
Abstract
Background and aims:
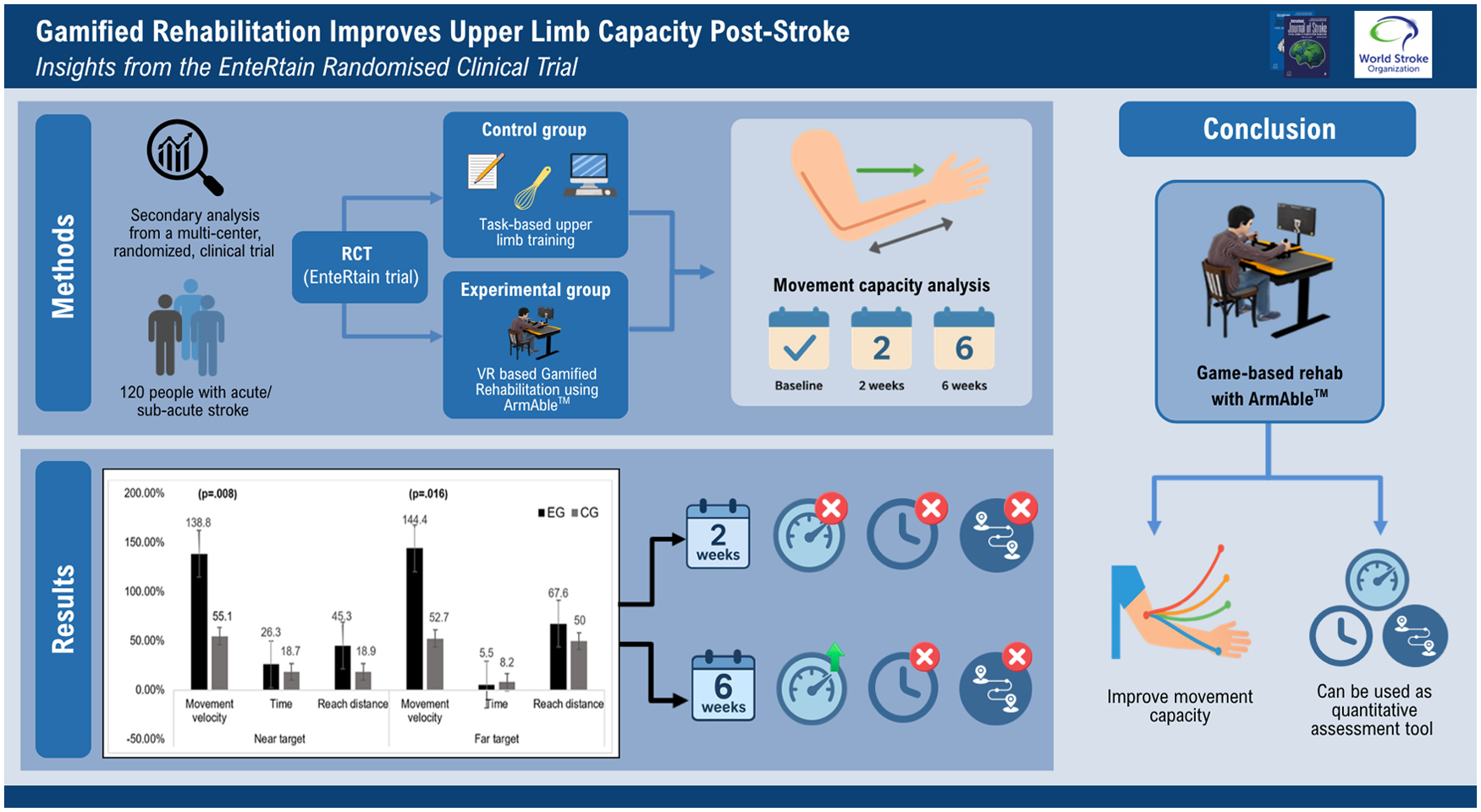
Although many gaming systems for early stroke rehabilitation capture kinematic data, studies on upper limb (UL) movement capacity analysis after virtual reality (VR)-based gaming interventions remain limited. This study is a secondary analysis of the EnteRtain randomized clinical trial and aims to examine the effects of gamified rehabilitation using a low-cost arm rehabilitation system compared to task-based training on UL movement capacity in individuals with acute or subacute stroke.
Methods:
This secondary analysis used data from a randomized, multicenter, single-blind clinical trial involving 120 participants (91 males) with unilateral stroke and an UL Brunnstrom motor recovery stage ⩾1 to ⩽5, recruited from four centers across India. Participants received either gamified training with the ArmAbleTM device (experimental group; n = 64) or task-based training (control group; n = 56), alongside conventional therapy for 2 h/day, 6 days/week, over 2 weeks, followed by 4 weeks of home-based UL rehabilitation. Movement capacity outcomes (reach distance, time, and movement velocity) were assessed by blinded evaluators at 2 and 6 weeks and analyzed using a linear mixed-effects regression model.
Results:
At 6 weeks, the experimental group demonstrated significantly greater improvements compared to control group in movement velocity for reaches to both near (mean difference (95% confidence interval (CI)): −2.8 (−5.0, −0.75); p = 0.008) and far targets (−2.7 (−4.9, −0.51); p = 0.016). No significant differences were, however, observed at 2 weeks. Changes in reach distance and movement time were not statistically significant between the groups at any time point.
Conclusion:
Gamified rehabilitation with the ArmAbletm device enhanced UL movement velocity at 6 weeks compared to task-based training in individuals recovering from acute/subacute stroke. These findings support the use of ArmAbletm both as an engaging therapeutic tool and as a quantitative assessment platform for evaluating UL function post-stroke.
