
Abstract
Background:
Studies assessing the relationship between high ambient temperatures and stroke risk yielded conflicting results, while potential associations of humidity and heat stress with stroke risk remain underexplored.
Objective:
To explore the association of ambient temperature, humidity, and heat index (HI) with the risk of total stroke (combined ischemic-intracerebral hemorrhage [ICH]), ischemic stroke (IS), ICH, and transient ischemic attack (TIA) among older adults during the warm season in the Mediterranean region.
Methods:
In this time-stratified case-crossover study, we utilized data from the Israeli National Stroke Registry. We included all first stroke and TIA events among individuals aged ⩾18 years that occurred during the warm season (2014–2019). Temperature and relative humidity were assessed using high-resolution satellite-based models and monitoring stations, respectively, based on patients’ residential addresses. A heat index (HI) was calculated based on a combination of temperature and relative humidity data. Conditional logistic regression models with Distributed Lag Non-Linear Models (DLNMs) were used with adjustment for potential confounders, including air pollution. The HI models were stratified by participants’ demographic and health characteristics.
Results:
The sample included 22,269 individuals with a first stroke (mean age 72 ± 14 years; 55% males) and 8728 individuals with a first TIA (mean age 69 ± 14 years; 52% males) during the warm season. Higher temperature (32°C vs. 27°C), particularly on the stroke event date, was associated with increased risk of total stroke (odds ratio (OR) = 1.32; 95% confidence interval (CI) = 1.23–1.41). The strongest association for relative humidity (90% vs. 70%) was observed 2 days before the stroke event (OR = 1.09; 95% CI = 1.06–1.12). An HI of 100°F was associated with an approximately 40% higher risk of total stroke compared to HI of 80°F on the event day (OR = 1.39; 95% CI = 1.32–1.47). Associations were slightly weaker for ICH, possibly reflecting its relatively smaller sample size, whereas associations with TIA were similar in magnitude to those observed for IS. No evidence of effect modification was observed across subgroups defined by sociodemographic characteristics or comorbidities.
Significance:
High temperatures combined with high humidity are associated with an immediate increase in the risk of stroke and TIA, even in a region where the population is acclimatized and most buildings are air-conditioned. Preparedness and prevention strategies may be crucial for reducing stroke risk during periods of heat stress.
Keywords
Background
Climate change is a major determinant of human health in the 21st century, with profound implications for physiological functioning and disease risk. 1 In particular, climate change has been increasingly linked to a heightened risk of stroke. 2 Stroke ranks as the second leading cause of disability and mortality worldwide, and its incidence is projected to rise. 3 Most stroke cases are preventable, and numerous international and local organizations work to reduce the global stroke burden through public awareness campaigns, clinician education, and preventive initiatives. 3
In addition to well-established vascular risk factors contributing to stroke pathogenesis, evidence suggests that ambient temperature may also play a significant role. 4 Both extreme cold and heat have been associated with increased mortality from ischemic and hemorrhagic strokes. 5 These associations vary, with colder temperatures showing stronger links to stroke risk than higher temperatures.6–8 Some studies suggest that elevated temperatures are associated with increased risk of intracerebral hemorrhage (ICH), but not ischemic stroke (IS), 7 while others report an inverse relationship between high temperatures and IS incidence. 8 Notably, a recent meta-analysis found no significant association between high temperatures and stroke morbidity. 9
The inconsistent findings regarding temperature-related stroke risk may be partially explained by variations in relative humidity across climate subregions.9,10 While most previous studies have treated relative humidity as a potential confounding variable in their statistical models, 9 its independent role in stroke pathogenesis remains understudied. The few studies examining the association between relative humidity and stroke risk were constrained by small sample sizes and reported no significant relationships.11,12 However, recent evidence from a Chinese study suggests that higher relative humidity may be associated with reduced stroke risk. 13
Effective thermoregulation is influenced by heat index (HI), a composite measure that integrates dry-bulb temperature and relative humidity to reflect perceived ambient temperature and physiological heat burden under outdoor conditions. 14 Elevated HI correlates with increased mortality risk. 15 However, the relationship between HI and stroke incidence remains underexplored.
