
Abstract
The potential adverse consequences associated with poor concussion management highlights the need to improve the translation of concussion guidelines into consistent use in real-world sport settings. To facilitate this process, New Zealand Rugby developed a community concussion management pathway to support concussion recognition, diagnosis, and management. This study adopted a pragmatic, descriptive qualitative approach to explore key stakeholders’ perceptions of the concussion management pathway, with the aim to inform policy and practice. Interviews were conducted with 123 participants, including players, parents, coaches, healthcare professionals, and school and provincial union representatives. The framework method was used to analyze data. Themes were organized according to the principles of realist process evaluation that considers contextual factors and mechanisms influencing a program's operation to produce specific outcomes. Contextual factors influencing the concussion management pathway's implementation included governing bodies’ support, existing local resources, general concussion attitudes, or concussion severity. The optimal functioning of the concussion management pathway (mechanism) was influenced by (i) pathway resources, (ii) roles and relationships, (iii) buy-in and support towards the concussion management pathway, and (iv) diligence and communication. Outcomes identified included (i) hitting the target (optimally managed and enhanced awareness) or (ii) missing the mark (dissatisfaction or management gaps). Overall, participants found the concussion management pathway valuable. However, the acceptability of certain policy-related aspects and the underlying attitudes associated with these perceptions, are some areas requiring further investigation and support. Tailoring programs according to end-users’ perceptions is crucial in developing context-sensitive interventions appropriate for a specific setting. These findings may act as a foundation for investigations of concussion management in other settings.
Introduction
Similar to most full-contact sports, rugby union (henceforth rugby) has a high risk of injury 1 with a high prevalence of concussion. 2 Concussion is a complex health concern, with a risk of adverse consequences if managed correctly.3–5 Removal from play, early clinical care, and staged return to activity are associated with faster, and safer, recovery.6–9 However, stakeholders’ (including general practitioners (GPs), coaches, parents, and players) knowledge and compliance with sports-related concussion guidelines may be inadequate. 10 Therefore, explicit efforts are required to facilitate the multi-level implementation of such guidelines.
In the era before international consensus guidelines for sports-related concussions were widely accepted, standardized protocols for concussion management were rarely utilized and it was common practice for athletes to return to play (RTP) after a suspected concussion within the same practice or game.11–13 For instance, a 2006 study conducted among New Zealand Rugby (NZR) players revealed that fewer than half of the players were aware of RTP guidelines after a concussion; 52% of players made the decision to RTP on their own; and only 22% returned to play after receiving medical clearance. 14 More recently, sports and medical organizations have intensified efforts to develop standardized protocols for injury management and RTP procedures following concussions.15,16 For example, in college athletics in the United States, significant efforts have been made over the past decade to promote best clinical practices in concussion management and raise awareness of concussion at both the institutional and athlete levels. 17 Current policies now require National Collegiate Athletic Association (NCAA) institutions to demonstrate compliance with the NCAA Concussion Safety Protocol, which covers preseason athlete education, pre-participation assessment, concussion diagnosis, post-injury management, and RTP guidelines after concussion.17,18 Implementation of these protocols has shown improvements in concussion management over the past 15 years, allowing athletes more time for recovery after concussion and reducing the risk of repeat concussions during the period of recovery. 17 Similarly, the Canadian Guideline on Concussion in Sport provides a clinical framework and resources to assist in the evaluation and management of Canadian youth and adults suspected of having a concussion.19,20
However, effectively managing sports-related concussions remains an ongoing issue in community sports due to a range of challenges.21,22 The implementation of guidelines is hampered, for example, by a lack of policy, inadequate staff education regarding concussion symptoms, and communication breakdowns among stakeholders. 23 In addition, there is often minimal consideration for the interaction of the challenges or their impact within the broader sport system. 22 In a study conducted among Australian community-level rugby union players, the majority of players did not receive RTP advice after a concussion, and among those who did receive advice, none adhered to the mandated three-week stand-down period. 24 In a recent study in South African rugby union, just 30% of community-level players who sustained a concussion followed a graded RTP protocol, 25 indicating poor adherence to the existing protocols. These findings underscore the pressing need for better dissemination and implementation of RTP regulations that take the specific context into consideration. 26
One of World Rugby's a strategies to enhance player welfare was the development of concussion management and pitch-side care guidelines. 27 Actual translation of guidelines into clinical practice requires careful cultural and context-sensitive adaptations to guidelines that are appropriate for a specific setting. 28 To facilitate this process, NZR systematically developed a community concussion management pathway (CMP) to support improved concussion recognition, diagnosis, and management. 29 From a system's thinking approach, injuries may have multiple, interrelated contributory factors created by the decisions and actions of people across all levels of a particular system. 30 Concussion management strategies should similarly consider the sport system as a whole, 21 and as such, the system's thinking played a guiding role in the development of the CMP, by involving various community rugby stakeholders. The CMP attempts to close the loop between suspected concussion recognition and RTP, by using technology to provide information to relevant stakeholders at appropriate time points.
Phase one of the CMP consists of pre-season player baseline testing. 31 If a player sustains a suspected concussion during training or match play, the incident is logged on NZR's bespoke phone application (app), developed by NZR, specifically for use as part of the CMP. The person responsible for logging the incident is referred to as the app manager (usually the team manager or physiotherapist). The app generates “suspected concussion” email notifications to the player, their parents/caregivers, coaches, school/club, and provincial union (PU), b containing a unique identifier code that will enable a GP to access that player's baseline concussion score through a secure web-based concussion portal. The portal also provides guidance for diagnosis and clearance. Once a diagnosis is made, email notifications are sent to relevant stakeholders. Thereafter, the player is required to follow graduated RTP and learn (GRTP/GRTL) protocols. After completion of the stand-down period, the player visits the GP once more for clearance to return to contact training, and clearance notifications are emailed to relevant stakeholders.
In 2019, the CMP was trialed within New Zealand (NZ). 32 Evaluation of the CMP, and identification of key factors that may influence its success, are important steps to the adoption and sustainability of the program. Instead of focusing solely on the efficacy of an intervention, truly determining the impact of an intervention also requires a deeper understanding of the intervention's uptake in real life. 33 Of particular importance is an understanding of the ecological systems and contexts in which the intervention is implemented. 26 This includes the recognition that individual behavior is a function of the interactions between people and their physical, social, and political environments, and that sustained change is unlikely if these environments do not encourage and support the desired change. 33
The CMP was designed by taking multiple levels (and thus multiple stakeholders) of the community rugby system into account and requires a number of different actions by those stakeholders.29,34 Thus, the implementation of the CMP, and the outcomes it delivers, is not likely to be a linear process. In this respect, realist process evaluation offers an approach that may assist in overcoming some of the difficulties associated with the evaluation of interventions in complex social systems. 35 From this perspective, the same intervention may have different outcomes, depending on the influence of contextual factors. 36 Overall, realist evaluation seeks to identify the varieties of success and failure that any program experiences and the factors that contribute to both intended or unintended outcomes, as opposed to focusing only on the worth or effectiveness of a program. 37 The growing concern around concussion emphasizes the need for interventions that aim to translate available evidence-based guidelines into real-world sport settings. 10 Thus, the aim of this study is to explore key stakeholders’ perceptions of the CMP, by gaining a deeper understanding of the implementation context, mechanism by which the CMP operates, and outcomes of the CMP.
