
Abstract
Physical tests and subjective measures, such as readiness and wellness, aid in optimising training and recovery, however, many tools lack proper validation, risking inaccurate conclusions. This study explores physical testing and readiness practices in female football. A cross-sectional web-based survey was conducted among practitioners working with female footballers. The survey, consisting of five sections and 24 questions, examined three key areas: testing, wellness, and readiness. A total of 51 practitioners from professional, semi-professional, and academy levels completed the survey, detailing their use of testing and monitoring data. Strength, speed, and aerobic capacity were rated as “extremely important” for soccer performance. Strength and aerobic capacity were tested 2–3 times per season (41% and 59%, respectively), while speed was tested weekly (76%), often integrated with regular monitoring. Qualitative tools were used daily to assess wellness and readiness, with validated questionnaires (55% and 39%), self-developed questionnaires (43% and 37%), and informal conversations (37% and 41%) being the most common methods. Research on physical qualities in readiness is extensive, yet subjective measures are more widely used in practice, with significant variability in their application. Practitioners prioritize a player's “feel” over their readiness to “perform.”
Introduction
Female football is now having extraordinary growth in popularity and visibility, with millions of fans following matches. 1 This was highlighted during the 2023 FIFA Women's World Cup, with a record attendance of almost two million, up by more than 600,000 on the previous record. 2 Similarly, the levels of athleticism in female football have also been increasing. 3 This is in part due to the increasing professionalisation, improved training structures, and support now available to players. 4 Although this is a great step forward, research in the area of female football is still behind research in men's football,5,6 for instance, more information is needed about the difference between male and female football players from a testing point of view, readiness monitoring, training load management and obviously, about the impact of the menstrual cycle on football performance.7–9
Sport science staff play a central role in supporting female players by performing fitness testing, monitoring the response to training, and assessing the players’ readiness to perform.8,9 Commonly, strength and conditioning (S&C) practitioners perform sprint, jump, and aerobic capacity assessments. 10 Such objective data collected during testing batteries is used to inform training programs and injury prevention strategies, as well as to assess the effectiveness of these interventions. 11 However, the time available to develop and implement such programs and strategies can be a challenge for practitioners due to the high number of matches and travelling duties that players typically experience during the pre- and in-season periods.8,10 Objective non-fatiguing physical assessments (e.g., countermovement jump [CMJ] force-time characteristics) 12 and subjective assessments (e.g., single-item Athlete Reported Outcome Measures (AROMs) 13 are commonly used in combination or independently to quantify the training response and inform decision making. These tools are very important to quantify the readiness status of the players, for example, if they feel tired, sore or if they have an objective decrease in lower limb performance. 14 Practitioners can assess the players’ readiness with the aim of making informed decisions about an athlete's immediate needs from a training and performance perspective. 9 Examples of single-item AROMs typically incorporated within the concepts of readiness, health and wellness are fatigue, muscle soreness and sleep quality. These concepts are commonly monitored by practitioners in research and practice, however, at times they are used interchangeably, and their constructs overlap, which can lead to confusion and misinterpretation. To avoid this, recent publications suggested including wellness and health, considered as delayed onset muscle soreness (DOMS), sleep quality, fatigue, stress and mood, within the readiness's framework.9,15 Readiness was defined as “the state of being fully prepared to train and perform physically and mentally” (we direct readers to this review if interested in learning more about the framework on readiness). 9 The assessment of fitness is also clearly needed as a player with higher fitness is also likely to have a greater readiness to play compared with a less fit player. Since the measurement of fitness through formal testing batteries is difficult,8,10 practitioners also rely on the measurement of chronic training load to assess changes and/or trends in the data that can help them design training plans on either an individual or team scale. 14
The research undertaken in the area of fitness, readiness, and wellness in female football is limited. 9 Previous work has considered the physical qualities assessed by S&C coaches in female football 16 or readiness procedures, however, further investigation is needed to understand the methods used in practice. Together, physical tests, and subjective measures such as readiness, may provide a more complete picture of a player's overall health and performance, allowing teams to optimize training and recovery plans to help players reach their full potential. A major limitation of the subjective measures, typically used to assess wellness, is the extensive use of inadequately validated tools, with response options that are yet to be justified. 13 The validity, reliability and sensitivity of all testing and monitoring tools are of vital importance to practitioners to detect meaningful change. Understanding the methods coaches use in female football is the first step in designing practical solutions. 17 This will allow staff to make informed decisions around training and recovery. 9 Indeed, more information regarding this topic would help coaches and medical staff make informed decisions about training and recovery schedules and identify potential injury risks with female athletes. Therefore, the purpose of the present study is to investigate the physical testing and readiness procedures used in female football to better support the methodologies sport scientists implement around training and recovery.
Methods
Research design
This was a cross-sectional web-based survey. Data was collected and stored with QuestionPro (California, USA). The survey was voluntary, and no monetary incentives were provided. Inclusion criteria were if respondents were working in female football in a capacity that involved them collecting and utilising testing and monitoring data. The survey contained five sections, and twenty-four questions, and examined three concepts including testing, wellness, and readiness (Appendix 1). The order of the sections and questions was not randomized to prevent bias. Data was collected between August 2023 and March 2024. The survey was approved by the University of Suffolk (Ipswich, UK) research ethics committee (ethics code: RETH(S)23/031). All participants gave electronic informed consent prior to participation.
