
Abstract
A growing body of evidence suggests that repetitive head acceleration events (HAEs), even in the absence of diagnosed concussion, could have implications for long-term neurological function. This study aims to determine the on-field validity of instrumented mouthguards (iMGs) in American football and to quantify HAE incidence in NCAA football players. Instrumented mouthguards were fitted to 35 male NCAA football players. Head kinematic data were collected during 68 player matches. On-field validity was determined through video review with positive predictive value (PPV) and sensitivity values calculated. HAE incidence was calculated as the number of HAEs per player match and stratified by Offense and Defense positions. On-field validity of the Prevent Biometrics iMG in NCAA American Football indicates a sensitivity of 0.89 and PPV of 0.98 based on false positive definitions. The mean incidence of HAEs above a range of peak linear acceleration (PLA) and peak angular acceleration (PAA) thresholds in Defense and Offense appear similar. The incidence of HAEs above 10 g was 11.2 and 11.3 HAEs per player match for Defense and Offense, respectively, while PAA incidence above 1.0 krad/s2 was 5.5 and 6.9 HAEs per player match for Defense and Offense, respectively. Incidence of HAEs above 30 g was 1.6 and 2.6 per player match and 0.9 and 1.4 for HAEs above 2.0 krad/s2 for Defense and Offense, respectively. The Prevent Biometrics iMG appears suitable for measuring HAEs in elite American football and benchmark HAE incidence in elite American Football lays a foundation for the development HAE mitigation strategies.
Introduction
American football is a high-impact contact sport characterised by frequent collisions during tackles, runs, blocks, and other physical confrontations.1,2 As a result, players are at an increased risk of head injuries, including concussions. 3 Several studies in sport have explored risk factors for concussion4,5 and various rule changes have been implemented in elite American Football to mitigate concussion risk and improve diagnosis and recovery protocols. 6 However, a growing body of evidence suggests that repetitive head acceleration events (HAEs), even in the absence of diagnosed concussion, could have implications for long-term neurological function.7–9 This raises significant concerns about the long-term health implications for American football players, particularly as the sport is known for the high number of HAEs that players are exposed to during games and practices. 10 In American Football, inertial head loads can be of similar magnitude to direct helmet impacts, suggesting that players may experience substantial HAEs during gameplay that are not easily detected. 10 One feature of American football is the unique nature of each player position on the field. Measuring the incidence of HAEs is an important step to understanding the exposure of players across various positions, which may inform tailored risk-mitigation strategies to protect player brain health.
In the past, in-vivo head kinematic data has been collected using helmet-based or skin sensors which are prone to artifacts from sensor movement relative to the head. 11 However, the development of instrumented mouthguards (iMGs) has allowed for more accurate and reliable measurement of both linear and rotational head kinematics, with iMGs offering rigid coupling to the skull via the upper dentition, producing valid and reliable measurement of linear and rotational head kinematics.11–13 The application of iMGs in sport provides a unique opportunity to measure HAEs during on-field match play and has previously been undertaken in sports such as American football, rugby, and soccer.14–17 The Prevent Biometrics iMG (Minneapolis, MN, USA) has been previously validated in laboratory for helmeted and unhelmeted head impacts as well as on-field in the un-helmeted sport of rugby.12,13,18 Jones et al. 12 undertook a large-scale validation and feasibility study of multiple iMG systems and indicated that the Prevent Biometrics iMG scored highest for player fit, function and comfort, laboratory-based impact testing using a crash test dummy headform (concordance correlation coefficient value of 0.98) and on-field in rugby with a positive predictive value (PPV) of 0.94 for detecting on-field HAE. Furthermore, Tooby et al. 19 found that applying a combined iMG recording threshold of 5 g (at head centre of gravity) and 400 rad/s2 improved PPV to 0.99 (95% CI: 0.97-1.00), yielding a sensitivity value of 0.86 (95% CI: 0.84-0.89) for direct head impacts. The FRI-Biocore iMG system evaluated by Jones et al. 12 achieved a PPV of 0.98 and sensitivity of 0.82 in an American football-based validation study. 15
While Prevent iMG performance has been studied extensively in rugby, differences in helmet use, impact mechanisms, and pulse durations in American football could influence device performance. This study aims to evaluate the context-specific on-field validity of the Prevent Biometrics iMG in NCAA Division I American football and quantify the incidence of HAEs across Defense and Offense player positions. The findings provide a benchmark assessment of HAE exposure in elite American football and lay the foundation for future position-specific interventions aimed at reducing HAE burden and enhancing player safety.