Methods
Study design
This study adopted a pragmatic, descriptive qualitative approach. 38 This approach was considered best suited to explore the CMP process from the perspectives of key stakeholders, to provide descriptive information that can inform policy and practice. 38 Ethical approval was granted by the University of Otago Human Research Ethics Committee (18/087). Additional information regarding the methods is contained in Supplemental Appendix 1.
Participants
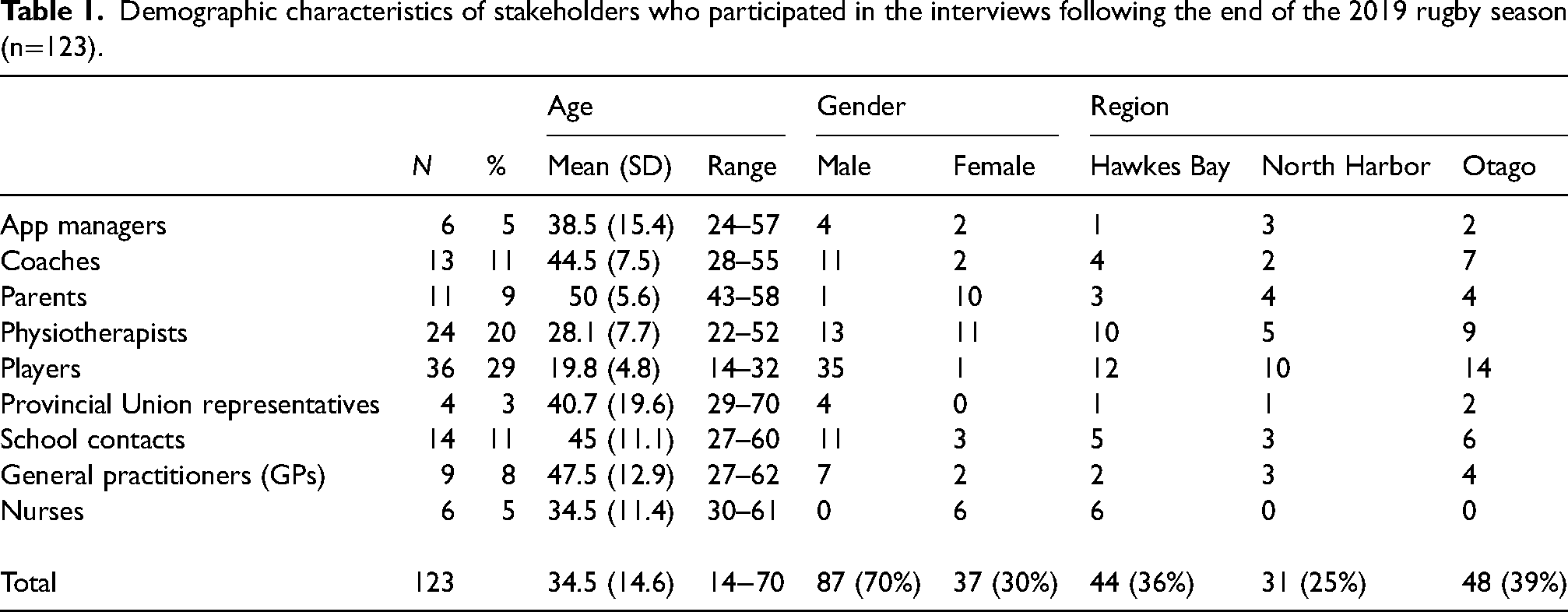
This project was conducted in four geographically and socioeconomically diverse PUs in NZ. Within each PU, rugby administrators in male and female rugby playing schools and premier-level community clubs were contacted to identify teams, from which; app managers, school contacts, coaches, players, parents, and nurses were invited to participate in the study. Additionally, PU representatives, physiotherapists, and GPs involved with the CMP within the four unions were invited to participate. Written informed consent was obtained prior to the start of the interviews. A total of 123 participants from these nine stakeholder groups were included in the study (Table 1).
Demographic characteristics of stakeholders who participated in the interviews following the end of the 2019 rugby season (n=123).
Data collection
Semi-structured interviews were conducted at the end of the 2019 rugby season. Interviews lasted between 30 and 75 min and were audio-recorded. Semi-structured interview questions were developed by our interdisciplinary research team (JR, DS, AC, SK, SJS, and SW) to explore participants’ experiences of the CMP (Supplemental Appendix 1). The questions were pilot-tested by relevant stakeholders within the rugby community and altered according to feedback. Interviews were conducted by six researchers experienced in qualitative methods. One research assistant was present during each interview to take field notes. The interview team consisted of one male and five female researchers, all involved in the implementation of the CMP. To facilitate consistency between interviewers, leading qualitative researchers (SW/AC) conducted a training session with the interviewers prior to the interviews. Additionally, interviewers and the research assistant met weekly with the research team to discuss interview consistency, by continually including the use of probing questions and paraphrasing to confirm understanding.
Data analysis
Interview recordings were transcribed verbatim and organized in NVivo 12 (QSR International). The framework method was used as it offers a structure whereby data can be systematically reduced to facilitate analysis and comparisons across stakeholders. 39 An initial set of interviews was coded independently by two coders (MB and a research assistant) and an analytical framework was developed and refined until a consensus was reached. A second research assistant then applied the framework to the same set of interviews. Thereafter the framework was refined until consensus was reached. In a final round of coding, all three researchers coded another set of seven interviews with the new revised framework, and coding was discussed. Finally, the data set was divided between the three researchers and the revised analytical framework was applied afresh to the whole data set. During this process, weekly meetings were held with the core coding team to discuss coding and test assumptions. The broader research team (MB, DS, SW, AC, SK, and GS) discussed the coding process and provided input on a bi-weekly basis. Once coding was completed, one researcher (MB) developed multiple framework matrices by summarizing the data by category from each stakeholder group according to each phase of the CMP. The matrices provided a structured overview of summarized data and facilitated the recognition of patterns and themes across the data set. 39
After initial themes and sub-themes were identified, a realist approach to process evaluation was used to guide interpretation and to conceptualize a practical presentation of the findings. 37 As such, themes were developed and organized according to a context-mechanism-outcome configuration. For this analysis, “mechanism” refers to participants’ perceptions around the factors involved in the operation, or flow, of the CMP. This “mechanism” is influenced by the specific “context” and stakeholders within the context. As a product of the interaction between “context” and “mechanism,” “outcomes” described concussion outcomes with respect to the overall goals of the CMP.
Results
The identified themes acted as either barriers or facilitators and were present across various stakeholder groups and CMP phases (Figure 1).
