
Abstract
Background:
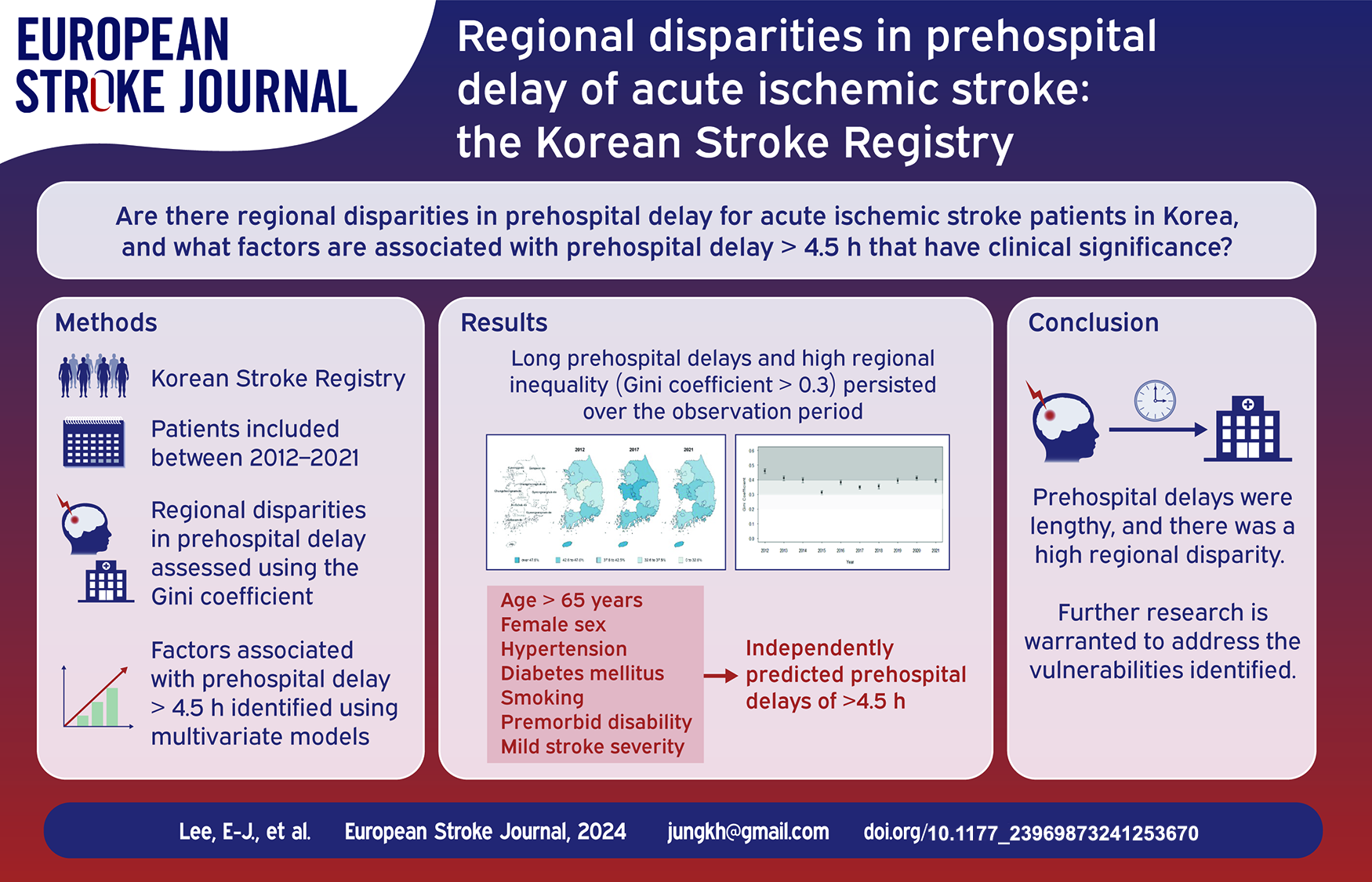
Late hospital arrival keeps patients with stroke from receiving recanalization therapy and is associated with poor outcomes. This study used a nationwide acute stroke registry to investigate the trends and regional disparities in prehospital delay and analyze the significant factors associated with late arrivals.
Methods:
Patients with acute ischemic stroke or transient ischemic attack between January 2012 and December 2021 were included. The prehospital delay was identified, and its regional disparity was evaluated using the Gini coefficient for nine administrative regions. Multivariate models were used to identify factors significantly associated with prehospital delays of >4.5 h.
Results:
A total of 144,014 patients from 61 hospitals were included. The median prehospital delay was 460 min (interquartile range, 116–1912), and only 36.8% of patients arrived at hospitals within 4.5 h. Long prehospital delays and high regional inequality (Gini coefficient > 0.3) persisted throughout the observation period. After adjusting for confounders, age > 65 years old (adjusted odds ratio [aOR] = 1.23; 95% confidence interval [CI], 1.19–1.27), female sex (aOR = 1.09; 95% CI, 1.05–1.13), hypertension (aOR = 1.12; 95% CI, 1.08–1.16), diabetes mellitus (aOR = 1.38; 95% CI, 1.33–1.43), smoking (aOR = 1.15, 95% CI, 1.11–1.20), premorbid disability (aOR = 1.44; 95% CI, 1.37–1.52), and mild stroke severity (aOR = 1.55; 95% CI, 1.50–1.61) were found to independently predict prehospital delays of >4.5 h.
Conclusion:
Prehospital delays were lengthy and had not improved in Korea, and there was a high regional disparity. To overcome these inequalities, a deeper understanding of regional characteristics and further research is warranted to address the vulnerabilities identified.
Introduction
Swift recovery of blood supply to the brain by intravenous thrombolysis (IVT) or mechanical thrombectomy (MT) is critical for neurological recovery after acute ischemic stroke (AIS). 1 Patients with AIS generally need to present to the hospital within 4.5 h of symptom onset to be eligible for IVT, and even if selected using automated perfusion imaging, within 9 h.2,3 Previous studies have suggested that the leading cause for the low IVT rate is late arrivals at the hospital.