Methods
A prospective observational cohort study was conducted using data from an NCAA Division 1 American Football team during the 2022 Mountain West Conference Regular Season. Thirty-five players were fitted with iMGs (Prevent Biometrics, Minneapolis, MN, USA). Participation was voluntary, and ethical approval was obtained from the University of Nevada Institutional Review Board (No. 1757959-5) and in accordance with the Declaration of Helsinki.
All iMGs were custom fit following three-dimensional dental scans with a dental assistant under the supervision of a certified dentist. The iMGs are equipped with triaxial gyroscopes and accelerometers sampling at 3200 Hz with a measurement range of +/−35 rad/s2 and +/−200 g, respectively. 20 HAEs were identified when linear acceleration exceeded an 8 g trigger threshold on any single axis of the iMG accelerometer. Linear acceleration was then transformed to the head centre of gravity. Time series data for HAEs were captured 10 ms prior and 40 ms after the trigger event, with a recording threshold of 5 g of resultant peak linear acceleration (PLA) and resultant peak angular acceleration (PAA) of 400 rad/s2 at the head centre of gravity.16,21 The degree of noise/artifact in each data signal was classified by a Prevent Biometrics proprietary algorithm as minimal (class 0), moderate (class 1), or severe (class 2). A 4-pole (2 × 2), zero-phase, low-pass Butterworth filter was applied to each kinematic signal, similar to previous studies.19,21 A 200 Hz, 100 Hz and 50 Hz cut-off frequency (−6 dB) were applied to class 0, class 1, and class 2 signals, respectively. 20 Proximity sensor readings were collected to ensure that iMGs were seated to the player's dentition during HAEs.19,21 NCAA footage was collected from mainstream television broadcasters, and all video analysis was performed by a trained video analyst with over 6 years of experience.22–24
The sample comprised of 35 players participating in a total of 68 player matches (games) across 4 games. The validation protocol was utilised from Jones et al. 12 All video analysis was conducted using QuickTime Player v.10.5 on a 32” monitor. The reviewer was permitted to pause, rewind, and zoom as needed. First, an unguided video analysis of all footage was performed with the reviewer blinded to all iMG data. The reviewer looked for instances of direct and visible contact to the head during gameplay, affecting any players actively wearing iMGs. The video time of each event was recorded in a list, organised by player and match. A total of 517 head impacts were identified in the unguided video analysis. Proximity sensor readings were used to exclude any recorded events where the players’ iMG was ‘off the teeth’ (n = 31). All events that did not meet the 5 g and 400 rad/s2 threshold were also excluded (n = 32). As such the sample size for unguided analysis was 454 impacts.
Next, the iMG data was synchronised with the video footage to ensure frame-to-frame synchronisation similar to Jones et al.
12
The iMG dataset was cross-referenced with the list of head impact events from the unguided video analysis. Each event with a corresponding iMG-triggered event was designated a True Positive and any event without was designated a False Negative. Sensitivity with a 95% confidence interval (CI) was calculated (Eq. 1).

