
Abstract
Introduction
The purpose was to explore if there are differences in extent of change in upper extremity motor function and activity capacity, in persons with ischaemic versus haemorrhagic stroke, during the first year post stroke.
Patients and methods
One hundred seventeen persons with stroke (ischaemic n = 98, haemorrhagic n = 19) and reduced upper extremity function 3 days after onset were consecutively included to the Stroke Arm Longitudinal Study at the University of Gothenburg (SALGOT) from a stroke unit. Upper extremity motor function (Fugl-Meyer Assessment Scale for Upper Extremity (FMA-UE)) and activity capacity (Action Research Arm Test (ARAT)) were assessed at 6 assessments during the first year; age and initial stroke severity were recorded. Differences between groups in extent of change over time of upper extremity motor function and activity capacity were analysed with mixed models repeated measurements method.
Results
Significant improvements were found in function and activity in both groups within the first month (p = 0.001). Higher age and more severe stroke had a negative impact on recovery in both groups. Larger improvements of function and activity were seen in haemorrhagic stroke compared to ischaemic, both from 3 days to 3- and 12 months, and from 1 month to 3 months. Both groups reached similar levels of function and activity at 3 months post stroke.
Conclusion
Although persons with haemorrhagic stroke had initially lower scores than those with ischaemic stroke, they had a larger improvement within the first 3 months, and thereafter both groups had similar function and activity.
Introduction
Stroke care as well as the characteristics of the person suffering from a stroke, has in high income countries changed over recent decades. Nowadays, a person with stroke is often independent prior to stroke 1 and has received better primary prevention such as hypertension treatment. 2 Furthermore, treatment with thrombolysis has become common, treatment at stroke unit is standard 3 and persons are often discharged to their own homes. 4 Fewer persons suffer an intracerebral haemorrhagic stroke compared to ischaemic stroke, 1 and even if the acute mortality rate after haemorrhage is higher, approximately the same long-term mortality for both stroke types has been presented. 5
Reduced upper extremity function after stroke is common,6,7 and despite type of stroke, recovery of motor function appears to occur predominantly within the first 3 months.7,8 However, persons with haemorrhagic stroke often have more severe deficits initially compared to those with ischaemic stroke.9–11 With regards to upper extremity recovery, a trend towards better functional outcome after haemorrhagic compared to ischaemic stroke has been described,11–13 but findings are conflicting.9,10 These inconclusive findings, in addition to the changes in the general stroke population and the stroke care development, highlight the need for further investigation of possible differences in recovery of upper extremity motor function and activity in different stroke subgroups. 14 Increased knowledge regarding recovery patterns is needed to support decision making and early rehabilitation planning when the hospital stays are shortened. Therefore, the purpose was to explore if there are differences in extent of change in upper extremity motor function and activity capacity, in persons with ischaemic versus haemorrhagic stroke during the first year post stroke.
Patients and methods
The study was a part of the prospective longitudinal cohort study, the Stroke Arm Longitudinal Study at the University of Gothenburg (SALGOT study).
15
Over 18 months in 2009–2010, all persons with stroke, treated at the largest of three stroke units at the Sahlgrenska University Hospital in Gothenburg, Sweden were screened. Persons were consecutively included with the following inclusion criteria: (1) first ever stroke (ischaemic or intracerebral haemorrhagic) confirmed with imaging; (2) reduced upper extremity activity at 3 days (±1 day) after onset, defined as <57 points on the Action Research Arm Test (ARAT);16,17 (3) at the stroke unit within 3 days; (4) residency in the Gothenburg urban area; and (5) ≥ 18 years of age. Exclusion criteria: (1) an upper extremity injury/condition prior to the stroke; (2) severe multi-impairment or diminished physical condition prior to the stroke and/or a life expectancy <12 months post stroke; and (3) non-Swedish speaking. In total, 763 persons were admitted to the stroke unit, whereof 158 met the inclusion criteria (Figure 1). Of these, 36 persons declined participation and 5 did not participate due to practical reasons. The SALGOT study resulted in 117 persons, details have been published previously.
18
No differences were seen between included and non-included persons in stroke severity as assessed with National Institute of Health Stroke Scale (NIHSS)
19
or in sex. However, the non-included persons were older on average; 76 years compared to 69 years (p = 0.027).
18
Data from all included 117 persons were used in the present study.