The current study aimed to explore the relationship of ambient temperature, relative humidity, and HI with ischemic and hemorrhagic stroke risk among older adults during the warm season. It also explored transient ischemic attack (TIA) as a separate outcome. Furthermore, the association of heat stress with stroke incidence was tested in subsamples to identify vulnerable subpopulations. The study focuses on the Mediterranean region, a “climate change hotspot” characterized by increased heat discomfort and thermal stress due to high temperatures and air moisture in the warm season. 16
Methods
Study sample
Daily data on stroke cases admitted to Israeli medical centers during 2014–2019 were gathered from the Israeli National Stroke Registry (INSR), which includes all permanent residents of Israel (aged ⩾ 18 years) who were admitted to one of the 26 general hospitals in the country and received a diagnosis of stroke or TIA according to the International Classification of Disease, Ninth Revision, clinical modification (ICD-9-CM). All Israeli residents are insured by law and can attend any public medical center. Here, we included only individuals admitted during the Israeli warm season, to minimize potential confounding by cold temperatures, which are well-known risk factors for stroke. 8 Although the warm season is often defined as June to August, we also included September based on climatological evidence indicating that September in Israel is characterized by continued frequent high heat stress. 17
During 2014 to 2019, 111,397 stroke and TIA cases were registered with the INSR, including 110,915 cases with valid address information. After excluding 16,403 repeated stroke events, the sample included 94,512 first-occurrence stroke cases. We focused on 22,269 (23.6%) stroke and 8728 (9.2%) TIA cases that occurred during the warm season.
Stroke and TIA ascertainment
Stroke was defined as rapidly developed clinical signs of focal (or global) disturbance of cerebral function, lasting >24 h or leading to death, with no apparent cause other than of vascular origin. 18 Stroke types were based on ICD-9 coding and included patients with ICH (ICD-9-CM code: 431), IS (including occlusion of cerebral arteries (ICD-9-CM code: 434)), occlusion and stenosis of pre-cerebral arteries with infarction (ICD-9-CM code: 433.x1), acute, but ill-defined, cerebrovascular disease (ICD-9-CM code: 436), and iatrogenic cerebrovascular infarction or hemorrhage (ICD-9-CM code: 997.02). The latter two codes were excluded for sensitivity analysis; TIA (ICD-9-CM code: 435) was tested separately. Cases of subarachnoid or epidural hemorrhage, subdural hematoma, or other and unspecified ICH were not included in the INSR. In the absence of a recorded onset date, the stroke event date was defined as the hospital admission date.
Air temperature, relative humidity, and heat stress
Daily ambient temperature data (mean, minimum, and maximum) were obtained using a spatiotemporally resolved model that allows prediction of temperature parameters on a 1-km grid across Israel. 19 Detailed information on model construction, input data sources, and validation procedures is provided in Supplementary Material Section 1.
Because relative humidity data were not available from satellites, we obtained this parameter from approximately 100 formal meteorological stations operated by the Israel Meteorological Service (IMS). Relative humidity values were obtained from the station closest to the participants’ address. Israel is a small country (≈21,670 km 2 ) with three main humidity subclimates: the coastal plain, the mountain ridge, and the Jordan Rift Valley. Within each region, warm-season variation in mean daily relative humidity is generally <10%. 20 Moreover, meteorological stations are more densely distributed in populated areas, such as the coastal plain. Given the country’s small geographic scale, dense station network, and limited within-region variability, this approach should capture regional humidity patterns with minimal spatial misclassification.
The HI was calculated based on the heat stress index equation of the National Oceanic and Atmospheric Administration (NOAA) of the US Department of Commerce. 21 The continuous HI was used to assess its relationship with stroke risk. We categorized the index into risk strata as follows: HI <80°F indicated no heat stress, 80–90°F indicated caution, and >90°F indicated danger. In the case of missing relative humidity values at a specific location, we used data from the next nearest meteorological station.
Covariate ascertainment
Information on age at admission, sex, ethnicity (Jews vs. others), country of origin (Israel vs. others), current smoking, and death during the acute hospitalization was obtained from the INSR. Socioeconomic status was determined based on the registered residential address, using classifications from the Israel Central Bureau of Statistics. Comorbidities, including obesity, atrial fibrillation, history of hypertension, diabetes, hyperlipidemia, congestive heart failure, chronic kidney disease, ischemic heart disease, myocardial infarction, and peripheral vascular disease, were obtained from the INSR.
Air pollution was estimated based on novel hybrid satellite-based spatiotemporal models for predicting particulate matter < 2.5 μm (PM2.5) on a 1-km grid across Israel, based on participants’ residential address. 19 This model has been well validated using standard validation methods such as “tenfold” out-of-sample cross-validation techniques, and its performance is excellent and in line with US and European models. 22
Statistical analysis
We reported means ± SD and frequencies (%), for continuous and categorical variables, respectively. A case-crossover study design was used to explore the association of mean daily temperature, relative humidity, and HI with stroke risk. Controls were selected using a time-stratified strategy: exposure on the stroke event date was matched with exposure dates on the same day of the week within the same month and year, to control for time-trend factors such as seasonality.23,24 We performed a conditional logistic regression to obtain odds ratios (ORs) and 95% confidence intervals (CIs) of stroke risk associated with: (1) an increase of 1°C in mean ambient temperature; (2) 10% in relative humidity, and (3) 1 unit of HI. The case-crossover design automatically controls for within-individual characteristics such as age, sex and comorbidities through self-matching; hence, our models adjusted only for climatic-environmental factors: mean ambient temperature, relative humidity, and air pollution. The models addressing the association between HI and stroke risk were adjusted for air pollution only. Based on previous estimates of lag times, 25 focusing on the Mediterranean region during the warm season,26,27 we used an exposure window of 7 days from the stroke event date. Lag 0 corresponded to the index day (stroke event date), while lags 1–7 represented the one to seven calendar days preceding the event.