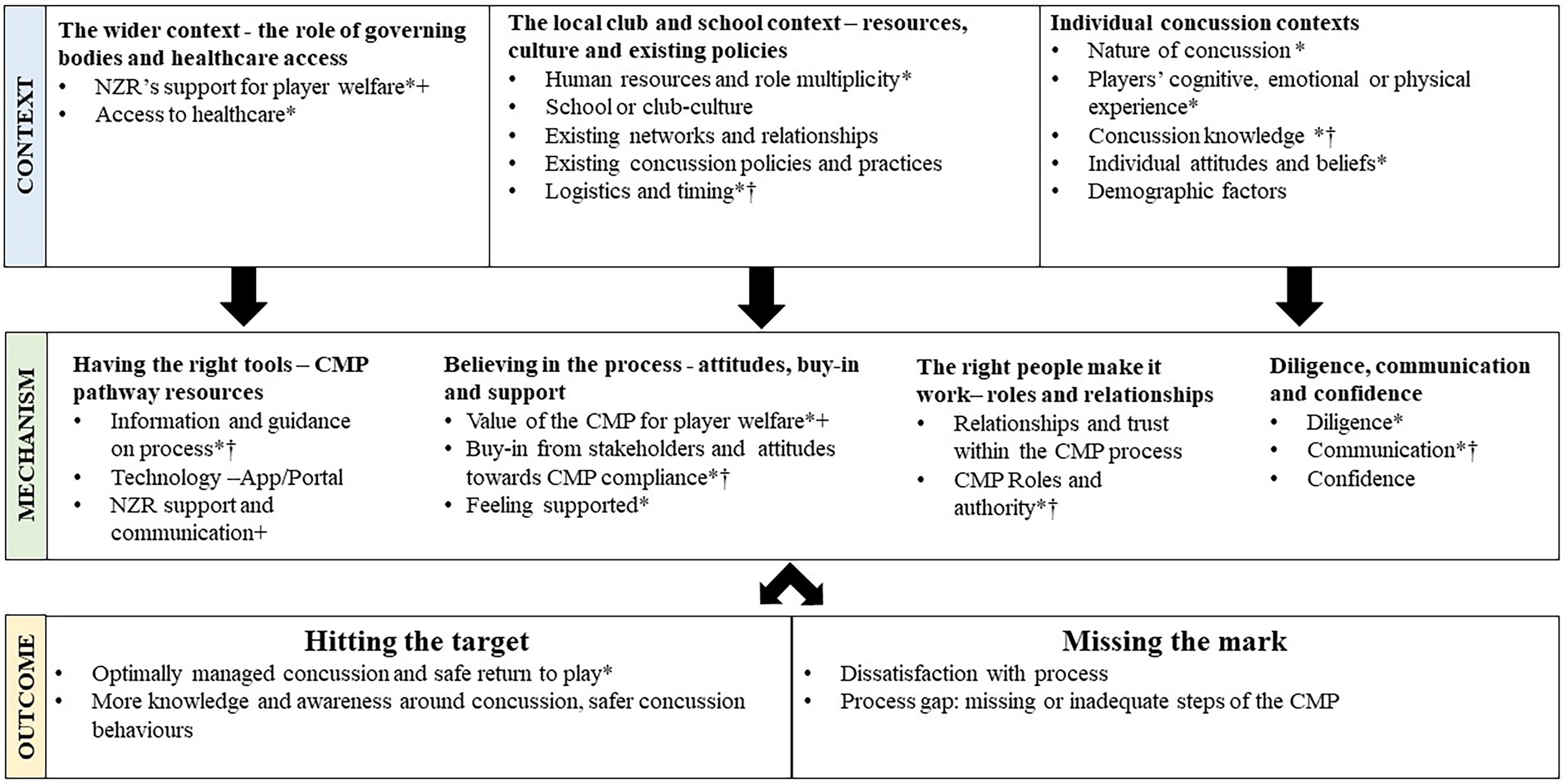
CMO configuration of key themes within the CMP—context and mechanism factors were identified as both barriers and facilitators.
Context
In this study, contextual themes describe the implementation setting and the existing factors present within this setting that could influence the functioning of the CMP. These contextual themes were developed according to their position within the wider, local, or individual context. Additional illustrative quotes can be found in Supplemental Appendix 2.
1. The wider context—the role of governing bodies and healthcare access It's a program that is needed in all sports, not just rugby. The sooner it gets adopted by all the other sports the better. (B4—app manager)
NZR's support for player welfare. Participants valued the CMP's role in facilitating the real-world application of existing concussion management protocols that could also be adopted in other sport settings in NZ:
However, for the stakeholders responsible for the process at the grassroots level, the CMP's implementation was not without challenges. These stakeholders valued the effort invested into concussion, but equally felt that governing bodies should provide assistance in enforcing the protocol, assist with getting buy-in from stakeholders, and provide human resource support.
Access to healthcare. As a wider contextual factor, access to healthcare influenced the CMP's functioning. Specifically, timely access to a GP (who was preferably CMP trained
c
) was identified as an important barrier to getting players the necessary care or clearing them in time for a specific match: Players couldn’t see the doctors because the doctors had allocated five appointments on a Monday and there were more than five concussions on Saturday. The next five had to wait till following Monday … we struggle with getting them to the doctor anyway, if they’re like, “no, you can’t see him until next Monday,” then compliance is really low. (B17—Physiotherapist)
Access to healthcare resources such as concussion clinics and physiotherapists during the GRTP phase varied between research sites but was identified as an important contextual facilitator if available.
2. The local club and school context–resources, culture, and existing policies It wouldn’t work just by itself. Just because teachers always complain they don’t have enough time for just their classroom … Even though they understand concussion's important, I just don’t think they’d take their time to do it without that external help. You would be educating, testing, all of that … on top of the job. (C15—Coach)
Human resources and role multiplicity. The extent of human resources available within a club or school was identified as an important contextual factor. For example, the availability of personnel (such as a physiotherapist for baseline testing or to guide the recovery of players) was an important consideration for the implementation of the CMP within most settings. In addition, some stakeholders had multiple roles and responsibilities which impacted their duties relating to the CMP. For example, coaches, who were also teachers, reported that it was challenging at times to manage players’ well-being as well as their other responsibilities within the team and school.
However, role multiplicity also facilitated management, as these stakeholders often had additional insight into rugby-related aspects of school life. The support provided by NZR mitigated some of these human-resource-related challenges, and some stakeholders felt that it may be difficult to sustain aspects such as baseline testing, without this support.
