
Abstract
Background and Aims:
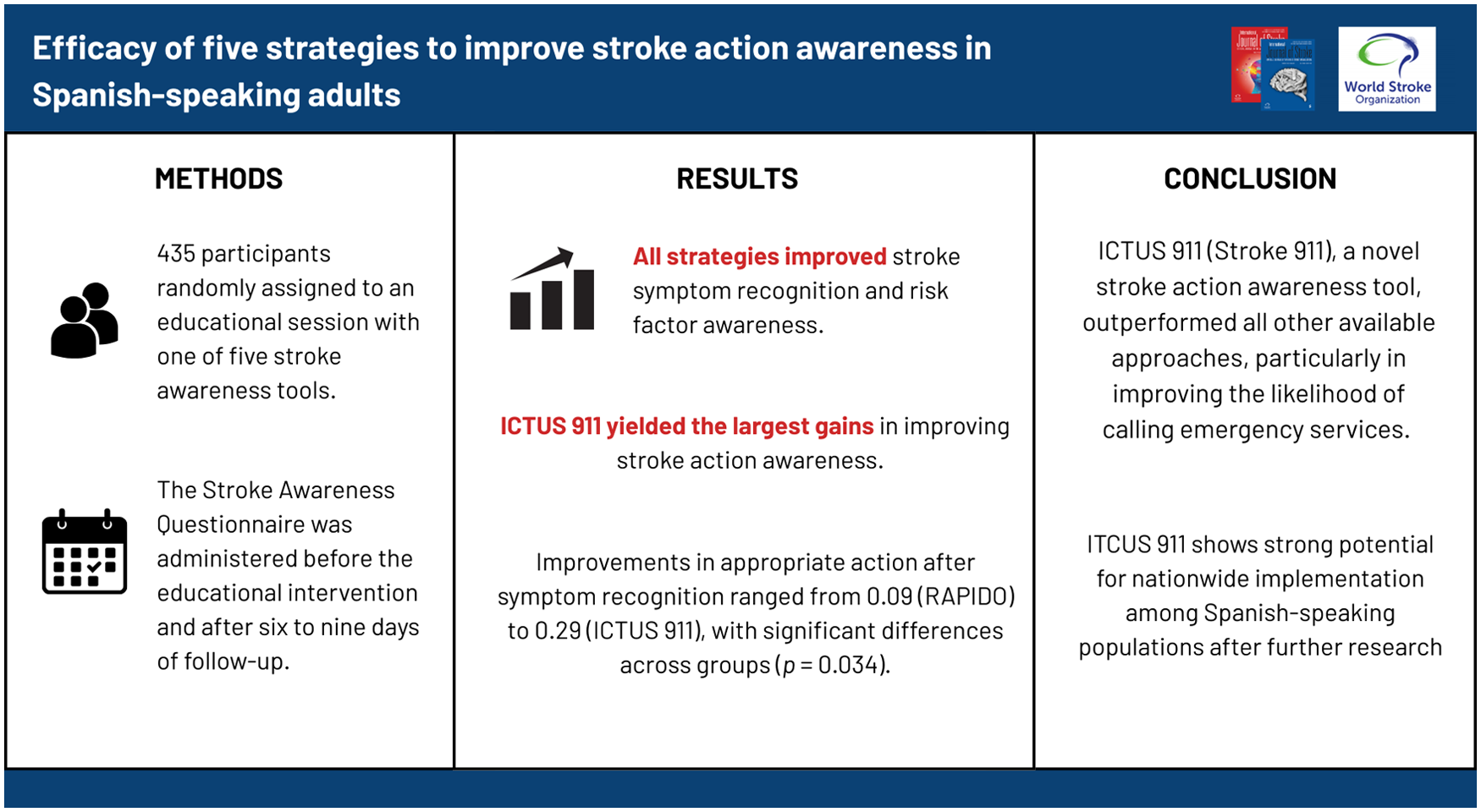
Improving stroke action awareness is challenging in non-English-speaking populations. In this study, we evaluated the effectiveness of five Spanish-language educational tools in improving recognition and making an emergency response to stroke symptoms among Spanish-speaking adults in Mexico.
Methods:
Spanish-speaking participants were recruited from public spaces. Individuals with a history of stroke were excluded. Participants were randomly assigned to receive an educational session tailored to one of five stroke awareness tools (RAPIDO, DALE, CAMALEON, CORRE, and ICTUS 911). Stroke knowledge was assessed using the Stroke Awareness Questionnaire before the educational intervention and after 6–9 days of follow-up. The primary outcome was the change in the proportions of correctly identified stroke symptoms. Secondary outcomes included changes in participants’ achievement of adequate stroke knowledge in individual FAST domains and their understanding of the appropriate actions to take after identifying stroke symptoms.
Results:
In data from 435 participants, all strategies improved stroke symptom recognition and risk factor awareness, although no statistically significant differences were observed in the primary outcomes. Changes ranged from 0.35 (DALE) to 0.49 (CAMALEON) for Facial Weakness, the symptom with the largest improvement, and from 0.00 (CAMALEON, CORRE, RAPIDO) to 0.15 (DALE) for Problems with Vision, the symptom with the smallest improvement. For the secondary outcomes, increases in adequate stroke knowledge ranged from 0.18 (CORRE, DALE) to 0.31 (ICTUS 911); between-group comparisons were statistically significant (p = 0.027). Improvements in appropriate action after symptom recognition ranged from 0.09 (RAPIDO) to 0.29 (ICTUS 911), with significant differences across groups (p = 0.034).
Conclusions:
This study shows that brief educational interventions can improve stroke symptom recognition and intended response in Spanish-speaking adults. Among five strategies, ICTUS 911 yielded the largest short-term gains, supporting its potential utility. Further research is needed to assess long-term effectiveness and broader applicability.