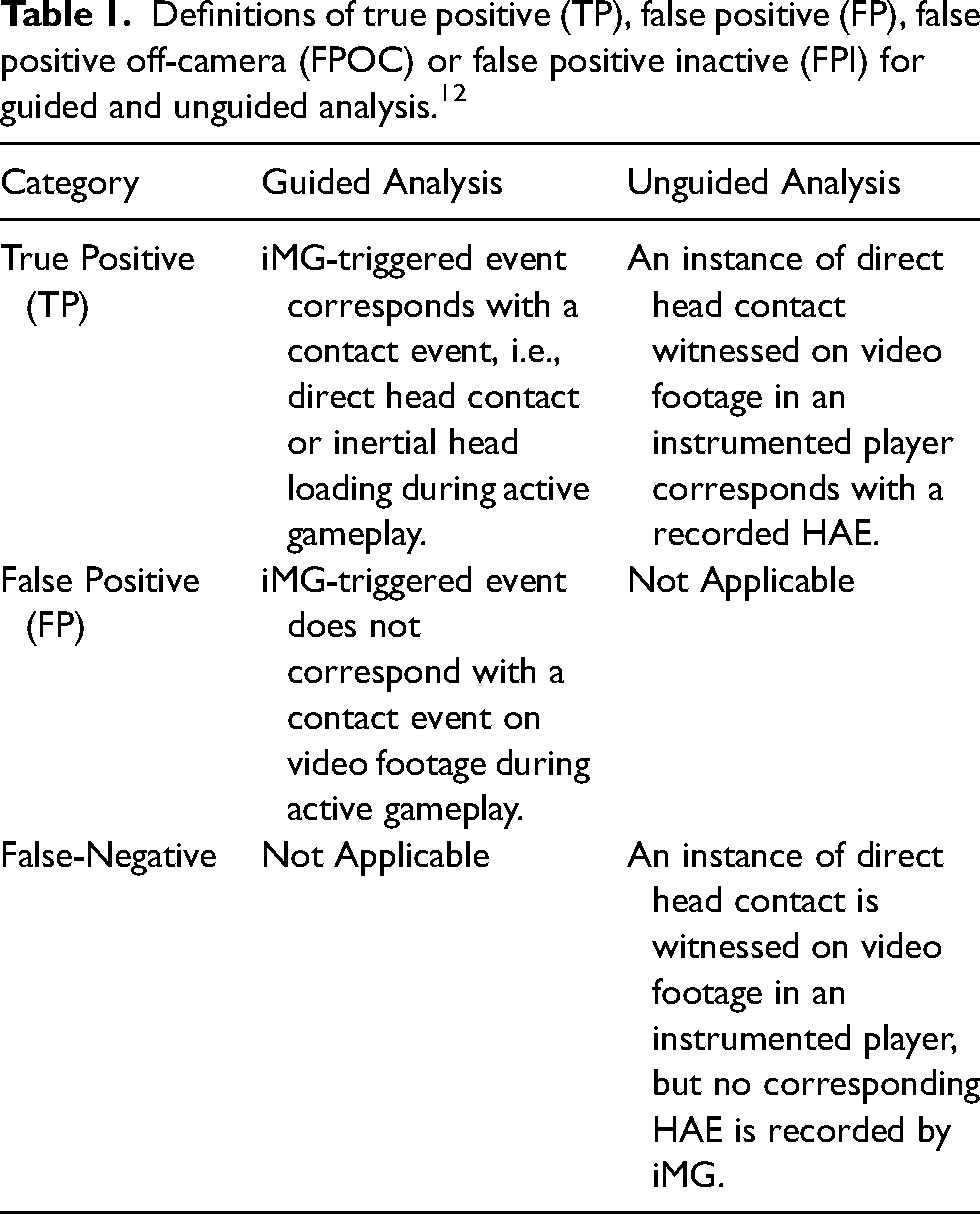
For the guided analysis, there were a total of 847 iMG triggered events that met the 5 g and 400 rad/s2 recording threshold. Each of these iMG triggered events was cross-referenced with the video footage and designated as either True Positive (TP) or False Positive (FP) based on the definitions in Table 1.