Clinical trials registry number:
CTRI/2020/09/027651
Keywords
Introduction
Following a stroke, the occurrence of upper limb (UL) motor dysfunction is between 50% and 80% in the acute phase and between 40% and 50% in the chronic phase of recovery, 1 with only 5–34% of the individuals eventually regaining full UL function following stroke. 2 These impairments make performing daily tasks such as opening a door or drinking a glass of water challenging/more difficult, substantially limiting functional independence and societal participation. 3 Recovery of UL function can occur through behavioral restitution or compensatory strategies, but they differ in the way the task is performed, especially in terms of the quality of the movement. 4 Therefore, differentiation of behavioral restitution from compensation is important to better understand the recovery of UL motor control post-stroke and subsequently design better interventions. 5 Measuring movement quality or capacity during standardized performance assays potentially allows for this differentiation. 5
Standardized clinical scales such as the Fugl–Meyer assessment–upper extremity (FMA-UE) and action research arm test (ARAT) are widely used to evaluate UL function, which are widely accepted, reliable,6,7 and responsive to change.8,9 However, they primarily capture task accomplishment and are limited in their ability to detect subtle changes in movement quality or underlying biomechanical deficits. 10 Technology-aided assessments offer objective and sensitive quantification of movement capacity through kinematic parameters such as the movement time (amount of time taken to complete the task), the path traveled (distance), and speed or movement velocity.11,12 By quantifying UL movement quality and capacity, these systems overcome key limitations of traditional clinical scales and provide a more sensitive method for characterizing motor impairment and recovery. 13
Several of the virtual reality (VR)-based gaming systems used in the acute/subacute phase of stroke recovery can provide kinematic data, thus allowing objective and accurate movement capacity assessment, real-time performance measurement, and UL recovery tracing. 14 The use of VR-based gaming systems as an assessment tool benefits from their standardized instructions, adaptation of tasks according to patients’ functioning levels, and accessibility to immediate feedback. 15 In addition, the Stroke Recovery and Rehabilitation Roundtable (SRRR) advised objective measurement of the quality of UL movement using technological tools to distinguish between restoration and compensation following a stroke. 16 Unfortunately, studies assessing UL movement quality or capacity following VR-based gaming interventions are lacking. In addition, a major limitation of current technology-based assessment tools, especially in low- and middle-income settings, is the high cost of equipment and the skills, time, and calibration needed, which hinder routine clinical use. For such assessments to be practical in clinics or at home, they should use standardized, affordable equipment and require a reasonable amount of time to complete. 17
Recently, a novel, low-cost, interactive gaming device, the ArmAbleTM (BeAble Health Ltd., IIT Hyderabad, Telangana, India), was developed that enables participants to move their arms in the anteroposterior and/or mediolateral directions via the affected arm (unimanual training) or both arms (bimanual training) while engaging in interactive functional games.18,19 While the device provides game-based rehabilitation, it can also measure the UL movement capacity through a short-duration assessment game. To define realistic treatment goals and determine who and when to target for rehabilitation, assessment of movement capacity is really helpful for stroke patients, their caregivers, and clinicians and increases the motivation while promoting evidence-based practice.16,20
In our recent randomized clinical trial, we found that game-based rehabilitation with the ArmAbletm device compared to task-based training was effective in enhancing UL function following acute and subacute stroke when evaluated with standardized clinical scales (FMA-UE and ARAT). 21 However, evidence regarding its impact on movement quality and capacity remains limited. Furthermore, there is ongoing equipoise regarding whether game-based rehabilitation provides advantages over conventional task-based training when assessed with movement capacity variables, especially during the acute and subacute stages of stroke recovery. Therefore, this secondary analysis from the EnteRtain randomized clinical trial aimed to investigate the effects of game-based rehabilitation using the ArmAble device compared with task-based training in improving UL movement capacity following acute or subacute stroke.
Methods
This study was a part of the EnteRtain trial, 21 which was approved by the institutional ethics committee, Kasturba Medical College and Kasturba Hospital (IEC-328/2020), and registered in the Clinical Trial Registry-India (CTRI/2020/09/027651).
We included 120 participants who were a part of the EnteRtain trial, with acute (1–7 days post-stroke) or subacute (7 days to 6 months post-stroke) unilateral stroke, between the ages of 18 and 80 years, of either sex, with ischemic or hemorrhagic stroke, some degree of UL weakness ranging from Brunnstrom motor recovery stage (BMRS) ⩾1 to ⩽5, a stroke severity score >6 on the National Institute of Health Stroke Scale (NIHSS), a Montreal cognitive assessment (MoCA) score ⩾26 points, and those recruited between October 2022 and January 2023 from the physical therapy departments of four stroke rehabilitation centers located across India.