In South Korea, regional inequality in healthcare resources is an important social and political issue. 4 Regional disparities in ambulance utilization rates, IVT application of patients with stroke, and age-standardized stroke mortality have been observed. 5 Regional disparities in prehospital delay have been noted as a core factor associated with differing stroke outcomes. 6 Diverse factors, including patient-specific and healthcare system factors, are associated with the late arrival of patients with AIS. 7 Identifying the disparity and clarifying its reasons is the first step to resolving the regional gap and improving stroke outcomes. However, previous studies on prehospital delay in patients with AIS in Korea remain at the single-center or area level.8,9
Thus, this study aimed to investigate the trends and regional disparities in prehospital delay based on the nationwide acute stroke registry, the Korean Stroke Registry (KSR). 10 Furthermore, we explored whether hospital arrival of >4.5 h was associated with unfavorable outcomes for patients with stroke and analyzed the significant factors associated with a late arrival of >4.5 h.
Methods
Data source
The KSR is a representative, prospective, and multicenter stroke registry in Korea.11,12 As of 2022, 81 hospitals across the nation participated in the KSR. The KSR covers hospitals in seven special metropolitan cities and nine provinces in South Korea. All primary stroke centers and thrombectomy-capable centers accredited by the Korean Stroke Society participated in the KSR, with a steady enrollment of more than 2000 patients with acute stroke per month and approximately 25,000 patients per year. In addition, 10 of the 13 regional cerebrocardiovascular centers certified by the Korean government participated in the KSR (Supplemental Table S1 and S2). 13 As hospitals of various sizes across the country participated in the KSR, it would be useful to understand the regional disparity. Patients who were diagnosed with stroke or transient ischemic attack (TIA) within 7 days of symptom onset were registered online through the website (www.strokedb.or.kr). All participating centers in the KSR were required to collect data on demographics, vascular risk factors, and time of stroke onset and type (clear or unclear onset), as well as to establish quality-of-care indicators, including prehospital delay, initial stroke severity evaluated by the National Institute of Health Stroke Scale (NIHSS) score, and modified Rankin scale (mRS) score before and after the incident stroke. Additional details of the KSR are described elsewhere. 12 Furthermore, as an indicator of the level of infrastructure in a region that is relevant to prehospital delays, we examined the number of emergency ambulances per 100,000 population per region for each year from the emergency statistics of the Korean government (Supplemental Table S3). 14 The procedure of this registry and the current study design were approved by the Institutional Review Board (IRB) of Seoul National University Hospital, which represented the involved hospitals (IRB No. H-1009-062-332 and H-2206-172-1336).
Study sample
Of the 81 KSR-participating centers, hospitals that had enrolled patients for at least 1 year and continued to participate in the monitoring and auditing process of the database till 2021 were selected for analysis. A total of 61 hospitals across the nine administrative districts in South Korea were included (Supplemental Table S1 and S2). Each hospital had different time points for the commencement of registration in the observation period. This study identified patients aged ⩾20 years with a diagnosis of AIS or TIA in the KSR between January 1, 2012, and December 31, 2021. Participants with missing data on age, sex, initial stroke severity, stroke onset time, or hospital arrival time were excluded.
Outcome measures
The prehospital delay was computed from the stroke symptom onset time (first abnormal time: the time when the symptoms were first noticed by the patient or observed by a witness) to the time of arrival at the hospital. If no eyewitnesses were present or if the time of symptom onset was unclear, the time from the last known symptom-free to hospital arrival was used. A 4.5 h hospital arrival rate was defined as the number of patients with prehospital delays of <4.5 h, divided by the total number of patients with stroke or TIA.
Regional disparity
Regional disparities in prehospital delay were assessed using data from nine administrative regions of South Korea. A Gini coefficient was utilized to calculate the inequality among the regions. 15 The Gini coefficient for regional disparities for each year was calculated and compared from 2012 to 2021 to determine whether regional disparities in prehospital delay in South Korea changed over the observation period. The Gini coefficient is a variable that has been widely used in previous studies to identify disparities in economics (personal income) and healthcare variables (treatment usage).16,17 Furthermore, previous studies have effectively demonstrated regional disparities in cerebrovascular disease management using the Gini coefficient.18,19 The Gini coefficient ranges from 0 (perfect equality) to 1 (perfect inequality) and is categorized as low (<0.2), moderate (⩾0.2, <0.3), high (⩾03, <0.4), or extreme inequality (⩾0.4). 18
Covariates
The factors associated with favorable stroke outcomes (mRS score at discharge ⩽2) were analyzed among the patients who were not disabled prior to the stroke. No disability before the onset of stroke was defined as a previous mRS score of ⩽1 recorded on the KSR. Old Age (>65 years), sex, initial stroke severity, late arrival at the hospital (>4.5 h), comorbidities (previous history of stroke or TIA, hypertension, coronary artery disease, diabetes mellitus, dyslipidemia, smoking, atrial fibrillation) and use of recanalization treatment were included in the analysis. In addition, old age (>65 years), sex, comorbidities, current intake of medications (anticoagulants, antiplatelets, antihypertensive agents, and statins), initial stroke severity, admission routes (via the emergency department, outpatient clinic), number of ambulances per 100,000 people in each region, and presence of a disability were included as potential characteristics that could affect the prehospital delay of >4.5 h.