12
PPV analyses and classified as unverifiable. Positive predictive values (PPVs) with 95% CI were calculated based on TPs and FPs (Eq. 2). iMG-triggered events occurring off-camera or inactive gameplay were not included in the analysis.

Definitions of true positive (TP), false positive (FP), false positive off-camera (FPOC) or false positive inactive (FPI) for guided and unguided analysis. 12
Only true positive iMG-triggered events (i.e., HAEs) that met the 5 g and 400 rad/s2 threshold were used in the incidence calculations. Proximity sensor data confirmed that iMGs were being worn during each analysed event. Only player matches where the instrumented player wore the iMG for at least 90% of their contact events were used (n = 58, 90.1%) in the incidence calculations.19,21 The approach produced a total of 828 HAEs, and 58 eligible player matches over 4 games. Data for the incidence analysis consisted of individual HAEs recorded across Defense and Offense positions. Positions were consolidated for analysis. Offensive positions comprised Offensive Linemen (Centers, Guards, Long Snappers, and Offensive Tackles; n = 6), Running Backs (n = 2), and Tight Ends (n = 4), while Defensive positions comprised of Defensive Linemen (Defensive Ends and Defensive Tackles; n = 2), Linebackers (n = 14), and Defensive Backs (Safeties and Cornerbacks; n = 7).