The methods used have in detail been published elsewhere.21,22 In short, this was a multicentric, single-blinded, randomized clinical trial of 6-week duration, investigating an experimental group for “game-based rehabilitation” and a control group for “task-based training.” Participants were stratified and randomized to receive either intensive, functional, gamified UL therapy using the ArmAbletm device or conventional UL task-based training, each delivered under therapist supervision for 45–60 min/day, 6 days/week for 2 weeks, alongside conventional therapy. A detailed description of the specially developed interactive functional games is provided in Supplemental Material 1. Both groups then completed a 4-week home-based functional UL training program (30 min/day, 6 days/week). Intervention procedures are summarized in Figure 1. More information about the device, games, and the progression of the intervention can be found elsewhere.18,21,22
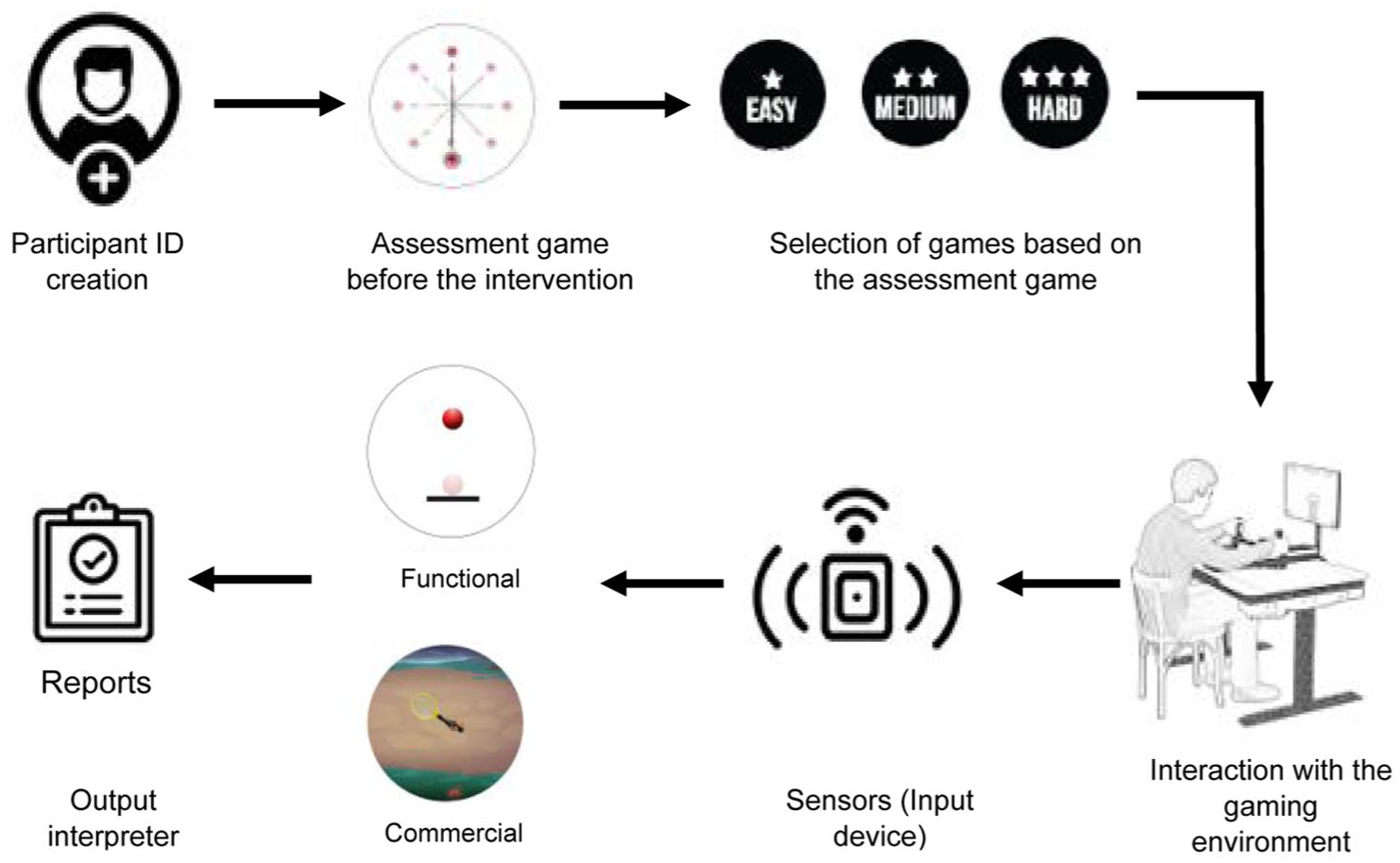
Details of the events occurred during the game-based rehabilitation with the ArmAbleTM device.
The outcome evaluated was UL movement capacity, which was measured with a customized assessment game built within the ArmAbletm device. The assessment game was carried out with two targets (with a circle appearing on the screen as the target): (1) a near target (objects that appeared within a 30-cm radius) and (2) a far target (objects appeared within a 45-cm radius) (Figure 2). The participants would hold the console of the ArmAbletm device, and when the target appeared on the screen, they would be asked to touch the target by moving the console for a minimum of 15 times (to a maximum of 20), 16 after which they would be asked to return the UL to its starting position. Kinematic analysis was performed for the unilateral arm while providing stability via a chest belt to prevent trunk compensation and to promote maximal UL movements. The variables analyzed at the end of the assessment were total reach distance covered (in meters (m)), time taken to complete the assessment game (in seconds (s)), and velocity of the UL movement (meters/second (m/s)).
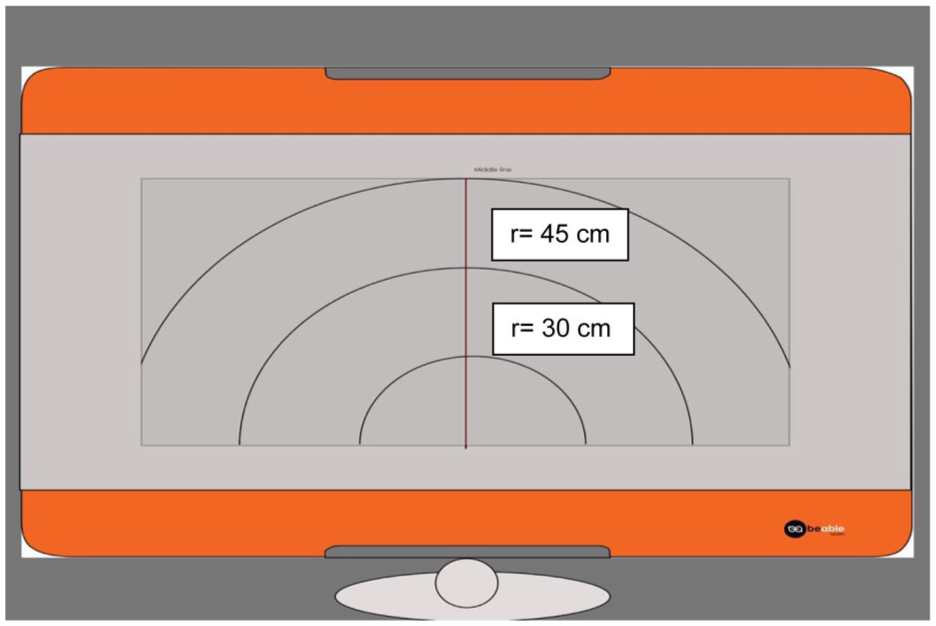
The ArmAbleTM device with different arcs of radii (30 and 45 cm) shown on the monitor screen.