To explore possible nonlinear and lagged associations of temperature, relative humidity, and HI with stroke, we incorporated the distributed lag nonlinear model (DLNM) into the conditional logistic regression models. This DLNM creates a flexible cross-basis function for the parameters and their changes, allowing for nonlinear exposure-response relationships in each lag day and nonlinear lagged effects. Based on visualization and the Akaike information criterion (AIC), we utilized natural cubic splines with 3 degrees of freedom in the exposure-response curve within the cross-basis function. Effects across different lag days were defined to exhibit linear trends, allowing for flexible lag effects at short delays. Median ambient temperature and relative humidity and the upper bound of the “no warning” HI category were selected as references.
Analyses were conducted separately for total stroke (IS + ICH), IS, ICH, and, as a complementary analysis, for TIA. As a sensitivity analysis, we evaluated the associations between the climate measures and total and ISs after excluding acute but ill-defined cerebrovascular disease (ICD-9-CM code 436) and iatrogenic cerebrovascular infarction or hemorrhage (ICD-9-CM code 997.02).
The associations between HI categories and stroke risk were repeated while stratifying for several sociodemographic and health factors to test for possible effect modifications using a test for heterogeneity: age, sex, ethnicity, country of origin, socioeconomic status, death in acute hospitalization, current smoking, obesity, atrial fibrillation, hypertension, diabetes, hyperlipidemia, congestive heart failure, chronic kidney disease, ischemic heart disease, past myocardial infarction, and peripheral vascular disease.
To ensure that effect estimates were presented within a valid exposure range, we limited the reported temperature, humidity, and HI values to their upper extremes based on the observed distributions. For each exposure metric, the upper bound was defined using the 99th percentile of the corresponding distribution, rounding values upward to facilitate interpretability and graphical presentation. Specifically, the 99th percentile of 31.4°C for ambient temperature was rounded to 32°C; the 99th percentile of 84% for relative humidity was rounded to 90% to facilitate presentation of humidity in 10-percentage-point increments; and the 99th percentile of 96.7°F for HI was rounded up to 100°F.
Data were analyzed by SAS version 9.4 and R software (R package: dlnm, survival version 4.1.1). Statistical significance was defined as p < 0.05. The University of Haifa IRB and the Ministry of Health Helsinki Committee approved this study.
Results
Among the 22,269 first stroke cases during the warm season, 20,099 (90.3%) were ischemic and 2170 (9.7%) were hemorrhagic (Table 1). The mean age was 71.8 ± 13.6 years; 55% were men, and individuals with IS and ICH stroke types presented different characteristics. For example, individuals with IS were more likely to be middle-aged (50–74 years; 46.6% vs. 38.3%, p < 0.001) and less likely to have high socioeconomic status (15.5% compared to 18.2%; p = 0.002) than those with ICH. Furthermore, those with IS were less likely to die during acute hospitalization (7.1% vs. 29.1%) but had a higher frequency of vascular risk factors including smoking, obesity, and history of diabetes, hypertension, hyperlipidemia, heart disease, and peripheral vascular disease, than those with ICH (Table 1). Summary descriptive statistics for temperature, relative humidity, HI, and heat stress categories during the study period are provided in Supplementary Material Section 2.
Baseline characteristics of the study sample.
