
Abstract
Background:
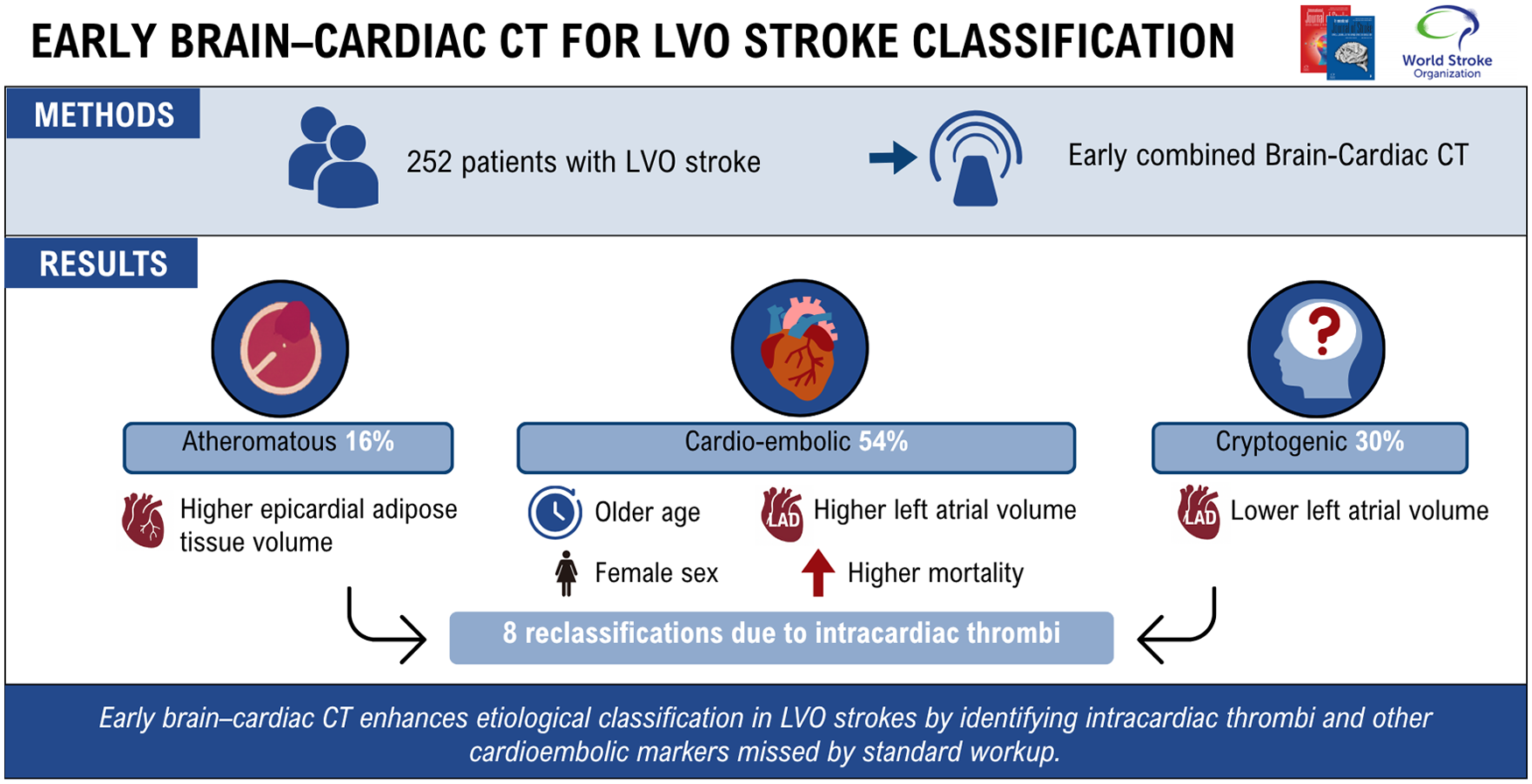
Timely identification of stroke etiology is crucial in managing large vessel occlusion (LVO) strokes. However, a substantial proportion remains cryptogenic despite comprehensive workup, raising concern about underdiagnosed cardioembolic sources. This study assessed the diagnostic contribution of early combined brain–cardiac CT imaging in patients with LVO stroke and explored imaging markers associated with each etiological subtype.
Methods:
A total of 252 consecutive patients admitted for LVO stroke who underwent standardized acute-phase brain and cardiac CT imaging were included. Patients were classified as atheromatous, cardioembolic, or cryptogenic LVO stroke before and after consideration of cardiac CT results. Clinical and imaging characteristics of patients were compared according to final causes of stroke.
Results:
Cardiac CT led to etiological reclassification in 8 patients (3.2%), including 7 cryptogenic cases upgraded to cardioembolic due to detection of intracardiac thrombi in the absence of atrial fibrillation. Patients with cardioembolic LVO stroke (n = 137, 54%) were older, more frequently women, and had higher left atrial surface areas and volumes compared to atheromatous (n = 40, 16%) and cryptogenic cases (n = 75, 30%). Epicardial adipose tissue volume was highest in atheromatous strokes, while cryptogenic cases lacked markers of atrial cardiomyopathy. At follow-up, mortality was highest in the cardioembolic group.
Conclusion:
Early brain–cardiac CT imaging enhances etiological classification in LVO strokes by identifying intracardiac thrombi and other cardioembolic markers missed by standard workup. A substantial subset of cryptogenic LVO strokes may represent a distinct pathophysiological entity. Broader adoption of cardiac CT could inform targeted stroke prevention strategies.
Get full access to this article
View all access options for this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.