Subjects
A total of 53 practitioners (8 ± 6 yrs. of industry experience) participated in this study (Figure 1). 12 practitioners identified as women whereas most (n = 41) identified as men. Although most respondents were S&C or fitness coaches (n = 31), there were a few sport scientists (n = 12), sports therapists (n = 7), physiotherapists (n = 2), and one practitioner who didn’t report their job title. Most practitioners (n = 32) worked only with professional athletes, whereas some practitioners worked with professional and other teams (n = 7), Semi-Professional (n = 4), Semi-Professional and others (n = 1) or only Academy (n = 9). Most participants were from the UK (n = 28) while the rest of the respondents were from mainland Europe (Italy, Denmark, Norway, France, Portugal, and the Netherlands) (n = 19), the United States of America (n = 5), or Australia (n = 1). Participants were recruited through social media platforms and the authors’ professional networks. The sample size was maximised through chain sampling, whereby participants were encouraged to invite relevant persons within their networks.
Statistical analysis
Raw data were initially exported into Microsoft Excel (Excel 2021, Microsoft, Washington, USA). Frequencies were determined for each closed-ended question or Likert-type scale response, with many of the responses also presented as frequency plots. All participants were included in the final analysis. Therefore, regardless of whether a participant did or did not complete the survey in its entirety, their responses were considered. Data was considered in absolute counts and as a percentage of the total number of responses. The proportion of responses was assigned to the following qualitative terms, adapted from previous football survey studies; All = 100% of respondents; Most = ≥75%; Majority = 55% to 75%; Approximately half = 45% to 55%; Minority = 30% to 45%; Few = <30%. 18
Results
Importance of physical qualities
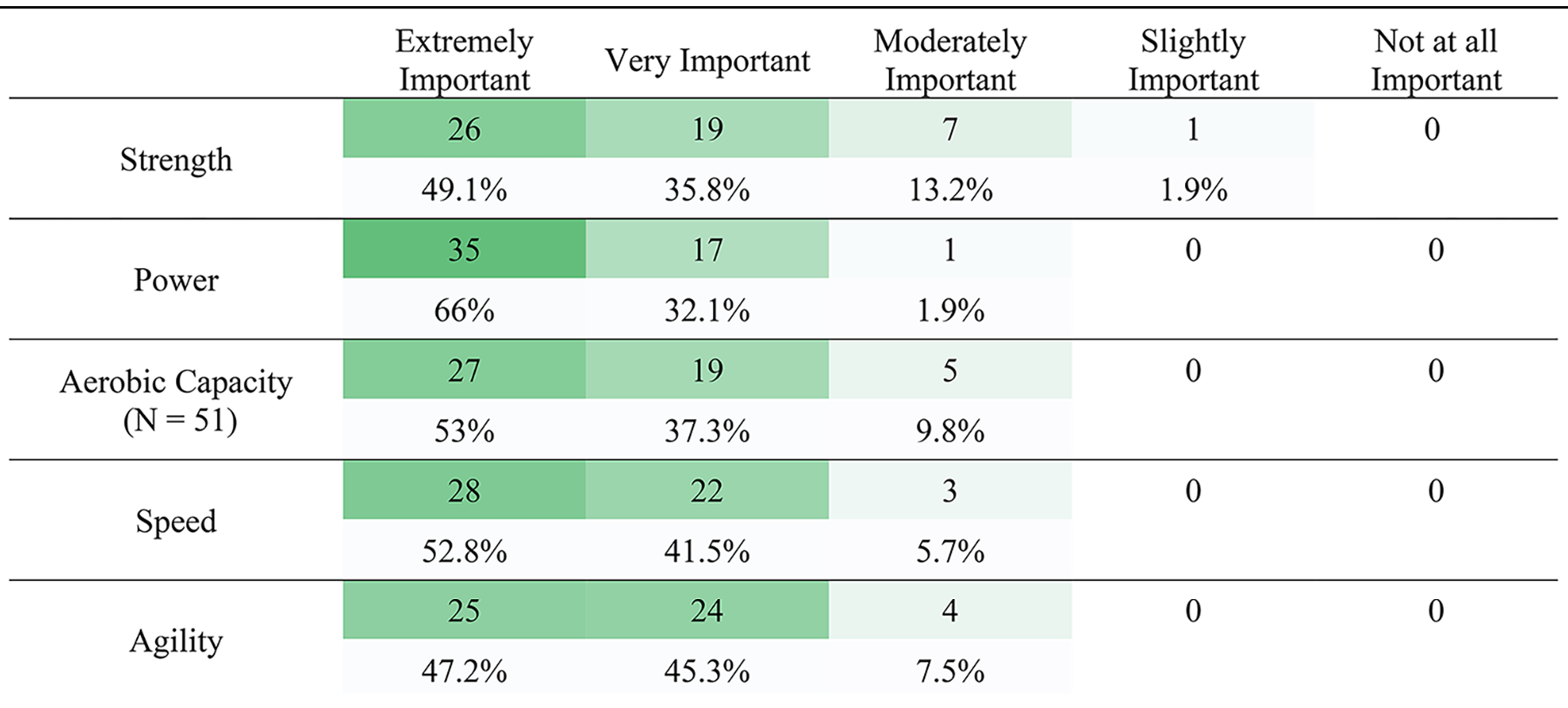
The majority of responders considered power to be “extremely important” compared to other physical qualities. “Approximately half” of respondents reported strength (49.1%), speed (52.8%), and aerobic capacity (53.0%) to be “extremely important” to soccer performance, with a similar split between “extremely important” and “very important” for agility (Table 1).
How would practitioners describe the following physical qualities for soccer performance? N = 53 unless stated otherwise.