School or club culture. In this study, it was evident that a positive school/club culture and a general appreciation of the seriousness of concussion often mitigated logistical challenges or limited human resources. However, differences were reported between support for rugby between boys’ and girls’ schools. Some stakeholders from one girls’ school indicated there was very little support for rugby. In comparison, some all-boys “big rugby schools” were well-resourced and invested in supporting rugby-related initiatives such as the CMP. However, in schools where rugby was a popular sport, the importance placed on winning hindered players to report suspected concussions, as staying on the field was deemed more important: The player knows they’re doing the wrong thing, but they’re being pressured by parents, and team expectations. You know, and when you’ve got a good athlete there, the pressure on them to just keep going is really, it's bad. (C21—Coach)
Existing networks and relationships. Participants emphasized the importance of strong, existing relationships and trust between stakeholders: We are associated to the school, but we are a rugby club so, and our rugby club is solely run by parents and non-teachers. We don’t have anybody in there in the school on a daily basis. But we have a teacher in charge of rugby at the school who gives us that communication link back into the school. That ties us back in quite nicely. Plus, we have a very strong relationship back in through the school ourselves individually. (C34—Coach)
App managers, who knew their players well, reported being alert to players “not being themselves” on the field or when progressing through their recovery. Similarly, physiotherapists with an existing working relationship with GPs, not only reduced GPs’ workload but also facilitated a smoother RTP process. In contrast, some coaches who were external to the school (e.g. not teachers) found it difficult at times to drive the CMP, as they lacked strong relationships with the school.
Existing concussion policies and practices. Schools previously involved in some form of baseline testing, or the knowledge and training of coaches acquired in the RugbySmart
d
courses, acted as a favorable foundation for the CMP process. This “familiarity” also extended to the GRTP protocol, as certain settings already followed concussion protocols provided by NZR in the past. There were, however, very few school processes in place for integrating players back into school/study after concussion: I know a lot of students who have been concussed this year, were at school on a Monday, and they would leave before morning tea because it was just too much for them. Then mom and dad would traditionally go, “Oh, he's milking it. He's just trying to get time off.” I think that's where parents aren’t educated and even some of the staff. (A17—School contact)
Logistics and timing. The club/school's ability to deal with logistics acted as an important barrier, specifically in the pre-season phase. Stakeholders involved in baseline testing, such as school contacts, physiotherapists, and coaches, reported the process could be time-consuming and disruptive to normal learning/training schedules, and the team may not yet be finalized when testing is organized. Thus, finding the best time to conduct testing or follow-up with players who missed baseline testing, were challenging: Getting that testing and organizing people to be there at the right time, getting it done. I don’t think that's an issue, but it's a timing thing. Because in our preseason … not all our players were there. (C22—Coach)
3. Individual concussion contexts
The nature of concussion. The presentation and severity of concussion played a pivotal role in the manner in which the CMP process would unfold. Participants reported that it was difficult to identify suspected concussions in players with only very mild symptoms. It's easy when they’re clearly concussed. Those ones are never really an issue. It's hard when they’re on the fence. (C12—Physiotherapist)
In severe cases, diagnosis was often easier and aided by the use of baseline scores. Similarly, players with few, or no symptoms, progressed with little trouble through the GRTL or GRTP, while for others this experience was challenging, with some being obviously symptomatic, finding it difficult to concentrate, or struggling to progress through the stages of recovery: I went to the school for like two days and in that first week, but I feel like I wasn’t actually there and concentrating was just … I just couldn’t, I literally, I would stare at a board and be like, seeing two of the boards and then you’d be going off into a … sort of like your own little world. (C14—Player)
Players’ cognitive, emotional, or physical experience. When removed from the field with a suspected concussion, players often reported feeling disappointed and worried about “missing out”: Yeah, because it was just … the timing was really hard for me because I … especially “cause I worked real hard to … I had finally gotten to the position.” I had worked hard for a year and then I was … it sort of got taken away from me, so that …Yeah, quite hard. (C33—Player)
These emotions affected their attitudes towards disclosure. Another important factor was whether players (and parents/coaches) believed they were concussed or not. Some players reported “feeling stressed” about their GP visit as they felt they had to “convince” the GP they were not concussed so they could RTP. Once recovered, players were excited to RTP. However, some felt unconditioned, scared, and “less aggressive” when returning to play. For parents, the emotional experience of the concussion was also pertinent, as they were often disappointed in their children, or found it difficult to manage the child's expectations and emotions, especially if they doubted the diagnosis.
Concussion knowledge. Existing concussion knowledge and awareness was important factor influencing the CMP experience for most stakeholders. Players were often unsure if their symptoms were concussion related. Similarly, parents’ concussion knowledge was either a significant concern or an important facilitator: Sometimes boys don’t know, or they won’t tell you they’re concussed … If you educate us as parents on some of the effects of concussion, like the delayed effects … they might be sick a day later, or forgetful … that’d be really good to know. (B34—Parent)
For physiotherapists, knowledge barriers existed in the “grey areas”; that is, identifying a concussion, deciding when to log a concussion or uncertainty around management. Some stakeholders felt that GPs were not suitably skilled, or were quick to diagnose without understanding the implications of a diagnosis for rugby. In contrast, participants appreciated GPs who gave good advice and used clinical reasoning for clearance (as opposed to “blindly following the rules”). Both physiotherapists and GPs acknowledged that not all their colleagues have the knowledge to diagnose and manage concussions.
Individual concussion attitudes and beliefs. The majority of stakeholders emphasized the importance of prioritizing player welfare: It's such a serious thing. If you’re not thinking about a person's wellbeing, then you’ve got issues. Especially a young person. I’m very conscious of people's wellbeing before all else. I don’t put winning first. We’re not going to be some elite winning school. I’m prepared to have difficult conversations with people over that. (A4—Coach)
However, coaches also mentioned getting frustrated as “not every head knock is a concussion” or felt that (other) coaches still downplay injuries. Comments made by coaches also revealed deep-rooted attitudes to girls’ rugby: some stating that more support is needed to “keep girls safe,” especially as they can differ in size and experience; or that it is difficult to know if “girls really have a concussion or just had a hard knock” based on their symptom presentation and being more cautious in their behavior after a big hit The majority of players considered concussion to be a serious matter, that may have longer-term consequences, and that it was important “to look after your head” and your teammates. However, several players reported that they could be stubborn, by not always listening to advice, and wanting to rush recovery, to get back onto the field: If I’m injured or something, say my name, and I’ll run the other way. I didn’t really want to hear what he has to say if I’m not allowed to play. Yeah, it's hard (to stand down), I love being out there, smashing people. (B25—Player)
Demographic factors. Factors such as the player's age or level of play, their concussion history, and family circumstances were important contextual considerations. Coaches felt that older players could take more responsibility, while they had to make sure that younger players’ parents were well informed. For senior players, work circumstances at times affected their ability to see the GP or to take time off for recovery. Coaches mentioned that they were more cautious with players with a concussion history, but also noted that these players knew the symptoms and could potentially be better at hiding them. Language-related communication difficulties with players and parents were also reported in the immediate management phase: I was trying to talk to his dad, his dad didn’t speak any English so, that was a struggle. And then we didn’t see him for three weeks until he was cleared to come back … He didn’t go see a doctor. We told him all this information, didn’t get passed to him…I don’t think he did. I told him to. His dad, I thought his dad got the idea but… (B15—Physiotherapist)
Pathway mechanisms
“Pathway mechanisms” refer to the factors directly related to the CMP, that appeared to be fundamental requirements for the day-to day functioning and optimal flow of the CMP as an intervention. As such, these themes describe the “mechanism” that drive the CMP's functioning.