Statistical analysis
Statistical analysis was performed using R Studio (version 4.2.3). Normality of the data was assessed using Q–Q plots and Altman’s criteria to evaluate skewness. A linear mixed-effects model was utilized to examine the relationship between treatment groups and changes in all outcome variables over the course of the three time points. We fitted the linear mixed-effects model with treatment, time, and interaction effect as independent variables for selected outcomes (movement capacity measures such as reach distance, time, and movement velocity). Baseline characteristics were compared using t-tests, Mann–Whitney tests, or chi-square tests as appropriate. In the linear mixed-effects model, adjusted analyses were performed with age, stroke severity, and baseline clinical score entered as covariates for each outcome. The effect size (Cohen’s d) was calculated using the t-statistic and degrees of freedom using standard formulas and interpreted using Cohen’s conventional thresholds as small (0.20–0.50), medium (0.51–0.80), and large (>0.80). 23 Participants unable to perform pre-intervention movement capacity tests but able to complete follow-up assessments were reported descriptively. An intention-to-treat analysis was performed, and the last observation carried forward (LOCF) method was applied to handle the missing data. The level of significance was kept at p < 0.050.
Results
All participants from the EnteRtain trial (n = 120) were included in this study, of whom 115 participants completed the 2-week intervention, and 98 participants completed the follow-up assessment at the end of the 6-week period. However, all participants were included in the final analysis. The baseline characteristics are summarized in Table 1.
Demographics and clinical characteristics of the study participants at baseline (n = 120).
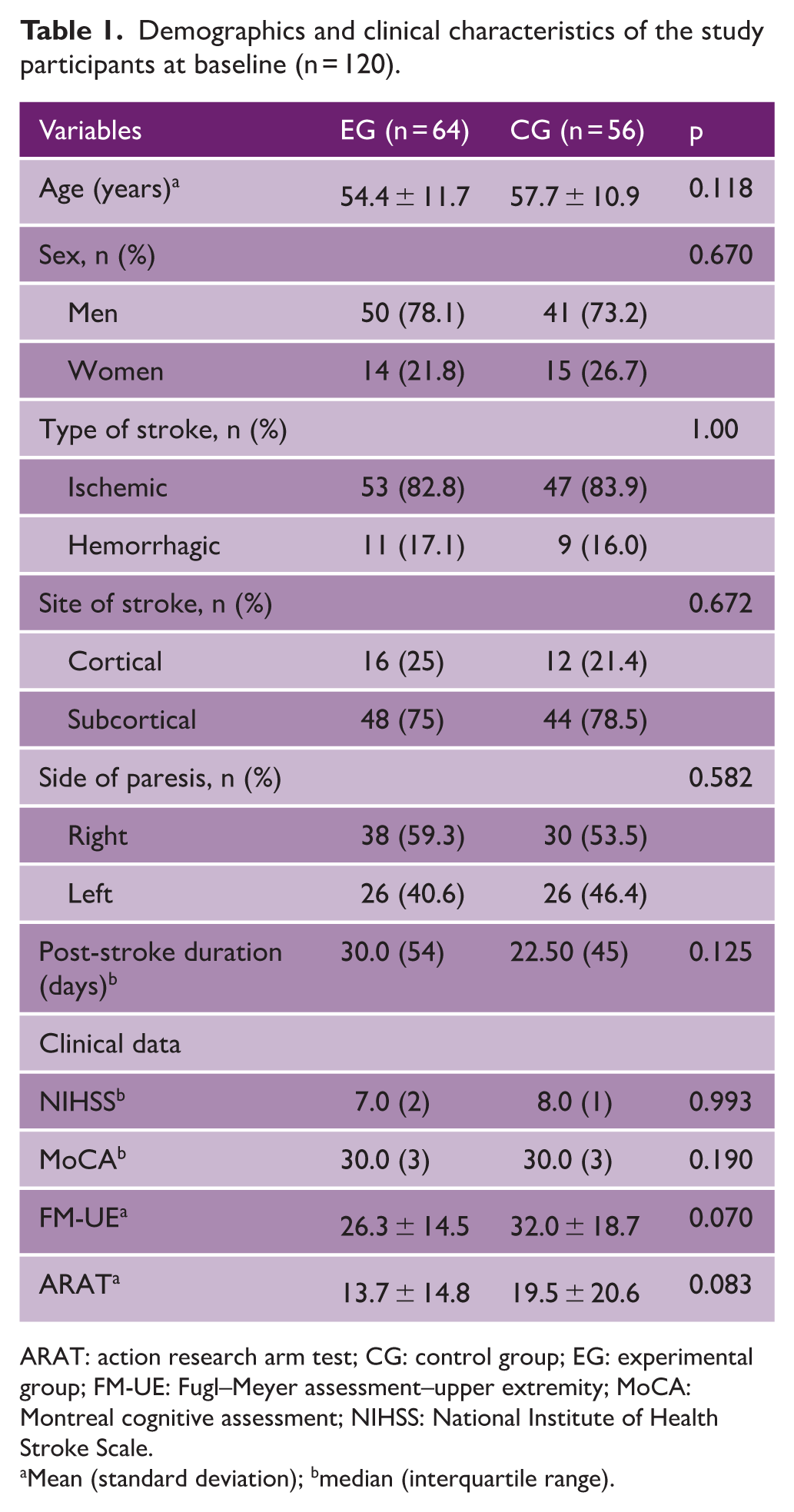
ARAT: action research arm test; CG: control group; EG: experimental group; FM-UE: Fugl–Meyer assessment–upper extremity; MoCA: Montreal cognitive assessment; NIHSS: National Institute of Health Stroke Scale.
