
Abstract
The importance of considering information related to athletes’ biological maturation within talent identification and development processes is frequently emphasized by both sport scientists and practitioners. Although there is evidence for the use of objective diagnostics for assessing biological maturation, little is known about its subjective determinations by coaches. Such approaches are particularly relevant when scientific support is limited. Therefore, the current study aimed to compare a practical subjective approach (coaches’ eye) to assess biological maturity timing (BMT) with objective reference diagnostics (MRI). For this purpose, data were collected from 63 male elite soccer players of the U12 and U14 age group who were part of the German talent promotion program. Players’ BMT (i.e., skeletal – chronological age) was assessed by MRI and a subjective rating of two coaches. Data analyses revealed high-rank correlations (rs = .55; p < .001) for the total sample as well as for U14 players (rs = .65; p < .001) and moderate rank correlations for U12 players (rs = .42; p < .05). Single case analyses showed substantial agreements between the diagnostics. However, particularly for U12 players, judgements did not always correspond with the MRI rankings. Although coaches seem to have the ability for recognizing the earliest and latest maturing players in the sample, inconsistencies exist in single cases, especially for players that were identified on-time by objective MRI diagnostics. Although utilizing subjective coach assessments as an alone-standing tool to assess a player's BMT is not recommended in applied practice, its use can be beneficial when applied in addition to common objective diagnostics or in circumstances where objective data are not available.
Introduction
In the context of competitive soccer, national federations invest high financial and human resources in the promotion and development of talented youth players. 1 This investment causes a large expense for federations as well as for players themselves. Therefore, it is important to ensure the effectiveness of talent development programs, for example, in terms of an efficient and fair selection of young players. 2 Scientific studies point out that such selection processes present a huge challenge requiring a sound understanding of the young players’ development, including their biological maturation.1,3,4
The separation of youth players into chronological age (CA) groups based on an annual cut-off date reinforces this notion as research on the Relative Age Effect (RAE) highlights. 5 The RAE6,7 refers to the overrepresentation of early-born players in selected squads which may be attributed to earlier born players’ advantages associated with age and experience already present in (early) childhood. On top of this, the non-consideration of a player's individual biological maturity status regardless of his or her CA represents an even more critical cause for a selection bias towards biologically advanced young athletes in talent squads. 8
Biological maturation refers to the progression towards the adult state and can be defined with respect to status, tempo and timing. 9 While biological maturity status describes the current stage of maturity an individual has achieved, tempo refers to the rate at which the maturation process progresses. 9 Timing describes specific maturational events which occur at a certain point of time at a different CA for every athlete. 10 For instance, such events include athletes’ estimated age at peak height velocity (APHV), which occurs at a lower CA for early maturing players compared to their late maturing counterparts.
The emergence of the selection bias in terms of biological maturation operates independently from relative age.11,12 Recent evidence from talent research in soccer suggests that relatively older (academy) soccer players are not beneficiaries of advanced maturation. 12 Indeed, maturation biases and those by RAE do not emerge at the same age. Johnson et al. 13 point out that individual variation in maturity status has a higher impact than the RAE when selecting players. In the pubertal stages in which rigorous and important selection processes take place, 14 the differences in players’ skeletal age could vary up to six years.15,16 In practice, these interindividual differences may lead coaches and talent scouts to select early-matured players due to performance advantages such as better sprinting and jumping ability through further developed physiological attributes based on their subjective evaluation of players’ skills/performance.17,18 This assumption finds support in the studies by Parr et al. 11 and Radnor et al. 19 who showed that physical performance tested via objective diagnostics (e.g., 20 m linear sprint) was closely related to the players’ maturity status in comparison to their relative age. In the worst-case scenario, even highly talented players experience less support and attention compared to their older counterparts. Thus, they may get deselected due to their time-delayed biological development in comparison with their on-time or early-developed peers. Consequently, talent research has continuously called for the consideration of players’ biological maturity status within talent identification and development programs of sports organizations. 20 However, a major challenge facing scientists, practitioners (e.g., coaches and talent scouts) and sports organizations is to find suitable diagnostics for determining this maturity status. 10 Such diagnostics should be not only both reliable and valid but also well implementable in practice.