1. Having the right tools—CMP pathway resources
Information and guidance on process. Adequate information, guidance, and general advice on the process acted as either a strong barrier or facilitator. For parents, this was one of the most important factors influencing their perception of the CMP: I feel like we were really well-informed. The process overall worked well, it was made quite clear to us that [her son] had to be assessed again by a GP and things like that. (B33—Parent)
Apart from the need for guidance for themselves, physiotherapists and GPs mentioned the importance of getting enough information to the player, which some felt did not always materialize. Players often reported not being able to remember whether they received any information after their concussion. In the sub-acute phase, several players were satisfied with the advice received from the GP. However, others felt overwhelmed after their GP visit and had hoped for more guidance. Multiple stakeholders reported a need for more information and guidance regarding the GRTL phase.
Technology—app/portal. GPs felt that the portal facilitated a structured approach to the diagnosis or clearance visits. In addition, most app managers and physiotherapists felt the app streamlined the process and that it was useful to have information (such as the red flags) at their fingertips, which made them more confident in their decisions. I found the app really quite simple to use, especially if I’m on the field for example … if they’ve got symptoms like blurry vision, double vision, they’re unbalanced, stuff like that … For me being a student, because I might not know much about what the right questions are to ask due to my lack of experience … I haven’t been in that situation enough. I press that button and I ask the players are you feeling any of these, and then they’ll be like yes or no, then that made me feel like I was confident enough to be like, you need to go be seen by a medical professional at this point or not … Which I thought was great in terms of the player welfare, like make sure player safety is really important, straight away, keeping them safe if they needed it. (A20—Physiotherapist)
NZR support and communication. Various stakeholders identified the communication and support received from NZR as an important factor in the operation of the CMP: There was awesome communication. I was straight to you guys [NZR] expressing what was going on, and it was that day there was a solution, and we had a plan. So, in terms of communication and support in that respect, that was probably the best I could have asked for. Knowing that you had a contact that you could just go straight to, rather than trying to go through multiple levels of hierarchy. (C10—Physiotherapist)
2. Believing in the process: attitudes, buy-in, and support towards the CMP
Overall, the belief, buy-in, and attitudes towards the CMP were the most prominent themes identified for the successful operation of the CMP.
Value of the CMP for player welfare. Participants appreciated having a structured process, which ensured better care: There weren’t any decent systems in place before this. If someone was concussed, I’d tell them to go see their doctor. I wasn’t really certain if they were all right or not, or if they had been seen, if they had been cleared. Often, I had to take their word for it, because I didn’t even know who their GP was. There wasn’t anyone for me to contact. So having an app where I can log it, I know that NZR knows about it. I know that a GP somewhere is aware of it … It's really positive for me. (B15—Physiotherapist)
Players reported feeling “relieved” to have a diagnosis, reassuring them they had made the correct decision to disclose. Similarly, the majority of stakeholders saw the value in the GRTP phase and the importance of managing player recovery correctly. Various stakeholders felt baseline testing was valuable, as it facilitated diagnosis and clearance, educated players about concussions, and helped them understand their recovery.
Buy-in from stakeholders and attitudes towards CMP compliance. The extent of buy-in from stakeholders played an important role in pathway compliance: One of the younger guys got a head knock. And we couldn’t see it from the sideline, he didn’t fall over, he wasn’t lying on the ground. He just … and the captain stood up and looked at him and asked if he feels all right and quite clearly he wasn’t, and [team captain] grabbed him, brought him to the sideline and he just said to the ref, “I’m taking [player] off.” We wouldn’t have seen it, he would have played on had it not been for the other players. I think that's a really key thing. They know how dangerous it is now, they know what to look for, and they know that if they’re managed properly … they get to return to play. (B5—app manager)
The buy-in was also demonstrated by coaches and physiotherapists who mentioned that despite the logistical challenges faced with baseline testing, they were still happy to do it because of its importance. Some players spoke about being accepting of the time they needed to take off to recover properly and that medical clearance was a necessary step to RTP safely. However, in some instances, player attitudes were problematic, with players pretending they were not injured or, being stubborn or angry when removed from the field: I didn’t really think that I was concussed. I didn’t really feel like I was concussed. I think it was just kind of frustrating thinking that I had just done the test all good. And then to hear that, because I’d had the head knock itself … I had to stay off for 24 days. I just didn’t understand that. I just didn’t understand why I wasn’t allowed to play. (B24—Player)
Similarly, in other stakeholders, although they saw the value in the CMP, the underlying importance of performance was evident, and it meant that player welfare was not always a priority: I know we said it would take five minutes per player (for baseline testing), but they’re in and out, in and out … That practice was a write-off. The other guy was, “Well, this is a waste of time.” I understood the importance of it, but we had a game on Saturday, it's pre-season, but I didn’t have a chance to work with them. (A25—Coach)
Importantly, some stakeholders felt that the mandatory stand-down period may be a barrier to disclosing and that some degree of leniency is required. Some of the patients with a logged concussion were sent off but hadn’t really had an assessment of a concussion, and so it was a presumed concussion diagnosis before they arrived to me, and they were automatically off for 23 days, even though they were functioning at the first visit, at or better than the pre-season assessment, and so I felt a bit bad and I thought, well, this could be a potential barrier to potential concussions being reported, because as soon as it's a query, concussion, it's treated as a concussion. And they’re off for that full period of time. (B11—GP)
Feeling supported. Factors such as baseline testing, the logging of concussions, or player experience through the CMP were influenced by the support received by others. Physiotherapists identified baseline testing as a “big task” which required sufficient support from coaches and schools. So they (NZR) helped us resource it, because in reality that was quite a big task. Yeah, and bear in mind we’re all volunteers, typically, doing this. And so, in a way, you guys are asking us to give up a fair bit of time for this. And for the most part, I think most of us would be fine with it, I was fine with it. But having one or two people come out to help made that job, turned it from a six hour job into a two hour job, and that made a massive difference. (C30—Physiotherapist)
For app managers, logging of concussions was either a challenging and isolating experience or much less stressful if coaches, parents, and referees were supportive of their decisions. For players, it was important to feel supported by teammates, coaches, and parents to disclose their suspected concussion while progressing through recovery. However, players identified a lack of support as a key barrier during the GRTL phase.
3. The right people make it work—roles and relationships I’ve had the same team and all of the same individuals for a number of years it all works quite well. This year I didn’t have any issues with them reporting or not reporting. I think as they’ve gained that trust, to some extent, they are happy to say, “Look, this is how I’m feeling, what do I need to do about it?” (C12—Physiotherapist)
Relationships and trust within the CMP process. Trust between stakeholders was required for the CMP to run smoothly.
Coaches reported trusting physiotherapists to make the right call when removing players or returning them to play. Trust between physiotherapists and GPs also streamlined player management. Parents reported trusting coaches, and the school, to not let a child RTP if they were not yet allowed and physiotherapists and coaches spoke about the importance of trusting their players to disclose an injury. Trust was also identified as being problematic, if coaches and physiotherapists had to rely on a player's word that they had been medically cleared, but no formal communication had been received.
