
Abstract
Background:
Several randomized clinical trials have indicated that intensive blood pressure (BP) lowering is associated with worse outcomes, leaving the optimal BP targets following endovascular thrombectomy (EVT) uncertain.
Aims:
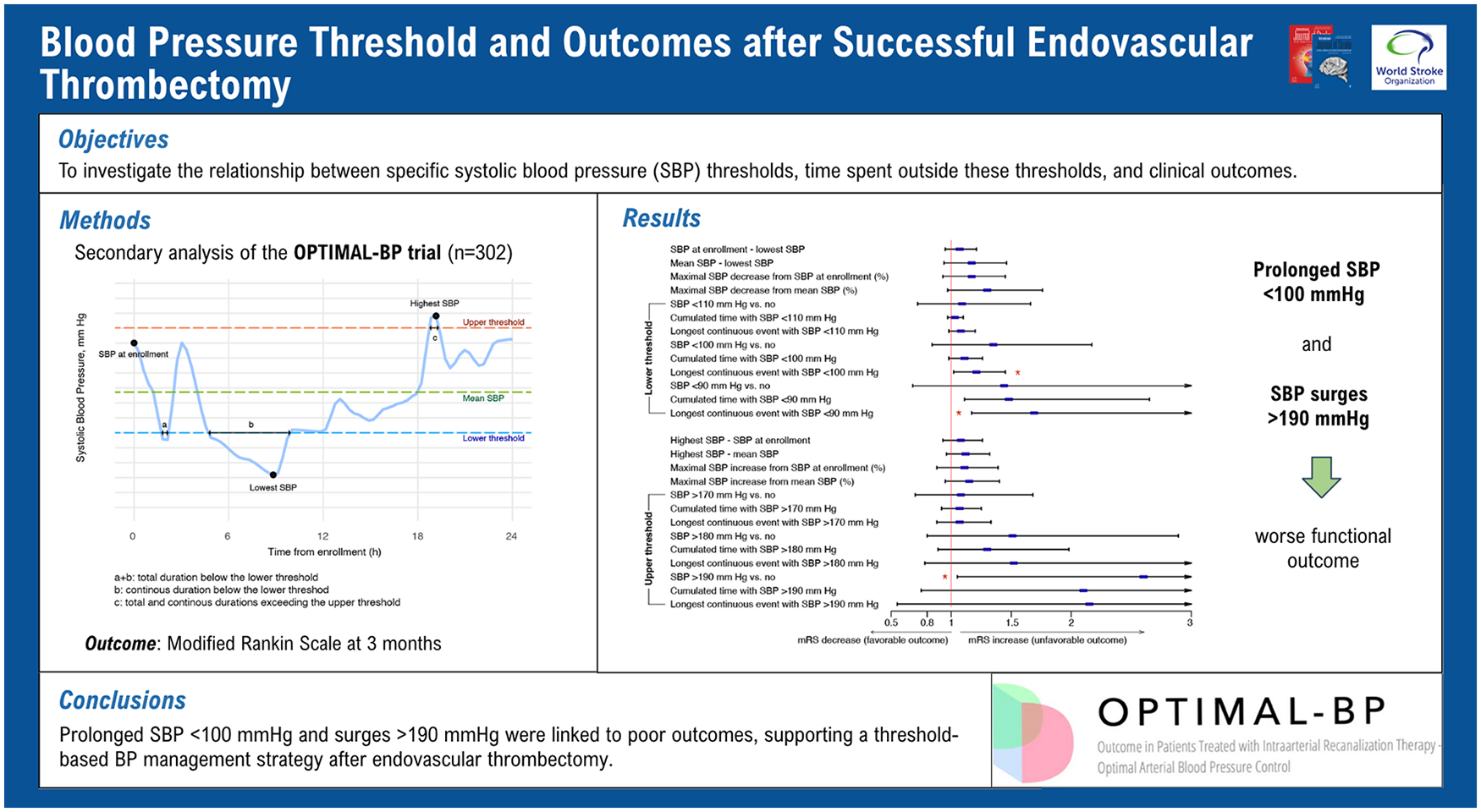
This study aimed to investigate the relationship between specific systolic BP (SBP) thresholds, time spent outside these thresholds, and clinical outcomes.
Methods:
This post hoc analysis of the Outcome in Patients Treated With Intra-Arterial Thrombectomy–Optimal Blood Pressure Control (OPTIMAL-BP) trial, included patients with successful EVT randomized to intensive (<140 mmHg) or conventional (140–180 mmHg) BP management. We analyzed SBP parameters, including mean, maximum, and minimum SBP during study period, as well as excursions beyond predefined SBP thresholds (<90, <100, <110, >170, >180, and >190 mmHg), and the cumulative and continuous durations of these excursions. Associations with 3 month modified Rankin Scale (mRS) and symptomatic intracerebral hemorrhage (sICH) were assessed using multivariable logistic and ordinal regression models.
Results:
A total of 302 patients (median 75 years; 180 [59.6%] men) were analyzed with 11,461 BP measurements recorded during the first 24 hours after EVT. Prolonged hypoperfusion (SBP below 100 mmHg for continuous duration) was associated with worse mRS score (adjusted OR [aOR] 1.21 per hour, 95% CI [1.02–1.45]; P = 0.030) and increased sICH risk (aOR 1.49 per hour, 95% CI [1.15–1.97]; P = 0.004). SBP surges above 190 mmHg were linked to mRS worsening (aOR 2.60, 95% CI [1.05–6.53]; P = 0.039), but upper threshold-related parameters were not significantly associated with sICH.
Conclusion:
Prolonged hypoperfusion below 100 mmHg and extreme surges above 190 mmHg, rather than specific SBP parameters, were associated with poor functional outcomes. These findings highlight the need for a threshold-based BP management approach post-EVT to minimize prolonged hypotension and excessive surges.
Get full access to this article
View all access options for this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.