were added. 60

Catapult Focus interface for video verification and analysis. The top shows the video footage available (purple box), and bottom shows each iMG tag ≥ 8 g (green vertical lines indicated by the white arrows) on a row for each participant.
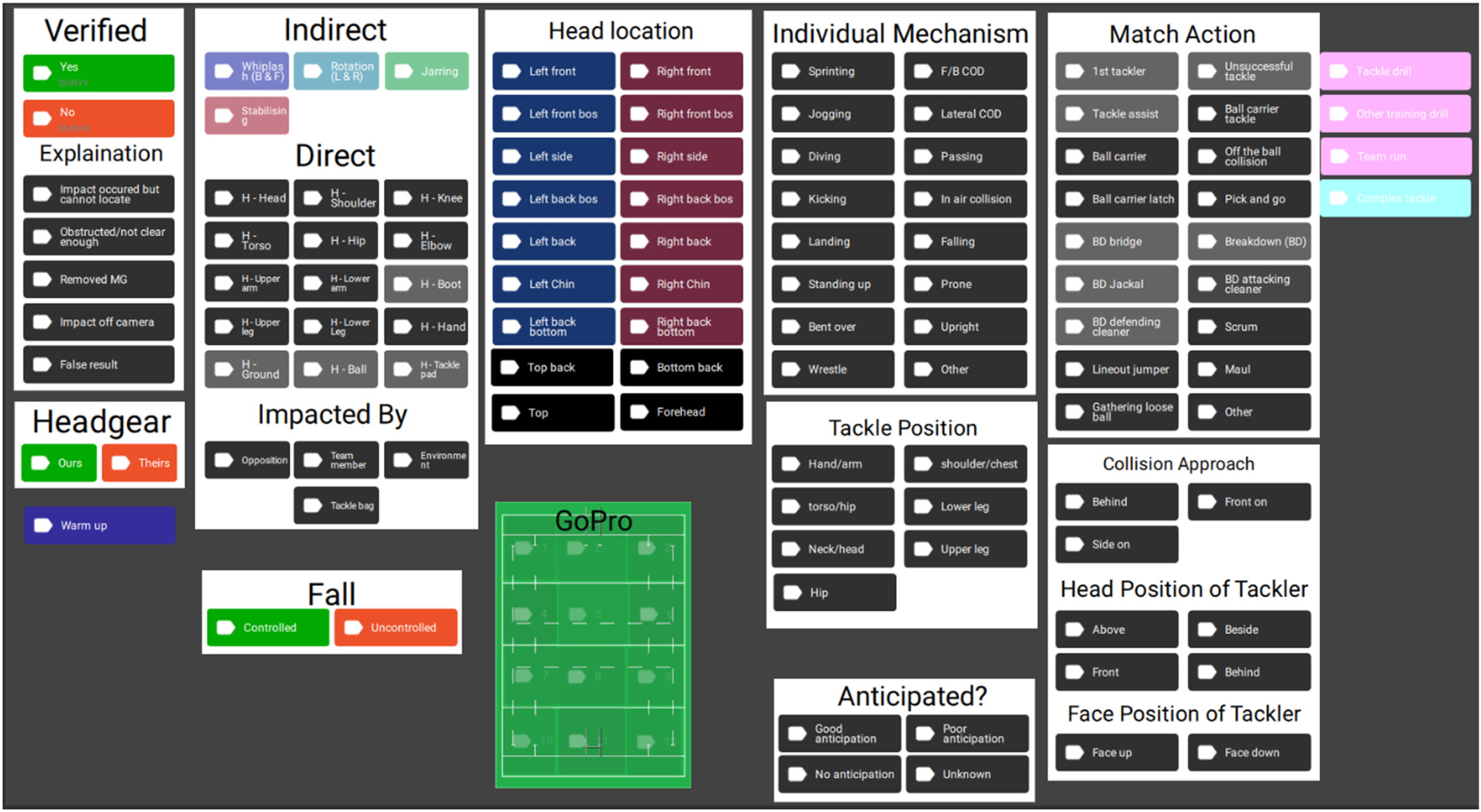
Catapult focus interface showing the coding template used for video verification and analysis.