Various methods are proposed that can assess different dimensions of biological maturity status objectively (e.g., skeletal age [SA] or somatic age 10 ). Measuring SA by using x-ray-images of the left handwrist is currently regarded as the most objective method.4,21 Due to ethical concerns such as exposing healthy children to (unnecessary) radiation, the implementation of this method in youth athletes is difficult and not feasible in some European countries such as Germany. 22 In response to this concern, several authors23,24 suggest that images of the handwrist can be produced reliably on the basis of radiation-free magnetic resonance imaging (MRI) diagnostics. 25 In practice, this reference method is from an ecological point of view very expensive and requires a lot of time. Therefore, there is a need for less technical and less costly methods to measure maturity status via SA. Here, using recently developed ultrasound diagnostics is considered as a promising alternative method.26,27 Besides SA measurements, an alternative assessment of maturity status is the determination of somatic age. 10 Commonly utilized methods are the estimation of individual APHV 28 as well as the percentage of predicted final adult height (PAH 29 ). Those methods are mostly used by practitioners from international soccer talent promotion programs. 3 In this context, recent research by Leyhr et al. 30 evaluated those objective diagnostics in youth soccer players (U12 and U14 age groups). The study revealed that both ultrasound diagnostics and the estimation of APHV and PAH sufficiently agree with MRI-method at a group level, while caution is necessary when analyzing single cases.
From a practical point of view, besides such objective diagnostics, it is common that coaches evaluate players based on subjective criteria, for example, in terms of biological maturation or sports performance. Related to the latter, recent studies compared subjective ratings of different physical or technical performance factors with objective diagnostics and highlighted the benefits of such approaches.31–33 However, research that evaluated assessments of biological maturation by holistic subjective expert judgements in talent research in soccer is scarce. One possible approach is that coaches categorize players in early, on-time and late maturing players with reference to their biological maturity timing (BMT). Specifically, coaches could evaluate their players independently according to certain characteristics (e.g., morphology). Such subjective assessments should be based on visible indicators from the existing scientific literature, like for example anthropometric and morphological measures used in the Khamis–Roche formula. This specific approach utilizes empirical findings showing that during the growth spurt the lower extremities grow first before the trunk. There are also other factors to look out for, such as changes in secondary sexual characteristics or changes in body structure (e.g., increase in fat-free mass, shoulder width).16,29,34 To date, the one study addressing this issue found a moderate correlation between coaches’ ratings of U15 youth elite Swiss soccer players’ BMT and objective assessment methods (i.e., x-ray diagnostics and APHV estimation). 20
Nevertheless, a further comprehensive evaluation of these expert judgements in comparison to accurate objective diagnostics is still pending. As subjective assessments offer advantages from an economical perspective, they may indicate important insights in circumstances where it is not possible to gain objective information on players’ biological maturity. For instance, coaches and scouts may have problems in evaluating their players on the pitch and they may not have access to more objective methods. In line with this, the question arises of how accurate subjective holistic assessments by coaches may determine players’ BMT. Particularly in players’ development phase around the APHV, it seems necessary to gain evidence as to whether coaches are able to recognize morphological characteristics that allow them to determine an individuals’ BMT. As those may differ depending on the current development phase it is worthy to perform evaluations in diverse age groups. Therefore, the aim of the present study was to evaluate the agreement of BMT assessed by objective MRI diagnostics and the subjective judgements by coaches within a sample of highly selected youth soccer players in the U12 and U14 age groups. Besides a group-level perspective, a focus was given to the analysis of differences between the objective and subjective assessments on the individual level (i.e., single case analyses).