Mean (standard deviation); bmedian (interquartile range).
We achieved well-matched groups concerning baseline characteristics (Table 1). With 89.1% and 85.8% intervention participation in the experimental and control groups, respectively, adherence to the intervention was very high. The mean age of the sample was 55.7 years (11.5); 72.5% were men. Upon inclusion, the median (Q1, Q3) time since stroke onset was 29.0 (14.8, 60.3) days.
Table 2 displays the outcomes of the linear mixed model analysis along with the measured mean values at three different time points. Compared with the control group, the experimental group (EG) had significantly better movement velocity at the 6-week follow-up assessment during both near (between-group mean differences (95% confidence interval (CI)): −2.8 (−5.0, −7.5); p = 0.008; d = 0.35) and far target (between-group mean differences (95% CI): −2.7 (−4.9, −0.51); p = 0.016; d = 0.32) reach movements. However, this improvement was not significant at the end of the 2-week post-intervention assessment. The covariates, such as age, severity of stroke impairment (NIHSS score), and baseline score for each outcome, did not influence the study results in a significant way. Figures 3 and 4 present the percentage change in movement capacity from baseline to post-intervention and follow-up period.
Gains in upper limb movement capacity in terms of time, reach distance, and movement velocity of upper limb reach movement at 2 and 6 weeks in the experimental and control groups (n = 120).
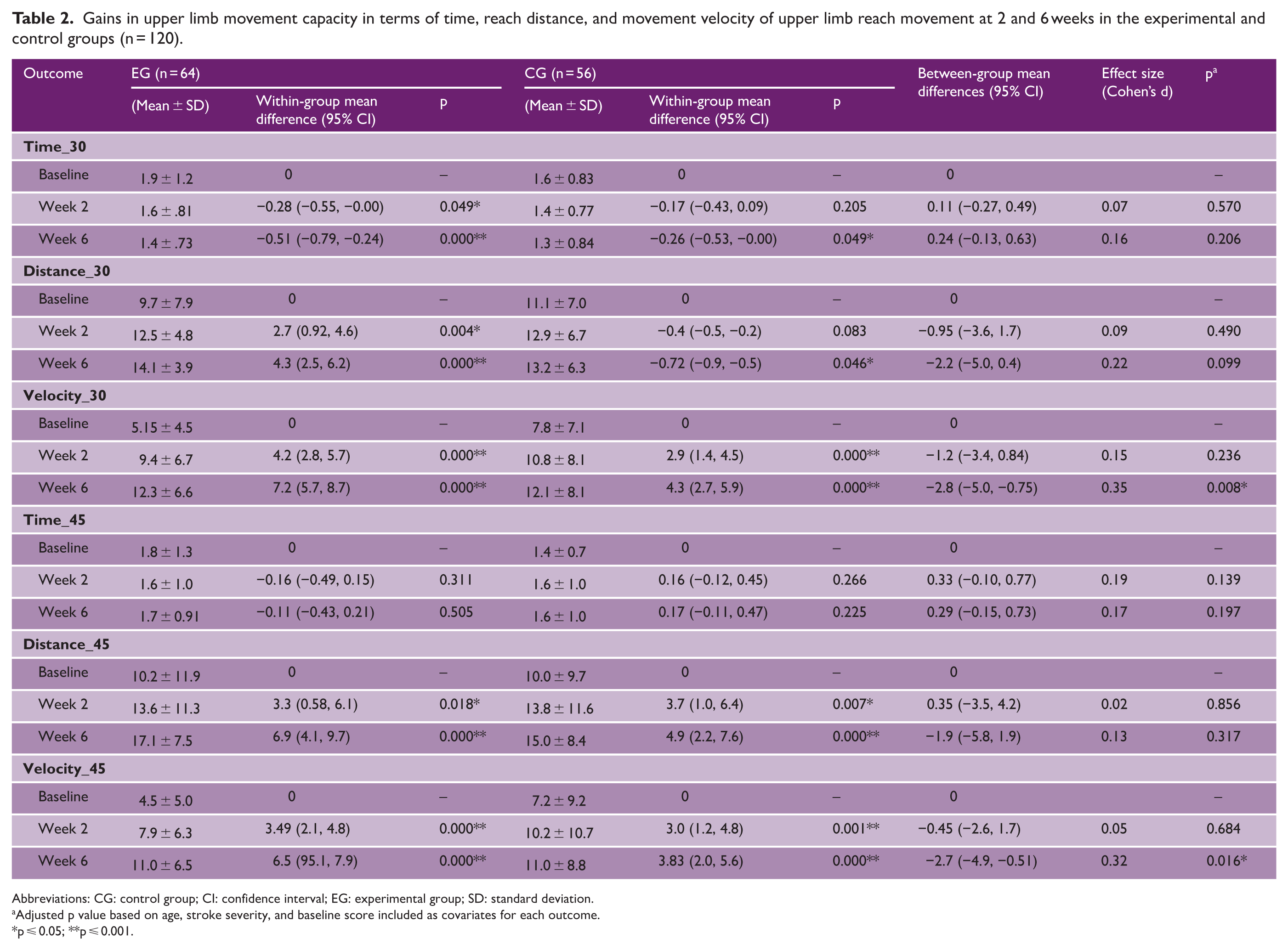
Abbreviations: CG: control group; CI: confidence interval; EG: experimental group; SD: standard deviation.
Adjusted p value based on age, stroke severity, and baseline score included as covariates for each outcome.
p ⩽ 0.05; **p ⩽ 0.001.