Physical performance testing
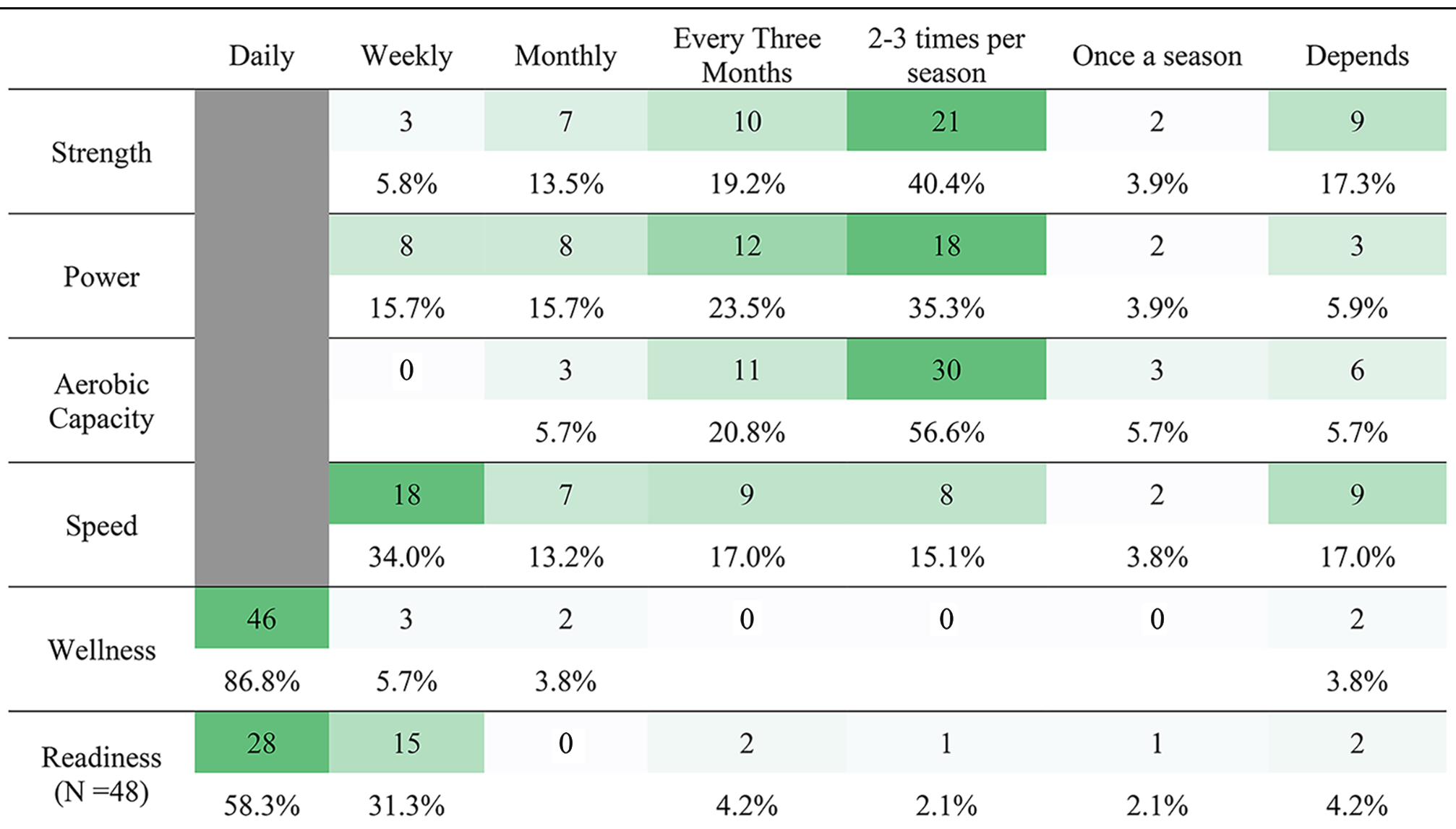
Physical qualities such as strength, power and aerobic capacity were most commonly assessed 2–3 times per season (40.4%, 35.3% and 56.6%, respectively), with speed most commonly assessed weekly (34%; Table 2). Interestingly, a “few” respondents reported that testing frequency for physical quality depends on other factors (5–20%; Table 2). Alternatively, Wellness was assessed daily by “most” (86.8%), and readiness was assessed weekly by “most” responders (58.3%).
Measurement frequency for all different physical qualities, wellness, and readiness.
Testing modalities, readiness and wellness
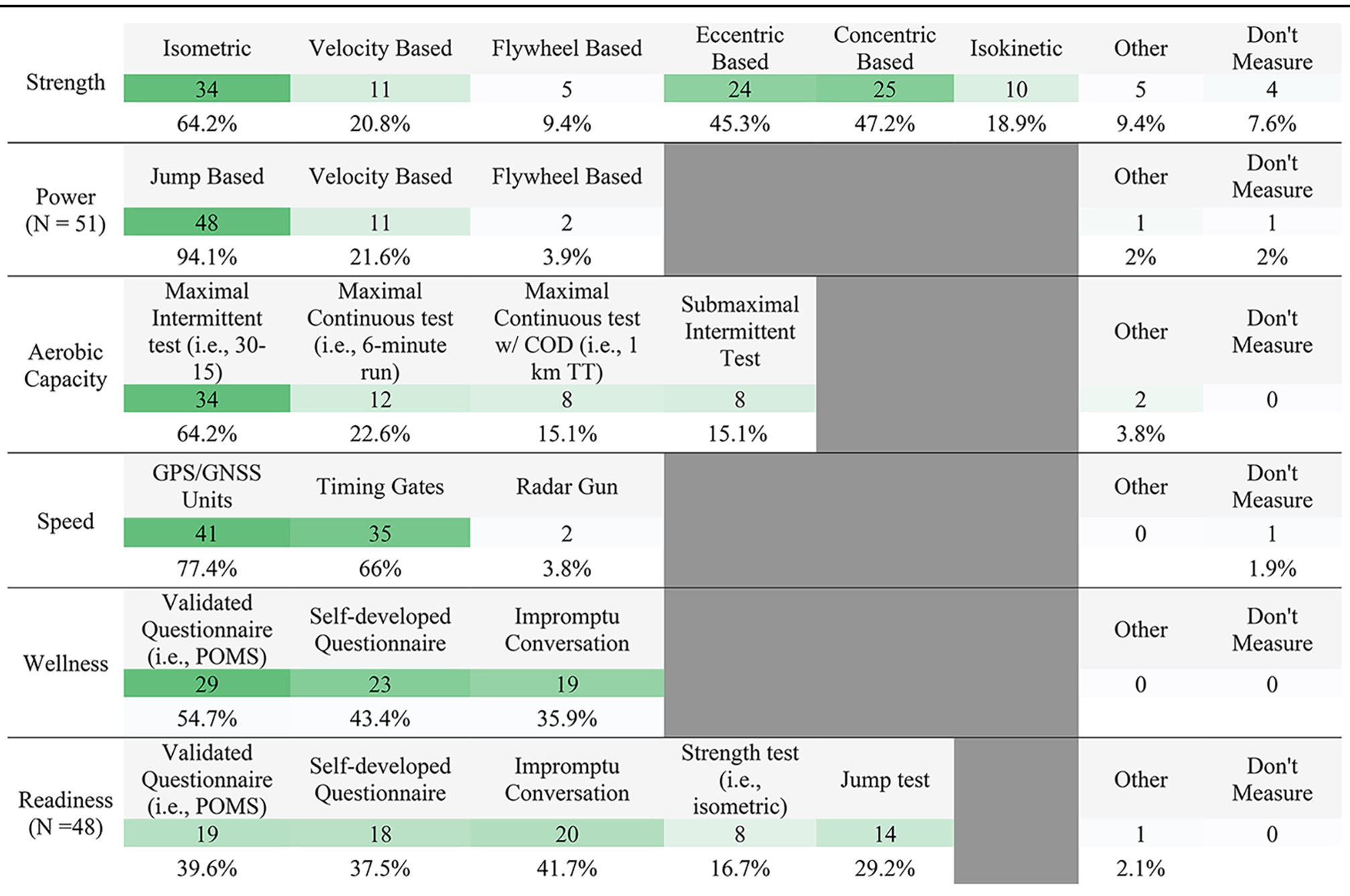
Strength assessments were conducted by 91.2% of responders, and typically oriented towards muscle contraction type with isometric (64.2%), concentric (47.2%) and eccentric (45.3%) as the most commonly reported (Table 3). Power was measured by the “most” responders (92.0%), predominantly via jump protocols (94.1%), with minimal use of alternatives (<25%; Table 3). Aerobic capacity was assessed by 100% of responders, with the “majority” (64.2%) using maximal intermittent tests. Almost all (97.8%) responders reported