Keywords
Introduction
The general population seems to know little about the signs and symptoms of stroke and what to do when symptoms occur.1 –3 There is also limited knowledge about the relationship between knowledge of stroke symptoms and time to hospital arrival.4 –7 Time is the most critical factor impacting the effectiveness of interventions for acute stroke.8,9 Many patients are excluded from reperfusion treatment because the prehospital delay exceeds the treatment window. 10 In high-income countries, public awareness strategies have been instituted, such as the “Stroke Chain of Survival” (the United States) and “Face, Arm, Speech, Time” (FAST)—Australia and the United Kingdom),11,12 to reduce delays in the arrival of patients with stroke symptoms at the hospital. These programs are based on the premise that a better identification of stroke symptoms will lead to an immediate call to an ambulance. However, translating these programs to countries with developing economies has been particularly difficult, mainly due to the language and cultural barriers. 13 In population-based surveys from Latin America, fewer than 50% of respondents can name even one warning sign of stroke, and only a minority report intent to call emergency services when symptoms occur.14,15 Median prehospital delay times in urban centers of Mexico and South America have been reported to range from 6 to 12 hr, far exceeding recommended treatment windows.16,17
One non-English language example of addressing these challenges is the Stroke 120 program in China, where 120 is used for calling emergency medical services. 18 This initiative adapted the FAST mnemonic to align with local linguistic and cultural contexts by utilizing the Chinese emergency phone number (120) to represent the main stroke recognition signs as one uneven face (crooked mouth), one weak arm (arm weakness), and two incoherent lips (slurred speech). This program highlights the potential of non-literal approaches for adapting strategies like FAST to overcome language and cultural barriers, making them more effective in diverse settings.
Still, efforts in Spanish-speaking populations have primarily focused on literal translations of the FAST acronym. Up to 2024, there have been at least four proposals for the literal translation of the FAST acronym into Spanish, with an additional stroke awareness strategy that is suitable for various language situations, including Spanish, where 911 is used as an emergency phone number: Stroke 911. 19 Understanding the effectiveness of these five potential strategies in increasing stroke symptom awareness in Spanish-speaking populations is paramount to developing effective implementation plans. Still, their performance has not been studied either individually or comparatively before. Therefore, in this randomized trial, we aimed to determine the performance of each approach and compare their efficacy in increasing stroke awareness in Spanish-speaking adults after a brief educational intervention. This is the first randomized trial comparing all five Spanish-language stroke educational tools.
Methods
Study design
This study was a randomized trial in a Spanish-speaking population to determine the effectiveness of five stroke awareness educational strategies in improving participant knowledge and recognition of stroke symptoms and actions: RAPIDO, DALE, CAMALEON, CORRE, or ICTUS 911.
Participants
Participants were recruited in the city of Aguascalientes, a mid-sized urban area in central Mexico, and Culiacán, Sinaloa, a larger metropolitan city in the northwest of the country, by one of the investigators (J.M.M.-R., C.D.P.-M., J.P.-L., or K.I.S.-R.). Recruitment occurred in public urban spaces, including plazas, sidewalks, and waiting areas outside primary care clinics, with no restrictions based on their health insurance status. Eligible individuals were adults aged 18 or older who provided informed consent to participate. Individuals with a history of stroke were excluded from the study. Participants who failed to complete both scheduled evaluations were withdrawn from the analysis.
Randomization
One of the recruiters (unblinded) randomly assigned participants to one of the five intervention groups using a pre-generated table of permutations of the five strategies. Patients were sequentially allocated to each permutation, ensuring that group sizes remained equal at all recruitment stages.
Sample size calculation
The required sample size was calculated to detect a medium effect size (Cohen’s d = 0.50) at a significance level of α = 0.05 and a power (1−β) of 80% using recommendations for educational interventions. 20 The calculation determined a minimum of 64 participants per group. This sample size calculation estimated the number of participants required to detect a medium effect size for within-group comparisons of pre- and post-intervention proportions, as these comparisons inherently reduce variability due to their paired nature, requiring fewer participants. In addition, the study design included comparisons between five groups, for which ANOVA calculations suggested a larger sample size per group (up to one thousand). However, given the dual focus on within- and between-group analyses, the sample size of 65 participants per group was deemed sufficient and practical. Post hoc power analysis confirmed adequate power for detecting medium effect sizes in the between-group analysis (Using an ANOVA approach with a medium effect size (Cohen’s f = 0.25), and a significance level of α = 0.05, power is 96.4% for detecting a medium effect size.
Intervention
After providing informed consent, one of the trial investigators (J.M.M.-R., C.D.P.-M., J.P.-L., or K.I.S.-R.) administered the baseline SAQ. Then, they proceeded to administer the intervention. The intervention consisted of a brief educational session lasting 10–15 min. This session included a presentation on stroke risk factors and symptoms and emphasized the urgency of calling an ambulance if symptoms occur. Each educational session was tailored to one of the five proposed strategies described below and illustrated in Figure 1. The investigators administering the intervention were experts in each strategy and ensured that every session was delivered consistently following a uniform, three-part structure: first, a brief introduction to stroke symptoms and risk factors; second, a comprehensive presentation of the strategy supported by visual materials; and third, a focused emphasis on the appropriate action when stroke symptoms are identified—namely, to call an ambulance.
RAPIDO (Quickly)—Developed in 2021 by researchers at the University of Texas to adapt the English FAST mnemonic for Spanish-speaking communities. The acronym emphasizes drooping face, balance disturbance, loss of strength in an arm or leg, visual impairment, difficulty speaking, and getting help quickly. 21
DALE (Give it)—Created in 2012 by researchers at the University of Guadalajara, Mexico, to mirror the English FAST mnemonic for Mexican populations. The acronym includes facial weakness, arm weakness, speech problems, and reaching out for help. 22
CAMALEON (Chameleon)—Developed in 2016 by Dr Miguel Ángel Barboza Elizondo in collaboration with the pharmaceutical industry in Costa Rica. The acronym conveys drooping face, heavy hand, tongue impairment, and call 911. 23
CORRE (Run)—Designed in 2022 by Colombian neurologist Dr Luis Fernando Roa Wandurraga. Includes: twisted face, visual disturbance, sudden weakness in an arm or leg, speech oddity, call emergencies. 24
ICTUS 911—This stroke educational tool was developed from the Stroke 911 strategy for people living in areas where 911 is used as an emergency phone number. 19 If there is difficulty speaking when repeating the number 911, A twisted face or mouth, or A weak arm or leg. J.M.M.-R. and R.L. performed the Spanish translation work.
Figure 2 depicts sample graphic representations of the five strategies in Spanish and FAST in English.