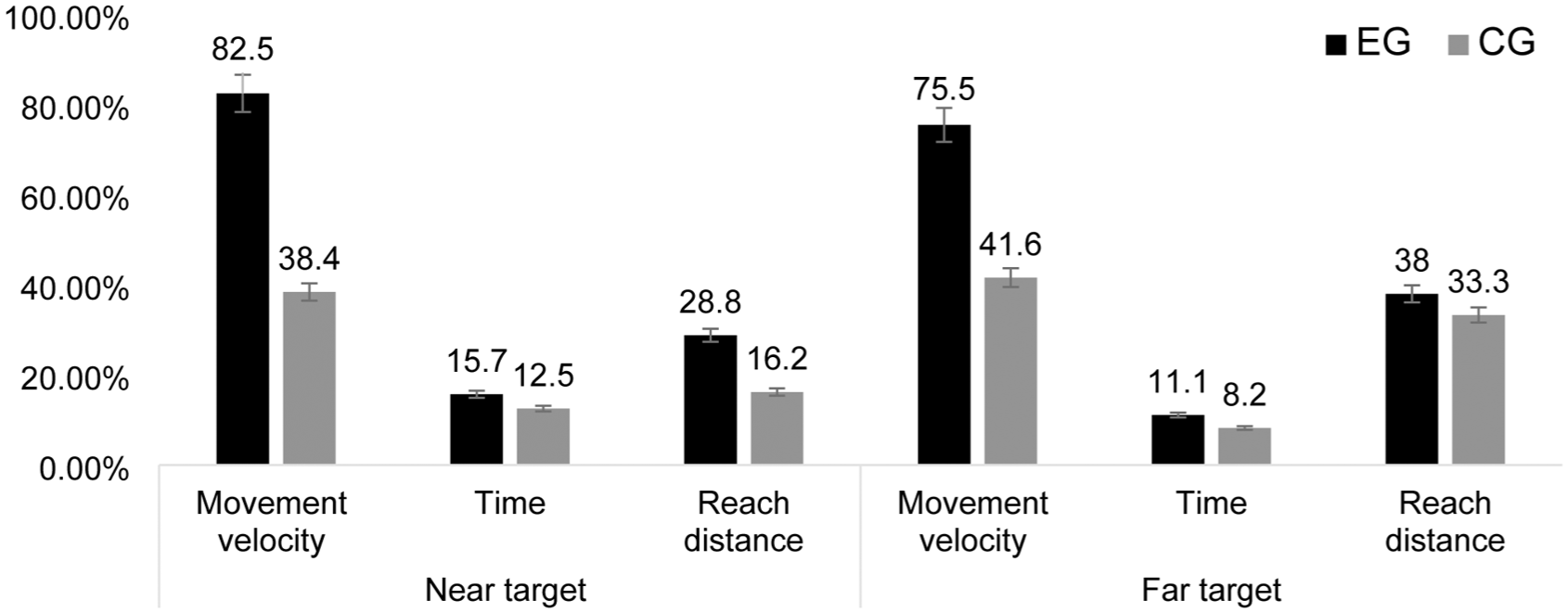
Percentage change in movement capacity variables from baseline to post-intervention.
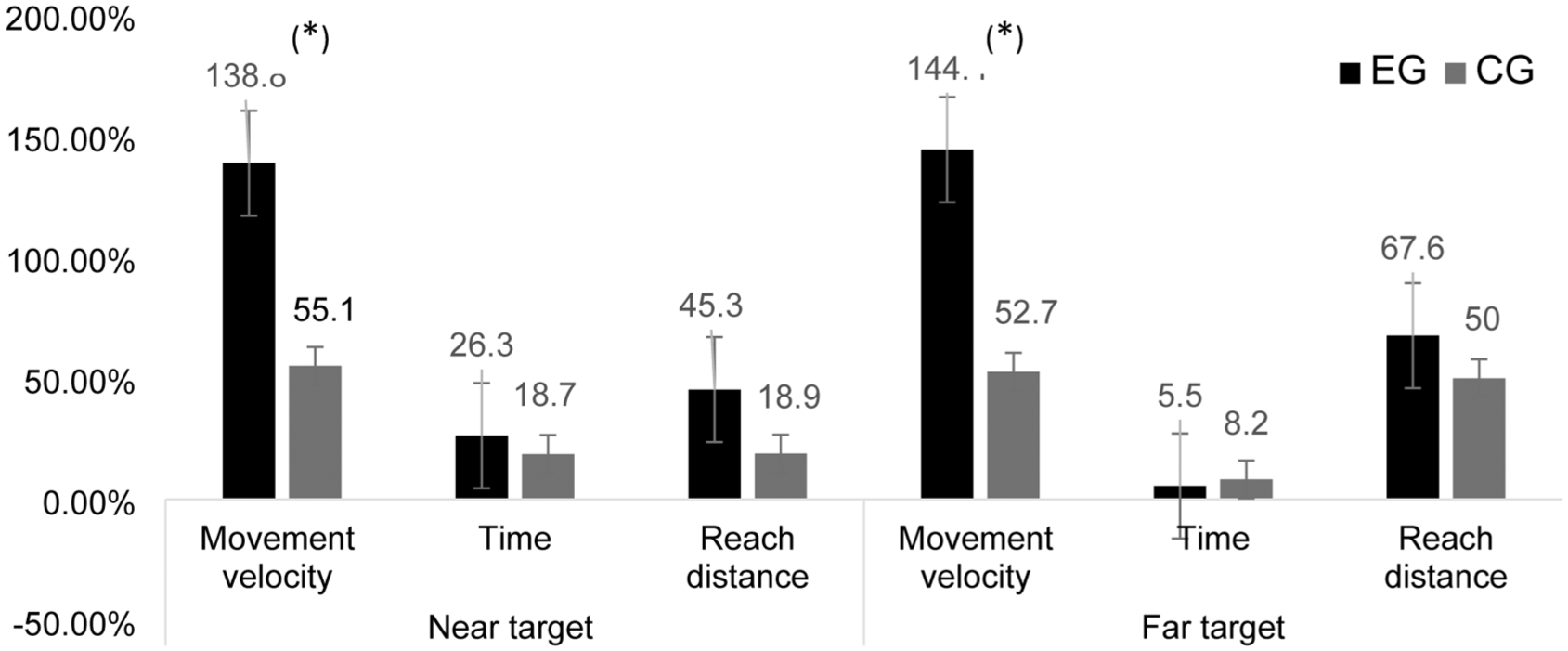
Percentage change in movement capacity variables from baseline to follow-up periods.