assessing speed performance, predominantly by using Global Positioning Satellite (GPS) units (77.4%) or timing gates (66.0%). All responders assessed readiness and wellness. Qualitative tools were predominantly used to assess both wellness and readiness, such as validated questionnaires (54.7% and 39.6%), self-developed questionnaires (43.4% and 37.5%) and impromptu conversations (35.9% and 41.7%).
Selection of methods for the measurement of strength, power, aerobic capacity, speed, wellness, and readiness. N = 53 unless stated otherwise.
Readiness and wellness – use of data
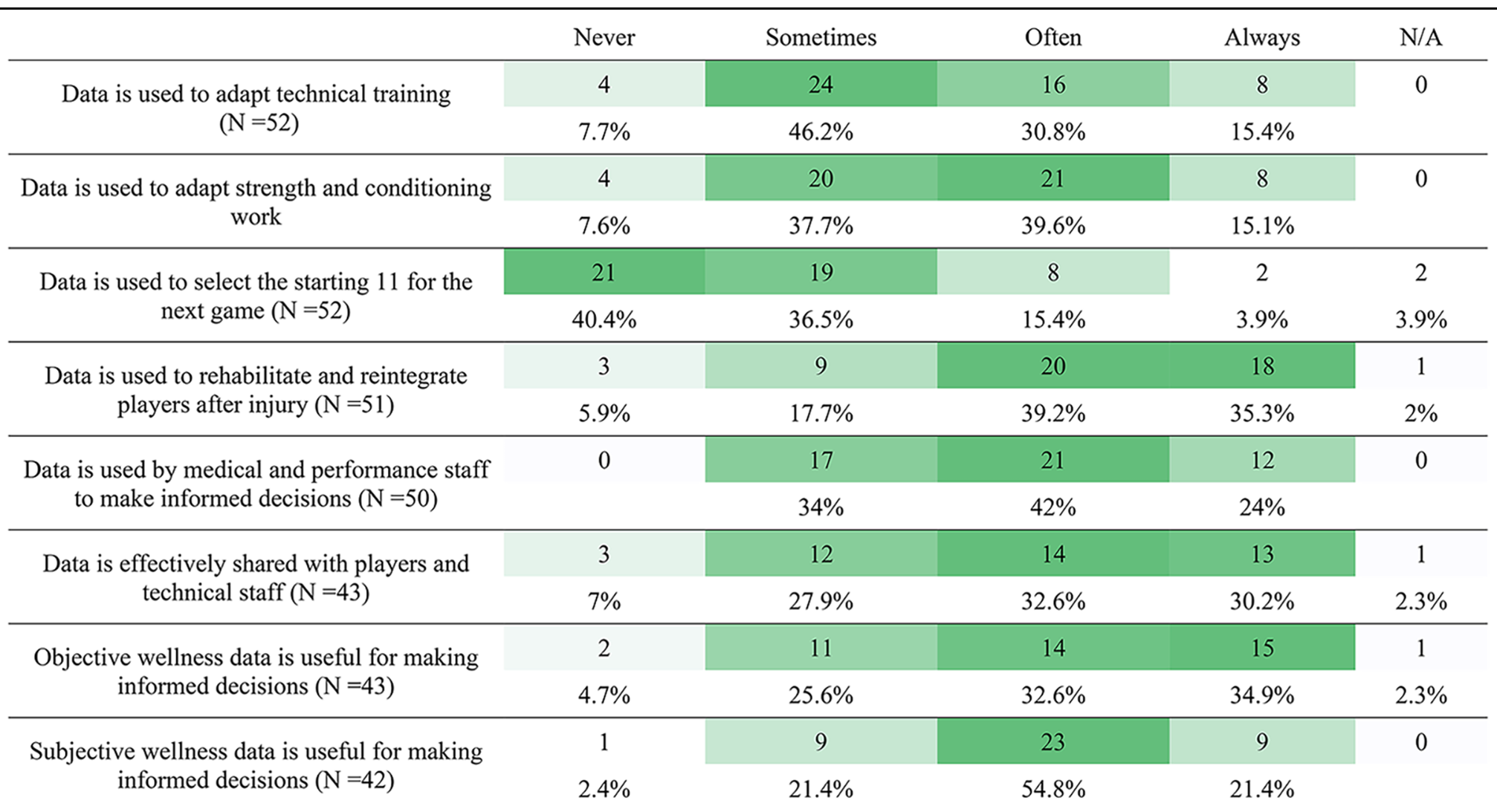
The use and frequency with which wellness and readiness data were collected varied, with no single option recording >50%, except for subjective wellness data being used in the decision-making process (Table 4). Wellness data was used by “most” responders as part of the decision-making process for strength and conditioning work (often = 39.6%, always = 15.1%), rehabilitation (often = 39.2%, always = 35.3%), and medical and performance decisions (often = 42.0%, always = 24.0%). Alternatively, Readiness data was used less frequently, with more responders selecting “sometimes” for all areas.