We employed the method of Field, et al. 60 whose overall positive predictive value was calculated by a thorough video review process (using timestamped footage, adjusting angles, pausing and using slow motion when needed to verify and descriptively code HAEs) and using visually verified events only, and the current directives of WR which defines false positives as ‘active events’. 61 To this end, the positive predictive value (PPV, see Table 1) was calculated using the following formula and found to be very similar to the values for HitIQ reported by Jones et al.: PPV calculation: all data. Positive Predictive Value (all) = true positivetrue positive + false positive (no + other). 10
Positive predictive value (calculation of false positives).

HAE = head acceleration event; TP = true positive; FP = false positive; PPV = positive predictive value.
Statistical analysis
Statistical analyses were conducted using Microsoft® Excel® for Microsoft 365 MSO (Version 2409 Build 16.0.18025.20214) 64-bit and IBM SPSS Statistics (v29.0.0.0).
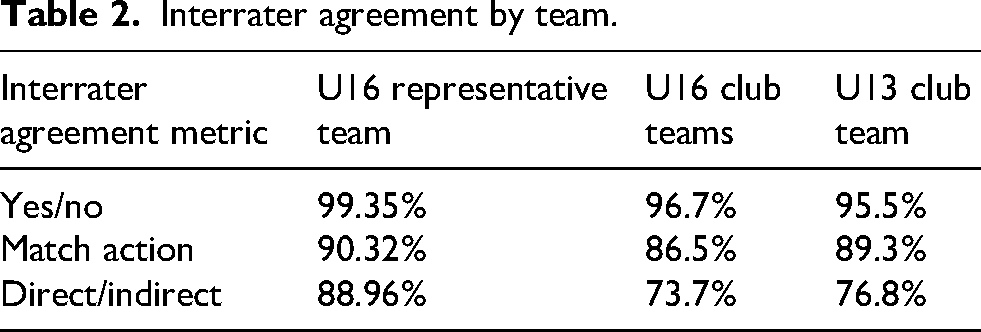
Expert reviewers were used to obtain inter-rater reliability for HAE verification (‘yes’ or ‘no’), indirect or direct head contact and match action (breakdown, tackle or other). This was calculated using the following formula: (agreements/(agreements + disagreements)) × 100%. The interrater agreement for verification of HAEs as ‘yes/no’, match action and ‘direct/indirect’ for the three teams can be seen in Table 2.
Interrater agreement by team.
A chi-square test was used to assess the differences in proportions between the different tackle directions and two-way chi-square tests were used to assess the differences in proportions between tackle direction and the other variables. Two-way ANOVAs were conducted to compare PLA and PRA magnitude across tackle directions (front on, side on and behind) within categories such as anticipation, match action and position. Post-hoc Tukey HSD tests were used to explore the source of the differences in the means between conditions, except where there were only two groups and an independent-samples t-test was used. For all analysis, the critical α-level was set at 0.05.
Results
Overall tackle direction statistics
There were significant differences in the proportion of tackles from the front, side and rear of the ball carrier for each of the three teams with tackles from the front vastly outnumbering tackles from the side and rear (see Table 3; U13: χ2 (2, N = 493) = 223.94, p = <0.001. U16 club: χ2 (2, N = 1810) = 554.287, p = <0.001. U16 reps: χ2 (2, N = 236) = 187.067, p = <0.001).
Tackle direction numbers and proportions by team.

PLA = peak linear acceleration; PRA = peak rotational acceleration; m = mean; SD = standard deviation; IQR = interquartile range.
One-way ANOVAs revealed a significant difference across tackle directions for PLA for the U16 club players (F 2, 1563) = 3.047, p = 0.048). Post-hoc Tukey's HSD tests for multiple comparisons found that the mean PLA for rear was significantly lower than for side tackles for the U16 club players (mean difference (MD) = 3.25 g, 95% confidence interval (CI) = 0.15–6.34 g, p = 0.037).