Patient selection process.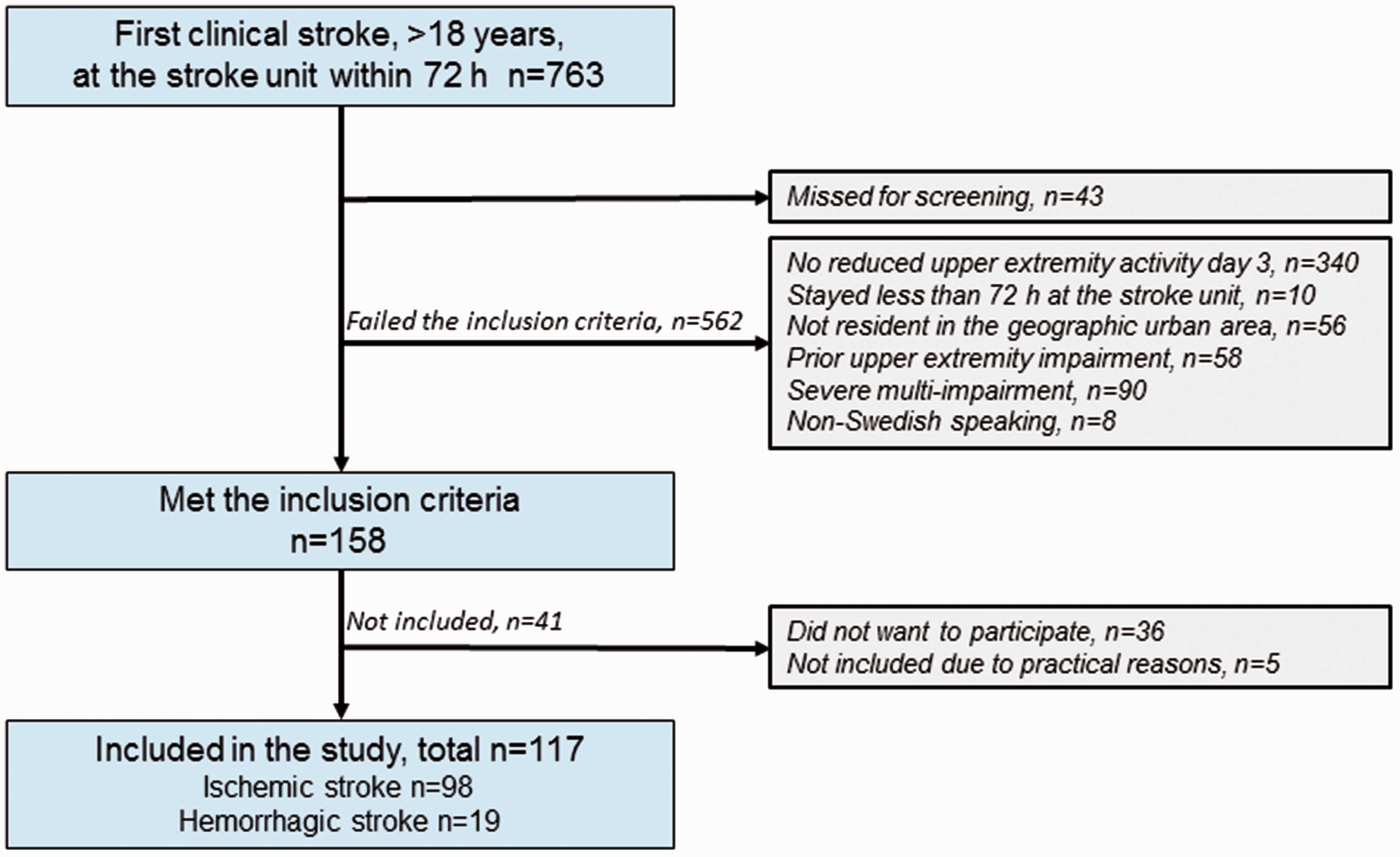
Fugl-Meyer Assessment Scale for Upper Extremity (FMA-UE)20,21 was used to assess motor function and ARAT16,17,22 assesses activity capacity. The FMA-UE consists of 33 items, scored on a 3-point ordinal scale (0–66) and the ARAT consist of 19 items, scored on a 4-point ordinal scale (0–57). Higher score in FMA-UE and ARAT indicates better function or activity. The initial stroke severity was assessed using the NIHSS (0–42) at admittance to the hospital. Background data were collected from medical charts and from the Swedish National Stroke Register.
Assessments were performed at 3 and 10 days and at 1, 3, 6 and 12 months after stroke onset. Three research physiotherapists, not otherwise involved in the care, conducted the assessments following a standardised protocol. 15 The majority of the assessments were performed at the hospital, and if the person was unable to travel the assessment was performed in the person's home, nursing home or at the rehabilitation unit. All persons received individually adjusted, functional task-specific rehabilitation (physiotherapy and/or occupational therapy) from the first day at the stroke unit according to standard routine. In-patient rehabilitation (at stroke or rehabilitation unit) was defined as rehabilitation ≥ 3 times/week, and outpatient rehabilitation (home or at community care units) as rehabilitation ≥ 1 times/week. The study was approved by the Regional Ethical Review Board in Gothenburg and all persons or their next of kin provided written informed consent. The STROBE guideline for observational studies 23 was followed in this report.