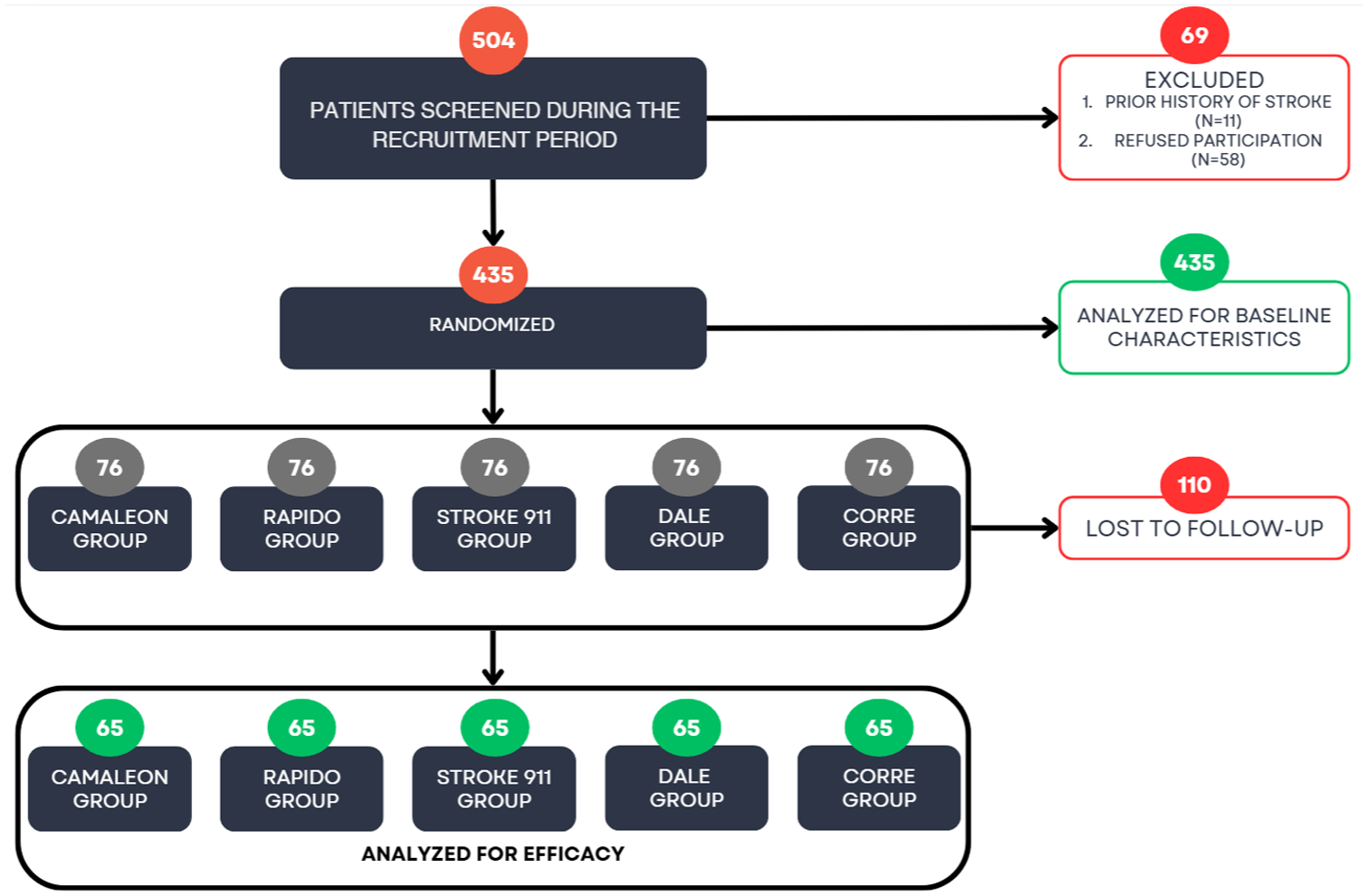
Flowchart of the trial.

Graphic representations of the five strategies in Spanish with English translation. RAPIDO means quickly; the acronym stands for drooping face, balance disturbance, loss of strength in an arm or leg, visual impairment, difficulty speaking, and getting help quickly. DALE means “give it”; the acronym stands for facial weakness, arm weakness, speech problems, and reaching out for help. CAMALEON is the word in Spanish for chameleon; The acronym stands for drooping face, heavy hand, tongue impairment, and call 911. CORRE means to run; the acronym stands for twisted face, visual disturbance, sudden weakness in an arm or leg, speech oddity, and call emergencies. ICTUS 911, the word ictus means stroke. In this strategy, there is no acronym, but the number 911 is used to detect difficulty speaking when repeating the number nine aloud; it also instructs to seek one twisted face or mouth, or one weak arm or leg.
Outcome measures
Stroke knowledge was evaluated using the Stroke Awareness Questionnaire (SAQ). 25 This tool evaluates three domains: stroke risk factors, symptoms, and the appropriate response to stroke symptoms. The primary outcome was the change in the proportions of each of the nine symptoms (plus the compound category “any FAST symptom”) contained in the SAQ’s symptoms domain. The change in the proportion of each symptom was calculated by subtracting the proportion of participants correctly identifying the symptom before the intervention from the proportion correctly identifying it after the intervention. Secondary Outcomes. (1) The change in the proportion of participants achieving adequate stroke knowledge after the intervention. Adequate knowledge was defined as correctly identifying at least one stroke risk factor and at least one stroke symptom, and taking appropriate action after identifying stroke symptoms. 15 (2) The change in the proportion of patients taking appropriate action after identifying stroke symptoms after the intervention.
While primary and secondary outcomes focused on specific SAQ domains, we also descriptively report changes in other SAQ items, such as TIA awareness and stroke risk factor identification.
Follow-up and participant retention
After the intervention, participants were contacted at least 6 days post-intervention via phone call or instant messaging service to complete follow-up assessments, which included administering sections A and B of the SAQ. At least five follow-up contact attempts were made before a participant was considered lost to follow-up.
Follow-up efforts were stopped once two criteria were met: (1) the minimum required quota of 64 participants per group, as determined by the sample size calculation, was achieved, and (2) all five groups were balanced in size. The final dataset included responses from 435 participants (65 per group), with 110 individuals lost to follow-up after meeting these defined stopping criteria. This process is demonstrated in Figure 1. Since sequential randomization maintained equal group sizes throughout recruitment and the stopping criteria ensured proportional follow-up across groups, the proportions of participants lost to follow-up were identical across the five groups.