Anticipation and tackle direction
Descriptive statistics of HAE incidence/magnitude for anticipation with tackle direction can be seen in Table 4. There were no significant two-way ANOVAs for tackle direction and anticipation. Post-hoc Tukey's HSD tests for multiple comparisons found significance for good vs poor anticipation in both the U13 and U16 club teams for both PLA (U13: MD = 5.08 g, 95%CI = 1.02–9.13, p = 0.007. U16 club: MD = 9.4 g, 95%CI = 7.35–11.45, p = <.001) and PRA (U13: MD = 593.04 radians/s2, 95%CI = 131.10–1054.98, p = 0.006. U16 club: MD = 882.35 radians/s2, 95%CI = 693.32–1071.39, p = <.001).
HAE incidence/magnitude for tackle direction and rugby specific factors.
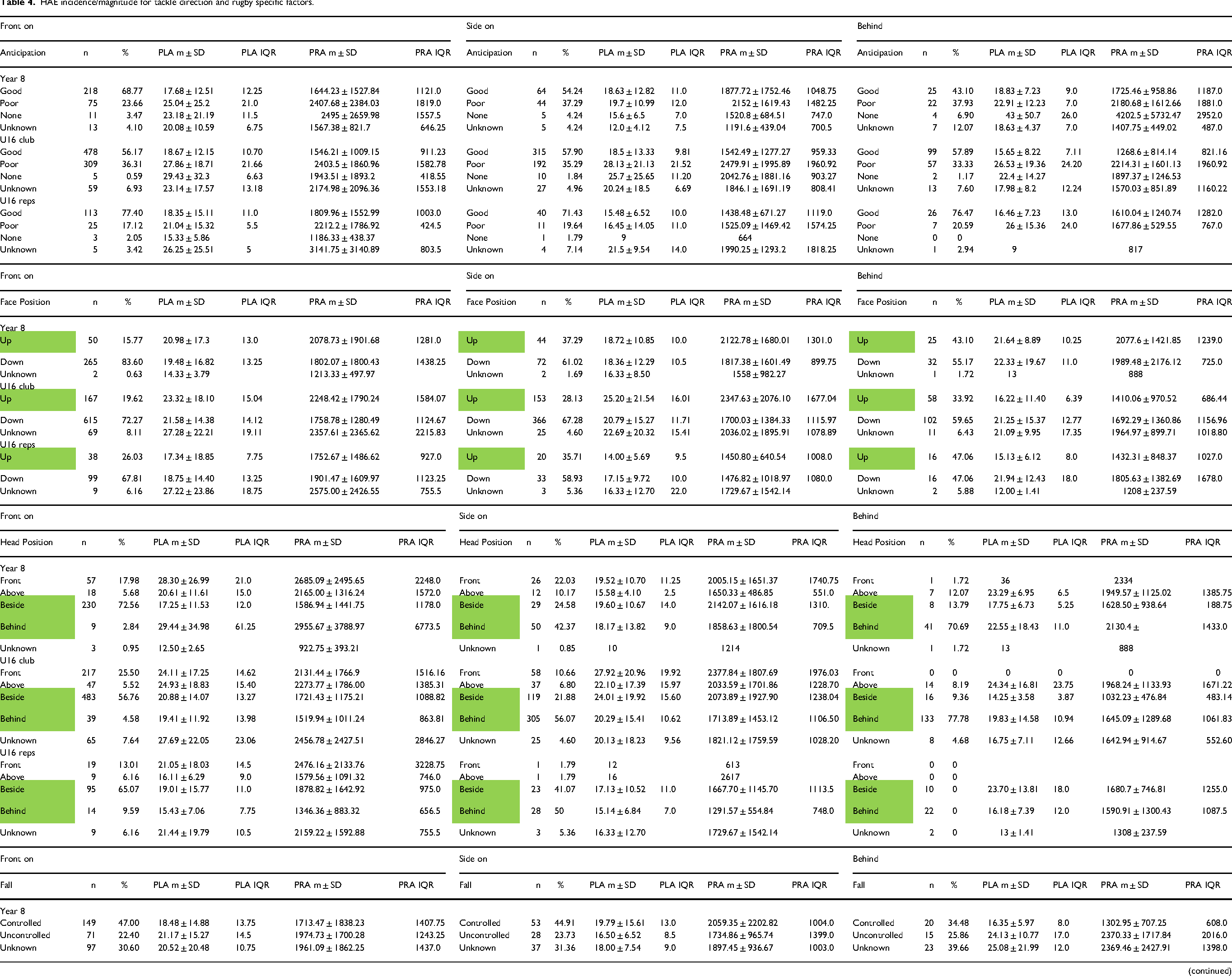
Notes: PLA = peak linear acceleration, g; PRA = peak rotational acceleration, radians/s2; m = mean; SD = standard deviation; IQR = interquartile range; green highlights indicate recommended tackle technique
There were significant differences in the proportion of anticipation levels in the U13 data (χ2(6, N = 493) = 25.53, p = <.001) with front-on tackles having ‘good’ anticipation 14.53% more often than side-on and 25.67% than tackles from behind.