Resultant peak linear acceleration (PLA) and resultant peak angular acceleration (PAA) were extracted from each HAE recorded. HAE Incidence was calculated as the number of HAEs per player match. Mean values for Offense and Defense were calculated across players and 95% CIs were estimated using a bootstrapping procedure. 19 The dataset was randomly resampled 2500 times and the 2.5th and 97.5th percentile of resampled means were used as the lower and upper bounds of CI, respectively. 19 Mean incidence along with 95% CIs, were calculated across a range of PLA and PAA magnitude thresholds for Offense and Defense and a significant difference was assumed if the CIs did not overlap. 19
Results
The total number of TP, FP and FN events with PPV and Sensitivity calculations are seen in Table 2. On-field validity of the Prevent Biometrics iMG in NCAA American Football indicates a sensitivity of 0.89 and PPV of 0.98 based on false positive and false negative definitions (Table 2). The incidence of PLA and PAA HAEs above a range of thresholds in Defense and Offense appear similar (Figure 1).
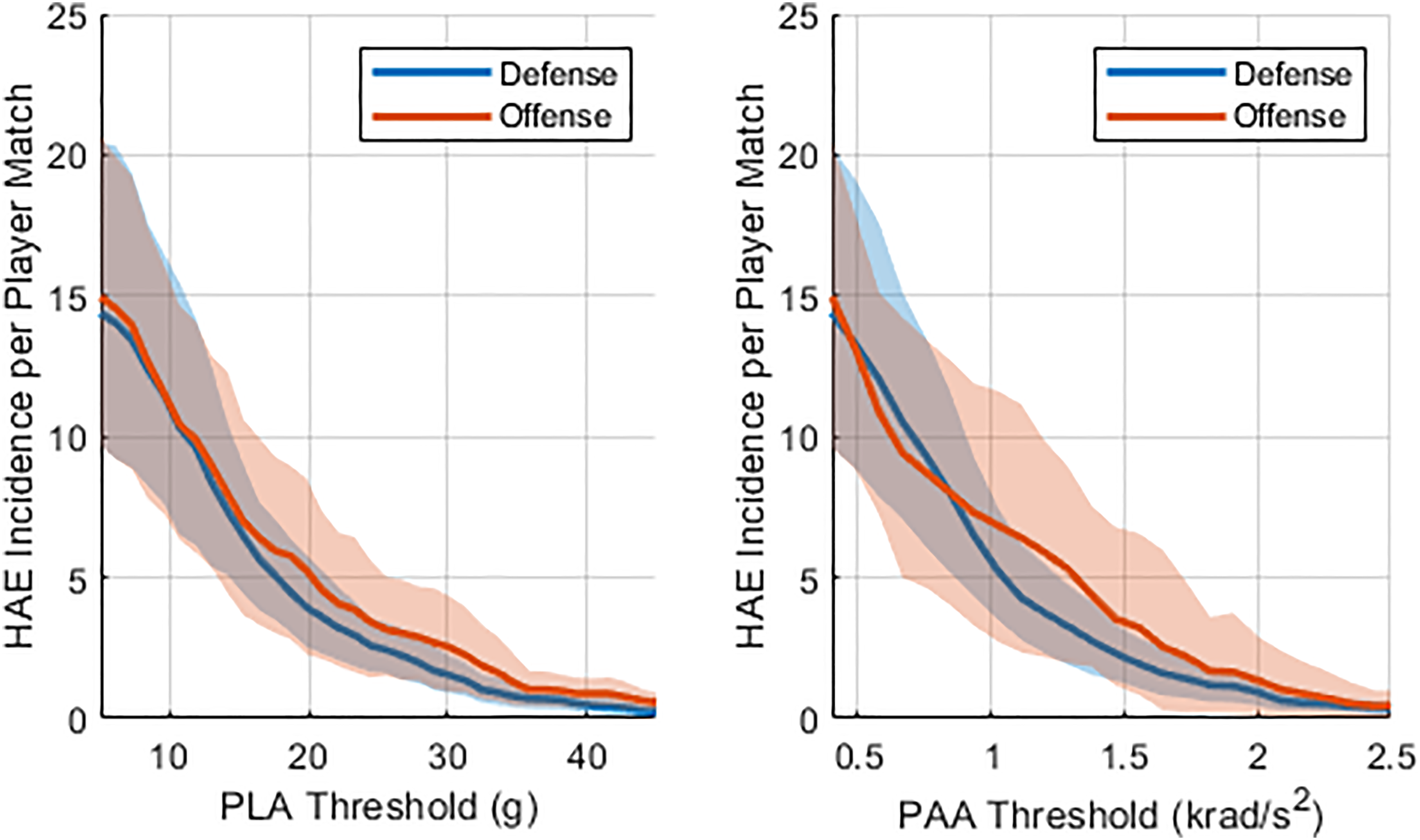
Incidence of HAEs for NCAA American football players for defense and offense positional groups.
On-field validity of the prevent biometrics iMG in NCAA football at recording threshold of 5 g and 400 rad/s2.
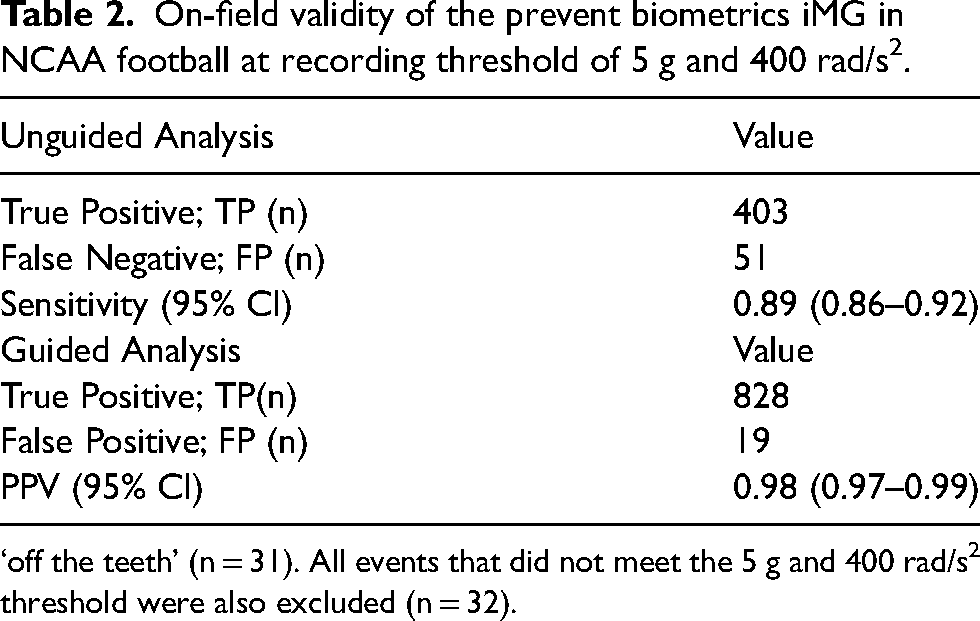
‘off the teeth’ (n = 31). All events that did not meet the 5 g and 400 rad/s2 threshold were also excluded (n = 32).