Materials and methods
Sample and procedures
The study sample consisted of N = 63 male youth soccer players (12.4 ± 1.1 years old) who were part of the German soccer talent promotion program. Players were born between 2006 and 2008 and belonged either to the U12 (n = 32, 11.3 ± 0.3 years old) or U14 age group (n = 31, 13.4 ± 0.3 years old). In these age groups, the talent promotion program comprises two important levels: competence centers where talented regional-level players get weekly an additional training session by qualified DFB soccer coaches; and youth academies. In order to get a representative sample of the promotion program, the sample included a balanced amount of competence center (U12: n = 16; U14: n = 16) as well as youth academy players (U12: n = 16; U14: n = 15).
All data were collected within two weeks at the University hospital of the fourth author's institution (MRI data) and at the competence centers or youth academies (subjective coaches’ rating). The MRI testing took approximately 15 min for each player. Participation in the study was voluntary and could be declined at every time point. Players’ legal guardian/next of kin provided written informed consent for the collection and scientific use of the data. The research was approved by the ethics committee of the Faculty of Medicine of the fourth author's institution.
Measures
MRI
A radiation-free MRI of the left hand and wrist of each player was taken. The conventional Tanner-Whitehouse-2-method was then used to determine players’ SA (to the nearest 0.1 years; for a detailed description of the measurement protocol, see Leyhr et al. 30 ). The average of three ratings by independent radiologists (ICC = .988, 95% CI = [0.980; 0.992]) served as players’ SA according to MRI. Players’ BMT was calculated by the difference between SA and CA. 35
Coaches’ rating
The subjective rating of BMT was performed by coaches who were responsible for the coaching of a respective player. All coaches held UEFA-B+ or a higher level in soccer. Specifically, two coaches (i.e., head and assistant coach) of a player's respective team independently classified the player in a holistic way into early, on-time or late maturing. Thereby coaches orientated themselves on certain characteristics of players’ body composition (i.e., muscle mass, body height, body hair and larynx expression). The agreement rate for the two coaches was 65.1% (Cohen's κ = .43). Whenever the ratings of the two coaches disagreed, a third coach from the player's competence center or youth academy was contacted (e.g., coach of another youth team in the same competence center or a further assistant coach in the youth academy). This coach evaluated the player independently from the two other coaches and his or her rating represented the category of BMT for the respective player.
Data analysis
Data were analyzed utilizing IBM SPSS version 26. Players’ BMT according to objective MRI diagnostics as well as players’ subjective BMT ratings by coaches were considered for a descriptive overview. Correlation analyses (Spearman rank correlations) were performed in order to investigate the relationship between objective BMT assessment by MRI (i.e., SA–CA) and subjective coach ratings for the total sample as well as for each age group (i.e., U12 and U14) separately. Correlation coefficients were classified in accordance with Cohen. 36
Besides this group-level analysis, differences regarding single cases are of high relevance, especially in clinical treatments or sensitive topics such as BMT assessment. 37 Therefore, in order to have a more detailed insight into deviations between the objective reference method MRI and subjective coaches’ ratings, all investigated players were additionally ranked according to their individual BMT outcome by MRI from early (player #1) to late maturing (player #63) and then, compared to coaches’ ratings. This single case analysis offered the opportunity to examine whether coaches’ BMT ratings agreed with the rankings based on MRI. Going beyond the analysis of the total sample, this approach was also followed for the investigated age groups separately. This enabled to detect the potential differences regarding the specific age groups before (i.e., U12) and during (i.e., U14) boys’ average APHV.
Results
Descriptive statistics of players’ BMT according to objective MRI diagnostics as well as players’ subjective BMT ratings by coaches are presented in Table 1. Regarding MRI diagnostics, players of the total sample were, on average, M = 0.6 ± 1.1 years older in terms of SA compared to their CA. Therefore, participants were advanced with regards to their BMT and can be described, on average, as on-time to early maturing. This tendency was also given by coaches’ BMT ratings. Although coaches rated the majority of players on-time (n = 40; 63%) or early (n = 17; 27%) maturing, coaches categorized only six players (10%) late maturing within the total sample. Moreover, significant high-rank correlations (rs = .55; p < .001) between the ranking of BMT based on the objective diagnostics (i.e., MRI) and coaches’ ratings were found for the total sample.