CMP roles and authority. Certainty of roles within the CMP included players acknowledging their role in being honest when they suspected a concussion in themselves or others: Actually I think the onus is just on the person (the player) … Sort of putting their hand up and saying, “Yeah. Nah. I’ve got a wee knock. I need rest and not do … yeah, not carry on playing.” (C17—Player)
However, other participants also emphasized that players often find it difficult to be honest about a suspected concussion because they want to keep playing and that it remains the responsibility of key stakeholders around the players, to look after them and help them understand the importance of managing concussion correctly: Coaches and the parents are the most important people. Because some students, if they think it's going to impact their ability to do things they love [like rugby], then they’re not concussed. Because yes, the players need to have an understanding, but they also need to be helped through it. And that's the adult's job. (C35—School contact)
Experienced physiotherapists felt they were well equipped and keen to take on more responsibility in making decisions about clearance to play, which allowed GPs to clear players remotely. However, lack of role clarity was also prominent in this theme. For example, app managers reported being unsure of where their responsibility ended after logging the concussion and whether they should be following up with players. Similarly, coaches reported feeling unclear on whether they should be following up with players during the GRTP phase. Some less experienced physiotherapists felt it was the GP's role to educate the player, yet GPs commonly felt that because of time pressures these responsibilities should be shared.
4. Diligence, communication, and confidence My coach, and my management, as soon as I said I was feeling a bit dizzy and faint, they pulled me straight off. There was no “Come on mate, you’ll be all right, carry on.” From there, they followed strict procedure. The physio checked me out and told me to go see my doctor. It was really cool to not get any hesitation. They just said straight away, this is what you’ve got to do, follow the procedure. (C41—Player)
Diligence. From the players’ point of view, the dedicated behaviors of stakeholders responsible for their care resulted in a streamlined process.
Diligence was also evident in players who disclosed their suspected concussions even when they were not sure, or really did not want to, and followed the GRTP nonetheless. For GPs, diligence was evident when they retested the player's baseline and gave the player adequate advice and guidance. For physiotherapists or coaches, diligence was demonstrated by spotting for concussions, removing players from play regardless of negative pressure, or not letting players RTP without receiving formal clearance information.
Communication. Efficient communication was identified as a key part of the CMP, reported in numerous phases and often related to the quality of relationships I think overall, that all worked fine for us. As I say, I don’t know how it would work without [GP] and [school nurse] here. And I suppose another thing too, is that we’ve got a very good support network, it's got the support services … If we’ve got guys concussed, we might have even had the notice up here, we say, look, he's been concussed on a Saturday, so we talk about it at a staff meeting on Monday morning. (B5—App manager)
In the immediate management phase, the process was often facilitated by good communication between physiotherapists and parents, while in the sub-acute phase, physiotherapists placed great value on timely communication between themselves and GPs. However, multiple stakeholders, including coaches, nurses, physiotherapists, and parents reported gaps in communication that made following the protocol difficult. Several physiotherapists felt they needed better, and timelier, communication from GPs.
Confidence. Confidence in dealing with a certain situation was often linked to the stakeholder's knowledge or the unpredictable nature of concussion and was evident in the process of logging concussion, diagnosis, or making decisions about the player's readiness to RTP: I’m acutely aware that when you hit that button, that there's a process in place. So, you know that, so you know that that's a binary event, that sends you this way as opposed to the other way, and that's just the reality of it … So, then you start to have to decide, “What do I?” Yeah, so in your own mind I think, “Okay, so what is it that I, where does that line…” So you have to put a line in a grey spectrum, if you like. And so where do you put that? And I put it, I decided, in my mind, prior, that this is what I was going to do. So, if I suspect, if it was a suspected, so if there was a, I don’t know, any more than about a 25% chance that it was a concussion, then I'd probably push it that way. So I was, there are definitely times it would be like, “Hmm, this could be, but I think it's probably not.” So, what with the probably not, it's a probability thing at the end of the day, that's the way I look at it. You’ve got to come up with something, in your own mind. (C30—Physiotherapist)
Outcomes
Two themes describing both favorable and unfavorable outcomes were identified.
1. Hitting the target Player: Yeah, no like it was good, I had [Physio] as my physio, he was … helped me out a lot, like took me through everything, like my steps and everything. And then obviously going through to the clinics and stuff. It was quite good, yeah. I was pretty unsure of it at the start, so that kind of made me a bit uneasy about concussion and everything. So just knowing that I was in pretty safe hands… (C29—Player)
Optimally managed concussion and safe RTP. As a key theme, most players felt “safe” and “taken care of” during their progression through the CMP regardless of the feelings they had around having to stand down.
This was echoed by parents and coaches, who appreciated having the reassurance that the player had progressed through a structured recovery process and was cleared to safely RTP.
More knowledge and awareness around concussion, and safer concussion behaviors. Several stakeholders reported that their experience with the CMP facilitated favorable attitudes and behaviors and enhanced their knowledge about concussions. All the boys have bought into it massively, which was really positive to see and I think there is just much more awareness now around getting the process right for a return to play and what I've seen in previous years and obviously this has helped massively with that. So that's, I think just the awareness now of our players is so much higher than what it used to be. (C9—Player)
2. Missing the mark
Dissatisfaction with process. Dissatisfaction with process was often due to players and parents not believing they had, in fact, sustained a concussion. For these players, the CMP felt like “a box that had to be ticked,” and caused frustration being kept away from play: Well, it was helpful in terms of, it gave me the thing I needed to get back, but I don’t think I really got anything out of it because I wasn’t … Maybe that would be different if I actually was concussed, yeah. But for me, it was just getting the box ticked off… (C33—Player)
Importantly, parents and GPs felt that these experiences could be a barrier to future disclosure. Parents talked about feeling as if “the trust was now broken” as their child may avoid disclosure because they want to avoid the strict protocol: He was gutted with the three weeks stand down. That worried me, if there are degrees of concussion, boys in particular, hiding these symptoms because they’ve now learned what the symptoms are. [Player] quietly conceded to his father that he's had worse … He didn’t consider he was concussed on this occasion, he's had worse knocks, where he's passed the tests. He is now very familiar with those things. They’re at this age where rugby is everything, and they’re not sensible. The results for him were so emotionally devastating. He wasn’t available for that final [game]. Is it possible to slice the onion a bit more finely in terms of those concussions? Or is it all, “we didn't like the look of that. You're out for three weeks.” I know they Have to be careful, but if there's an over-reaction to it, the boys will hide the symptoms. (C46—Parent)
Process gap. A process gap meant a step(s) of the CMP were missed or inadequately executed. For example, not all players had a baseline test, or in some instances, GPs did not use the GP Portal or access the player’s baseline in the diagnosis visit. Some GPs reported time constraints as a barrier to the diagnosis visit, technological challenges using the portal, and or players arriving without their system-generated codes, making it more difficult to locate them on the portal. In addition, not all GPs were part of the CMP pilot, so although they should receive information when players arrive with their codes, it did not always materialize.
A few stakeholders noted players returning to play before being formally cleared: But I couldn’t actually get clearance for the second or the third week because we never heard back from him [GP]. So I ended up just playing the fourth week without clearance. She [the physio] ran me through the processes of going out training … So we sort of cleared ourselves because we couldn’t hear anything back from the doctor. (C42—Player)
Various stakeholders, especially players, identified a lack of support in the GRTL phase Some players reported going straight back to study or work, and some had difficulties managing symptoms in this time.