Falling and tackle direction
Descriptive statistics of HAE incidence/magnitude for falling with tackle direction can be seen in Table 4. There were no significant two-way ANOVAs for tackle direction and falling. Post-hoc independent-samples t-tests revealed significant differences for PLA (t1164 = 6.025, p = <0.001, MD = 6.95 g, 95%CI = 4.92–8.98) and PRA (t1164 = 6.025, p = <0.001, MD = 566.41 radians/s2, 95%CI = 381.94–750.89) for the U16 club players when falling was controlled versus uncontrolled.
Head position and tackle direction
Descriptive statistics of HAE incidence/magnitude for head position with tackle direction can be seen in Table 4. There were no significant two-way ANOVAs for tackle direction and head position. Post-hoc Tukey's HSD tests for multiple comparisons found significance for front vs beside for the two club teams for PLA (MD = 8.07 g, 95%CI 2.85–13.29, p = <0.001. U16 club: MD = 3.57 g, 95%CI = 0.53–6.61, p = 0.014) and PRA (U13: MD = 815.13 radians/s2, 95%CI = 218.49–1411.77, p = 0.002. U16 club: MD = 408.55 radians/s2, 95%CI = 129.58–687.52, p = <0.001), and for front vs rear for the U16 club team for PLA (U16 club: MD = 4.90 g, 95%CI = 1.72–8.07, p = <0.001) and PRA (U16 club: MD = 506.25 radians/s2, 95% CI = 215.25–797.24, p = <0.001).
There were significant differences in the proportion of head position in the U13 data (χ2(8, N = 499) = 219.26, p = <0.001), U16 club (χ2(8, N = 499) = 743.55, p = <0.001) and U16 reps (χ2(8, N = 240) = 96.42, p = <0.001).
Face position and tackle direction
Descriptive statistics of HAE incidence/magnitude for face position with tackle direction can be seen in Table 4. There were significant two-way ANOVAs for tackle direction and face position for the U16 club data for both PLA (F (2, 1563) = 4.009, p = 0.018) and PRA (F (2, 1563) = 4.713, p = 0.009). An independent samples t-test for face-up vs face-down found face-up tackles had significantly higher PRA in the U16 club data (t1453 = 4.799, p = <0.001, MD = 429.41 radians/s2, 95%CI = 253.87–604.95).
There were significant differences in the proportion of face positioning in the U13 data (χ2(4, N = 503) = 36.89, p = <0.001) and U16 reps data (χ2(4, N = 240) = 35.53, p = <0.001).