Descriptive overview of players’ anthropometry and BMT according to objective MRI diagnostics and subjective coaches’ judgements.
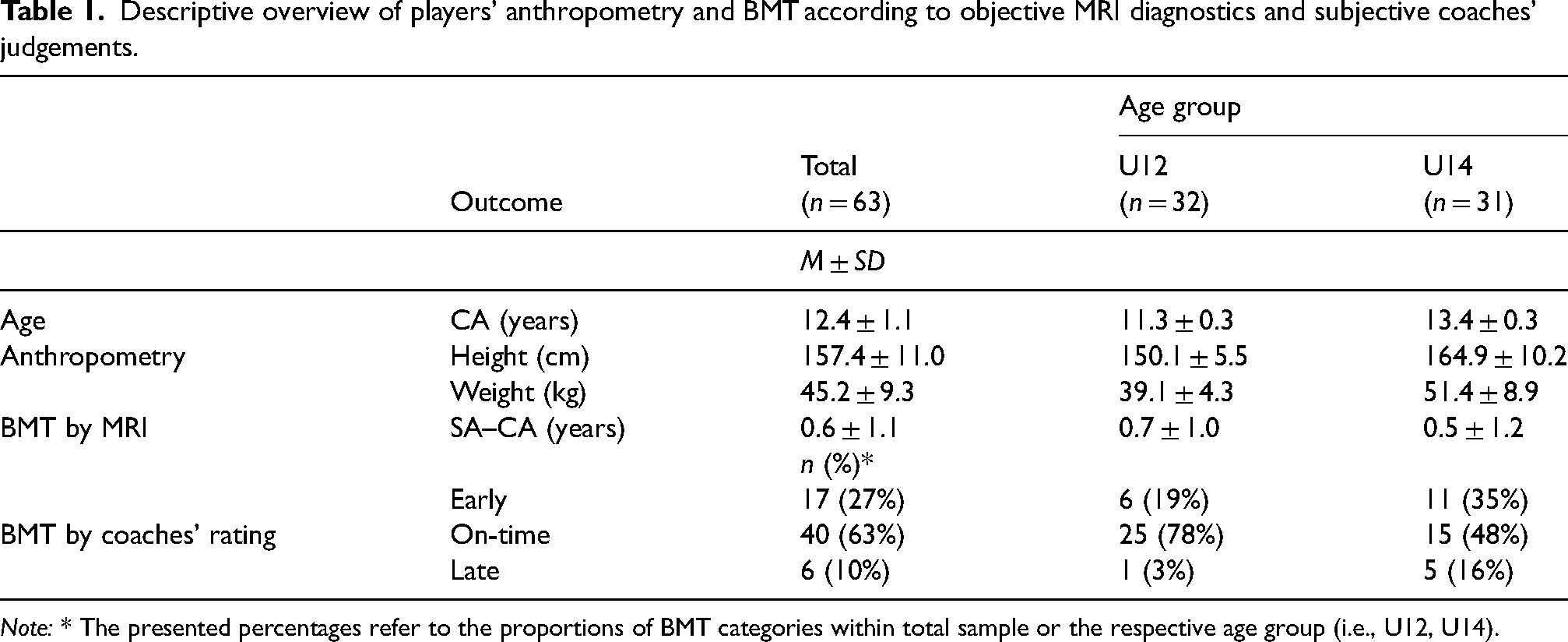
Note: * The presented percentages refer to the proportions of BMT categories within total sample or the respective age group (i.e., U12, U14).