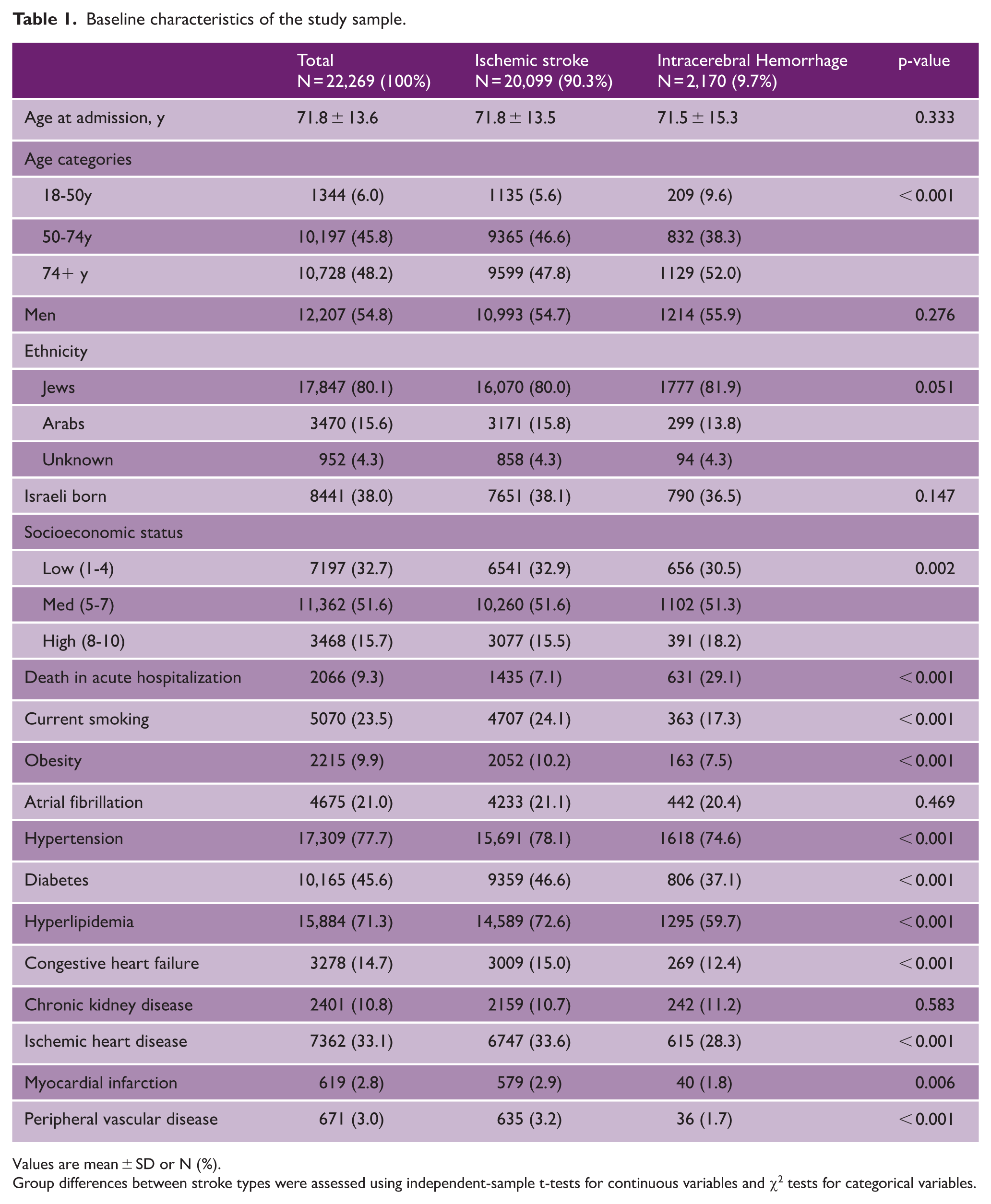
Values are mean ± SD or N (%).
Group differences between stroke types were assessed using independent-sample t-tests for continuous variables and χ2 tests for categorical variables.
Figure 1(a) and Supplementary Table 1 present the associations between mean ambient temperature and stroke risk (IS and ICH) during the warm season, with a 7-day lag, after adjustment for relative humidity and air pollution. Compared to the reference temperature of 27°C, stroke risk increased gradually on the stroke even date (lag 0) and 1–2 days prior (lag 1–2), with stronger associations when ambient temperatures exceeded 30°C and on lag 0. Specifically, the OR for stroke was 1.32 (95% CI = 1.23–1.41), 1.18 (95% CI = 1.12–1.24), and 1.07 (95% CI = 1.02–1.13) on lags 0, 1, and 2, respectively, comparing 32°C to the reference of 27°C. This risk was attenuated and no longer significant 3 days prior to the stroke event. Similar results were observed when IS and ICH were examined separately (Figure 1(b) and (c), Supplementary Table 1). Likewise, relative to the reference of 27°C, lower temperatures were gradually associated with a modestly reduced risk of both stroke types, particularly at lag 0.