Statistical analysis
Categorical variables are expressed as frequencies with percentages, and continuous variables are represented as means with standard deviations or medians with interquartile ranges (IQRs). The distribution of prehospital delays did not follow a standard normal distribution. Therefore, median and IQR were used to represent the prehospital delay in each region for each year. A rate of 4.5 h hospital arrivals was calculated for each region by year. We represented geographic variations in prehospital delay across the nation using a choropleth map and calculated Gini coefficients to identify regional inequalities between 2012 and 2021 in the nine regions. Furthermore, the 95% confidence intervals (CIs) of Gini coefficients were estimated using 2000-bootstrapping sampling. Subsequently, an analysis to identify any differences between the two Gini coefficients was conducted using the bootstrapping method. If the 95% CI did not contain zero, then the two Gini coefficients indicated statistically significant differences. Univariate and multivariate analyses were conducted to determine whether presenting to the hospital after 4.5 h was independently and negatively associated with functional independence at discharge after acute stroke. The dependent variable was functional independence at discharge, defined as an mRS score of ⩽2. Covariates included age, sex, moderate to severe stroke, comorbidities (previous stroke or TIA, hypertension, coronary artery disease, diabetes mellitus, dyslipidaemia, smoking, atrial fibrillation), and reperfusion therapy [IVT or MT]. Significant variables (p < 0.1 in the univariate analysis) were included as covariates in the multivariate analysis. In addition, univariate and multivariate analyses were performed to identify factors independently associated with a prehospital delay of >4.5 h. Differences in prehospital delay according to stroke severity were also examined. All analyses were performed using SAS (version 9.4; SAS Institute, Inc.) and R version 4.2.2 (https://www.R-project.org). A two-sided p-value of <0.05 was considered statistically significant.
Results
Baseline characteristics of the patients
A total of 155,367 registered patients from 61 hospitals were identified in the KSR between 2012 and 2021. Of these, 3305 patients diagnosed with hemorrhagic stroke, 3135 patients with missing data on age, sex, initial severity, and time of stroke onset or hospital arrival, as well as 4913 patients with in-hospital stroke, were excluded. Finally, a total of 144,014 patients with AIS or TIA were included (Supplemental Figure S1). The patient characteristics are summarized in Tables 1 and 2. The mean age was 68.3 (±12.3) years. Among all patients, 59.1% were men, and 31.0% had unclear stroke onset. During the last 10 years, 8.2% of all patients with AIS underwent IVT, and 4.6% received MT. IVT rates have declined since 2014 (9.2%), reaching 7.8% in 2021. Meanwhile, MT rates have increased, reaching 5.6% in 2018, albeit a slight decrease in recent years. The median prehospital delay in all regions of South Korea throughout the observation period was 460 min (IQR, 116–1912), and the minimum time was 429 min in 2016 (IQR, 109–1868), the trend of the change was not statistically significant (p-value for trend = 0.167) (Supplemental Figure S2).
Baseline characteristics of the total participants.
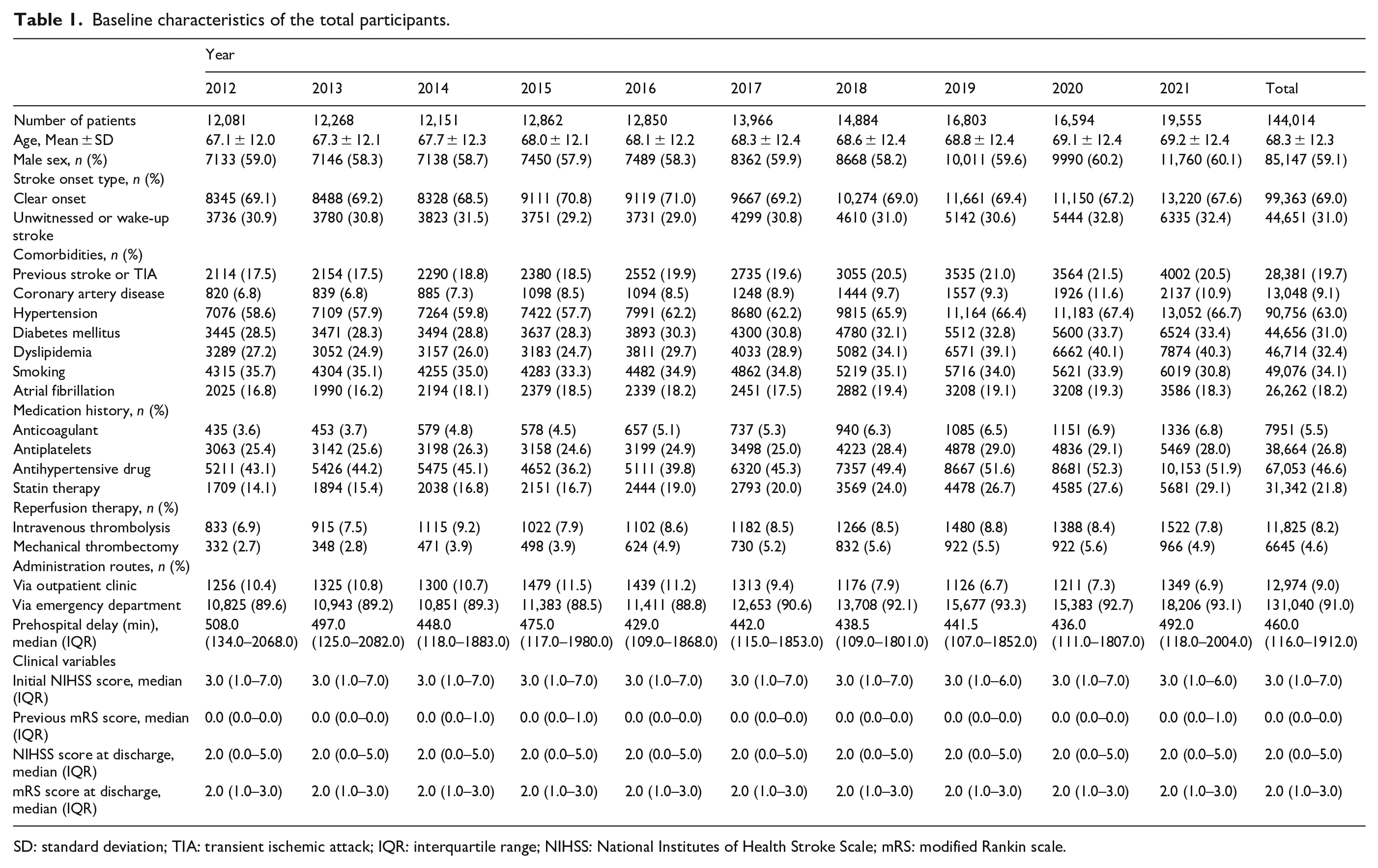
SD: standard deviation; TIA: transient ischemic attack; IQR: interquartile range; NIHSS: National Institutes of Health Stroke Scale; mRS: modified Rankin scale.