Statistical analysis
Continuous variables were described as mean ± SD or median (IQR), depending on normality (determined by the Shapiro–Wilk test). Categorical variables were expressed as frequencies and percentages. Changes in proportions within groups (pre- and post-intervention) were analyzed using McNemar’s test. All proportions were presented as percentages. Between-group differences across the five strategies were assessed using the chi-square or Fisher’s exact test for small sample sizes. All analyses were conducted using R (R Foundation for Statistical Computing, Vienna, Austria), with statistical significance set at 0.05.
Results
During the recruitment period, 435 participants were randomized to receive the intervention; 249 (57.2%) were females. The mean age was 40 ± 18 years. Data on medical history and demographics in the SAQ were obtained from all of them. Baseline characteristics and SAQ responses did not differ significantly between participants who completed follow-up and those who were lost to follow-up. Supplemental Table 1 summarizes the responses with comparisons by participation group. Employment was the predominant occupational status, accounting for 53.6% of participants, though a slightly larger proportion of those included in the study were working compared to those lost to follow-up.
Most participants resided in low- to middle-income housing (64.6%), which was more frequent among the lost group than the included group (72.7% vs 61.8%, p = 0.077). Social security coverage was reported by 83.4% of participants, with slightly higher coverage among those lost to follow-up (88.2%) compared to those retained (81.8%). The prevalence of chronic health conditions, such as high blood pressure and high cholesterol, was generally low, and no substantial differences were observed between groups. Smoking was uncommon, with 6% of participants reporting smoking daily.
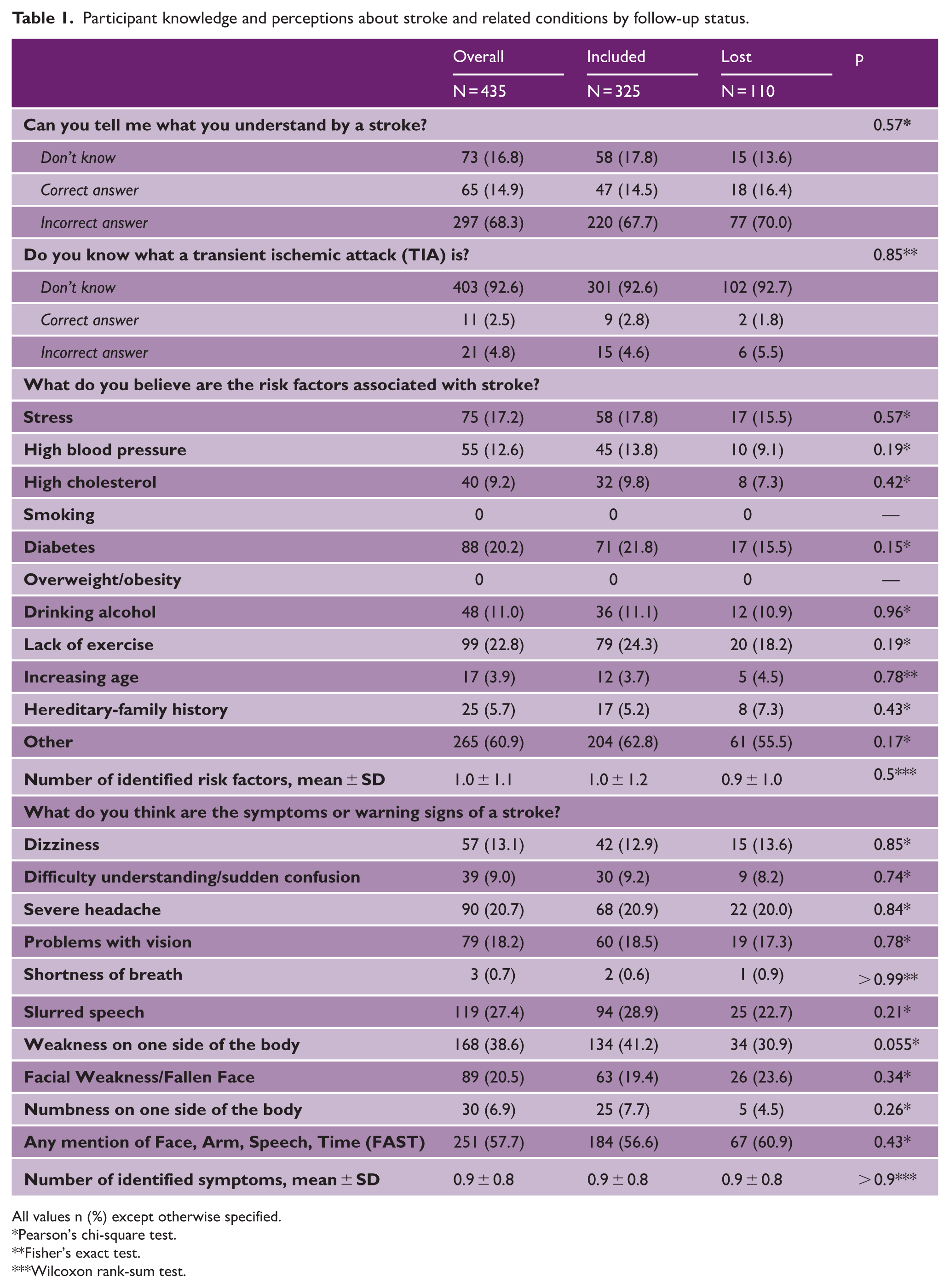
Table 1 presents participants’ knowledge and perceptions about stroke (SAQ section A), transient ischemic attack (TIA), and related conditions. When asked about their understanding of a stroke, 17% of participants reported no knowledge, while 14.9% responded correctly. Knowledge about TIA was limited, with 93% stating they did not know what a TIA was, and only 2.5% providing an accurate definition.
Participant knowledge and perceptions about stroke and related conditions by follow-up status.
All values n (%) except otherwise specified.
Pearson’s chi-square test.
Fisher’s exact test.
Wilcoxon rank-sum test.