Absolute and proportion of how regularly wellness data is used in the decision-making process. N = 53 unless stated otherwise.
Discussion
The use of physical performance testing and monitoring of player readiness and wellness are common practices in professional football. The aim of this study was to collect such information from practitioners working in female football. The most important physical quality to most coaches was “power”, primarily assessed using jump tests, every 2–3 months (Tables 1 and 2). There was consistency in how physical qualities were assessed, however, there was a range of validated, unvalidated and impromptu methods to assess readiness and wellness, typically monitored daily. For example, a “minority” of practitioners also incorporate jump assessments as a part of their readiness monitoring process. Readiness was reportedly used less to inform decisions than wellness, despite wellness being a subcomponent of readiness (Tables 4 and 5). The spread among opinions shows there is much variability in practice. These findings may support coaches and medical staff in making informed decisions on topics such as training and recovery strategies with female athletes.
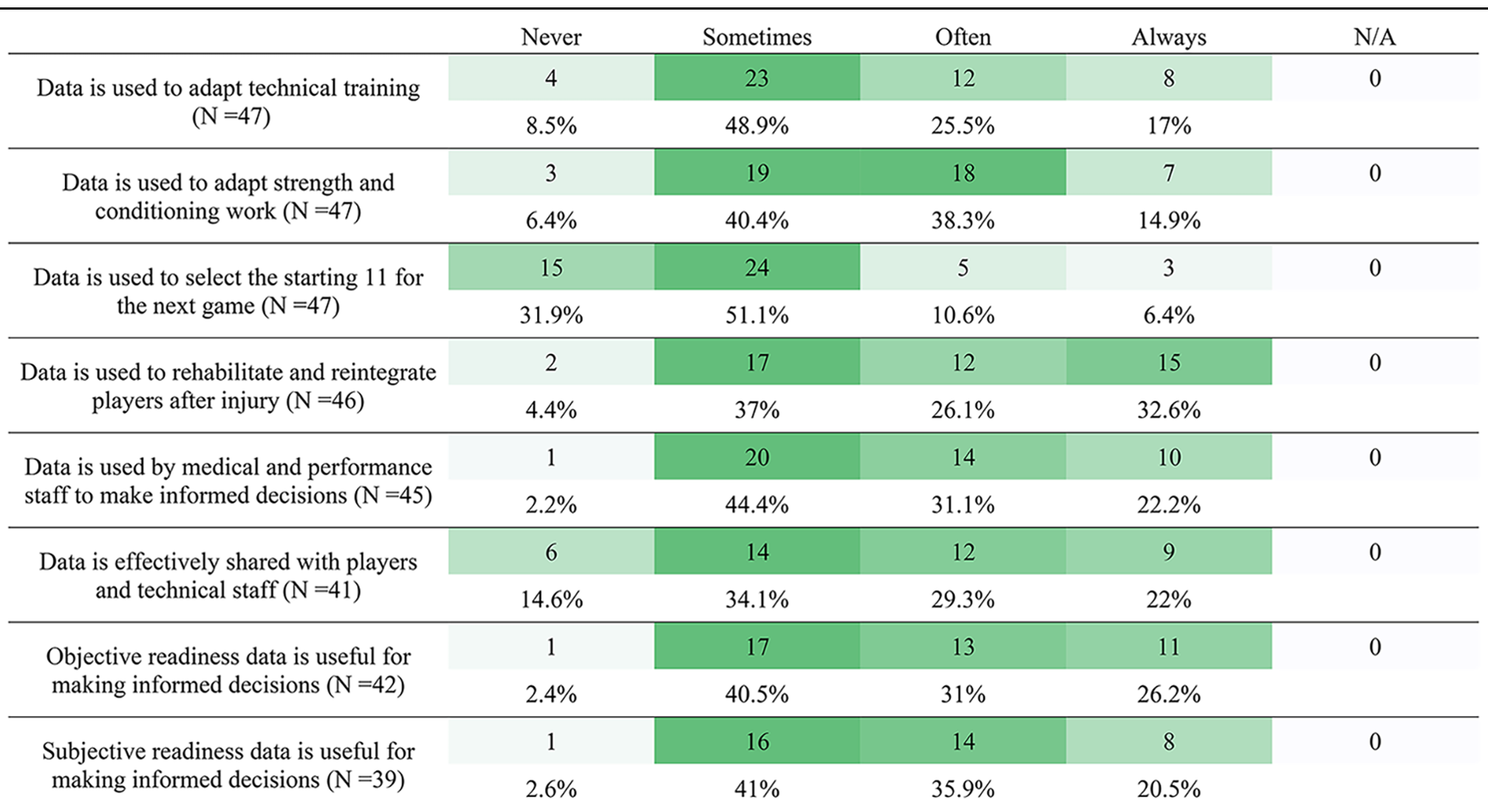
Absolute and proportion of how regularly readiness data is used in the decision-making process.