The agreement of the objective MRI diagnostics and subjective coaches’ ratings of players’ BMT at an individual level is shown in Figure 1. First, substantial agreements can be discovered when regarding the total sample (see Figure 1(a)). Most of the earliest maturing players within the total sample identified by MRI rankings were also categorized early by coaches (grey font). That is, among the first 11 players (i.e., ranks #1 to #11) nine individuals were categorized early by coaches. Furthermore, players who were rated late by coaches (black font) were also identified as comparably late maturing by MRI rankings (i.e., #43, #46, #50, #52, #57 and #61). However, when looking at some individual cases, coaches’ judgements did not correspond to the MRI rankings. For instance, two players (i.e., #38 and #48) were rated early by coaches but ranked comparably late according to MRI diagnostics.
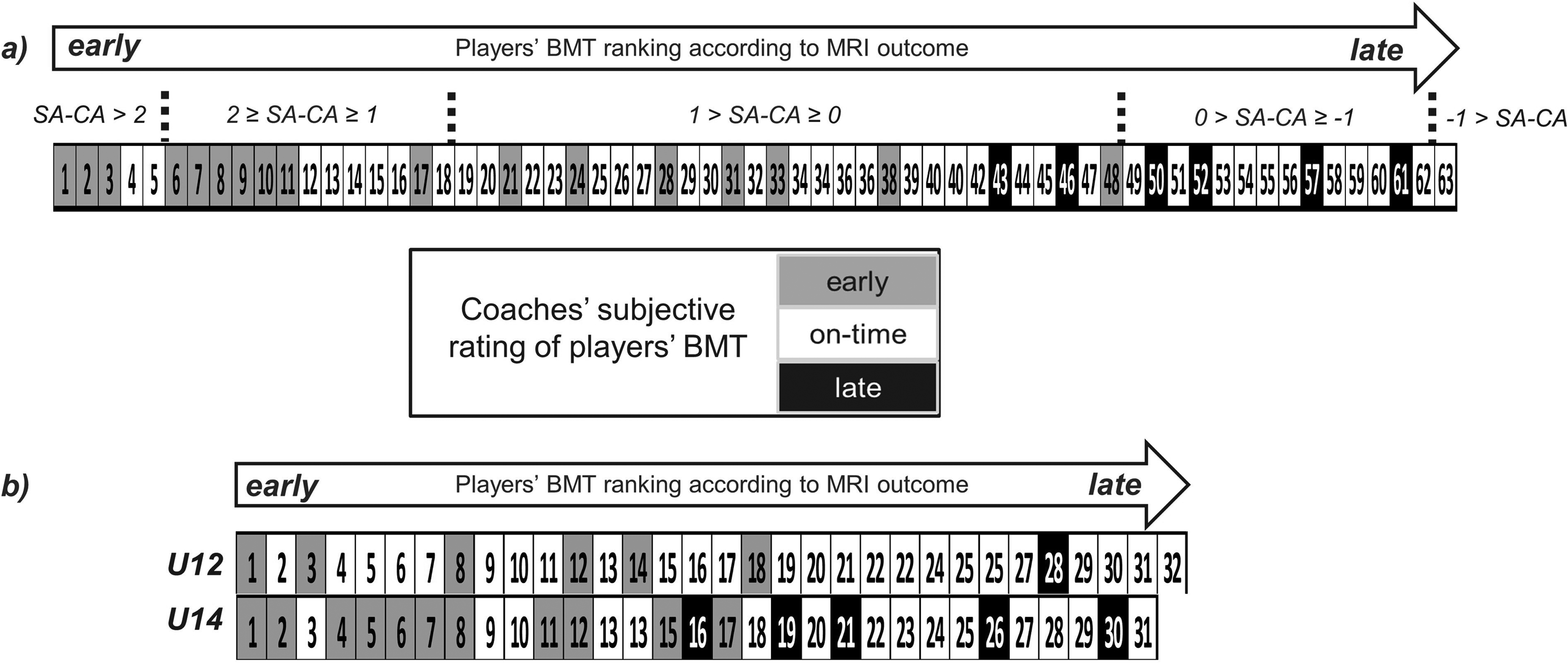
Agreement of objective diagnostics and subjective judgement of players’ BMT (single case analysis). SA = skeletal age; CA = chronological age.