Participants identified multiple stroke risk factors, with stress (17.2%), diabetes (20.2%), and lack of exercise (22.8%) being the most frequently mentioned. The number of identified risk factors was low overall, with an average of 1.0 ± 1.1 per participant. Awareness of stroke symptoms was similarly limited; weakness on one side of the body (39%) and slurred speech (27%) were the most recognized symptoms. Only 58% of participants mentioned components of the FAST mnemonic. Table 2 shows the baseline knowledge of stroke symptoms. There were no statistical differences across the five groups. Regarding perceptions of disease severity, stroke and cancer were most frequently rated as “worst imaginable condition” (34.0% and 45.7%, respectively); perceptions about other conditions, such as heart attack and diabetes, were categorized mainly as “very serious” or “extremely serious.”
Percentage of participants in each group with baseline knowledge of stroke symptoms.
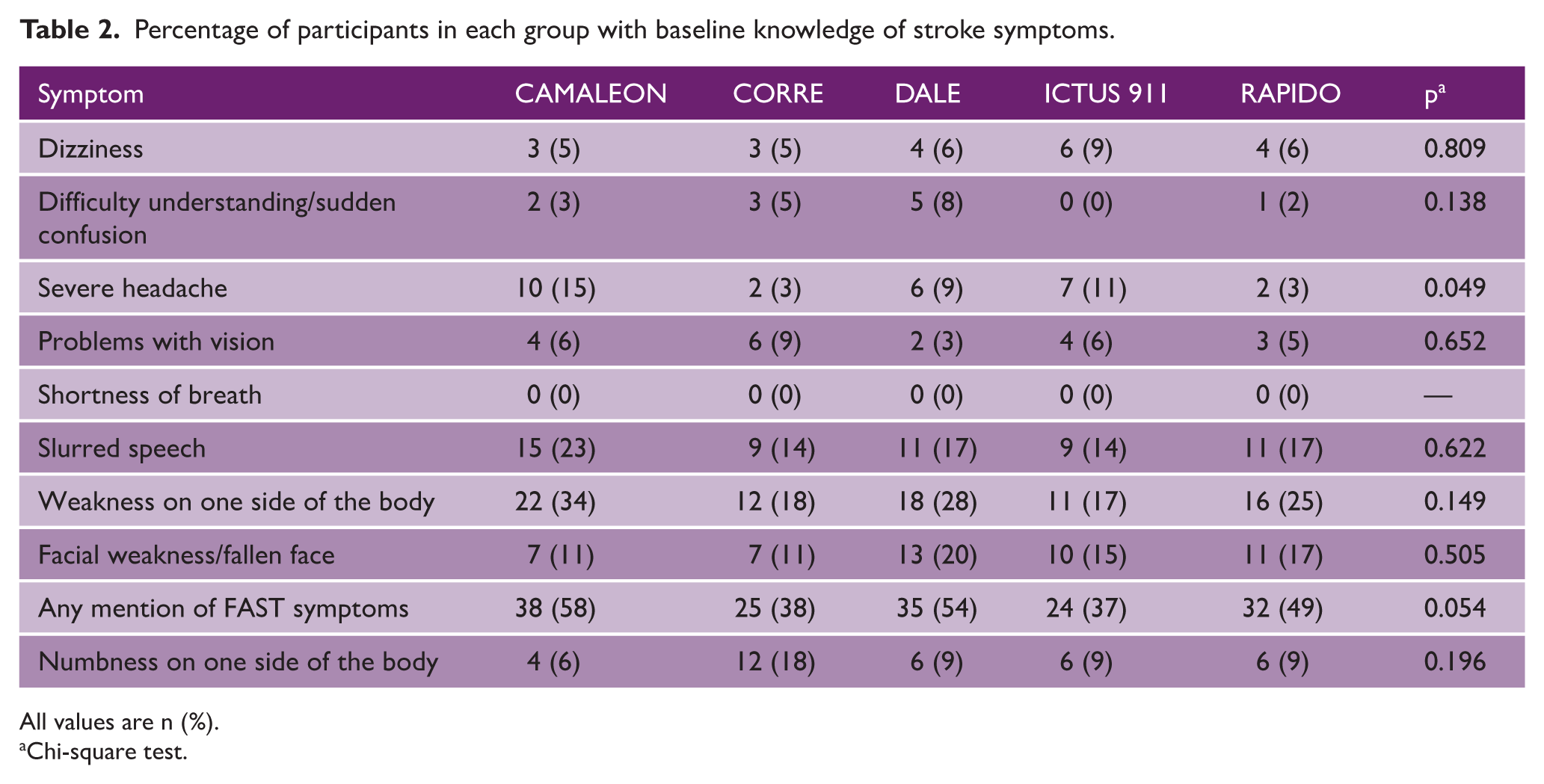
All values are n (%).
Chi-square test.
Primary outcome
Table 3 and Supplemental Figure 1 depict the trial’s primary outcome results. Overall, symptom awareness increased in all groups, but there were no statistically significant between-group differences in the change in symptom identification groups. The largest improvements in the proportion of identified stroke symptoms were observed for facial weakness or fallen face recognition, with an increase of 49% in the CAMALEON group and 46% in the ICTUS 911 group. Recognition of slurred speech and weakness on one side of the body also improved significantly across all groups, with changes up to 43% (ICTUS 911 group). Recognition of the symptoms in the FAST acronym varied, with the highest increase of 45% in the CORRE group. In contrast, symptoms such as shortness of breath and problems with vision saw minimal changes. Figure 3 provides a detailed description of the pre- and post-intervention proportion of symptoms identified in each group.
Post-intervention changes in percentage points for stroke symptom identification by group.