Discussion
The aim of this study was to explore the perceptions of key stakeholders involved in the CMP. Various wider contextual factors (governing bodies and healthcare), as well as local, and individual factors, were identified that may affect the implementation of the CMP. In addition, four themes were identified to play an important role in the optimum functioning of the CMP. Collectively, these factors may affect the functioning and subsequent outcomes of the CMP either positively or negatively, depending on whether they are acting as a barrier or facilitator within a specific setting. Both intended and unintended outcomes were identified in this study. Firstly, the majority of participants, including players, felt that concussions were optimally managed, which aligns with the CMP's primary goal. In addition, participants noted that being part of the process cultivated knowledge and safer concussion behaviors. However, dissatisfaction with the process was reported when participants felt the management of the suspected concussion was unnecessary or inflexible and raised concerns that some players may not want to disclose a suspected concussion in the future. From a practical perspective, both intended and unintended outcomes appeared to be the result of a complex interaction between contextual and pathway mechanism factors present within different settings.
Importance of context
These findings have demonstrated the importance of understanding the implementation context as the foundation for the implementation of health interventions such as the CMP. 25 These wide, local, and individual contextual factors may influence the manner in which the CMP functions and ultimately, the outcome of the player.
As part of the wider context, participants appreciated the governing body of the sport leading the charge by providing a supported pathway to manage concussions in the community. Research has shown the importance of top levels of the sports system hierarchy driving injury risk management strategies at the community level. 40 From the outset, favorable perceptions of the governing body built a foundation for buy-in towards the CMP. Despite this appreciation, participants voiced the need for continuous assistance from the governing body in enforcing the protocols, providing resource support for baseline testing, and getting buy-in from stakeholders. Participants felt the message coming from NZR (a respected, authoritative body), would result in better compliance from clubs and schools.
It was clear that physiotherapists and GPs play key roles within concussion management, supporting previous research.41,42 However, accessing these providers was challenging in some contexts. In settings where concussion management programs can be embedded, for example, in a university-based healthcare system, strong resource support and organizational leadership can be influential in the flow of a program 42 but other settings may require additional support. Dedicated primary care concussion clinics were specifically identified as important facilitators of the CMP. Previous research has similarly suggested the important role of such clinics in offering multidisciplinary concussion management, 43 potentially decreasing primary care resource utilization and facilitating more consistent concussion care. 44
As is the case with injury prevention, 33 injury management programs will only be successful if they are adopted by the local context. In this study, local contextual factors were identified that may influence future adoption of the CMP, such as resources, existing policies, relationships, and culture of the club/school which, if favorable, worked to facilitate implementation and flow of the CMP. The extent of human resources available (e.g. to help with baseline testing), and logistical capacity of the school/club often acted as a barrier. Similarly, role multiplicity is common in community sport, 45 and in this study, it acted as a barrier if the stakeholder became overwhelmed with multiple task responsibilities. Of specific concern, was the gap identified in actioning return to learn support in schools. This finding is consistent with other studies indicating the need for guidelines and policies for schools, students, and parents, as well as improved communication with GPs.4,46 The recent Consensus Statement on concussion in sport recommends the implementation of GRTL strategies. 16 Nonetheless, recommendations at a higher level do not automatically lead to the implementation of relevant practice at lower levels. 40 Previous research reported that teachers feel ill-equipped to implement return-to-learn guidelines without specific instructions in the complex school environment. 46 Dedicated strategies are required to assist schools with the implementation of GRTL processes.
An important finding of this study was the influence of individual contextual factors, and the nature of concussion, on the implementation, and outcomes related to the CMP. These factors included the severity of the concussion, and stakeholders’ general concussion knowledge and attitudes. The pathophysiological nature and presentation of concussion make it one of the most complex sports injuries to recognize and manage. 16 Differing presentations and severity of the concussion acted as a catalyst for stakeholder buy-in towards the actual “on-the-ground” operation of the CMP. In this sense, more severe concussions often lead to better compliance with the CMP. Sensitivity towards these variable presentations and the potential consequences of these attitudes and beliefs must be a consideration as players progress through the CMP. Similarly, players’ emotional and physical recovery-related experiences may differ. Numerous post-concussion symptoms identified by athletes may result in difficulty in coping with emotions, school, or their roles in social/sporting environments. 47 These findings reiterate the need for tailored support to enhance players’ experiences.
Coaches and parents play an important role in concussion attitudes and behaviors of players.48,49 As such, they are ideally placed to provide the necessary information and guidance to players when dealing with a concussion. To offer this support, these stakeholders must have favorable attitudes, be knowledgeable about concussions, and have their priorities regarding player welfare aligned. Findings within the broader project showed that stakeholders are aware of concussions and care about their consequences. However, these favorable attitudes and behaviors are often countered by players, parents, and coaches, downplaying the seriousness of concussion and being driven to win, regardless of the risks. 50 Additionally, stakeholders’ general concussion knowledge and awareness may influence the player's management. Research shows that coaches, parents, and GPs, do not always know about or use concussion guidelines.10,51 In this sense, continuous efforts to enhance system-wide concussion knowledge and safe concussion behaviors, may align stakeholders’ and implementers’ vision of what is important when considering player welfare. 52
The CMP “Mechanism”
Identifying the key mechanisms by which a program appears to operate is important for its future development and support. 53 The successful use of program resources depended on the right people to make it work, which included certainty in roles, strong relationships, and trust between stakeholders directly involved in the CMP. In this study, information and guidance on the CMP was essential. Of specific concern was multiple stakeholders’ need for more recovery information specific to returning to school and learning post-concussion. As mentioned previously, there is a need for structured school policies to guide the implementation of GRTL protocols. This may improve the flow of information and guidance during this phase.
Furthermore, the adoption of a program depends more on the end-users’ subjective perception of its’ value or the extent to which they believe the program is better than current practices than it does on the objective evidence of the program's efficacy.26,54 Similarly, in this study, attitudes and buy-in towards the CMP were identified as one of the strongest facilitators towards the CMP's functioning. Importantly, believing in the CMP's goal often mitigated contextual challenges within the implementation process. However, some perceptions of the appropriateness of the policy-related aspect of the CMP acted as a distinct barrier. If players did not believe they were concussed, their overall experience of the CMP was often negative, as it felt they were “just ticking a box.” This study also highlighted the importance stakeholders placed on feeling supported when making concussion-related decisions. In a study evaluating the implementation of concussion guidelines in community Australian football and rugby league, similar challenges were highlighted with parents, players, and coaches disputing or resisting immediate management or RTP decisions, and the difficulties experienced if there is a lack of support for the person making the decision. 55
Finally, diligence, communication, and confidence in the execution of CMP-related tasks were required to facilitate the CMP's flow. These facilitators have previously been identified in the implementation of concussion policies in schools. 56 Again, these factors may be heavily influenced by contextual factors. For example, stakeholder confidence in executing specific tasks may increase as the CMP continues and is also influenced by stakeholders’ general knowledge of concussion management, and the availability of human, or other, resources.