With respect to the separate age groups, U12 players showed, on average, M = 0.7 ± 1.0 years higher SA compared to their CA according to MRI. The difference between SA and CA in U14 (M = 0.5 ± 1.2 years) was slightly, but not significantly lower compared to U12 (t(61) = 1.08, p = .28) and still indicated advanced BMT of the investigated U14 players. A similar result pattern was detected when considering the coaches’ ratings. In U12, 31 out of 32 players (97%) were categorized early (n = 6; 19%) or on-time (n = 25; 78%) maturing. This finding holds true to a slightly lower extent also for U14 (26 out of 32 players: 83%; early: n = 11, 35%; on-time: n = 15, 48%). Besides, only one player (3%) was categorized late in U12, whereas five players were defined as late in U14 (16%). The correlational analyses revealed moderate rank correlations for the age group U12 (rs = .42; p < .05) as well as significant rank correlations indicating a high effect size for the U14 age group (rs = .65; p < .001).
Considering the agreement between MRI diagnostics and coaches’ ratings, similar result patterns were found for U14 age group when compared with those for the total sample (see Figure 1(b)). Seven out of the first eight players were classified early by coaches (exception: #3 was categorized on-time). All late categorized players appeared in the second half of the ranking scale (i.e., rank ≥ #16). Due to the high proportion of on-time categorized players in U12, the result pattern for this age group is only roughly comparable to U14 or the total sample. Nevertheless, except for player #18, all U12 players who were categorized early by coaches (i.e., w#1, #3, #8, #12 and #14). Those covered the first half of the rankings by MRI. Furthermore, the only player classified late by coaches (i.e., #28) was also ranked comparably late by MRI.
Discussion
The present study compared a pragmatic subjective approach addressing the consideration of BMT to a well-established objective BMT diagnostics (i.e., MRI). The study sample comprised a representative talent identification and development environment (i.e., selected youth elite soccer players from the two central institutions of the German TID and TDE program, competence centers and youth academies). The results of the present study provide a scientific rationale for the subjective evaluation of elite youth soccer player's BMT by coaches. Here, utilizing subjective coach ratings as an alternative tool (in isolation) to assess a player's BMT instead of objective diagnostics seems not recommended in practice. However, in line with further research on comparisons between subjective and objective performance assessments in youth elite soccer, 32 its use can be beneficial when utilized in addition to common objective diagnostics.
Comparing coaches’ subjective eye to the reliable and valid objective MRI diagnostics revealed moderate to high Spearman-rank correlations for the investigated sample (rs = .55). This is in line with the relationship found by Romann et al. (rs = .62). 20 In addition, the single case consideration led to the conclusion that coaches seem to be quite capable of identifying youth soccer players in terms of their BMT in those that are notably early or late maturing. Presumably, those players showed some maturity-related characteristics that were already well-developed/still undeveloped (e.g., high/low height or muscle mass, pronounced body hair or larynx). Among players identified on-time maturing by MRI, coaches assigned several individuals to the early or late maturing group. This result pattern aligns with the findings from Romann et al., 20 where the largest lack of agreement existed for on-time players between the objective determination of SA by x-ray diagnostics and the subjective coaches’ ratings.