Statistics
The persons were divided into two groups; ischaemic (n = 98) or haemorrhagic (n = 19) stroke. Differences between the groups at baseline were investigated with Mann–Whitney U-test, with Fisher’s exact test and an independent sample t-test. A p-value of < 0.05 was considered statistically significant. Statistical analyses were conducted using IBM SPSS 21.0 statistics (IBM, Armonk, NY).
In order to investigate the extent of change in motor function and activity capacity as well as to explore differences between stroke types, the mixed models repeated measures was used (Statistical Analysis Program, SAS proc mix, version 9.3). Two separate models were explored, one for upper extremity motor function (FMA-UE) and one for activity capacity (ARAT). In each model, stroke type (ischaemic or haemorrhagic), age at onset and the initial stroke severity (NIHSS) were used as independent variables, an interaction between the stroke type and the time since stroke onset was also included. The group size with haemorrhagic stroke (n = 19), limited the number of variables to be included in the mixed models of repeated measures, and the age at onset and stroke severity, considered as most important for the recovery process24,25 were therefore used. Visual inspection of residual plots of all observations (ARAT n = 585, FMA-UE n = 580), revealed small negative deviations from normality and a ceiling effect in both scales. The unstructured covariance matrix was used according to the lowest Akaike’s information criterion (AIC). Significant factors impact on over time were further explored, generated from the models. Differences in extent of change in motor function and activity capacity between stroke types were calculated at four time periods: from 3 days to 1, 3 and 12 months respectively, as well as from 1 to 3 months post stroke. Significant factors (from the mixed models repeated measures) were controlled for when calculating differences in changes in FMA-UE or ARAT scores, including two-sided 95% confidence intervals (CI). The time periods were selected based on studies of recovery.7,26 At day 10, FMA-UE scores from 20 persons were missing due to administrative causes, however these values were estimated and included in the analysis, as previously described. 27
Results
Demographic characteristics of included persons.
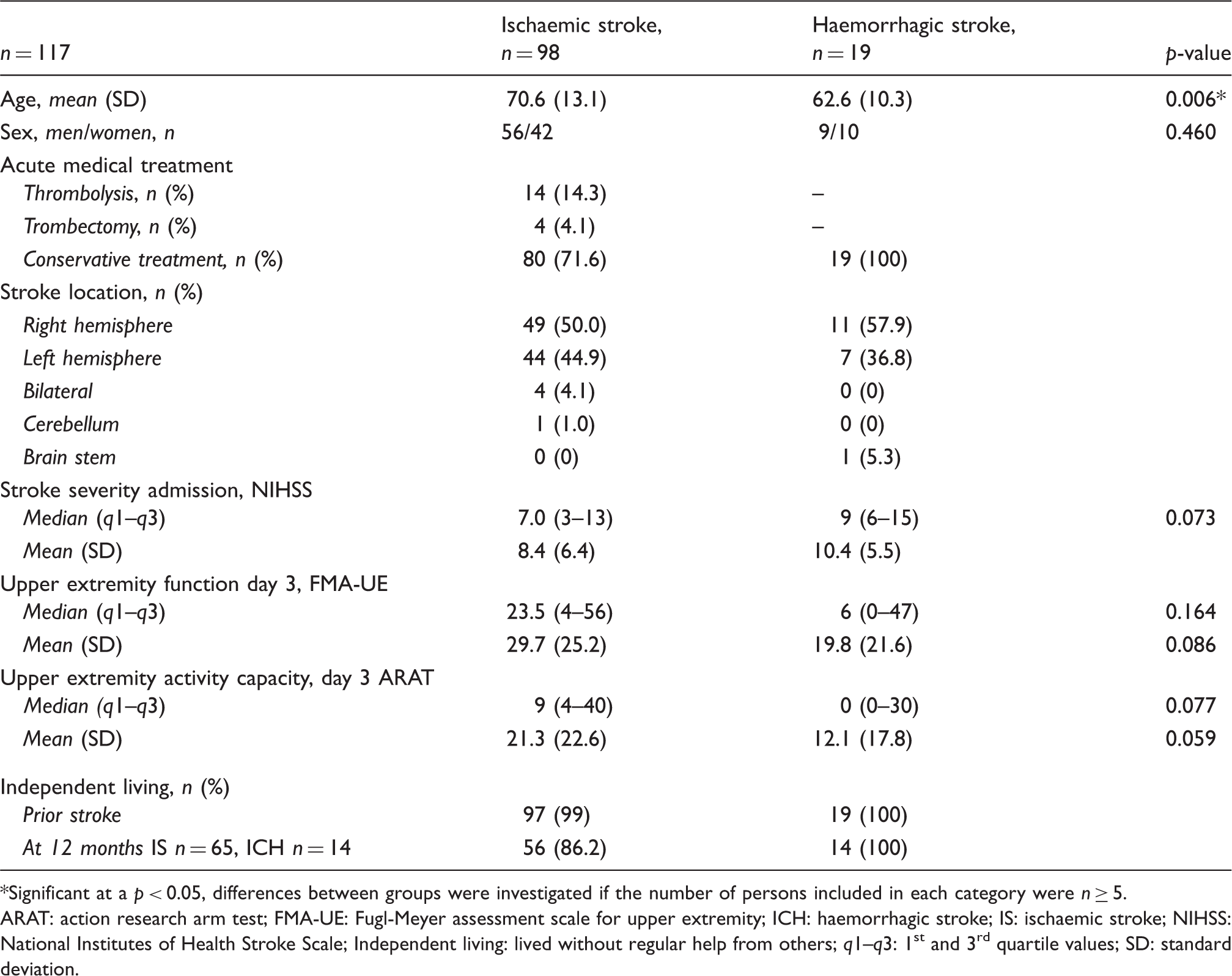
Significant at a p < 0.05, differences between groups were investigated if the number of persons included in each category were n ≥ 5.