Baseline characteristics according to geographical region.
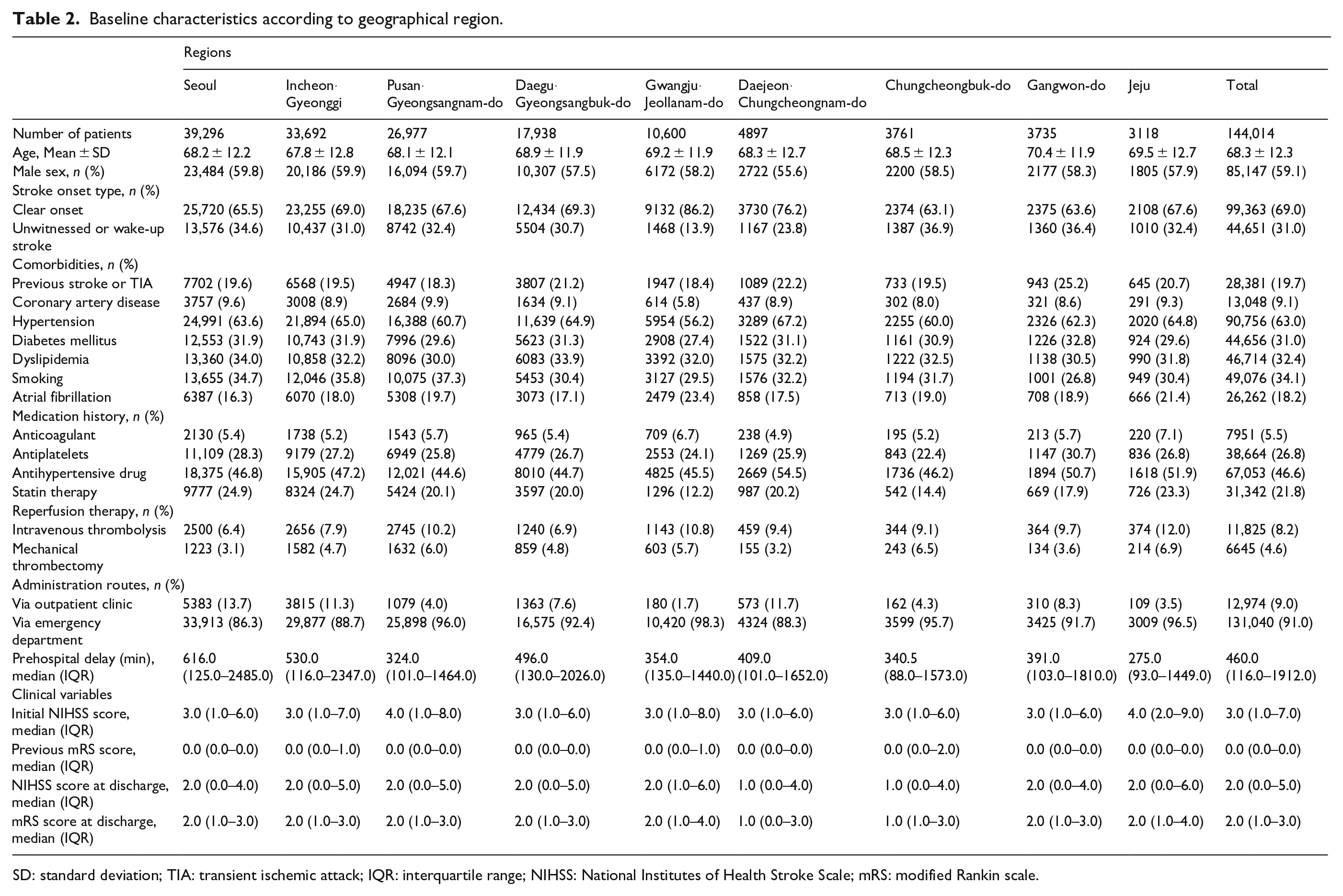
SD: standard deviation; TIA: transient ischemic attack; IQR: interquartile range; NIHSS: National Institutes of Health Stroke Scale; mRS: modified Rankin scale.