Tackle direction and high magnitude collisions
Using World Rugby's adult male HIA standard of 75 g/4500 radians/s2 to establish a high magnitude HAE threshold, we see the U13 and U16 reps players having most come from front on collisions and the U16 club players having a relatively even mix of front and side collisions resulting in HIA-level HAEs (see Table 5). Chi-square tests reveal significant differences in the proportions of tackle directions resulting in HAEs exceeding the 75 g/4500 radians/s2 HIA triggering thresholds for the U13 (χ2 (2, N = 10) = 9.80, p = 0.007), U16 club (χ2 (2, N = 26) = 7.93, p = 0.019) and U16 reps (χ2 (2, N = 10) = 6.40, p = 0.011).
Head injury assessment and 25 g/2000 radians/s2 threshold head acceleration events.
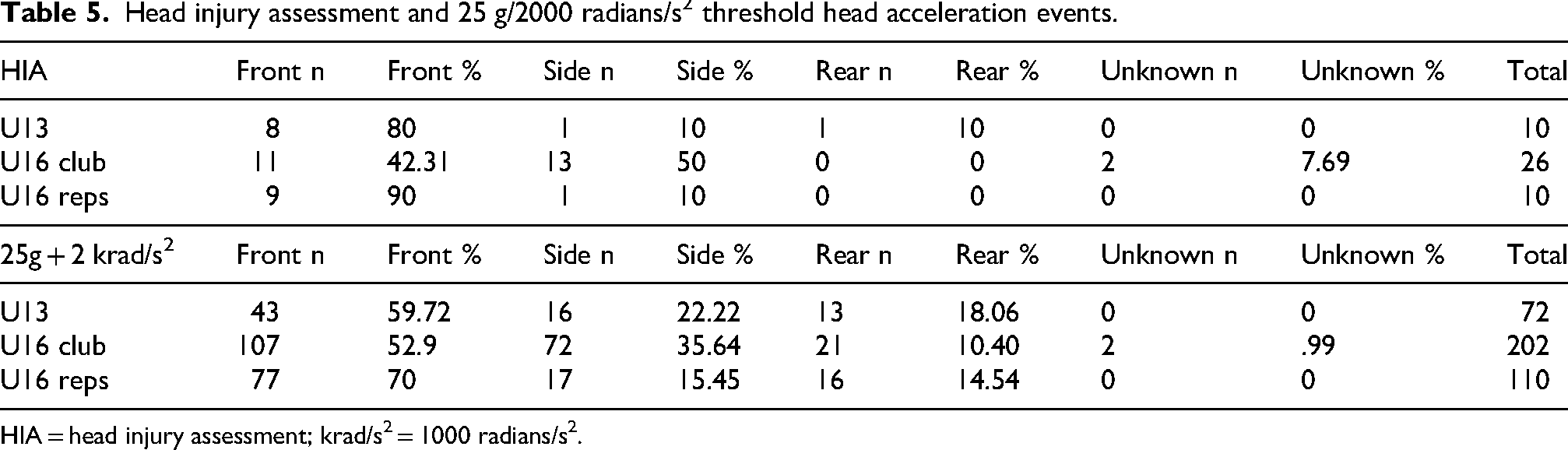
HIA = head injury assessment; krad/s2 = 1000 radians/s2.
Using a moderate, but still above average threshold we see similar data to the HIA threshold but with slightly more rear tackles. Chi-square tests revealing significant differences in the proportions of tackle directions resulting in HAEs exceeding 25 g/2000 radians/s2 for the U13 (χ2 (3, N = 202) = 136.18, p = <0.001), U16 club (χ2 (2, N = 72) = 22.75, p = <0.001) and U16 reps (χ2 (2, N = 110) = 66.56, p = <0.001).
Discussion
This study aimed to examine proportions of tackles from different directions and how that affected HAE magnitudes as well as impact anticipation, falling, head position and face position. While previous HAE/iMG studies have examined tackle height,46,62 this is among the first studies to utilize HAE field data from matches to examine different elements of rugby such as tackle direction and impact anticipation across different age and skill levels of youth rugby. This study continues to accumulate HAE data in youth rugby and provides information for coaches with potential implications to mitigate HAE exposure in youth rugby players.