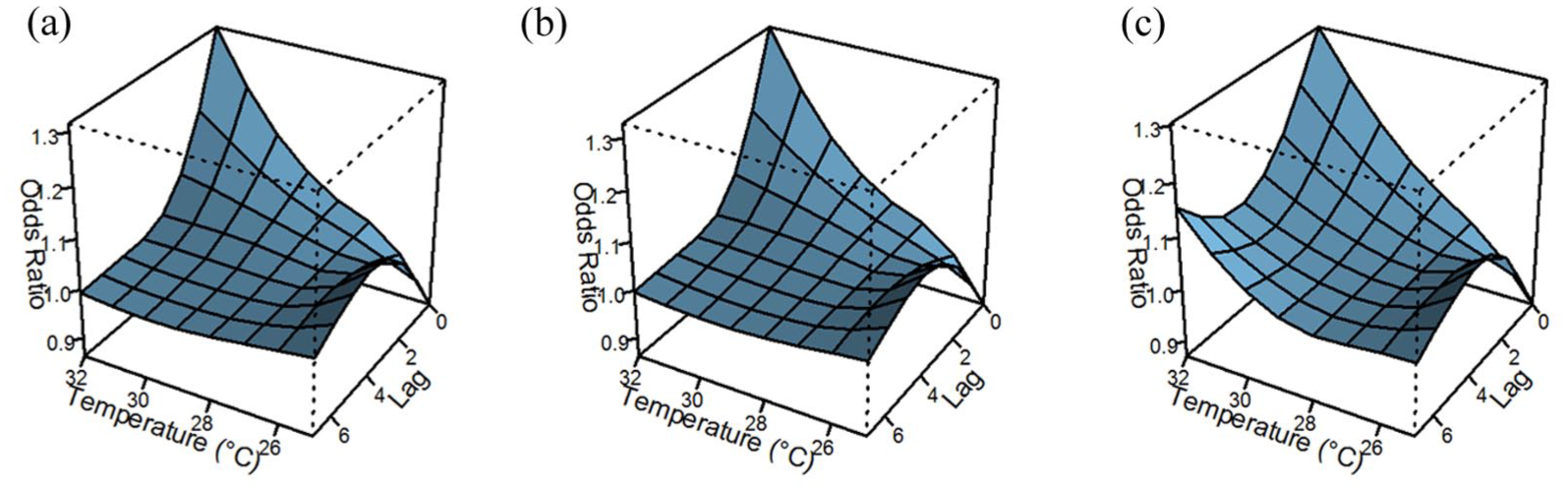
The association between mean ambient temperature (°C) and risk of total stroke (a), ischemic stroke (b), and intracerebral hemorrhage (c). Adjusted for relative humidity and air pollution; reference: temperature at 27°C.
The association between relative humidity and stroke risk after adjustment for ambient temperature and air pollution is depicted in Figure 2 and Supplementary Table 2. Compared to the reference of 70%, humidity was positively associated with stroke risk at lag 0, with 60% humidity having a 5% decreased risk (OR = 0.95; 95% CI = 0.94–0.96), and 80% having a 3% increased risk (OR = 1.03; 95% CI = 1.02–1.05). With increasing relative humidity, a lag of several days was observed. Compared to 70%, the risk for stroke at 90% relative humidity was highest at lag 2, with a 9% increase in stroke risk (OR = 1.09; 95% CI = 1.06–1.12) and was statistically significant at lags 1–4. Similar results were obtained for IS, while weaker associations were observed for ICH, possibly due to limited statistical power.
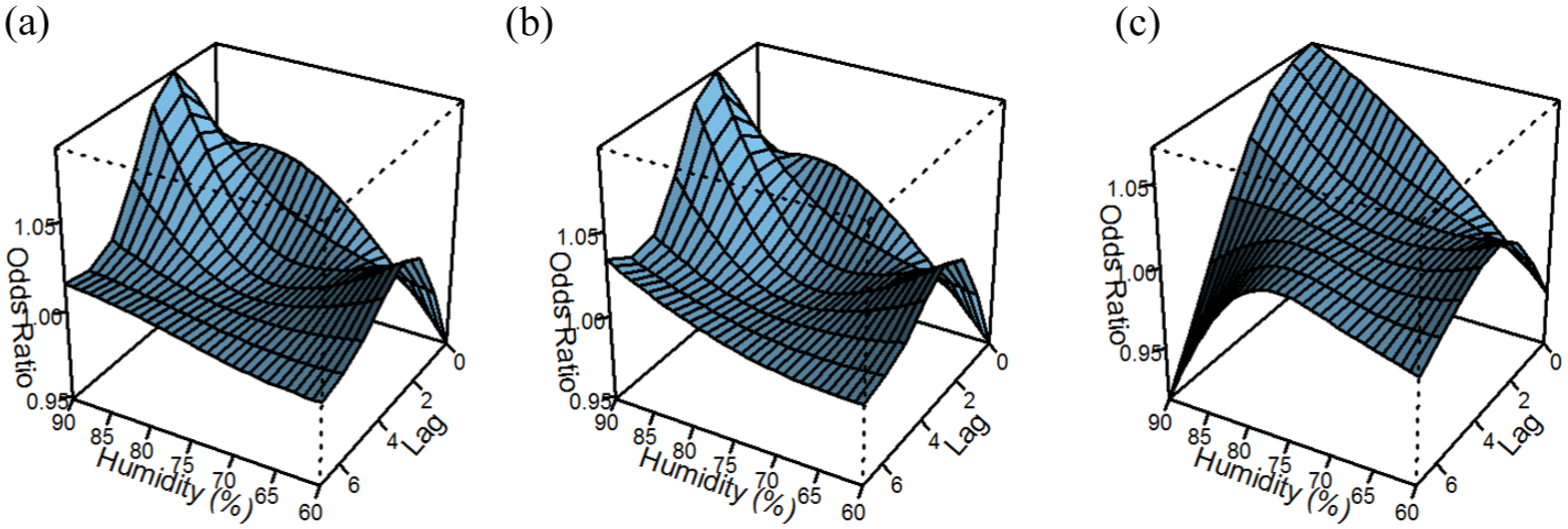
The association between relative humidity (%) and risk of total stroke (a), ischemic stroke (b), and intracerebral hemorrhage (c). Adjusted for mean ambient temperature and air pollution; reference: humidity at 70%.