Regional disparity in prehospital delay
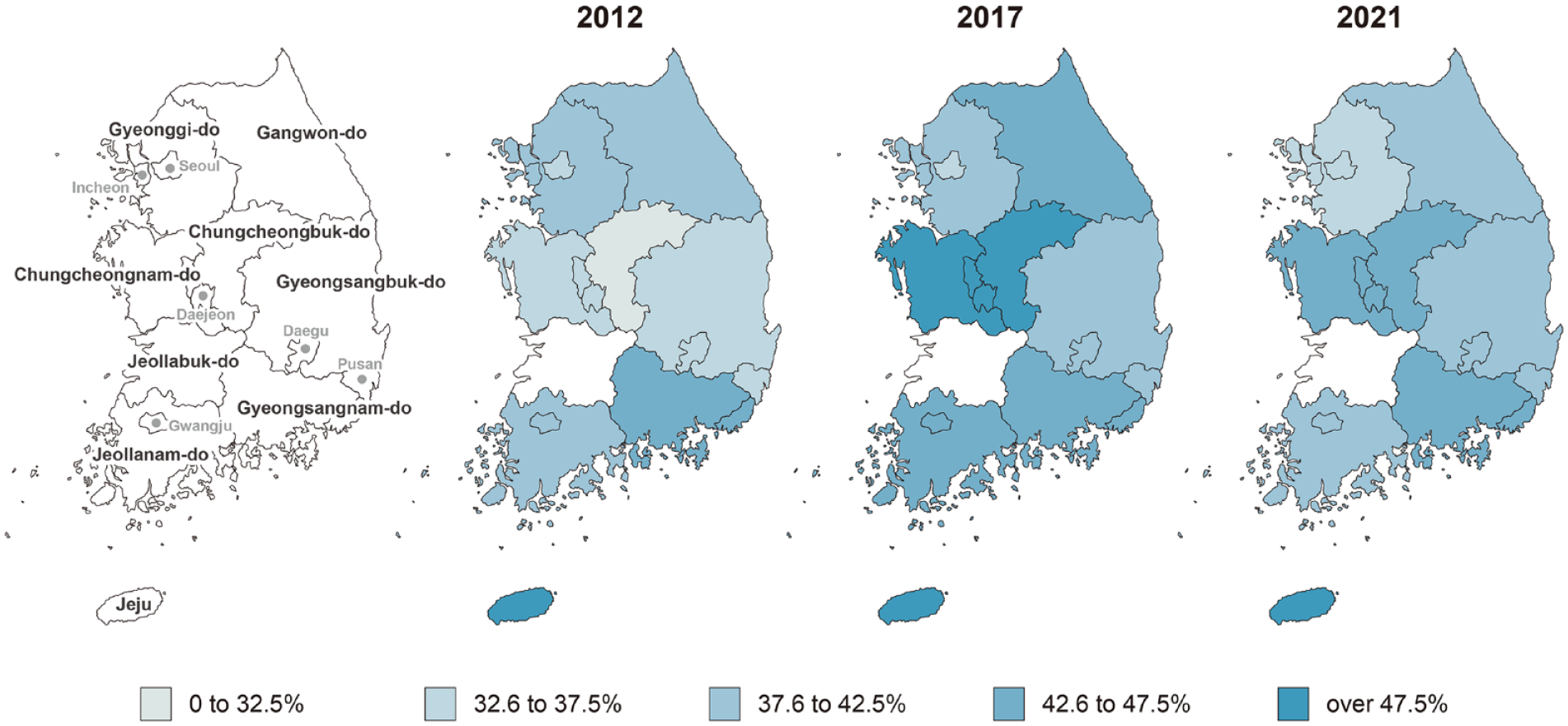
During the observation period, substantial regional differences existed in the prehospital delay across the country (Table 3 and Supplemental Table S4). In 2021, the most recent year for which data were available, the difference between the shortest (Jeju, median 316 min) and longest prehospital delays (Seoul, median 646 min) was over two-fold. The Seoul metropolitan area tended to have longer prehospital delays than other regions. The rate of people reaching the hospital within 4.5 h for each region was calculated and plotted on a map (Figure 1). The rates of patients with a prehospital delay of ⩽4.5 h were also observed to vary significantly by region, ranging from approximately 28.6% to 55.7% (Supplemental Table S4). The overall regional disparity in the prehospital delay was quantified using the Gini coefficient, which suggested high inequality (>0.3) (Figure 2). Although small differences exist between years, no significant changes were observed between the Gini coefficients at any time point when statistical tests using the bootstrapping method were performed.
Yearly prehospital delay in each region (min, median [IQR]).
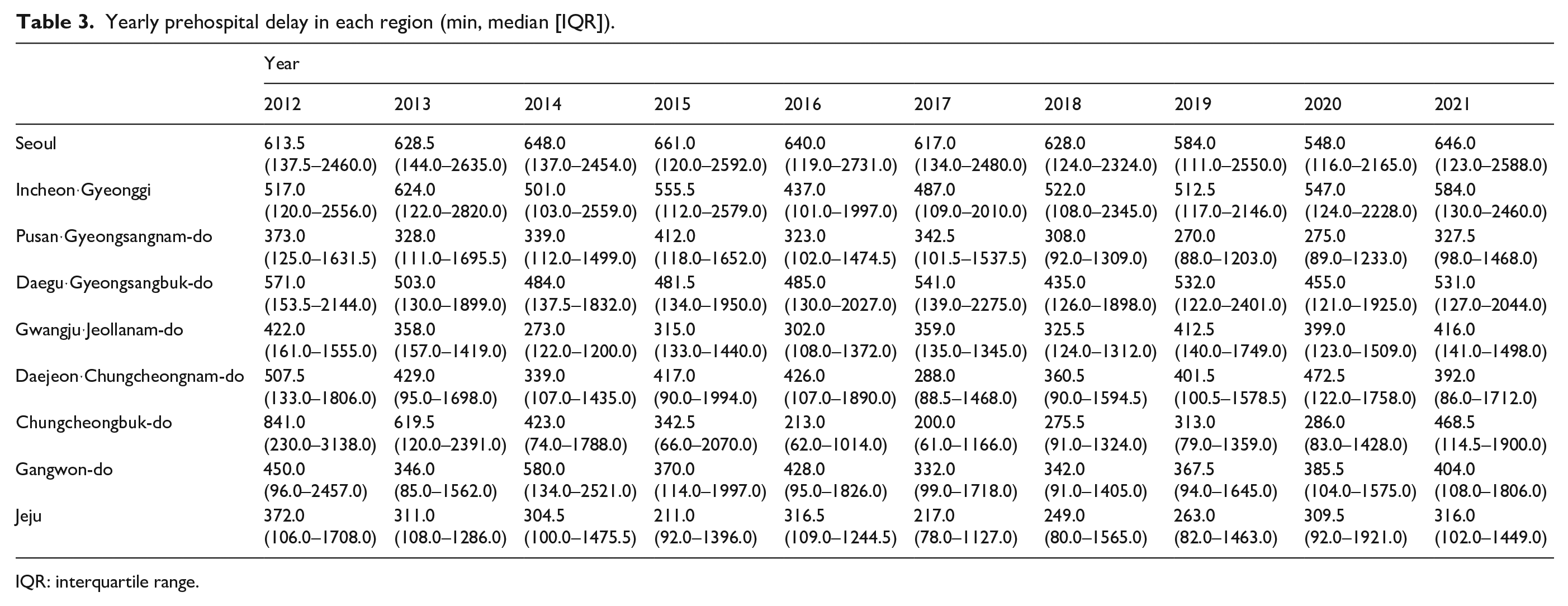
IQR: interquartile range.
Rate of prehospital delay of <4.5 h by region.