The overall incidence of HAEs above our recording threshold of 5 g and 0.4 krad/s2 was 15.0 and 14.4 HAEs per player match for Defense and Offense, respectively. HAE incidence greater than a PLA of 10 g was 11.2 and 11.3 for Defense and Offense, respectively. Above 20 g, HAE incidence was calculated at 5.2 and 3.9 HAEs per player match for Defense and Offense, respectively. Incidence of HAEs above 30 g was 1.6 and 2.6 HAEs per player match, while above 40 g we calculated an incidence of 0.9 and 0.5 HAEs per player match, for Defense and Offense, respectively. HAE incidence above 1.0 krad/s2 was 5.5 and 6.9 HAEs per player match, for Defense and Offense, respectively. Above 2.0 krad/s2, an incidence of 0.9 and 1.4 HAEs per player match was calculated for Defense and Offense, respectively. Above 3.0 krad/s2, incidence fell to 0.04 and 0.07 HAEs per player match for Defense and Offense, respectively.
Discussion
Previous studies have validated the accuracy of the Prevent Biometrics iMG in both laboratory and on-field settings. In rugby, similar on-field video-verification validation studies using the Prevent iMG produced comparable results. Jones et al. 12 reported a PPV of 0.94 (95% CI 0.92-0.95; no recording threshold applied) which was comparable to 0.98 (95% CI 0.97-0.99) in the current study. Tooby et al. 19 applied the same 5 g and 400 rad/s2 recording threshold as in the present study and reported a PPV of 0.99 (95% CI 0.97-1.00). The sensitivity value of 0.89 (95% CI 0.86-0.92) in the current study resembled rugby data presented by Jones et al. 12 and Tooby et al. 19 who reported 0.75 and 0.86, respectively. The findings are also similar to the FRI-Biocore iMG system that achieved a PPV of 0.98 and sensitivity of 0.82 in American football. 15 Our data support the validity of the Prevent iMG in detecting head acceleration events (sensitivity, specificity) in NCAA American football.
HAE incidence per player match provides an approximation of player exposure to contact events on a match-to-match basis. HAEs above 30 g or 2.0 krad/s2, which have previously been considered higher magnitude, 19 were relatively rare. HAE incidence between Offense and Defense appeared similar. Offensive Linemen are typically some of the largest players on a team, predominantly responsible for protecting the Quarterback and creating running lanes.25,26 This can results in frequent, lower-speed collisions at a short range. In contrast, defensive backs are marginally smaller, more agile players who tackle fast-moving players like the running back.25,27 Somewhere in between these two roles is the Tight End, who can serve as a receiver, ball carrier, or blocker depending on the play.25,28 This likely exposes them to a mix of lower and high-speed impacts.