Higher HI was associated with increased stroke risk, particularly on the stroke event date, reaching an increased stroke risk of approximately 40% comparing an HI of 100°F to that of 80°F (OR = 1.39; 95% CI = 1.32–1.47). The risk declined gradually with an increasing number of lag days but was statistically significant at lag 7. However, lower risk was noted at lags 3 and 4 comparing HI of 100°F to 80°F (OR = 0.97; 95% CI = 0.96–0.98 and OR = 0.98; 95% CI = 0.97–0.99). Similar findings were observed for IS and ICH stroke types, although the latter were less robust, possibly due to the smaller sample size (Figure 3 and Supplementary Table 3).
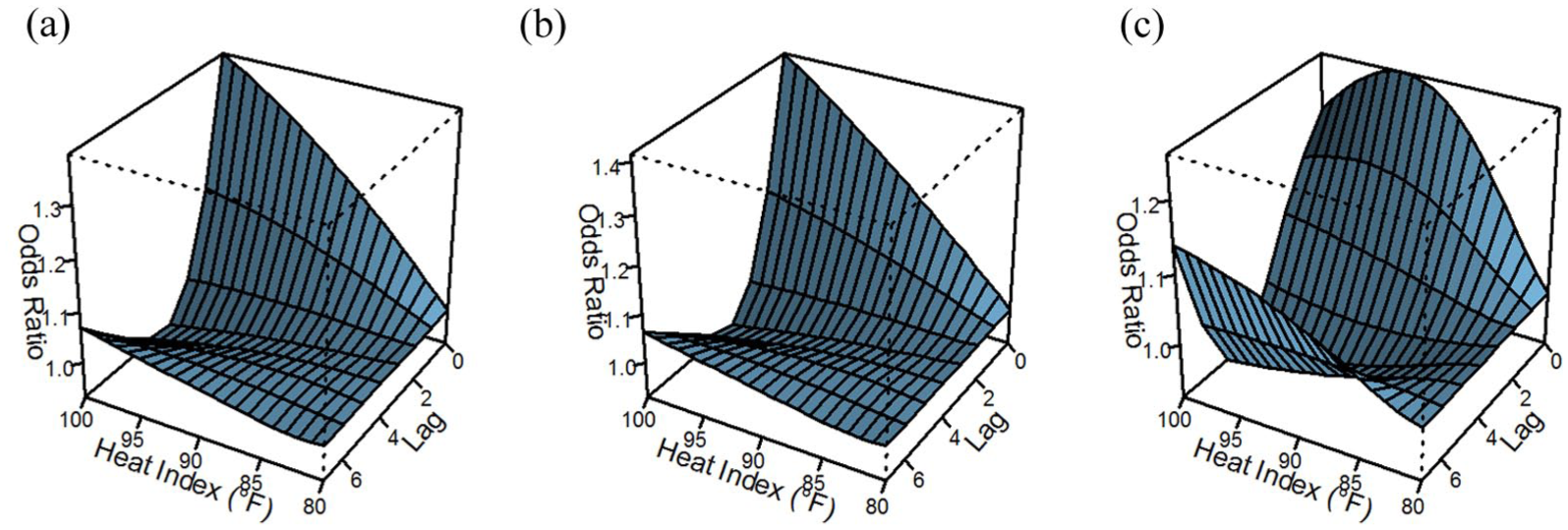
The association between heat index (°F) and risk of total stroke (a), ischemic stroke (b), and intracerebral hemorrhage (c). Adjusted for air pollution; reference: heat index at 80°F.
In sensitivity analyses excluding acute but ill-defined cerebrovascular disease (n = 1464) and iatrogenic cerebrovascular infarction/hemorrhage (n = 170), results were consistent with the primary analyses and were slightly stronger in most cases (Supplementary Tables 4–6).