Implications
Access to structured concussion management support remains a major barrier for athletes across different sports47,57,58 and highlights the need for context-sensitive interventions, such as the CMP. For the future of the CMP, the local context is an important consideration. Key stakeholders within the local context are optimally positioned to identify where the flow of the CMP can be facilitated within their own setting. Careful consideration of the responsibilities, level of resource and logistical support, and existing medical infrastructure, should be included in a context-specific plan. The extent of responsibilities may be challenging for individuals, especially those with multiple roles, particularly in female schools where there are often less resources and support. Establishing a multi-disciplinary team with a strong passion and competence in this area is vital. 42 Physiotherapists play a key role in concussion management. 59 Future work should consider how this profession could be optimally involved and supported in this process.60,61 Active engagement of currently under-utilized stakeholders such as school nurses, or other opportunities for task-shifting among stakeholders must be considered. 62 Concussion clinics may play a pertinent role in this respect. In addition, the heterogeneous nature of concussion means it may affect various systems in the body with varying levels of severity. A multimodal clinical assessment and rehabilitation approach, ideally by a multidisciplinary team, can provide a comprehensive and streamlined service to players, especially for those with prolonged symptoms.6,43,60
Local implementers should bear in mind that the nature of the concussion and the individuality of players, as well as general concussion attitudes and knowledge of stakeholders, may influence the CMP flow. Future work should consider strategies facilitating the provision of information and guidance, communication between stakeholders, and additional multi-level concussion education initiatives within local contexts. The findings showed the value that stakeholders place on the CMP and the buy-in towards its execution may mitigate many of the potential contextual challenges identified. However, a system-wide approach to concussion management cannot rely only on a “top-down approach,” but also relies on the attitudes and behaviors of players. However, some of the underlying drivers of player behavior are difficult to influence. For example, “warrior mentality” (putting your body on the line or playing through injury) has been described as a culturally engrained component of rugby.50,63 This mentality may override the knowledge players possess on concussion risks.64,65 For these reasons, we should continue to invest in opportunities to model positive change for players. Therefore, the focus of policy, education, and support should be emphasized for the key stakeholders around the players, such as coaches and parents, whose responsibility it is to look after them. It is concerning then, that although these stakeholders value keeping players safe, the underlying discourse of “winning” or “performance” is never far behind.
We cannot afford to have these discourses continually creating an internal battle for some key decision makers, and just hope that player welfare will always come first. It can be argued that to keep the majority of players safe, some stakeholders may have to accept the guidelines regardless of whether they agree with them. However, should this mean that players do not want to disclose in the future—the overall success of the CMP may be affected. These are important mechanisms for the growth and support of the CMP, and future research in this regard is warranted.
We believe that the findings of this research are significant in a number of ways. This study shows that various factors, across a community rugby system, work together to influence the management of concussions. Instead of only focusing on individual aspects of concussion management, such as improving player disclosure, or access to healthcare, multiple factors must be considered collectively to enhance the care we provide for players. The results of this study may serve to initiate discussions within various community sporting contexts on how concussion management practices within their respective environments may be approached and enhanced. We also feel that this research creates impetus for other qualitative researchers to not shy away from “big data.” Studies into individual stakeholders’ (e.g. players, coaches, etc.) can provide voice and insight into specific aspects of a phenomenon, but often do not take into account the impact of the wider system they operate within. Parent, coach, and player behavior does not occur in a vacuum, and ultimately, we believe a system thinking approach conducted qualitatively, can offer insights more conducive to bringing about real on the ground change to practice, which is the goal of this overall program of research.
Limitations
The analysis of this project adopted the principles of a realist evaluation to conceptualize the various factors that may play a role in the outcomes of a study. It was applied in a broad fashion, across the system, without focusing on individuals’ pathways through the CMP. The findings are intended to highlight high-level factors that play a role in CMP implementation, as opposed to an in-depth exploration of unions or stakeholder groups. Additional quantitative investigations may assist in drawing conclusions about the progression of players through the CMP. Nonetheless, the value of this study lies in the contribution of multiple stakeholder groups’ views to provide a deeper contextual understanding of factors influencing the implementation and outcomes of the CMP.
Conclusion
In this study, the principles of a realist evaluation contributed to an understanding of the context and specific process mechanisms present in the implementation of a concussion management intervention. Tailoring programs according to these understandings is an important step towards context-sensitive interventions that consider the end-users’ perception of the applicability and acceptability of the program. We have shown that the implementation setting stretches beyond the culture and capabilities of the local context, and that wider contextual issues and individual factors, including the characteristics of the injury, play an important role. Overall, participants found the CMP valuable. However, the acceptability of certain policy-related aspects and the underlying attitudes associated with these perceptions; uncertainty of roles; lack of information and guidance; communication flow, and resource support are areas requiring further development.
Supplemental Material
sj-docx-1-spo-10.1177_17479541231218518 - Supplemental material for Managing concussion in the real world: Stakeholder perspectives of New Zealand Rugby's concussion management pathway
Supplemental material, sj-docx-1-spo-10.1177_17479541231218518 for Managing concussion in the real world: Stakeholder perspectives of New Zealand Rugby's concussion management pathway by Danielle Margaret Salmon, Simon Walters, James Brown, Zachary Yukio Kerr, Amanda Clacy, Sierra Keung and S John Sullivan, Johna Register-Mihalik, Chris Whatman, Gisela Sole, Marelise Badenhorst in International Journal of Sports Science & Coaching
Supplemental Material
sj-docx-2-spo-10.1177_17479541231218518 - Supplemental material for Managing concussion in the real world: Stakeholder perspectives of New Zealand Rugby's concussion management pathway
Supplemental material, sj-docx-2-spo-10.1177_17479541231218518 for Managing concussion in the real world: Stakeholder perspectives of New Zealand Rugby's concussion management pathway by Danielle Margaret Salmon, Simon Walters, James Brown, Zachary Yukio Kerr, Amanda Clacy, Sierra Keung and S John Sullivan, Johna Register-Mihalik, Chris Whatman, Gisela Sole, Marelise Badenhorst in International Journal of Sports Science & Coaching
Footnotes
Acknowledgements
The authors acknowledge the support of the high schools for working with us and the players, coaches, physiotherapists, volunteers, parents, teachers, general practitioners, and nurses who volunteered to participate. We would also like to thank the NZ Provincial Rugby Unions who agreed to participate in the study and for their assistance with the recruitment of the schools. We would also like to thank the many research assistants who assisted with the data collection and Christina Sutherland and Jason Chua for assisting with the coding of the data
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: DS was employed by New Zealand Rugby for the duration of the study. Funding for this study as part of the NZR Community Concussion Initiative was provided by World Rugby, New Zealand Rugby Foundation, and ACC through the RugbySmart program. The funders were not involved in any aspect of the design or conduct of the study, or the interpretation of the findings.
Supplemental material
Supplemental material for this article is available online.
Notes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.