
Abstract
Background:
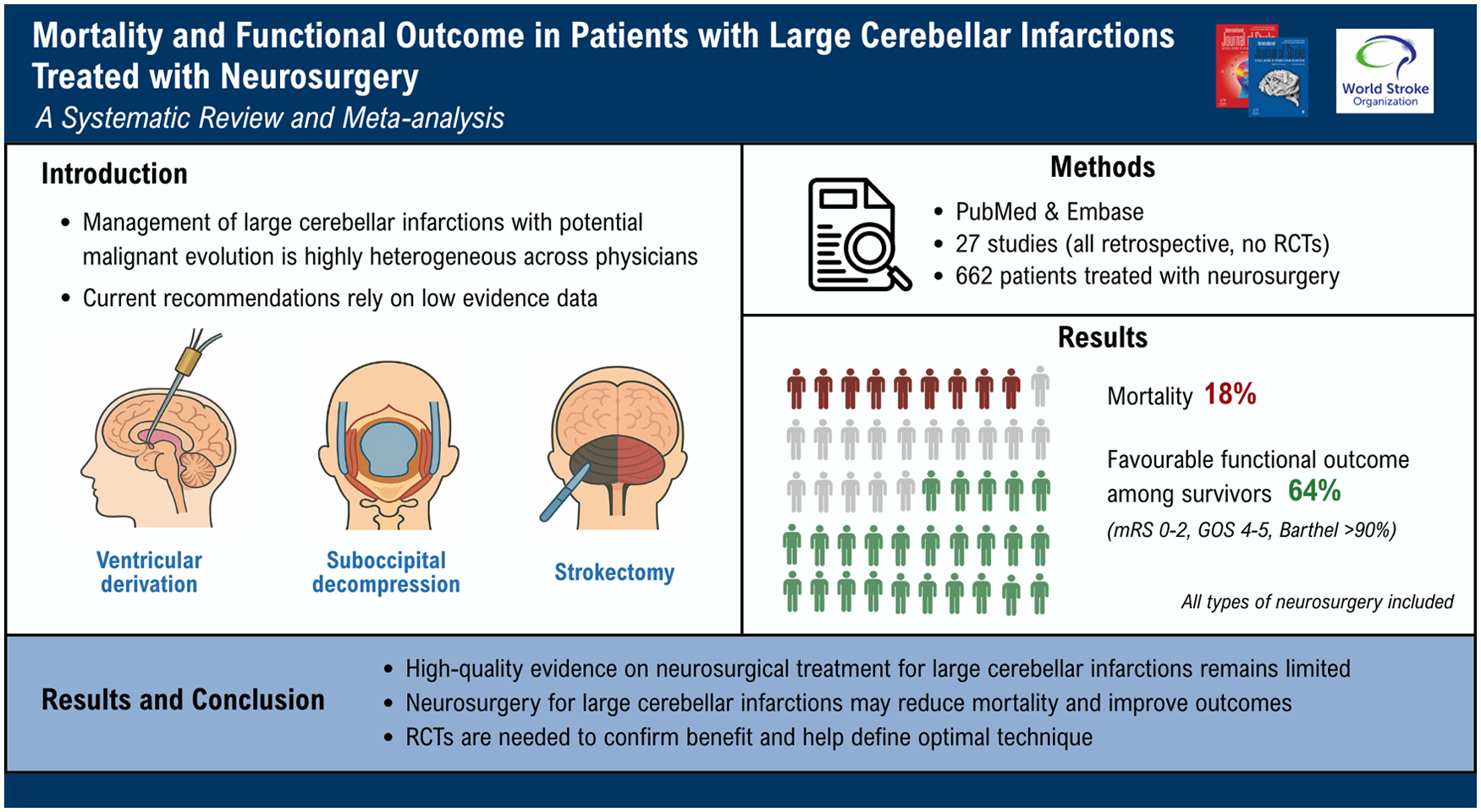
Management of large cerebellar infarctions with potential malignant evolution is highly heterogeneous across physicians, and recommendations rely on low-evidence studies.
Aim:
We aimed to perform a systematic review and meta-analysis on patients with large cerebellar infarction undergoing neurosurgery, to study mortality and functional outcome, according to neurosurgical technique.
Summary of review:
We searched on PubMed and Embase according to pre-defined selection criteria and we assessed their quality according to a predefined risk of bias scale. Our primary outcomes were mortality and functional outcome rates. Favorable outcome was defined as a modified Rankin scale of 0–2, a Glasgow Outcome Scale of 4–5, or a Barthel Index > 90%. Pooled rates were obtained using random effect model and heterogeneity was quantified using I2 statistics. Among 27 included studies (including 1173 patients), we studied the 662 patients undergoing neurosurgery. All studies were retrospective and observational; there was no randomized clinical trial (RCT). The median selection bias score was 5 (IQR, 4–6). Mortality rate was estimated at 18% [95% CI, 13–24%], I2 58%. Among survivors, 64% achieved a favorable functional outcome [95% CI, 51–77%], I2 82%. Study design and heterogeneity in patients’ characteristics limited a meaningful comparison of mortality and functional outcome according to neurosurgical techniques.
Conclusion:
High-quality evidence on neurosurgical treatment for large cerebellar infarctions remains limited. Our systematic review and meta-analysis, despite moderate risk of bias, suggest that neurosurgery may reduce mortality and improve functional outcomes. These findings support its potential benefit, but RCTs are needed to confirm effectiveness and evaluate best surgical technique.
Keywords
Get full access to this article
View all access options for this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.