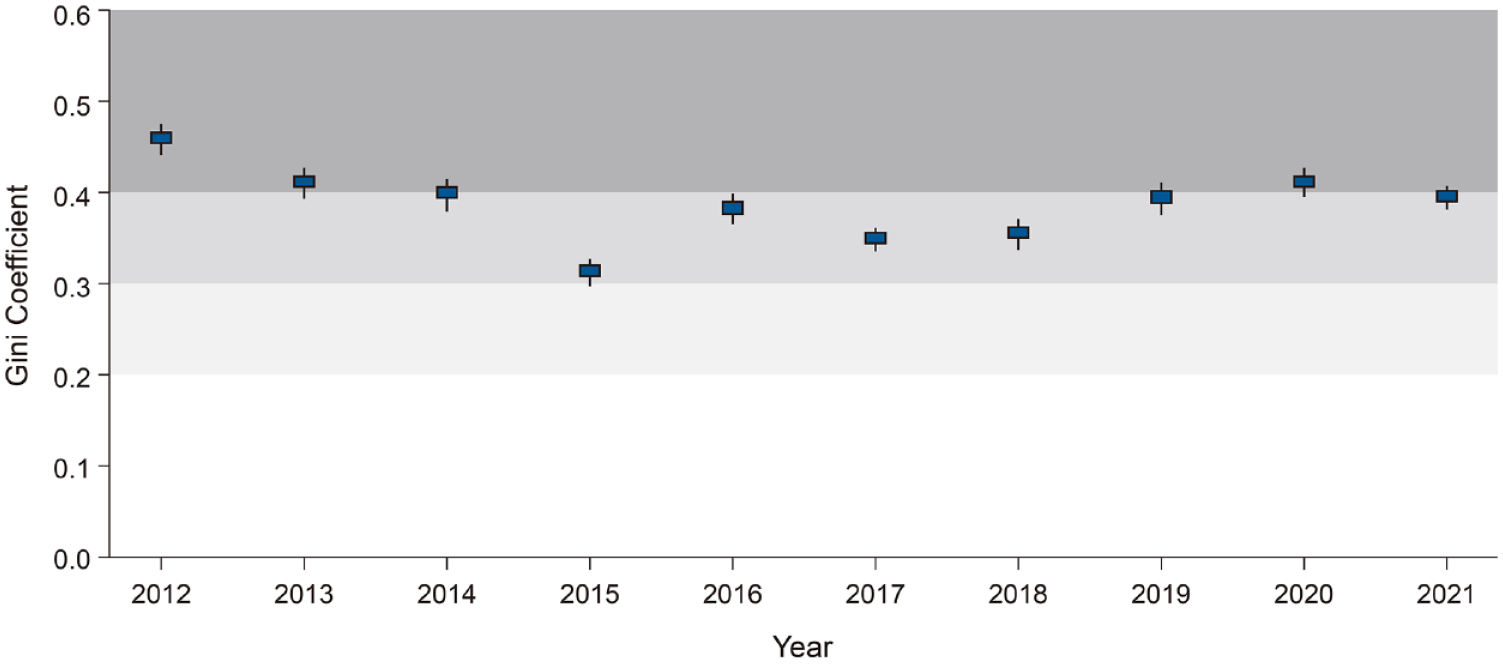
Regional disparity in prehospital delay.
Late arrival of >4.5 has an independent predictor of functional dependence at discharge
To investigate whether presenting to the hospital after 4.5 h was associated with functional independence (mRS ⩽ 2) after stroke, only patients (n = 82,461) with no disability (mRS ⩽ 1) prior to the index stroke were included. As presented in Figure 3(a), a multivariate analysis showed that patients with a prehospital delay of >4.5 h were less likely to have functional independence at discharge (adjusted odds ratio [aOR] = 0.65; 95% CI, 0.62–0.68; p < 0.001).
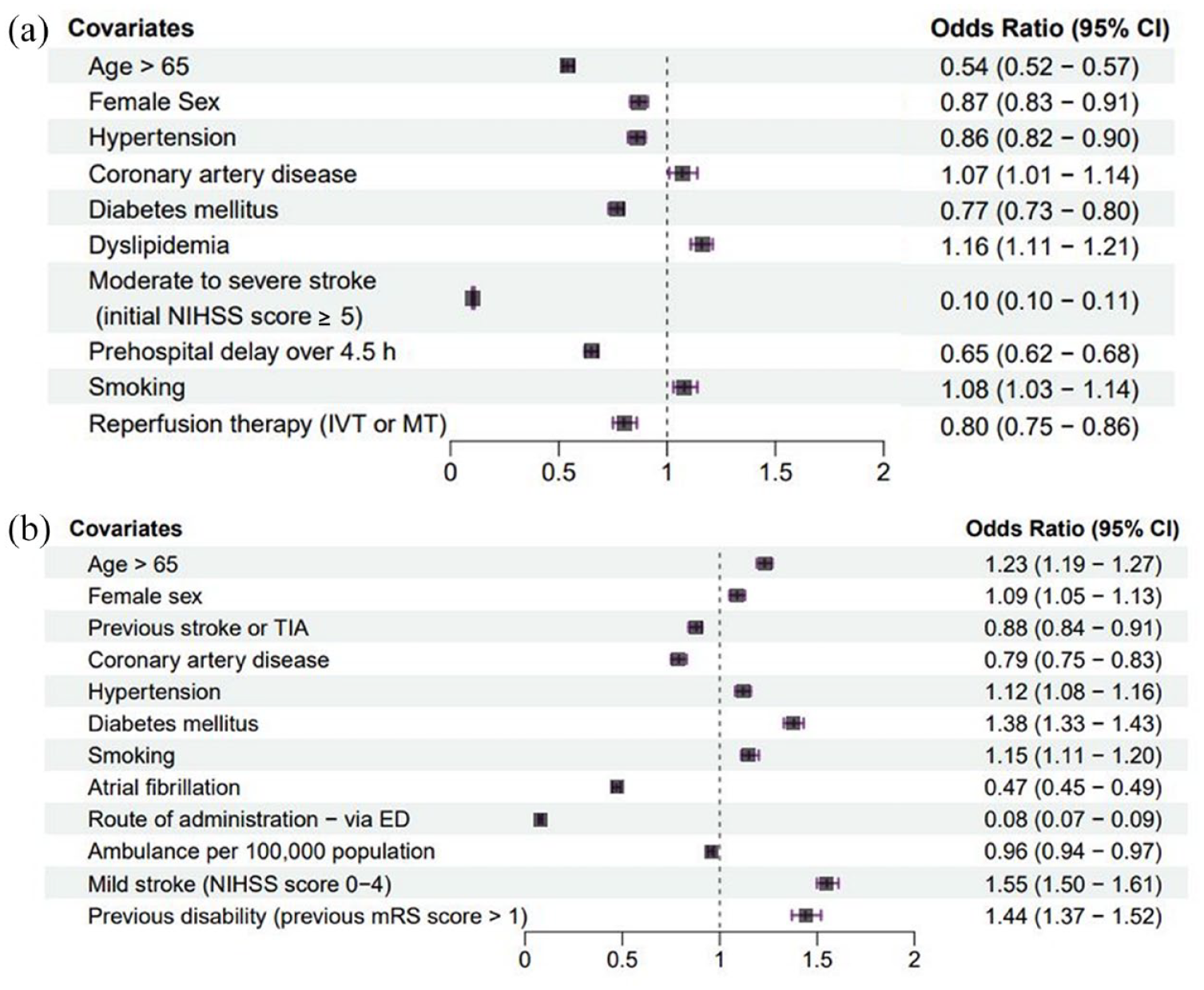
Forest plot showing the factors associated with functional independence after incident stroke (a) and prehospital delay of >4.5 h (b). CI: confidence interval; TIA: transient ischemic attack; ED: emergency department; NIHSS: National Institute of Health Stroke Scale; mRS: modified Rankin scale, TIA: transient ischemic attack; IVT: intravenous thrombolysis; MT: mechanical thrombectomy.
Factors associated with prehospital delay >4.5 h
To identify the factors that cause any delays in arriving at the hospital after becoming aware of their symptoms, we restricted our analysis to patients with clear onset stroke (n = 99,075). Of these, only 36.8% of patients (n = 36,459) were admitted to the hospital within 4.5 h. The results of the multivariate analysis of the factors associated with a prehospital delay of >4.5 h are presented in Figure 3(b). Age over 65 years old (aOR = 1.23; 95% CI, 1.19–1.27; p < 0.001), female sex (aOR = 1.09; 95% CI, 1.05–1.13; p < 0.001), hypertension (aOR = 1.12; 95% CI, 1.08–1.16; p < 0.001), diabetes mellitus (aOR = 1.38; 95% CI, 1.33–1.43; p < 0.001), smoking (aOR = 1.15; 95% CI, 1.11–1.20; p < 0.001), disability prior to incident stroke (aOR = 1.44; 95% CI, 1.37–1.52; p < 0.001), and mild stroke severity (NIHSS score < 5) (aOR = 1.55; 95% CI, 1.50–1.61; p < 0.001) independently predicted a prehospital delay >4.5 h. On the other hand, a history of previous stroke or TIA (aOR = 0.88; 95% CI 0.84–0.91; p < 0.001), coronary artery disease (aOR = 0.79; 95% CI 0.75–0.83; p < 0.001), atrial fibrillation (aOR = 0.47; 95% CI 0.45–0.49; p < 0.001), administration via the emergency department (aOR = 0.08; 95% CI 0.07–0.09; p < 0.001), and the number of ambulances available per 100,000 population (aOR = 0.96; 95% CI 0.94–0.97; p < 0.001) were negatively and significantly associated with prehospital delays longer than 4.5 h.
Discussion