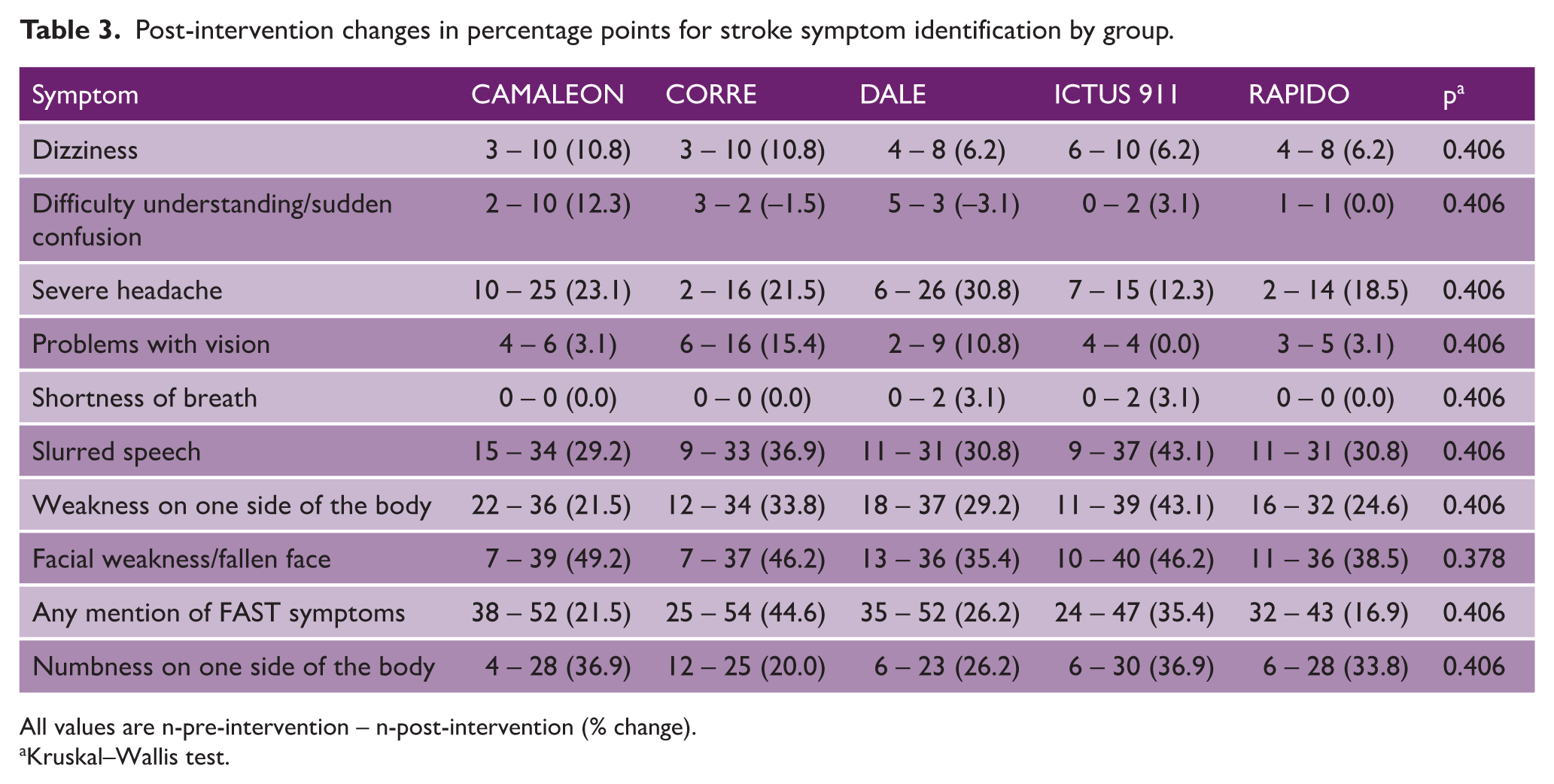
All values are n-pre-intervention – n-post-intervention (% change).
Kruskal–Wallis test.
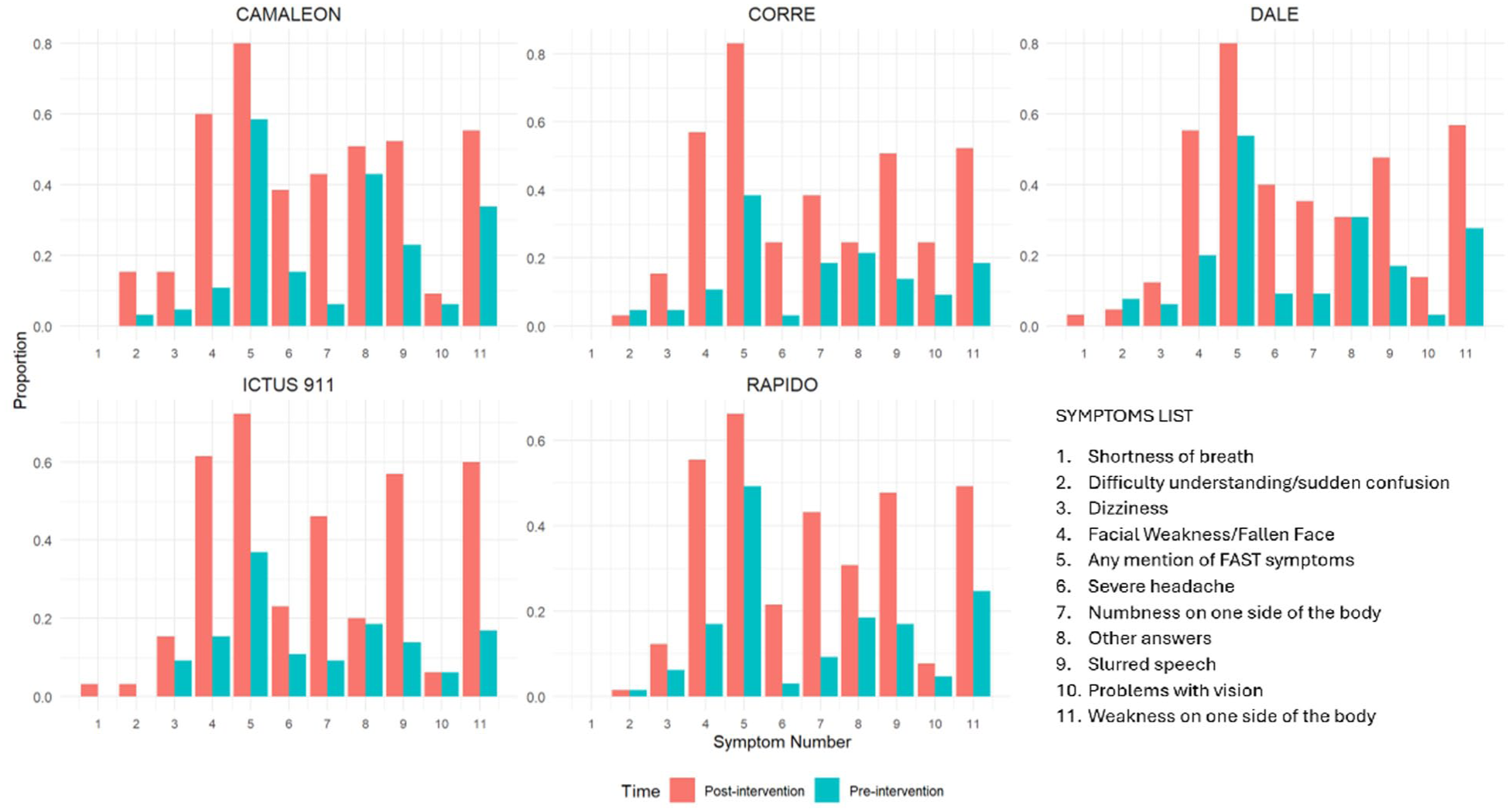
The proportion of symptoms identified pre- and post-intervention by the group.