ARAT: action research arm test; FMA-UE: Fugl-Meyer assessment scale for upper extremity; ICH: haemorrhagic stroke; IS: ischaemic stroke; NIHSS: National Institutes of Health Stroke Scale; Independent living: lived without regular help from others; q1–q3: 1st and 3rd quartile values; SD: standard deviation.
No significant differences were seen between stroke types in number of persons receiving inpatient rehabilitation at 3 days, 10 days and 1-month post stroke (Supplemental Table II). Seventy-nine percent (n = 15) with haemorrhagic stroke were referred to an inpatient rehabilitation unit, compared to 47% (n = 46) with ischaemic stroke (p = 0.012, Table 1). A larger proportion of persons with haemorrhagic stroke received outpatient rehabilitation at 3, 6 and 12 months post stroke, but there were no significant differences between stroke types (Supplemental Table II).
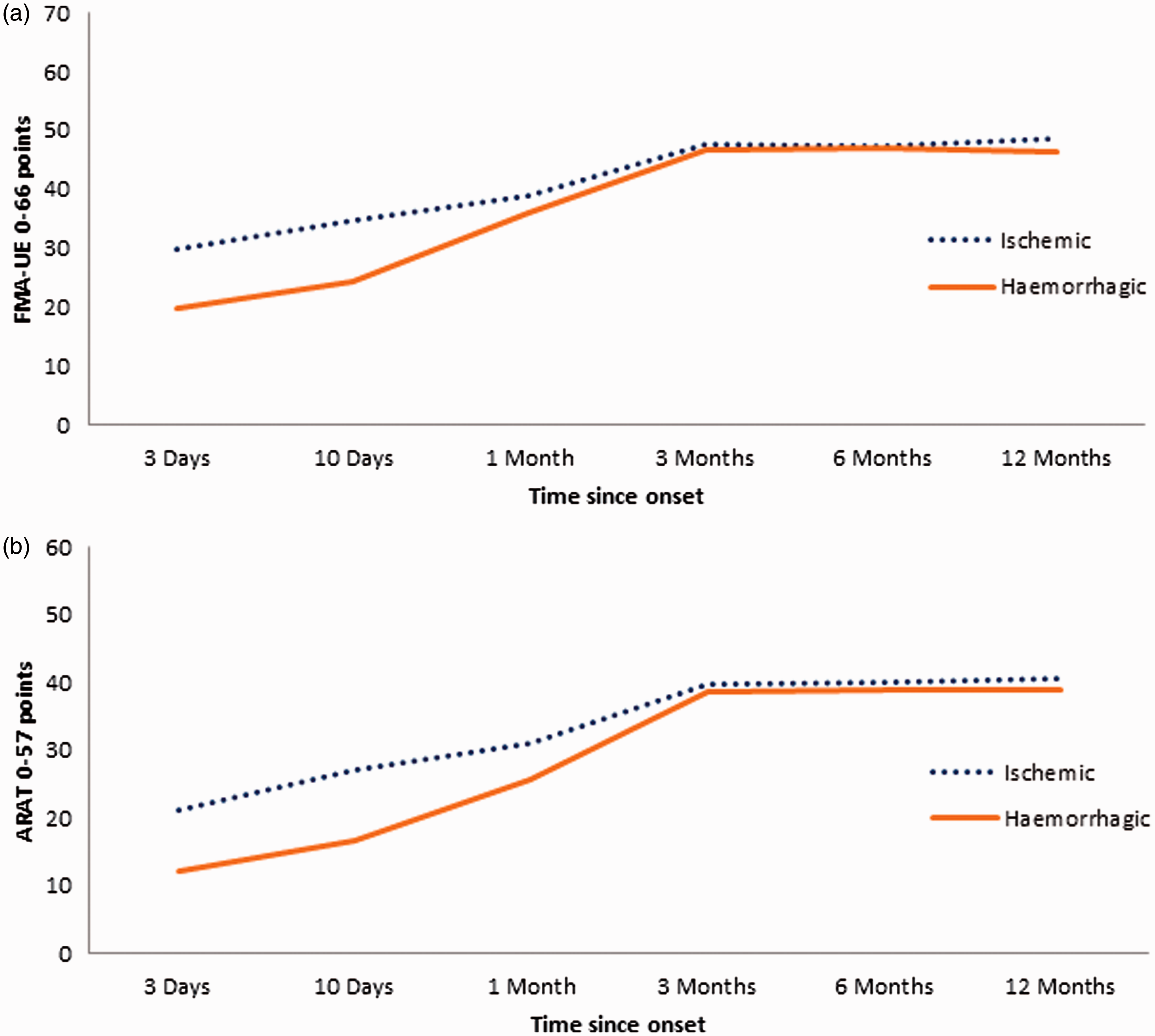
Upper extremity motor function and activity capacity followed a similar pattern during the first year with widest variations seen early post stroke, including a wide dispersion in extent of change that could be seen at all assessments (Figure 2(a) and (b)). The mean scores of motor function and activity capacity were higher in