Regarding the distribution of coaches’ categorizations of players’ BMT, 10% of players (n = 6) within the total sample were identified late. The moderate sample size may have limited the classification of players who were assigned to each category in general. The low proportion of players categorized late is not surprising. Indeed, the average BMT according to MRI in the present study indicates a biased sample in favor of early-matured players (i.e., M = 0.6). That is, on average, players were well over a half year older in terms of SA compared to CA. This finding aligns with further research that recently discovered a prevalence of early maturing players within youth elite soccer programs. 38 In fact, coaches were basically being asked to differentiate between on-time and early-maturing players. That is, effectively, differentiating between two, rather than three categories. On the one hand, the fact that coaches recognized more players as early or on-time and less as late in this study supports the tendency of a well-conducted categorization. On the other hand, it will be important to extend the study to a sample with a greater proportion of late-maturing players.
Furthermore, the proportion of identified on-time players by coaches was very high (78%) in U12 age group and lower in U14. Here, only less than half (48%) were allocated to the on-time category. This can possibly be attributed to the beginning of the growth spurt (i.e., on-set) that had already been reached by many players in the U14 but not in the U12 age group. This is due to the fact that the average age of players’ on-set of the growth spurt is 12.8 years. 39 If the on-set had already been passed by a player, coaches might have identified visible player characteristics more easily that help them to assign players to the correct BMT category. Future work on identifying such characteristics would certainly provide helpful information for coaches to support their subjective ratings of players’ BMT. Vice versa, categorizing players who are currently situated in a development phase before their on-set of the growth spurt (i.e., a major part of the considered U12 players) appears more challenging. Consequently, subjective judgements tend to be more suitable for the U14 and less for the U12 age group. Further, to adequately utilize the subjective approach for evaluating players’ BMT, it seems evident to adjust the assessment criteria specifically to that age group or development phase (especially with regards to U14). Although coaches may have implicit knowledge of players’ physical development through their years of experience, they may lack explicit knowledge of specific characteristics (i.e., muscle mass, body height, body hair, larynx expression) that might be important in properly determining BMT. Here, a future approach could be to comprehensively implement this topic in coach license education. This would raise coaches’ awareness of the importance of the topic and sensitize them to characteristics indicative of players’ BMT. Additionally, it is important to note, that at an individual level, substantial variance in skeletal age among youth players of the same pubertal stage may occur. Therefore, the agreement between indicators of skeletal, somatic and sexual age cannot be perfect.
The method of ranking the players based on MRI diagnostics from early to late in terms of BMT gave additional inside into the agreement of the objective diagnostics and the subjective assessment. While in general, the single case analysis showed good matches when categorizing players, some larger discrepancies between MRI and coaches’ eye exist at an individual level. For instance, the question arises as to why #48 is rated as early by coaches although the MRI diagnostics identified the player comparably late. Indeed, player #48 was relatively tall (i.e., 169.5 cm) compared to the average height of the examined U14 players (M = 164.9 ± 10.2 cm, see Table 1). Therefore, one might assume that coaches’ ratings were influenced by that players’ relatively advanced height or potentially further characteristics (e.g., morphology) relevant for the evaluation of players’ BMT were neglected. It seems evident that future studies aim to investigate to which extent coaches’ BMT ratings are influenced by strong (motor) performance or certain anthropometric characteristics of players.40,41
Briefly summarized, the two following approaches (i.e., correlational analyses and single case analyses) provide a better idea of the accuracy of the subjective coach rating on players’ BMT. Although the correlational analyses showed tendencies to agree with the provided objective methods on the group level, the single-case analyses highlight the limitations of the subjective method, especially when applied to individual cases.
Limitations
Although the current study is characterized by several strengths (e.g., highly skilled sample of youth elite soccer players, use of the radiation-free MRI diagnostics as a reference method, and the involvement of qualified coaches conducting the subjective evaluations) limitations of the study should be addressed. First, the practical constraints such as the availability of players and the permission from their legal guardian/next of kin as well as the high time and cost expenditure and availability for the MRI diagnostics provided challenges in obtaining larger sample sizes. Thus, results are specific to a rather small sample of elite youth soccer players and the generalization to players who, for instance, compete at different levels or are younger or older in terms of age need to be considered with caution. Similarly, the sample size of coaches performing the evaluations was limited. Although the agreement between two coaches was considered satisfying and in case of disagreement also a third coach was involved, it is not assured that the findings would be the same for a larger number of coaches.