Secondary outcomes
Statistically significant differences were found in both secondary objectives (Table 4).
Post-intervention changes in percentage points for stroke knowledge and intended action by group.
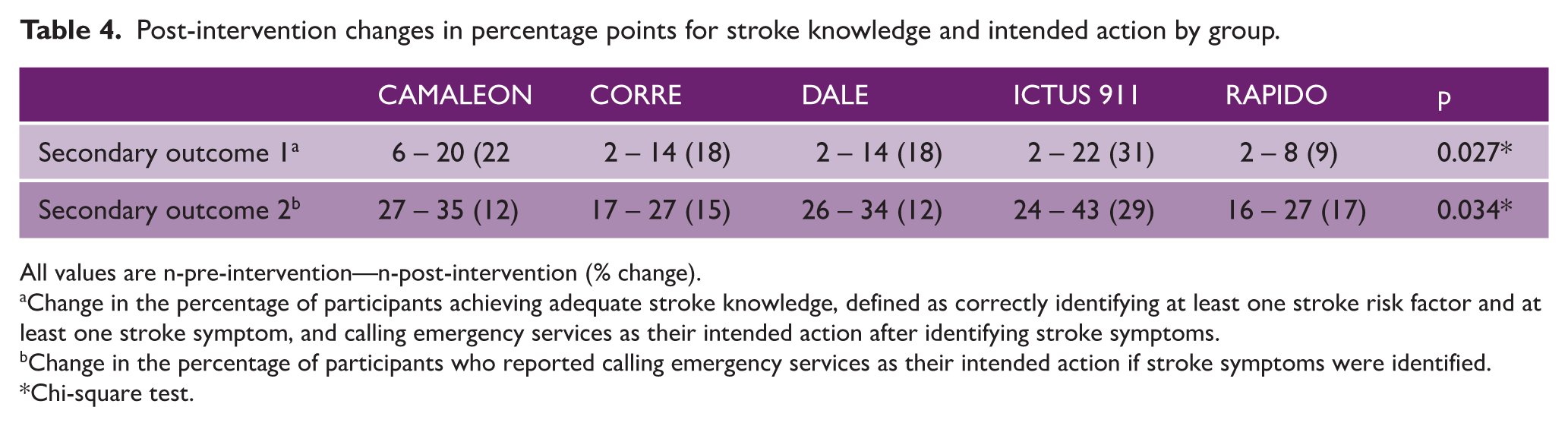
All values are n-pre-intervention—n-post-intervention (% change).
Change in the percentage of participants achieving adequate stroke knowledge, defined as correctly identifying at least one stroke risk factor and at least one stroke symptom, and calling emergency services as their intended action after identifying stroke symptoms.
Change in the percentage of participants who reported calling emergency services as their intended action if stroke symptoms were identified.
Chi-square test.
Change in Adequate Stroke Knowledge: The ICTUS 911 intervention demonstrated the most significant improvement in the proportion of participants achieving adequate stroke knowledge (31% increase), followed by CAMALEON (22% increase), while RAPIDO had the lowest change (9% increase).
Change in Appropriate Action After Identifying Stroke Symptoms: The proportion of participants taking appropriate action after identifying stroke symptoms consistently increased from 12% to 17% for the CAMALEON, RAPIDO, DALE, and CORRE strategies. However, the increase in the ICTUS 911 group (29%) was significantly higher.
Stroke knowledge
Supplemental Table 2 compares participant responses before and after implementing the interventions across the first part of the SAQ. Across all groups, the average proportion of participants who correctly defined stroke increased significantly from 14% to 61% following the intervention (p < 0.001; see Supplemental Table 2).
Similarly, awareness of transient ischemic attack (TIA) improved, with the percentages of correct responses rising in all the groups. The number of stroke risk factors identified increased significantly post-intervention for all strategies. Smoking and obesity were more frequently identified as risk factors after interventions, particularly in the CAMALEON and DALE groups, where participants initially did not mention these factors at all.
Discussion
This is the first randomized study to assess the efficacy of brief educational interventions using different stroke awareness tools in a Spanish-speaking population. Unlike English-speaking countries where tools like FAST or BEFAST are widely used, many Spanish-language tools exist, yet few have been formally evaluated. Spanish is the second most spoken native language globally, with about 500 million speakers. 26 Thus, these findings are relevant not only for Spanish speakers but also for other non-English-speaking populations. All strategies improved short-term recognition of stroke symptoms and risk factors, especially those in the FAST acronym. ICTUS 911 showed the most significant improvement in both adequate stroke knowledge (31%) and appropriate intended action (29%), suggesting it may be the most effective approach.
Recognizing stroke symptoms is key to reducing prehospital delays. Other contributors include symptom progression, home onset, and use of private transport. 27 In LMICs and non-English-speaking communities, cultural factors, such as hoping symptoms resolve on their own, reluctance to travel 17 or attending facilities unequipped for stroke care, 16 may further delay care.
Educational tools for stroke awareness must go beyond symptom recognition, as proposed recently as “Stroke action awareness”; 28 must also create an instinctive connection between identifying stroke symptoms and calling emergency services. In this regard, the FAST acronym, while effective in English-speaking populations, has several limitations when adapted to other languages: (1) it is English-dependent, it may lose the meaning of fast after translation, (2) it does not include the word “stroke,” and (3) it lacks a direct link to an emergency phone number. These shortcomings reduce its intuitive effectiveness in non-English-speaking contexts. In contrast, tools like ICTUS 911 integrate critical elements: (1) the word ictus (stroke), (2) clear symptom recognition pointers with a single number, and (3) a direct link to an emergency number. This integration improves knowledge and facilitates action, potentially creating a “knee-jerk” response to call emergency services when stroke symptoms are suspected.