the group with ischaemic compared to haemorrhagic stroke at all time points from 3 days to 3 months (Figure 3(a) and (b)).
Individual patterns in extent of change in upper extremity motor function and activity capacity during the first year post stroke. The recovery pattern of upper extremity motor function and activity capacity during the first year post stroke.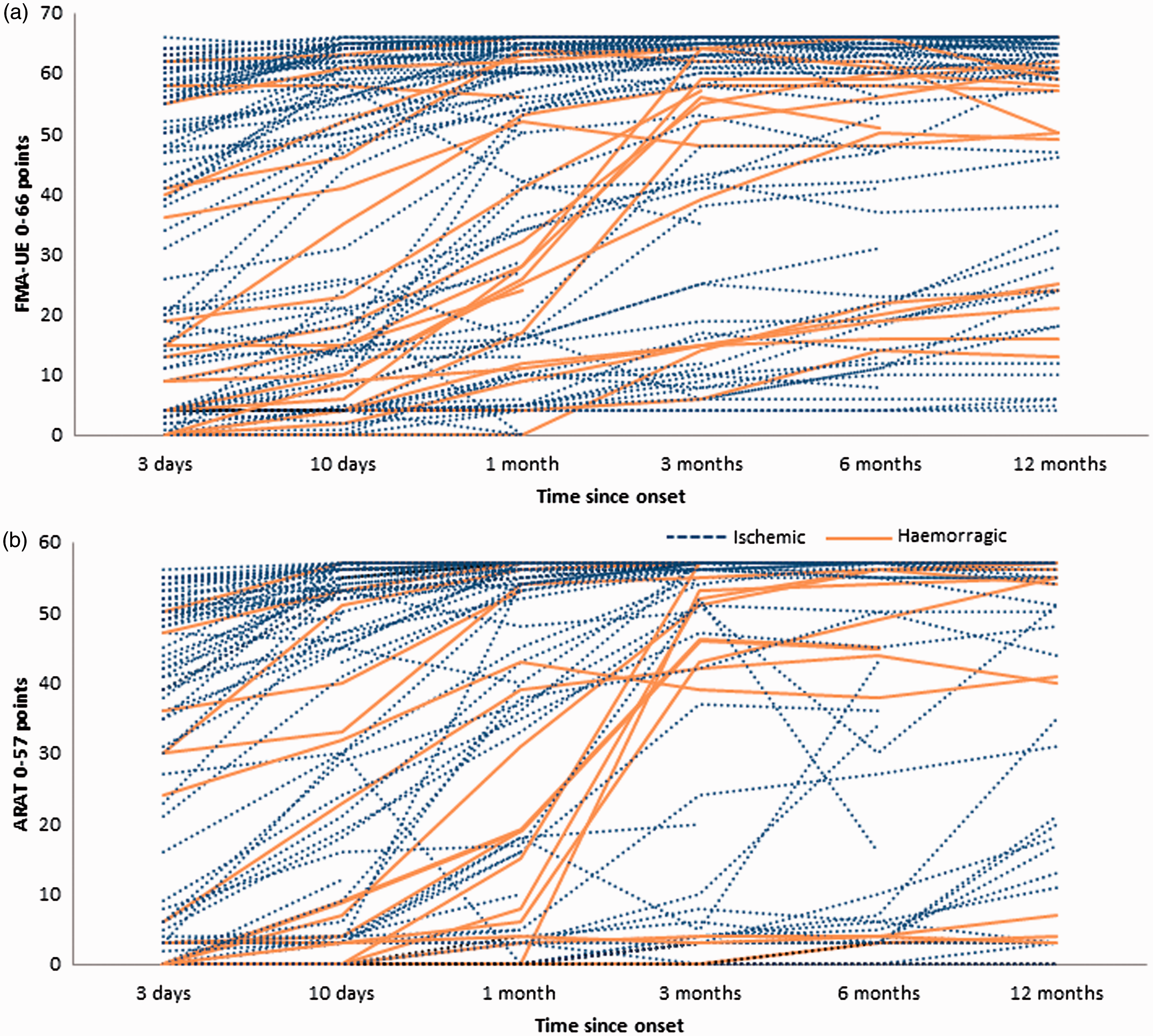
Extent of change in function and activity in persons with ischaemic and haemorrhagic stroke within the first year after stroke onset. Estimates of fixed effects
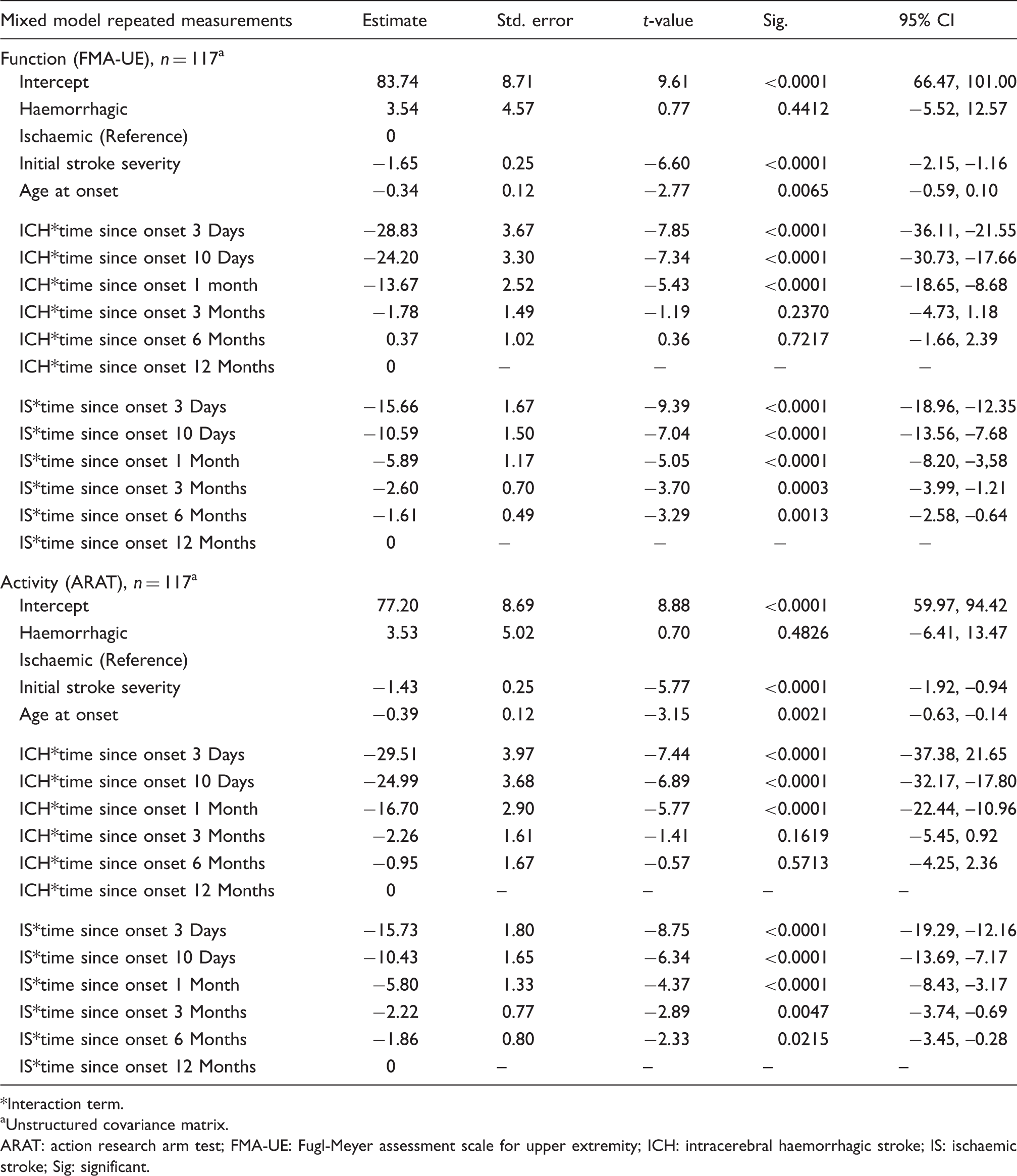
Interaction term.