Based on a nationwide stroke registry, this study demonstrated trends in regional disparities in prehospital delay from 2012 to 2021. As assessed using the Gini coefficient, high inequalities persisted with a low proportion (36.8%) of patients visiting the hospital within 4.5 h. Furthermore, factors associated with a prehospital delay of >4.5 h included old age, female sex, the presence of vascular risk factors, and mild stroke severity.
We believe that our study is of great value as it is based on a nationally representative stroke registry, examines trends in stroke care over the last 10 years, and confirms the existence of geographic inequalities in prehospital delay among the nine administrative regions of Korea. During the observation period, prehospital delays were long, with a median of 460 min, and while a gradual decrease was observed, the change was not statistically significant. In other words, there was no improvement. Notably, an increase in prehospital delay was observed in 2021, with a median of 492 min, as compared to 2020 (median of 436 min), suggesting a possible impact of COVID-19 (Supplemental Figure S2). Further research is needed on the improvement or worsening of prehospital delay following the COVID-19 era.
Regional disparities have not improved either; recent studies have reported population density, traffic congestion, and pathways to hospital as key factors associated with regional differences in prehospital delay.20–22 Interestingly, prehospital delay was observed to be longer in large metropolitan areas such as Seoul. First, we found that Seoul has the lowest number of ambulances (1.9 as of 2021) per 100,000 population, which may be the reason for the low utilization of emergency medical vehicles. Therefore, patients in metropolitan areas most likely use their own vehicles to reach the hospital at a higher rate in Korea. 23 As a result, prehospital delays can be prolonged due to traffic congestion associated with high population density. In addition, if the patient goes to the hospital on their own, they may not be able to get directly to a stroke center where they can receive proper diagnosis and treatment. Based on this hypothesis, the results of the study show a significant difference in prehospital delay (646 vs 316 min in 2021), with 13.7% of cases in Seoul being administered through an outpatient clinic, as compared to only 3.5% in Jeju, which has 4.7 ambulances per 100,000 people as of 2021 (Table 2 and Supplemental Table S3). Further research is needed to investigate the use of emergency vehicles by patients after the onset of stroke, the route, and the time delay to the hospital.