Baseline characteristics of individuals with TIA (N = 8728) are presented in Supplementary Table 7. Their mean age was 69.4 ± 14.0 years, and 51.8% were men. The associations between climate measures and TIA were similar in magnitude and direction to those observed for IS (Supplementary Tables 8–10).
Supplementary Table 11 shows the association between HI categories at lag 0 and stroke risk stratified by potential modifiers. Statistically significant heterogeneity was observed by hypertension status when comparing caution level heat stress days with no heat stress days. In contrast, no differences by hypertension status were observed when comparing danger heat stress days with no heat stress days. No additional effect modification was observed by sociodemographic factors or other comorbidities.
Discussion
In our nationally representative study in the Eastern Mediterranean region, we demonstrate that both high ambient temperature and elevated relative humidity independently contribute to increased stroke incidence. Furthermore, we identify a significant association between HI, a composite measure integrating both variables, and stroke risk.
Previous studies assessing the link between high temperature and stroke risk yielded inconclusive results, which were attributed, at least partly, to geographic location. While most previous studies were conducted in Europe and China,6,9 our study adds data from the Mediterranean basin, which is highly impacted by climate change. 28 Furthermore, although the region’s population is acclimatized to high temperatures and most buildings are air-conditioned, 29 we showed that the impact of heat on stroke risk remains significant. In our study, ambient temperature was positively associated with stroke risk, with more than a 1.3-fold higher stroke incidence on days with temperatures of 32°C compared to those with 27°C. These findings contrast with meta-analyses that have reported substantial between-study heterogeneity in effect estimates of ambient temperatures during the warm season. Many studies included in these meta-analyses reported non-significant associations between high temperature and stroke morbidity or mortality, 6 and at least one comprehensive meta-analysis reported an overall null association. 9 However, evidence suggests that the strongest associations between elevated temperatures and cardiovascular morbidity and mortality, including stroke, are observed in tropical and Mediterranean regions. 9 Furthermore, our findings align with evidence indicating that elevated temperatures on hot days exert a short-term effect on stroke risk, with the impact most pronounced on the stroke event date or the preceding day. 30
Our findings reveal significant associations between relative humidity and incidence of stroke, particularly IS, independent of ambient temperature. These findings underscore the role of humidity in amplifying the adverse effects of ambient temperature on stroke risk, contrary to earlier studies that reported no clear association between relative humidity and incident stroke, 12 and a study in China suggesting a potential protective effect of higher humidity during the warm season. 13 Several methodological differences may account for these discrepancies. For instance, previous studies assessed humidity throughout the year rather than focusing on the warm season, 12 relied on self-reported stroke data, 13 and were limited by small sample sizes or low methodological quality. 12 While temperature tends to exert short-term effects on stroke occurrence, our analysis indicates a longer lag period for relative humidity, with the strongest associations observed 2–3 days prior to stroke onset. This suggests a distinct underlying mechanism driving the relationship between humidity and stroke risk.
Our study found a significant association between increasing HI and stroke risk, where exposure to HI values of 100°F (danger) was associated with a 1.4-fold increase in stroke risk. Although studies directly examining the relationship between HI and stroke are limited, research on related health outcomes supports our findings.15,31 Collectively, these findings suggest that relative humidity may exacerbate the adverse effects of high ambient temperature, underscoring the importance of HI as a critical environmental risk factor for stroke, particularly in the context of climate change.
Previous research suggests that high ambient temperatures may disproportionately increase IS risk.5,32 However, our findings indicate comparable effect sizes for both stroke types. Notably, we found a trend toward smaller effect sizes of relative humidity and HI on ICH, particularly at the highest humidity/HI levels. Thus, extreme heat conditions may exert differential impacts on stroke types. Nonetheless, given the limited statistical power of ICH due to lower incidence, these findings should be interpreted with caution and warrant validation in larger, independent cohorts.
The slightly stronger associations observed in the sensitivity analyses, excluding acute but ill-defined cerebrovascular disease and iatrogenic cerebrovascular infarction or hemorrhage stroke, suggest that the inclusion of these diagnoses may have attenuated the primary estimates since they are less affected by ambient environmental conditions. Furthermore, the similarity of results observed for TIA and IS may indicate shared underlying pathophysiological mechanisms linking short-term heat exposure to cerebrovascular risk.
We observed no consistent evidence of effect heterogeneity across sociodemographic, lifestyle, or clinical characteristics. This contrasts with findings suggesting stronger associations between heat exposure and IS among individuals with underlying cardiovascular risk factors. 33 This inconsistency may be partly explained by methodological differences, particularly the use of hourly temperature estimates in the previous study compared with daily exposure metrics in our study. Our findings support the hypothesis that heat stress may be a general acute trigger for stroke across diverse subpopulations.