Physical performance testing
Physical performance testing is a standard practice in football as it can support the design of training programs, injury prevention strategies, as well as physical benchmarks to profile players. In agreement with previous literature, power was identified as the most important physical quality for football performance, likely due to it being a combination of high-force and high-velocity, and its association with activities that can influence match outcomes.19–21 In this study, power was commonly assessed using jump tests (94.1% of respondents), which aligns with previous research carried out with first-team male and female football practitioners (83%). 10 The increasing accessibility of systems, such as force plates, makes this an increasingly viable option for practitioners. Another important physical attribute identified by practitioners in football is speed, particularly due to its role in match-defining moments. 21 For example, speed testing 1was most reported to occur once per week (33%; Table 2), with most practitioners using GPS units to record the maximum velocity achieved (77.4%; Table 3). This is likely to allow an integrated assessment during training sessions, which would align with the physical focuses of that training day. With improvements in technology in recent years, GPS units show acceptable accuracy when compared to timing gates, 22 and are a reliable method to assess peak running velocity (as well as other external load parameters) with good to excellent interunit reliability. 23 Unlike jump and speed, assessments of strength and aerobic capacities were conducted less often, typically 2–3 times per season (40.4% and 56.6% respectively, Table 2). This is likely due to the time required to complete the testing and the fatigue associated with typical assessments of these attributes (e.g., maximal efforts).24,25 Alternative assessments, such as the isometric mid-thigh pull (IMPT), are likely to facilitate testing in football as they are less time-consuming and fatiguing (because of the isometric contraction). Isometric strength tests have shown strong associations with dynamic strength26,27 and high reliability. 28 Additionally, metrics derived from isometric testing have strong associations with jump, 29 sprint,30,31 and change of direction performance 31 in athletic populations. This would likely explain the prominence of isometric strength testing compared to concentric methods (64.2% and 47.2%, respectively; Table 3).
Readiness
Readiness can be defined as a status of physical and mental preparedness to train and perform at that specific moment in time, with wellness being a sub-component of this concept. 9 Due to this multifaceted construct, it has been proposed that readiness monitoring should include both objective and subjective measures to provide a comprehensive understanding of a player's state. 9 Beato et al., in their framework, explained that objective readiness measures can be categorised into on-field and off-field methods. 9 Off-field methods like CMJ, peak power cycling tests, isometric tests and heart-rate variability can give useful information to practitioners about their players’ status. Using on-field methods such as short sprinting tests and submaximal fitness tests may also allow practitioners to evaluate readiness using “invisible monitoring approach” (without formally testing players during their pitch-based session). In our survey, practitioners reported that the most commonly used objective readiness measures were jump assessments and strength testing (29.2% and 16.7% of respondents, respectively, Table 3). In support of this, evidence suggests that following a high-intensity bout of intermittent exercise, output variables such as jump height, peak power and peak force returned to baseline within 72 h, highlighting their capacity to assess a player's readiness. 32 Practitioners need to be aware that changes in underpinning jump-strategy metrics, due to prolonged stretch-shortening cycle fatigue, may negatively impact time-related variables. 32 Although metrics derived from jump-based assessments were not collected as a part of this survey, the authors believe that large variability in responses exists on this topic, and it is not yet clear what is best practice. Therefore, the decision around which metrics from jump-based assessments should be used is another important consideration for practitioners. 8 Similarly to jump assessments, the assessment of strength is an important consideration for the practitioner. Norris et al. conducted IMPT assessments 48 h, 72 h and 96 h post a professional Australian Rules Football game and saw trivial changes in peak force at all time points following match play. 33 Whereas the rate of force development at 100–200 ms was reduced up to 72 h. While the specific testing protocols may vary and require further investigation, there appears to be consistency in what practitioners consider important, the testing modalities used and the regularity with which they are assessed between male and female football. 10
Regarding subjective measures, most respondents assessed readiness daily (58.3%; Table 2), with validated questionnaires, self-developed questionnaires and impromptu conversations displaying a similar response (Table 3). Each of these subjective methods was more consistently used than the objective methods, which have been previously suggested to assess readiness in female football. 9 The variety of methods used was consistent with how often the information is used in the decision-making process. The largest proportion of responses for each option is “sometimes” rather than “often”, except for “Data is used to select the starting 11 for the next game” and “Data is used to rehabilitate and reintegrate players after injury” (Table 5). There is currently a theme whereby data is only sometimes effectively shared or used to make informed decisions. This potentially highlights the complexity of the decision-making process or the utility of the measures available to practitioners in their respective environments. Although readiness data is “sometimes” used to adapt technical training, practitioners are more likely to manipulate strength and conditioning work (Table 5). How training and strength and conditioning work will be altered based on readiness monitoring should be explored further, with little information available on this. Interestingly, readiness data is more commonly used for player rehabilitation and reintegration (“always” = 35.3%) than for other options. The importance of a player's readiness during this process is paramount to ensure progression towards full training can be effectively managed.