Moreover, an overall reduction in prehospital delay is the most vital aspect for resolving regional disparities. A sex disparity was present in prehospital delay; women tended to arrive at hospitals later. Previous research indicated that women are generally older and more likely to live alone at the stroke onset. 24 Being alone at the time of symptom onset has been associated with late visits. 25 About 70% of the senior citizens living alone in Korea are women. 26 In this study, older age was also found to be significantly correlated with late arrival. Older adults have limited mobility, and age-related frailty may interfere with the early recognition of new neurological symptoms. Functional impairment prior to stroke onset, estimated using the mRS score, was also associated with late arrival at the hospital. Due to disabilities, the process of visiting the hospital can be lengthy.27,28 However, reperfusion therapy should be considered even in the presence of a premorbid disability. 29 Our study highlights the need for a policy to ensure that underprivileged patients arrive at the hospital sooner after AIS.
Another remarkable finding of our study is the need for education to improve awareness regarding the symptoms and treatment of stroke. Similar to previous studies, the milder symptom was associated with later visits.30,31 However, even if initial stroke symptoms are mild, patients can be left with disabilities if not treated appropriately.32,33 In addition, patients with vascular risk factors, except atrial fibrillation, all visited the hospital late. Previous reports have shown that only having a stroke risk factor does not increase stroke knowledge.34,35 In contrast, patients who experienced cerebro-cardiovascular disease tended to present earlier. This was inferred to result from their awareness of stroke. In addition, it is possible that the initial symptoms were misinterpreted by the first healthcare provider who encountered the patient as something other than a stroke. 36 Therefore, further research is required to identify ways of increasing stroke awareness in vulnerable populations and healthcare providers.
Our study had a few limitations. Factors such as the route and mode of transportation used by patients to get to the hospital from the area at which symptoms occurred, including ambulance use, were not routinely captured in the registry used. When it comes to inter-hospital transfer, the time taken for patients to arrive at the first hospital was impossible to determine, especially if the patient was transferred from another hospital. However, the time taken for patients to receive acute stroke care could be determined, as patients likely would have been transferred without receiving any special treatment at the first hospital due to the unique circumstances of Korea. This is an important healthcare issue in Korea that warrants further research. Second, although excluded from the analysis of factors associated with prehospital delay (>4.5 h), the analysis of regional disparities included patients with unclear onset times, which may have overestimated the prehospital delay. Third, the catchment area of each hospital and the number of populations it serves may play a role in regional differences in prehospital delay. However, we could not account for this because the information currently collected in the KSR does not allow this. Further research is required to account for this if we can collect the necessary information. Finally, KSR-participating hospitals are certified stroke centers and may not reflect the situation in all regions and hospitals in Korea. Further, there was one Province (North Jeolla) where it was impossible to depict the trend since no hospitals in this area were participating in the KSR. Nonetheless, the KSR includes hospitals of varying sizes across the country and is, therefore, useful for examining regional disparities.
Conclusion
This retrospective analysis of a nationwide representative stroke registry found that prehospital delays were long with no improvement over the years and that high regional disparities in the same exist in Korea. Overall reduction of prehospital delays combined with a targeted regional approach would be the best strategy to alleviate the burden of stroke. A deeper understanding of regional characteristics is required to overcome the inequalities between regions, and further research is warranted to address the vulnerabilities identified in this study.
Supplemental Material
sj-docx-1-eso-10.1177_23969873241253670 – Supplemental material for Regional Disparities in Prehospital Delay of Acute Ischemic Stroke: The Korean Stroke Registry
Supplemental material, sj-docx-1-eso-10.1177_23969873241253670 for Regional Disparities in Prehospital Delay of Acute Ischemic Stroke: The Korean Stroke Registry by Eung-Joon Lee, Han-Yeong Jeong, Jayoun Kim, Nan Hee Park, Min Kyoung Kang, Dongwhane Lee, Jinkwon Kim, Yo Han Jung, Sungwook Yu, Wook-Joo Kim, Han-Jin Cho, Kyungbok Lee, Tai Hwan Park, Mi Sun Oh, Ji Sung Lee, Joon-Tae Kim, Byung-Woo Yoon, Jong-Moo Park, Hee-Joon Bae and Keun-Hwa Jung in European Stroke Journal
Supplemental Material
sj-docx-2-eso-10.1177_23969873241253670 – Supplemental material for Regional Disparities in Prehospital Delay of Acute Ischemic Stroke: The Korean Stroke Registry
Supplemental material, sj-docx-2-eso-10.1177_23969873241253670 for Regional Disparities in Prehospital Delay of Acute Ischemic Stroke: The Korean Stroke Registry by Eung-Joon Lee, Han-Yeong Jeong, Jayoun Kim, Nan Hee Park, Min Kyoung Kang, Dongwhane Lee, Jinkwon Kim, Yo Han Jung, Sungwook Yu, Wook-Joo Kim, Han-Jin Cho, Kyungbok Lee, Tai Hwan Park, Mi Sun Oh, Ji Sung Lee, Joon-Tae Kim, Byung-Woo Yoon, Jong-Moo Park, Hee-Joon Bae and Keun-Hwa Jung in European Stroke Journal
Footnotes
Acknowledgements
Not applicable
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by a grant (#2023-ER1006-00) from the Korea Disease Control and Prevention Agency.
Ethics approval
All procedures were in accordance with the Declaration of Helsinki and approved by the Ethical Committee of our University Hospital. The number of the approved ethical statement numbers are H-1009-062-332 and H-2206-172-1336.
Patient consent for publication
Not applicable.
Guarantor
Keun-Hwa Jung, MD, PhD
Contributorship
KJ, EL, and HJ designed the study. EL, JK, MKK, DL, JK, YHJ, SY, WK, HC, KBL, THP, MSO, JSL, JK, BY, JP, HB, and NHP performed the literature search and review of evidence before the study. EL and HJ collected the data under the supervision of KJ. EL, JK, and NHP analyzed the data. EL created the figures. All authors contributed to the interpretation of the results. All authors reviewed and approved the final version of the manuscript. The study was guaranteed by KJ, who had access to the data and made the final decision to publish.
Data availability statement
The data supporting this study’s findings are available from the corresponding author upon reasonable request.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.