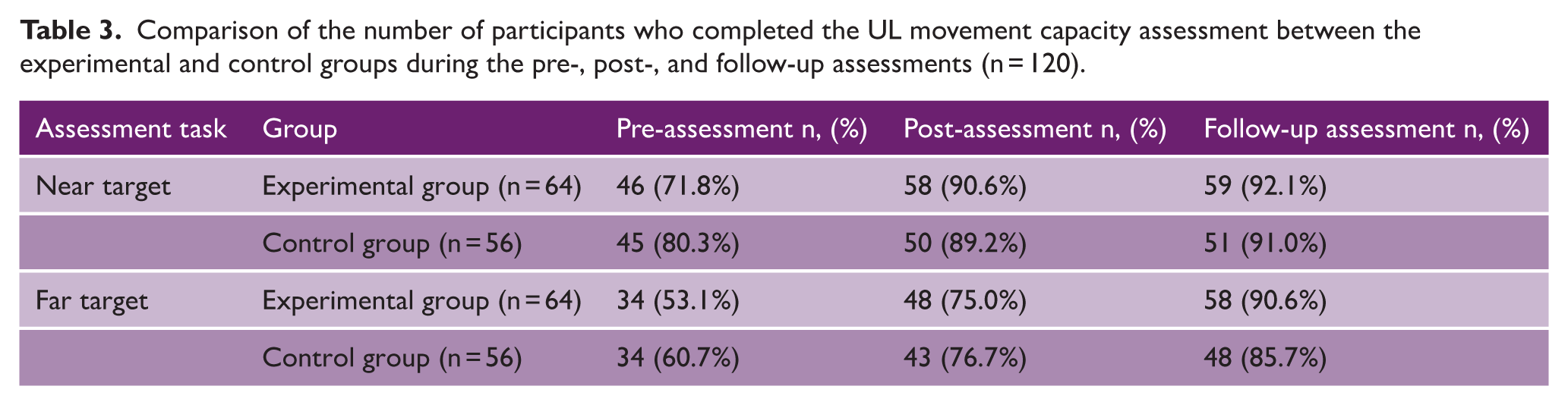
The study also investigated how many participants who were unable to perform the pre-intervention movement capacity analyses were then able to perform post-intervention and follow-up assessments. Table 3 shows that the number of participants who could not perform pre-intervention movement capacity analyses increased after the intervention, and more participants were thus able to perform post and follow-up assessments in both the experimental and control groups.
Comparison of the number of participants who completed the UL movement capacity assessment between the experimental and control groups during the pre-, post-, and follow-up assessments (n = 120).
Discussion
This study presents the second report of the results of a multicenter, single-blind randomized controlled trial (RCT) that focuses on the kinematic actual movement capacity of UL as assessed with the ArmAbletm gaming device. These findings demonstrate that low-cost, sensor-integrated gaming platform (ArmAbletm device) can serve as an assessment tool to quantify UL movement kinematics post-stroke. It further shows that game-based rehabilitation using the ArmAbletm device has the potential to enhance UL movement capacity, as reflected by improvements in movement velocity, reach distance (for both near and far targets), and movement time. Among these, only the improvement in movement velocity reached statistical significance at the 6-week follow-up. The other movement capacity parameters, such as reach distance and movement time, showed positive trends but did not achieve statistical significance.
The observed improvement in movement velocity may be attributed to the presence of defined targets during the training, which necessitated precise muscle control to reach specific positions. Our findings are in line with previous studies, which demonstrated that goal-directed reaching toward specified targets significantly reduced movement time (~22%) and the number of velocity peaks (~23%), indicating smoother and more efficient UL movements in individuals with chronic stroke. 24 In addition, robot-assisted reaching interventions have been associated with increased mean and peak velocities, reinforcing the notion that structured, target-oriented movements enhance movement performance. 25
The improvements observed in the game-based rehabilitation group may also be due to the repetitive, task-specific nature of the exercises combined with the interactive and engaging nature of the games along with real-time data-driven feedback within a closed-loop motor learning framework. Such approaches are known to enhance patient motivation and adherence to rehabilitation protocols. The ArmAbletm platform incorporates functional games that simulate activities of daily living and are specifically designed to promote UL recovery. This design likely facilitated greater active participation, increased repetition, and reduced training fatigue or disengagement.
The repeated, target-based reaching practice allowed participants to complete many repetitions without realizing they were in rehabilitation. This implicit, intensive practice likely helped them develop smoother and more efficient movement. The ArmAbletm device enabled bilateral arm training, which was especially useful early in stroke recovery when the affected arm could not move voluntarily. Engaging both limbs simultaneously probably increased practice with the affected limb, aiding motor relearning through bilateral activation and interlimb transfer. Repeated practice of reaching tasks post-stroke has been shown to enhance movement capacity, as evidenced by reductions in movement time, improvements in reach distance, and increases in movement velocity. These gains, also seen in VR-based rehabilitation studies, are mainly due to better motor control and less reliance on compensatory movements from repetitive, goal-directed training.26–28
Notably, in this study, a greater number of participants who were initially unable to initiate or complete the reaching task (for both near and far targets) with their affected UL were able to successfully perform these tasks during post-intervention and follow-up assessments. This observation supports previous literature indicating that intensive, task-oriented, and repetitive training can facilitate the restoration of functional reaching ability in individuals with stroke by promoting cortical reorganization and reducing motor deficits. Moreover, such training has been shown to improve movement initiation, trajectory control, and task completion even among individuals with severe UL impairments.29–31 These results are consistent with earlier research showing that training in a virtual environment helps to promote learning in healthy controls and is relevant in stroke survivors. 32 This is reinforced by the provision of augmented feedback from the device and therapist related to the individual’s movement performance. 33
The difficulty level of each game was set on the basis of the results of the movement capacity assessment, which was completed before the intervention commenced and can be adjusted to fit each individual’s motor skills to ensure an appropriate level of challenge. This approach ensures that each patient’s program is personalized for their needs. In addition, because it was a supervised therapy program, participants received real-time feedback from the device and the therapist on their performance and outcomes (knowledge of both performance and results).