The key findings of this research are that most rugby tackles are approached from the front of the ball carrier and tackle direction makes no significant difference in HAE magnitude with regards to anticipation, falling and head position. Additionally, while the overwhelming majority of HAEs were found to be low in magnitude, the tackler having poor anticipation and placing the head in front of the ball carrier's body were both found to play significant roles regardless of tackle direction in HAE magnitude in the different teams, as has been seen in previous research.19,63
Overall tackle direction statistics
Most tackles seen in the three teams in this study occurred with the tackler approaching the collision front on and there was no obvious trend across the teams of differences in magnitude based on tackle direction. Unlike Seminati et al. 50 who found higher impact forces in front-on tackles in adult male rugby players, our results had no significance with regards to front vs side-on tackles. Our only significant difference for tackle direction was in the U16 club data with higher PLA for side-on than rear tackles, however no comparison can be made with Seminati et al. 50 as they did not conduct trials with tackles from the rear. Lower PLA/PRA would likely result from tackles from the rear as the tackler and ball carrier have a much smaller difference in velocity when direction is considered. 64 Tackles from the front and side would logically lead to a greater change in momentum of the tackler's head.
Anticipation and tackle direction
The two older teams had very similar anticipation numbers across all three tackle directions, while the U13 players had much better anticipation with front-on tackles. The U13 players’ worse anticipation for tackles from the rear could be due to a lack of experience/expertise65–67 and anecdotally from a lack of coaching and training experience in tackles from the rear. Coaches may want to spend additional time coaching tackles from the side and particularly the rear with younger players as they have worse anticipation when tackles are not front-on.
Head position and tackle direction
All three teams showed significantly higher rates of proper head positioning from the rear and mixed results from the side/front, which is reasonable considering it's difficult to get one's head around the ball carrier from behind. The U16 reps players had higher rates of proper head positioning during side-on and front-on tackles than both the U13 and U16 club players (there was only one tackle from behind across the three teams which had a head position in front). This increased rate of proper technique could be a consequence of their higher skill with Stockwell et al. 55 finding tackles with the ‘head across the bow’ (‘head across and in front of’ the ball carrier's body, per their study's operational definition) being successful 64.8% of the time versus 98.0% for tackles with the head beside the ball carrier (or ‘inside the shoulder) in American football. This proper head positioning can also play a significant role in reducing HIA-level HAEs 52 and concussion risk.36,68
Face position and tackle direction
While tackle direction made no significant difference, face-up tackles in general had significantly higher PRA in the U16 club data, which goes against recommended tackle technique. Spriggs et al. 54 also found higher PRA with face-up tackles and that players mostly tackled with their face down. As noted by Brague et al., 69 a face down position creates a rigid structure from the head and through the neck/spine, increasing stability of the head and cervical spine and which may attenuate force imparted to the head. As we recommend in Spriggs et al. 54 coaching a face-up position during the pre-contact phase of a tackle allows for visual feedback, then adopting a face-down position prior to contact maintains a more stable spinal posture that can better absorb impact energy.
Front-on tackles had significantly higher rates of face-down positioning than from the side and particularly rear in the U13 and U16 reps teams. This is in line with Posthumus and Viljoen who specifically recommend a face up position for side on tackles. 44 Future studies should consider not only face position, but also spinal positioning to see if these tackles from the side and rear with the face up have proper spinal alignment.