Unstructured covariance matrix.
ARAT: action research arm test; FMA-UE: Fugl-Meyer assessment scale for upper extremity; ICH: intracerebral haemorrhagic stroke; IS: ischaemic stroke; Sig: significant.
Differences between ischaemic and haemorrhagic stroke in extent of change over time in FMA-UE (function) and ARAT (activity), adjusted for stroke severity and age.
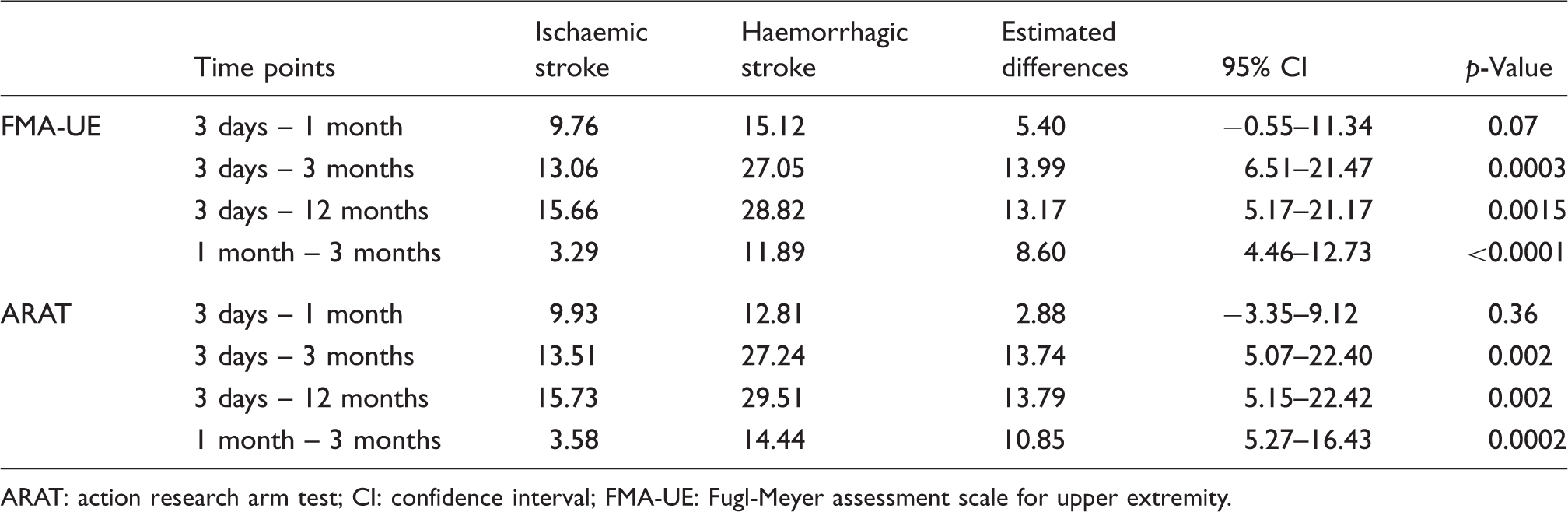
ARAT: action research arm test; CI: confidence interval; FMA-UE: Fugl-Meyer assessment scale for upper extremity.
Discussion
The main finding from this study was that the extent of change in motor function and activity capacity during the first year after stroke differed between persons with ischaemic and haemorrhagic stroke. Findings from the current study can be summarised as follows: (1) persons with haemorrhagic stroke started from a lower level and gained more motor function and activity capacity during the first year, when controlling for age and stroke severity; (2) the largest difference between stroke types in the extent of recovery progress in function and activity capacity was seen from 1 to 3 months; (3) both stroke types reached approximately same level of function and activity capacity after 3 months. These results have important clinical implications as hospital and inpatient rehabilitation stays are getting shorter, which in turn requires rehabilitation planning and appropriate goal setting early after stroke onset.