The findings of this survey suggest practitioners have a preference for the use of subjective over objective measures. Objective measures may require a longer recording procedure than subjective measures like surveys. Another factor that may limit the use of objective measures is that they require a maximal, although brief, effort that may be difficult to organise and execute in-season. Despite these limitations, objective measures offer data that is reliable, standardised and less influenced by subjective factors (e.g., the result of the previous match and other contextual factors) if collected appropriately. Subjective measures are advantageous because they are easily implemented. For example, players would be able to complete online surveys at the training ground or at home (after the match). However, practitioners need to be aware of the validity of the subjective tools used, which has recently been questioned. 13 Some of the most common AROMs used in sports have not been properly validated according to established guidelines. 13 For example, adaptations of previously validated tools with colour coding, imagery or alteration of scales may influence how an athlete interprets a scale compared to the original. These changes in response options should be guided by conceptual and computational factors, and any modification should undergo a validation process. Such differences should be considered by practitioners, and an appropriate rationale justified if validated tools are being altered. However, if a validated tool is altered, as 43.4% of practitioners report doing in the present survey (Table 3), it is unknown whether this tool is still measuring what it is intended to measure. Further, it is common practice for practitioners to create their own questionnaires relevant to their context, 34 and how reported above, altered or subjective tools designed in-house (with no previous validation), they may not measure what they are intended to measure, therefore, the authors of this paper do not recommend their use.
While wellness is a sub-component of the readiness construct, it is often used interchangeably with readiness itself. 9 More so than readiness, 86.8% of respondents reported assessing wellness daily (Table 2), through validated questionnaires, self-developed questionnaires, and impromptu conversations (54.7%, 43.4% and 35.9% respectively, Table 3). Wellness data is “sometimes” to “often” used to adapt technical training, strength and conditioning work in supporting the decision-making process of the medical and performance staff, and more frequently used to inform the rehabilitation processes (Table 4). The similar pattern seen in the utilisation and importance of both wellness and readiness information, suggests that practitioners value the insights that these daily variables can provide into a player's current state. Subjective wellness monitoring is cost-effective, simple to implement and can provide a contextual understanding of an individual's state if practitioners follow up with athletes. 35 However, there are questions around player buy-in and how this may affect the quality of data collected. 34 The importance of which wellness items are monitored should not be underestimated. Items such as non-training stress, fatigue and physical recovery have been reported as responsive to changes in well-being, whereas depression, emotional stress and sleep quality may not be. 35 This is supported by Thorpe et al., who reported a significant correlation between daily training load and subjective fatigue in English Premier League male football players. 36
An important aspect of wellness and readiness assessment amongst female athletes involves the monitoring of female athlete health. Indeed, a variety of approaches (ranging in quality) can be used to monitor menstrual cycle function. 9 Although not assessed in the present study, menstrual cycle tracking can provide useful information on a player's health and performance. 9 Future studies into the topic of female athlete health with specific considerations and recommendations for practical application are needed and are currently beyond the scope of the present study.
A limitation of this study is the inclusion of both first team and academy coaches within this sample from different global regions. With the range of environments in which practitioners operate, numerous factors may influence their practice, such as time and resources. 37 Due to the design of the survey, we have described the “what” and “how” of physical performance testing, and readiness and wellness monitoring, but not the “why”. This would help give important context to the decisions practitioners are making. Future work should investigate the rationale behind the methods that coaches have outlined here.
Practical applications
Practitioners can use a combination of objective and subjective tests and readiness procedures to assess the status of their players. Objective assessments can be used to further categorise off- and on-field procedures (e.g., invisible monitoring). Jump and strength (e.g., isometric) assessments are important to practitioners as they are utilised to assess performance and readiness. There is large variability in how measures of readiness and wellness are used in the decision-making process. Although together with more regular use of subjective measures, practitioners value how a player “feels” more so than how ready they are to “perform”. When practitioners decide to use subjective tools, it is strongly recommended to avoid using self-designed or altered scales (e.g., colours) because they may not assess what they aim to do.
This study underscores the importance of power as a key physical attribute in professional football, with jump tests being a common assessment method. This study reported how practitioners assess the readiness of their players using subjective and objective (off-field and on-field) monitoring strategies. Despite consistent evaluation of physical qualities, there is significant variability in readiness and wellness monitoring practices. This variability highlights the need for a greater understanding of these approaches to enhance decision-making in training and recovery, especially for female athletes. The insights from this research can aid coaches and medical staff in optimizing performance management strategies.
Flow chart of respondents.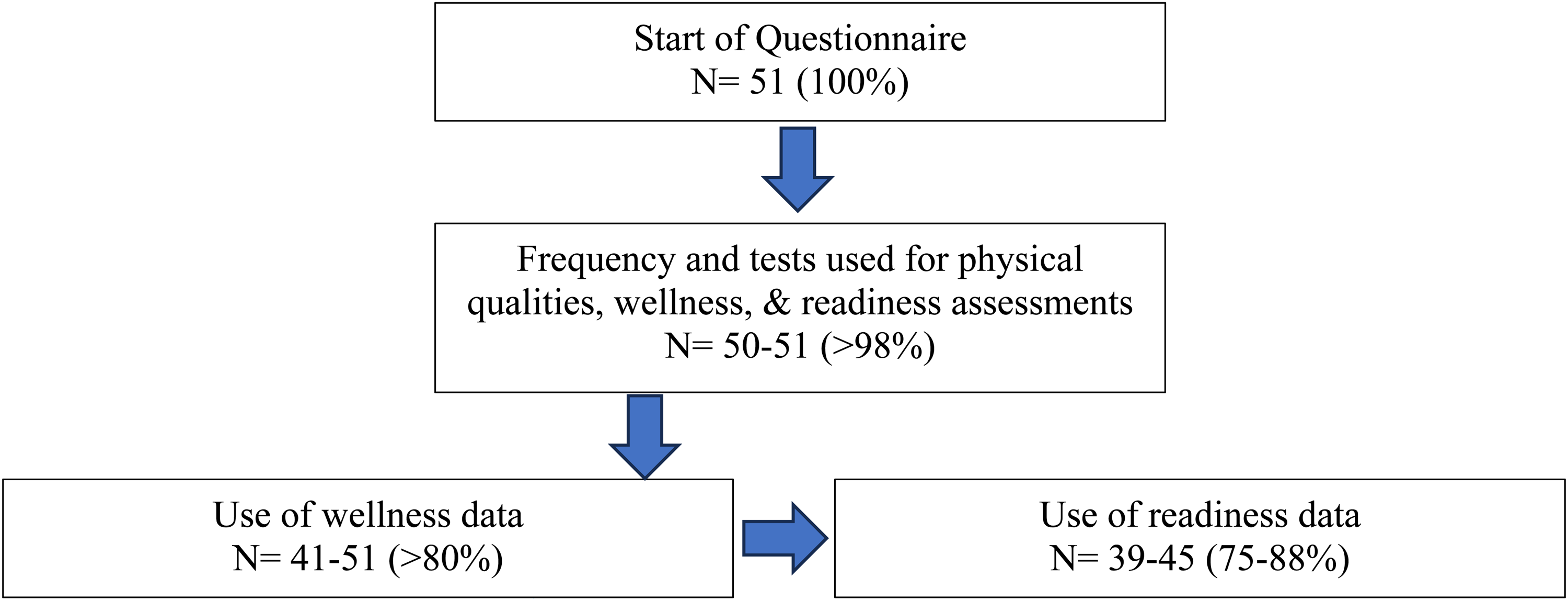
Footnotes
Acknowledgements
The authors would like to thank those who participated in this study.