Research on concussion incidence in elite American Football has identified Tight End, Running Back and Cornerbacks as the most diagnosed, followed by Defensive Ends and Linebackers. 29 Offensive Tackles, Guards, Centers and Long-Snappers reported some of the lowest rates. The use of iMGs in sport compliments these findings by providing information on HAE frequency and severity that players can be exposed to over a playing career allowing potential risk mitigation strategies to be proactively implemented. 30
To reduce match HAE exposure in active players, approaches can aim to (1) reduce match exposure, (2) minimise the frequency of HAEs and (3) minimise the magnitude of HAEs. Optimising diagnostic techniques for both acute and chronic brain injury through protocol assessments and longitudinal cognitive evaluation will ideally include HAE exposure if it has the potential to be damaging. It is thought that susceptibility to concussion increases with increased HAE exposure. 31 Limiting full-contact reps in training 32 and emphasising safer tackling techniques, such as discouraging players from tackling with their helmet, would likely help reduce HAE exposure.4,33,34 iMGs offer a means of measuring HAE incidence and exposure, but the threshold at which intervention might be required remains unclear. Data collected from iMGs might be used to retrospectively evaluate cumulative exposure faced by players who suffer a concussion, prior to their diagnosis. Future research might also involve larger sample sizes of iMG data and evaluate HAE mechanisms across more granular positional groups, which could be used to create tailored mitigation strategies for each position and explore the effect of contact technique on HAE incidence and propensity.
A recent study on HAE in 243 American football players from the National Football League (NFL) and from D-I of the National using a different iMG system was conducted. 35 The study found no significant differences between leagues in the distribution of kinematic-based metrics across any of the position groups studied (p ≥ 0.320). For peak linear acceleration, the median (IQR) values for NFL and NCAA, respectively, were 17.2 g (9.3) and 17.0 g (8.6) for linemen, 20.7 g (13.8) and 20.0 g (13.5) for hybrid positions, and 21.0 g (17.0) and 20.8 g (15.5) for speed positions. 35
Similar to Jones et al., 12 a single rater was utilised for video verification. While experienced, an additional rater may have been beneficial to enable inter-rater agreement. Proximity sensor readings were used to exclude any recorded events where the iMG was ‘off the teeth’ (n = 31) in the unguided analysis. Given the length of time the iMG were ‘off the teeth’, it cannot be confirmed whether the player had removed the iMG or that it was still in the player's mouth and the sensor failed to detect a firm seating on the dentition. Assuming the latter would reduce the sensitivity to 0.83. The study method aligned with the current state of the art in rugby for threshold selection, according to Tooby et al. 19 Including ‘off the teeth’ in the sensitivity analysis along with the removal of the 400 rad/s2 threshold would have resulted in a sensitivity of 0.84. This study was of a limited sample size, spread unevenly across playing positions. Conducting HAE incidence analysis on the Gabler er al. 35 dataset would be beneficial and could allow more granular analysis on positional groups. Players switching positions temporarily, which happens occasionally in American Football, was not controlled for. The dataset was limited to HAEs recorded during match play and did not include training sessions where HAEs can occur. 32 The signal processing of noisy signals performed in-house by Prevent Biometrics and the proximity sensor data used to ensure rigid fit to the dentition have not been independently validated but used in similar studies.19,30 The findings are limited to the Prevent Biometrics iMG system. Signal processing methods such as HEADSport have been developed to enable data comparison across different iMG systems. 36 This study used only peak linear and angular head kinematics, which do not account for directionality or temporality (i.e., pulse duration) which may influence injury risk and/or HAE severity. Contact mechanisms (e.g., tackle technique) can influence HAE magnitude and should be a focus of future work. 37
Conclusion
iMGs were validated and subsequently used to quantify HAE incidence in elite NCAA American Football. The high sensitivity and PPV is comparable to un-helmeted sports such as Rugby, suggesting that the iMGs are suitable for use in American Football. Position-based variability in HAE incidence and magnitude highlights the need for tailored mitigation strategies, though offensive and defensive players showed similar overall rates. This study provides a benchmark assessment of HAE incidence in elite American Football. The data generated in this study lays a foundation for the development of position-specific interventions aimed at reducing HAE exposure. A more comprehensive understanding of the complex relationship between HAEs, concussion risk and long-term brain health is needed to pave the way for evidence-based strategies to enhance player safety and mitigate the risk of long-term neurological sequelae.
Footnotes
Acknowledgments
We thank the participating team for their cooperation and support in this study.
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: GT has previously received research funding from Prevent Biometrics.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.