After controlling for age and stroke severity, persons with haemorrhagic stroke started from a somewhat lower motor function and activity capacity level, but demonstrated larger improvements compared to persons with ischaemic stroke within the first year. Major differences in change scores between the two groups were seen from the first to third month, where persons with haemorrhagic stroke gained a mean score, which can be considered as clinically important28,29 but after 3 months both stroke types reached approximately the same level. The initial more severe stroke and higher age were associated with reduced function and activity at 1 year post stroke in both groups. A rapid recovery of neurological signs and symptoms has previously been shown in persons with haemorrhagic stroke and a more gradual pattern of recovery is expected in persons with ischaemic stroke. 13 Differences in pathophysiological processes in the acute and sub-acute phases could be one explanation13,26 as well as the time since onset affects the spontaneous neurological recovery. 26 Comparisons of recovery between stroke types can be challenging, mainly because in general persons with haemorrhage suffer a more severe stroke11–13 and are younger. Persons with haemorrhagic stroke who survive the acute phase have a better prognosis and outcome, compared to ischaemic stroke, if the initial severity is similar.9,12 In the rehabilitation phase, persons with haemorrhagic stroke has shown larger improvements,12,13,30 or there were no differences between stroke types. 10 These diverging results could emerge due to several factors such as initial assessment time, type of rehabilitation, inclusion criteria or time points for follow-up, and a strength of the present study is that it uses longitudinal data with several fixed repeated assessments in an unselected sample of patients with first ever stroke.
In this study, the large inter-individual variations also seen in large confidence intervals indicate high variability in recovery patterns in both groups, and highlight the importance of rehabilitation planning to be individualised in the early phase after stroke.
The organisation of stroke care in the present study may have an impact on recovery.4,31 The data were collected at a stroke unit in a high income country with tax funded care, where rehabilitation starts the first day after stroke onset. These are the factors that need to be taken into account when generalising the findings. In the present study, a higher percentage of persons with haemorrhagic stroke were referred from the stroke unit to in-patient rehabilitation, and even if there was a trend towards a higher percentage of persons with haemorrhagic stroke receiving out-patient rehabilitation at different time points, no statistically significant differences between groups were seen. The present study comprised persons who received care at a stroke unit within 3 days after stroke onset, which excluded persons in intensive or neurosurgical care and those who died prior to 3 days, which might be more frequent after haemorrhagic stroke.
This study is not without limitations and some issues need to be discussed further. In the statistical analysis, a parametric method, mixed model repeated measures, was chosen in order to handle missing data, longitudinal change, differences between groups and interaction between variables. Psychometric properties of the FMA-UE 32 and the ARAT 33 may allow the use of parametric calculations; however, the use of sum scores in ordinal scales can be questioned and further psychometric studies are needed. 32 The present study included few persons with haemorrhagic stroke, which restricted the number of variables that could be included in the models. The two most important variables24,25 for recovery were selected; other possible variables such as location and size of the stroke, comorbidity factors, level of cognition and amount of rehabilitation received or initial medical treatment were not included. Several persons started in the upper 1/3 of the assessments scales and achieved maximum score early in the follow-up period and the ceiling effect may have influenced the results of FMA-UE and ARAT. Furthermore, the ARAT only captures a part of upper extremity activity and does not measure activity in daily life or social participation. Improved understanding of individual changes over time in motor function and activity capacity, could be gained by combining various methods such as motor functional scores and neuro imaging. 34
The present study describes the extent of recovery progress in both motor function and activity capacity of upper extremity after different types of stroke. The recovery after ischaemic stroke has previously been more extensively investigated than after haemorrhagic stroke. Thus, further research with larger sample sizes of persons recovering from haemorrhagic stroke 14 and adjusted for confounding factors could improve the knowledge.
Conclusions
This study found time-dependent differences in recovery patterns between stroke types with haemorrhagic stroke recovered more rapidly from an initial lower level of motor function and activity capacity, compared to persons with ischaemic stroke. Major differences in motor function and activity capacity were present from 1 to 3 months, where persons with haemorrhagic stroke had larger improvements, and similar motor function and activity capacity were present in both types of stroke at 3 months.
Footnotes
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Dr Persson, Dr Opheim, Dr Lundgren-Nilsson, Dr Alt Murphy and Dr Danielsson report no disclosures. Dr Sunnerhagen works for the National Board of Health and Welfare regarding guidelines for Stroke.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded in parts by the Swedish Research Council (VR 2012-70X-22122-01-3), the Swedish Heart-Lung Foundation, the Norrbacka Eugenia Foundation, the Foundation of the Swedish National Stroke Association, the Local Research and Development Board for Gothenburg and Södra Bohuslän, Greta and Einar Asker’s Foundation, the Swedish Brain Foundation, Stroke Centre West, Renée Eander’s Foundation and Hjalmar Svensson’s Research Foundation.
Ethical approval
The study was approved by the Regional Ethical Review Board in Gothenburg.
Informed consent
All persons or their next of kin provided written informed consent.
Guarantor
HCP.
Contributorship
HCP, AO, ÅLN, MAM, AD and KSS contributed to the design of the study concept, in analysis and interpretation of results and in drafting/revising the manuscript for content. All authors have read and approved the final manuscript. HCP and MAM performed the acquisition of data. HCP and KSS obtained funding.
Acknowledgements
Thanks to Eva-Lena Bustrén (data collection), Kjell Pettersson (statistical advice) and the Riks-Stroke Collaboration (help with demographic data).