Most of the games encouraged the UL to reach a closed kinetic chain pattern that prevented abnormal synergistic patterns and stimulated shoulder protraction, shoulder flexion without the abduction component, and elbow and wrist extension, which aided in breaking the flexor synergy of the UL that is predominant following a stroke. Even though the device cannot provide objective data on movement smoothness and trajectory, we believe that there was reduced arm and trunk compensation and an increase in elbow extension movement, as described by a recent study that reported a similar methodology and used an arm support device combined with the Wii interface compared to conventional therapy in chronic stroke survivors. 32 As the participant moves the arm in a closed kinetic chain while holding the gaming console, this helps preserve energy and prevents fatigue, which would otherwise have further extended the task duration.
Given the heightened window of recovery during the acute and subacute phases, game-based therapy provided in this period may have contributed to improvements in UL function, consistent with evidence on neuroplasticity-induced motor recovery. 34 As brain plasticity is particularly pronounced during the acute/subacute post-stroke period, 35 early, appropriately dosed training may facilitate recovery. 36 However, the short study duration and the natural course of spontaneous recovery in the early post-stroke period may have independently contributed to the observed improvements, potentially confounding the intervention effects and leading to an overestimation of treatment efficacy.
Even though we found immediate and short-term improvements in UL function when assessed with clinical scales (FMA-UE and ARAT) in the EnteRtain trial, 21 a significant effect on movement capacity parameters was not observed. While clinical scales such as FMA-UE and ARAT are widely recommended for evaluating UL function, 13 they primarily capture task accomplishment and lack sensitivity to detect subtle or gradual changes in complex motor performance and do not capture movement quality or underlying biomechanical deficits.10,37,38 Therefore, the use of kinematic assessment can be considered a strength of this study, as it allows for a more sensitive evaluation of movement capacity and provides additional insight into motor recovery beyond conventional clinical measures. The lack of statistical significance in terms of movement time and reach distance could be attributed to the intervention’s brief duration of 2 weeks. As a result, this study should be replicated with long-term intervention and follow-up. In addition, even though the mode of delivery was different, the content and dosage of therapy in both groups were similar. This could also lead to a lack of significant differences between the groups.
Limitations
Our study has several limitations. First, given the contemporary reality of brief hospital stays due to planned early discharge, our intervention period could be considered short.14,39 Second, the evaluation game had a one-directional reach and may not have been able to measure the sophisticated multidirectional task gains. Hence, it is suggested that assessment games with multidirectional reach components should be developed to examine the complicated nature of UL movements. The assessment game could not provide information on the available range of movement at the joint level, smoothness, or trajectory of the task performed. Moreover, as we collected only objective data, we were unable to gather subjective experiences and qualitative feedback from the participants regarding the assessment game and movement capacity evaluation. Such data could have provided valuable insights into the reasons for the non-significant findings in movement time and distance variables.
Conclusion
Compared with task-based training, game-based rehabilitation using the ArmAbletm device was found to increase UL movement capacity in individuals with acute/subacute stroke, as assessed with a new evaluation game. Following game-based rehabilitation, movement capacity assessment can be used as a routine outcome measure to assess the functionality of the affected UL in people with stroke. In addition, a movement capacity assessment should be conducted before the intervention begins to select games that are appropriate for the participants’ motor abilities.
Supplemental Material
sj-docx-1-wso-10.1177_17474930261448299 – Supplemental material for Game-based rehabilitation improves upper limb movement capacity compared to task-based training in people post-stroke: Kinematic analyses from the EnteRtain randomized clinical trial
Supplemental material, sj-docx-1-wso-10.1177_17474930261448299 for Game-based rehabilitation improves upper limb movement capacity compared to task-based training in people post-stroke: Kinematic analyses from the EnteRtain randomized clinical trial by A Sulfikar Ali, Ashokan Arumugam, Charlotte K Häger, Girish N, Punitha Nirmal, Manikandan Natarajan, John M Solomon, Vasudeva Guddattu, Aparna R Pai and Senthil Kumaran D in International Journal of Stroke
Footnotes
Acknowledgements
The authors would like to thank all the participants in our study and acknowledge Mr Habib Ali and Mr Sreehari K G for their technical assistance. In addition, they would like to acknowledge Mrs Sanjukta Sardesai and Mrs Amritha Unni for their assistance in data collection and reviewing the article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study is partially funded by an industry grant provided through the BeAble Health Pvt Ltd. (IIT Hyderabad, Telangana, India) and the Society of Indian Physiotherapists in the Young Researcher category [Ref No: SIP_2021_YR01].
Ethical approval
This study was approved by the Ethics Committee of Kasturba Medical College and Kasturba Hospital, Manipal (IEC: 328/2020). All participants provided written informed consent prior to enrolment in the study.
Consent to participate
All participants provided written informed consent prior to enrolment in the study.
Consent to participate
All participants voulntarily consented to participate in the study.
Consent for publication
Not applicable
ORCID iDs
Data availability statement
The data that support the findings of this study are available from the corresponding author upon reasonable request.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.