The success of similar tools in other linguistic contexts supports this approach. For example, Stroke 120 has significantly improved stroke recognition and emergency medical services activation in Chinese-speaking populations. 29 Likewise, Stroke 112 has been proposed for regions where 112 is the emergency phone number, demonstrating its adaptability in different language environments and potential effectiveness. 30
We believe that adopting a comparable approach in Spanish-speaking populations has the potential to replicate these successes. Strategies such as ICTUS 911, which directly embed the condition’s name, symptom recognition, and emergency number, offer a clear pathway to increasing stroke knowledge and ensuring immediate and appropriate action when symptoms arise.
These findings are particularly relevant in the broader effort to reduce prehospital delays in stroke management, a critical barrier to timely reperfusion therapy.27,31,32 This trial provides evidence that culturally and linguistically adapted strategies can achieve similar benefits in Spanish-speaking populations to those of the FAST acronym in English-speaking countries. By measuring each strategy’s effectiveness in several desirable outcomes, this study adds knowledge to support implementing focused public health initiatives to mitigate delays and improve stroke outcomes globally, particularly in LMICs.
Several methodological constraints must be considered when interpreting these findings. First, recruiting participants from public spaces might have introduced selection bias, as individuals present in these locations may be more socially engaged or have higher baseline health awareness than the general population. This could lead to an overestimation of the intervention’s impact, particularly when considering underserved or rural populations who may have lower exposure to health education and reduced access to emergency services. As such, caution is warranted when generalizing these findings to less accessible or more socioeconomically vulnerable groups. Moreover, although differences in stroke knowledge at baseline were not statistically significant between included and lost participants, the trend toward lower socioeconomic status (housing type) among those lost to follow-up suggests possible sample bias, which may limit the generalizability of the findings to more disadvantaged populations. Second, self-reported measures, such as the SAQ, may have been influenced by recall or social desirability bias. In addition, the short follow-up period limits the ability to assess the long-term retention of knowledge and sustained behavior change. Finally, while the interventions were tested independently, real-world applications might involve competing or overlapping health campaigns, which were not accounted for in this study. The non-significance among all the strategies could be due to small samples with multiple tools. The relatively small improvement in the secondary outcome could be due to short or simple educational efforts. The education and educational delivery methods could potentially enhance the effectiveness.
Finally, as the study was conducted in two urban locations in Mexico where 911 is the standard emergency number, generalizability to other Spanish-speaking countries, particularly those with different emergency systems or distinct emergency telephone numbers, may be limited.
Therefore, future research should explore the scalability and sustainability of these interventions in diverse settings, including rural and underserved communities where stroke awareness is even lower. 14 In addition, longitudinal studies are needed to evaluate the long-term impact of these strategies on stroke awareness and patient outcomes. Finally, adapting and testing these strategies in other languages and cultural contexts could extend their global applicability and contribute to reducing stroke-related disparities worldwide.
This study demonstrates that educational strategies targeting Spanish-speaking populations can modestly improve stroke symptom recognition and appropriate response actions. While the primary outcome did not show significant differences between strategies, ICTUS 911 yielded the largest short-term gains in adequate stroke knowledge and intended action among the five groups. This supports its adoption as a leading strategy for Spanish-speaking populations, although further studies should confirm long-term and real-world effectiveness.
Supplemental Material
sj-docx-2-wso-10.1177_17474930251378229 – Supplemental material for Efficacy of five strategies to improve stroke action awareness in Spanish-speaking adults: A randomized comparison
Supplemental material, sj-docx-2-wso-10.1177_17474930251378229 for Efficacy of five strategies to improve stroke action awareness in Spanish-speaking adults: A randomized comparison by Juan Manuel Marquez-Romero, Karen Itzel Sánchez-Ramírez, Carlos David Pérez-Malagón, Jannett Padilla-López, Gary A Ford, Jing Zhao and Renyu Liu in International Journal of Stroke
Supplemental Material
sj-docx-3-wso-10.1177_17474930251378229 – Supplemental material for Efficacy of five strategies to improve stroke action awareness in Spanish-speaking adults: A randomized comparison
Supplemental material, sj-docx-3-wso-10.1177_17474930251378229 for Efficacy of five strategies to improve stroke action awareness in Spanish-speaking adults: A randomized comparison by Juan Manuel Marquez-Romero, Karen Itzel Sánchez-Ramírez, Carlos David Pérez-Malagón, Jannett Padilla-López, Gary A Ford, Jing Zhao and Renyu Liu in International Journal of Stroke
Supplemental Material
sj-tiff-1-wso-10.1177_17474930251378229 – Supplemental material for Efficacy of five strategies to improve stroke action awareness in Spanish-speaking adults: A randomized comparison
Supplemental material, sj-tiff-1-wso-10.1177_17474930251378229 for Efficacy of five strategies to improve stroke action awareness in Spanish-speaking adults: A randomized comparison by Juan Manuel Marquez-Romero, Karen Itzel Sánchez-Ramírez, Carlos David Pérez-Malagón, Jannett Padilla-López, Gary A Ford, Jing Zhao and Renyu Liu in International Journal of Stroke
Footnotes
Acknowledgements
None.
Author contributions
Study conception and design: J.M.M.-R., R.L.; data collection: J.M.M.-R., K.I.S.-R., C.D.P.-M., J.P.-L.; analysis and interpretation of results: J.M.M.-R., R.L., G.A.F., J.Z.; draft manuscript preparation: J.M.M.-R. All authors reviewed the results and approved the final version of the manuscript.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study received funding from the Convocatoria 2025 para el desarrollo o continuidad de protocolos de investigación en salud sobre Temas Prioritarios del Instituto Mexicano del Seguro Social.
Ethical approval and informed consent statements
This study was approved by the Institutional Review Board CLI-101 of the IMSS (Mexico), reference R-2024-101-110. All participants provided written informed consent, and their confidentiality was safeguarded in compliance with the Declaration of Helsinki. Participation was voluntary.
Data availability statement
Data from this study will be made available to the corresponding and first author upon reasonable request.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.