Consent to participate
All participants gave electronic informed consent before participation.
Consent for publication
All participants were informed of the potential publication of research findings.
Data availability
Data will be made available in a public repository upon publication.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical considerations
The survey was approved by the University of Suffolk (Ipswich, UK) research ethics committee (ethics code: RETH(S)23/031).
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
1.
I agree to participate
2.
I do not agree to participate
1.
Man
2.
Woman
3.
Prefer Not to Say
1.
Professional (Full-Time) Athletes
2.
Semi-Professional (Part-Time) Athletes
3.
Amateur Athletes
4.
Academy (Youth Team) Athletes
1.
S&C or fitness coach
2.
Sport scientist
3.
Physiotherapist
4.
Medical doctor
5.
Sports therapist
6.
Other
Question
Not at all important/Slightly important/Moderately important/Very important/Extremely important
1.
Strength
2.
Power
3.
Aerobic capacity
4.
Speed
5.
Agility
1.
Isometric testing
2.
Isokinetic testing
3.
Velocity based testing
4.
Flywheel testing
5.
Eccentric-based testing (i.e., Nordic Hamstring Exercise)
6.
Concentric-based testing (i.e., 3RM)
7.
Other (Feel free to specify)
8.
We do not measure strength
1.
Every week
2.
Every month
3.
Every 3 months
4.
2 to 3 times per season
5.
Once a season
6.
It depends (feel free to expand)
1.
Flywheel based testing
2.
Jump based testing
3.
Barbell with a linear transducer
4.
Other (Feel free to specify)
5.
We do not measure power
1.
Every week
2.
Every month
3.
Every 3 months
4.
2 to 3 times per season
5.
Once a season
6.
It depends (feel free to expand)
1.
Maximal intermittent test (i.e., 30-15; Yo-Yo)
2.
Maximal continuous test (i.e., 6 minute run)
3.
Maximal continuous test with change of direction (i.e., 1 km time trial)
4.
Submaximal intermittent test
5.
Other (Feel free to specify)
6.
We do not measure aerobic capacity
1.
Every week
2.
Every month
3.
Every 3 months
4.
2 to 3 times per season
5.
Once a season
6.
It depends (feel free to expand)
1.
Maximal sprint with GPS
2.
Maximal sprint with timing gates
3.
Maximal sprint with radar gun
4.
Other (Feel free to specify)
5.
We do not measure speed
1.
Every week
2.
Every month
3.
Every 3 months
4.
2 to 3 times per season
5.
Once a season
6.
It depends (feel free to expand)
1.
Validated questionnaire (i.e., POMS questionnaire)
2.
Self-developed questionnaire
3.
Impromptu conversation (via message or in person)
4.
It depends (feel free to expand)
1.
Every day
2.
Every week
3.
Every month
4.
Every 3 months
5.
2 to 3 times per season
6.
Once a season
7.
It depends (feel free to expand)
Question
Never/Sometimes/Often/Always
1.
Data is used to adapt technical training
2.
Data is used to adapt strength and conditioning work
3.
Data is used to select the starting 11 for the next game
4.
Data is used to rehabilitate and reintegrate players after injury
Question
Never/Sometimes/Often/Always
1.
Data is used effectively by medical and performance staff to make informed decisions
2.
Data is effectively shared with players and technical staff
3.
Objective wellness data is useful for making informed decisions
4.
Subjective wellness data is useful for making informed decisions
1.
Validated questionnaire (i.e., POMS questionnaire)
2.
Self-developed questionnaire
3.
Impromptu conversation (via message or in person)
4.
Strength test (i.e., Isometric)
5.
Jump test
6.
It depends (feel free to expand)
1.
Every day
2.
Every week
3.
Every month
4.
Every 3 months
5.
2 to 3 times per season
6.
Once a season
7.
It depends (feel free to expand)
Question
Never/Sometimes/Often/Always
1.
Data is used to adapt technical training
2.
Data is used to adapt strength and conditioning work
3.
Data is used to select the starting 11 for the next game
4.
Data is used to rehabilitate and reintegrate players after injury
Question
Never/Sometimes/Often/Always
1.
Data is used effectively by medical and performance staff to make informed decisions
2.
Data is effectively shared with players and technical staff
3.
Objective readiness data is useful for making informed decisions
4.
Subjective readiness data is useful for making informed decisions