Second, players’ ethnicity status was not considered. Researchers controversially discuss the potential influence of ethnicity on existing objective SA assessments. Although Timme et al. 42 emphasize that no impact of ethnicity on SA assessments exists, other studies found significant differences in SA assessments between European and African populations. 43 Some researchers advise to use or develop correction formulas for an adjustment of maturity status assessment methods to a specific ethnicity. 31 Although such objective adjustments are not well-elaborated and validated yet, the subjective rating of BMT may be advantageous in that coaches may implicitly include their knowledge regarding differences in SA for players of different ethnicities. By improving the knowledge of coaches about the different developments of the growth spurt among various ethnicities, 44 coaches might be able to consider this information within their subjective evaluations. In this context, a challenging demand in the future could be creating an overview of development phase-specific (e.g., morphological and phenotypical) characteristics for each individual ethnicity.
Practical implications
Implications for practice can be derived from the present study. Since the use of less costly and affordable procedures is desirable, applying a combination of pragmatic objective diagnostics (e.g., ultrasound- or Mirwald-method) and coaches’ rating could be a reasonable solution that is convertible in daily work practice. Although some problems were detected when coaches evaluated on-time players the subjective judgement could be an appropriate complement to overcome discrepancies existing between objective diagnostics for individual players. Besides, the fact that objective diagnostics show partial inaccuracies even in longitudinal analyses 45 makes the subjective approach a strong and helpful additional method that is based on a holistic consideration of maturity-related characteristics throughout the players’ development process. Especially, in circumstances where it is not possible to conduct objective diagnostics of a players’ maturation (e.g., when scouting and promoting grassroot players), subjective assessments might provide first insights to optimize talent development.
Then, the determination of players’ BMT could be appropriate in terms of time and costs economic way in order to better evaluate the performance of players in CA groups. Assessing players’ BMT enables coaches to band players in more homogeneous groups than in the previously existing CA groups. This classification strategy is currently named as bio-banding 9 and might be useful in various domains of talent promotion. These are conducting new competition formats, grouping players in strength and endurance training to prevent injuries or having a more comprehensive insight into talent identification with respect to drafting players for promotion programs. 3 While, to date, there exist few studies that have evaluated bio-banding in initial trials,46–48 there seems still not only a need for further research supporting the scientific but also practical evidence for the use of bio-banding within talent identification and development purposes. Although bio-banding seems promising, it must be remembered that it should be embedded into a multifaceted, holistic talent development process. Other practical approaches like coach education should be given just as much importance.
Conclusion
Although coaches seem to have the ability for recognizing players who are comparably early or late maturing inconsistencies exist in single cases for players that were identified on-time by the objective MRI diagnostics. Therefore, utilizing subjective coach assessments as an alone standing tool to assess a players’ BMT seems not recommendable in practice. Its practical value, however, is probably the greatest when applied to circumstances where objective data on biological maturity is not available (e.g., in grassroot players). Going beyond that the subjective approach might offer further insights when utilized in addition to common objective diagnostics. Hence, performed together with objective diagnostics that are appropriate in daily practical work within youth soccer (e.g., estimation of APHV and/or PAH; ultrasound-based diagnostics; see e.g., Leyhr et al. 30 ) the subjective approach may provide a comprehensive evaluation of players’ BMT. Especially for case-by-case considerations, a strength of experienced coaches’ judgements lies in the possibility to consider the player in a more holistic way. Such an approach is in line with current studies in which players’ general performance factors were evaluated both subjectively and objectively.31,33 However, further studies are needed to establish sufficiently validated measurements of biological maturation in longitudinal study designs combining both subjective and objective assessments.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the German Soccer Association (Deutscher Fußball-Bund, DFB).