Tackle direction and high magnitude collisions
More tackles exceeding the HIA threshold occurred particularly from the front, but also the side than the rear. The side tackles exceeding the HIA threshold were almost exclusively found in the U16 club data, which may reflect different coaching and/or player technique/ability versus the U16 reps as well as anthropometric differences with the U13 players. While the HIA thresholds have been established for adult players based on elite adult data, they have been established as meaningful to the rugby community for both ‘recognize and remove’ decision-making70–72 and as readily understood by players, coaches and fans. As noted in the introduction, previous research has mixed findings regarding tackle direction and injury risk/impact force. Our HIA-level HAE results align with Seminati et al. 50 who found tackling from the front resulted in higher impact force and head acceleration forces with a tackle simulator, Tucker et al. 46 who found increased injury risk with tackles from the front and Sherwood et al. 68 who found no concussions with tackles from behind in an NFL study, but disagree with previous rugby studies.19,47–49
Practical applications
While tackling from the side/rear has been recommended by coaching initiatives, it has been posited that ball carriers are at an increased risk of injury with tackles outside of their field of vision 41 as they cannot make appropriate anticipatory postural adjustments. 73 Improving impact and general anticipation through deliberate practice may be most helpful during childhood and adolescence, so the age groups of this study represent profound times for coaches to implement programs to improve this anticipation.74,75 Based on this study, the official recommendation of tackling with the face up appears to be best for reducing PLA/PRA in tackles from the rear, while the recommendation of Spriggs et al. 54 of face down tackling appears to be best for reducing PLA/PRA in front-on tackles and more research is needed to determine if there is an optimal face position for side-on tackles. While this paper has focused on tackling technique, ball carriers should also be encouraged and coached to have a greater awareness of the field and dynamic flow of gameplay. 41
Limitations & avenues for future research
The sample of tackles from the U16 reps team was much smaller than the other two teams, likely due to it being a shorter season taking place after the longer club season. However, it should be noted that significant anticipation from all elements of rugby, not just tackling, and head position findings have been previously seen in this dataset. 19
This study must be viewed in light of the inherent limitations of iMGs, notably linear acceleration bias, tackles that were missed due to the 8 g recording threshold and player compliance. It should be noted that all participants wore the iMGs every game within the season, however false negatives may have occurred with re-triggering times during complex tackles and mouthguard faults may have resulted in some data loss. While the analysts were trained and experienced in coding, this cannot be considered a perfect process and ongoing training will help facilitate high reliability in future studies.
This study did not consider performance metrics such as tackle success rate and rate of preventing offloads; players and coaches may be more likely to take heed of specific techniques designed for player safety if they also improve performance or at least do not hinder competitive success. To borrow from a concept from cutting/change of direction research, there may exist a ‘performance-injury conflict’76,77 which must be considered when making concussion/head injury prevention recommendations that may have performance decrements.
Future research should be conducted with boys and girls rugby players in other regions and countries to examine how different playing/coaching styles as well as gender differences impact tackle techniques and head kinematics. Future tackle direction and general tackle research should consider known risk factors like speed,45,48,49,68 dominant or recessive shoulder tackles, 50 head axis of rotation, 78 location of impact on the head,36,79 step pattern preceding contact, 52 inter-individual differences in brain anatomy, 80 repetitive head contact, 81 previous concussion 82 and impact location on the body. 46
It is notable that between the two U16 teams, the more highly skilled reps team had better rates of good anticipation and had lower PLA, but not PRA across all three tackle directions. Perhaps this speaks to their skill and that they can anticipate contact better and make anticipatory adjustments that limit PLA. Future research should seek to explain why this is not also true for PRA. Additionally, more research is needed for anticipation in youth sports in general 74 and how to improve youth athletes’ ability to anticipate sport-specific situations particularly with regards to impact anticipation in contact sports.
Footnotes
Acknowledgements
We thank Simon Felton, Ross Keenan, Nick Palmer, Sarah Green, and Jacob Cameron at Pacific Radiology for the expertise in setting up and running the MRI protocol; Damien Hawes, Jeremy Smith, and Alex Patchett at HitIQ for the expertise and trouble-shooting of instrumented mouthguards; Donna Batchelor and the team at Donna Batchelor Orthodontist for their expertise in conducting 3D dental scans for the participants; and the coaches, players, parents, and staff at NZ Rugby, Crusaders Rugby, Canterbury Rugby Football Union, Ellesmere Rugby Sub-Union, Lincoln Rugby Football Club, and Waihora Rugby Football Club for their support of the research.
ORCID iDs
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The project was funded by the Canterbury Medical Research Foundation, Pacific Radiology, Maurice and Phyllis Paykel Trust and Cure Kids.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
Data are available on reasonable request to the corresponding author.