The mechanisms underlying the associations between high temperature and stroke risk are complex and speculative. Dehydration, caused by increased sweating and skin blood flow, may lead to hemoconcentration and hyperviscosity and electrolyte disturbance, which enhance thromboembolism and promote the development of IS. 34 Exposure to high temperatures can also lead to inflammatory response and endothelial dysfunction, 35 which may enhance consumptive coagulation, thus explaining the associations observed for both IS and ICH.32,36 The role of heat stress, which combines both high temperatures and humidity, has been less studied. We suggest that the slower evaporation of sweat due to high humidity may cause difficulty in maintaining a stable core body temperature. The body’s attempts to restore heat balance despite the high humidity, by increasing sweating and blood flow to the skin, exert strain on the heart and may result in hemoconcentration and cerebral thrombosis, particularly in individuals with pre-existing atherosclerosis. 37 Indeed, our findings show stronger associations of relative humidity and HI with IS risk compared with ICH risk.
This study has several notable strengths. First, stroke event data were obtained from a national registry covering all hospitals in Israel. Second, the case-crossover design with time-stratified sampling controls for inter-individual characteristics as well as regional and seasonal confounding. Third, the use of DLNM enables modeling of both nonlinear and lagged effects of heat exposure on stroke risk, while accounting for correlations across days. Finally, ambient temperature and air pollution parameters were derived from satellite-based sources at a very fine spatial resolution. The study also has several limitations. First, exposure assessment was based on meteorological measures assigned to participants’ residential address at time of admission, without accounting for potential residential mobility or time spent in other locations. Nevertheless, resulting exposure misclassification was likely limited. Air-conditioning availability in Israel is nearly universal (~ 96.8% of households reporting ownership), likely reducing variability in heat exposure across indoor environments. 29 In addition, misclassification due to occupational heat exposure is unlikely to have substantially influenced our findings. The mean age of the study population was 71 ± 14 years; most participants were therefore beyond the statutory retirement age in Israel (67 years for men and 65 years for women). Although approximately 13% of the Israeli workforce is occupationally exposed to heat, physically demanding outdoor work is largely performed by younger, foreign workers. 38 Indeed, a recent survey indicated that most occupationally heat-exposed workers are 22–45 years of age. 39 While some degree of exposure misclassification cannot be excluded, it is unlikely to differ systematically by outcome status, thus leading to an underestimation of the true associations. Second, the INSR includes only cases of individuals who reached the hospital, potentially missing those who died before admission or recovered without hospitalization. In addition, because admission dates served as proxies for true stroke onset, some misclassification is likely, potentially delaying or attenuating the estimated associations across lag days. Third, different approaches were used to measure climate parameters. Notably, relative humidity data were obtained from meteorological stations due to the lack of satellite-based models. Fourth, despite the overall large sample size, stratification by heat stress categories and participant characteristics may have limited statistical power. Fifth, we cannot exclude the possibility of residual confounding by environmental and behavioral factors that were not available in our database. Finally, the findings are generalizable only to the warm season.
Conclusion
We demonstrate that high temperature, humidity, and HI during the warm season are independently associated with increased risk of both ischemic and hemorrhagic stroke, particularly on the stroke event date and the preceding week. These findings support previous research focusing on ambient temperature and extend existing evidence to HI and the Middle Eastern population that is acclimatized to high temperatures and in which most buildings are air-conditioned. Since the observed warming trends in the Mediterranean basin are projected to continue and intensify throughout the 21st century, 40 policy recommendations are crucial for public health. These recommendations should address both humidity and heat stress, in addition to temperature. Particularly, clinicians and stroke-vulnerable individuals should take adequate steps in the days following increased heat stress exposure to prevent the subsequent development of acute stroke.
Supplemental Material
sj-docx-1-wso-10.1177_17474930261429880 – Supplemental material for High ambient temperature, humidity, heat index, and stroke risk in a Mediterranean region
Supplemental material, sj-docx-1-wso-10.1177_17474930261429880 for High ambient temperature, humidity, heat index, and stroke risk in a Mediterranean region by Maya Negev, Shlomit Paz, Shiraz Vered, Itai Kloog and Galit Weinstein in International Journal of Stroke
Footnotes
Author contributions
All authors contributed to the study conception and design, revised the manuscript, and approved its final version. Drs G.W. and S.V. contributed to the study design and methodology. Dr S.V. conducted the statistical analysis. Dr G.W. wrote the original draft. Drs G.W., M.N., and S.P. acquired the funding that supported this research.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was funded by the Israel Science Foundation (grant no. 583/20).
Ethical statement
The Helsinki approval number is 7765-20-SMC. The University of Haifa ethics committee approval number is 160/21. This study did not involve the collection of new data from human participants. Consequently, informed consent was not required.
Supplemental material
Supplemental material for this article is available online.