
Abstract
Background:
An increased risk of femoral fractures after ischemic stroke (IS) and transient ischemic attack (TIA) has been shown previously. However, it remains unclear whether the ischemic cerebral event is directly associated with the risk of femoral fractures.
Aims:
The aim of this study was (1) to assess the association between the frequency of femoral fractures in patient with IS and TIA, and (2) to compare the risk of femoral fractures to the Austrian general population.
Methods:
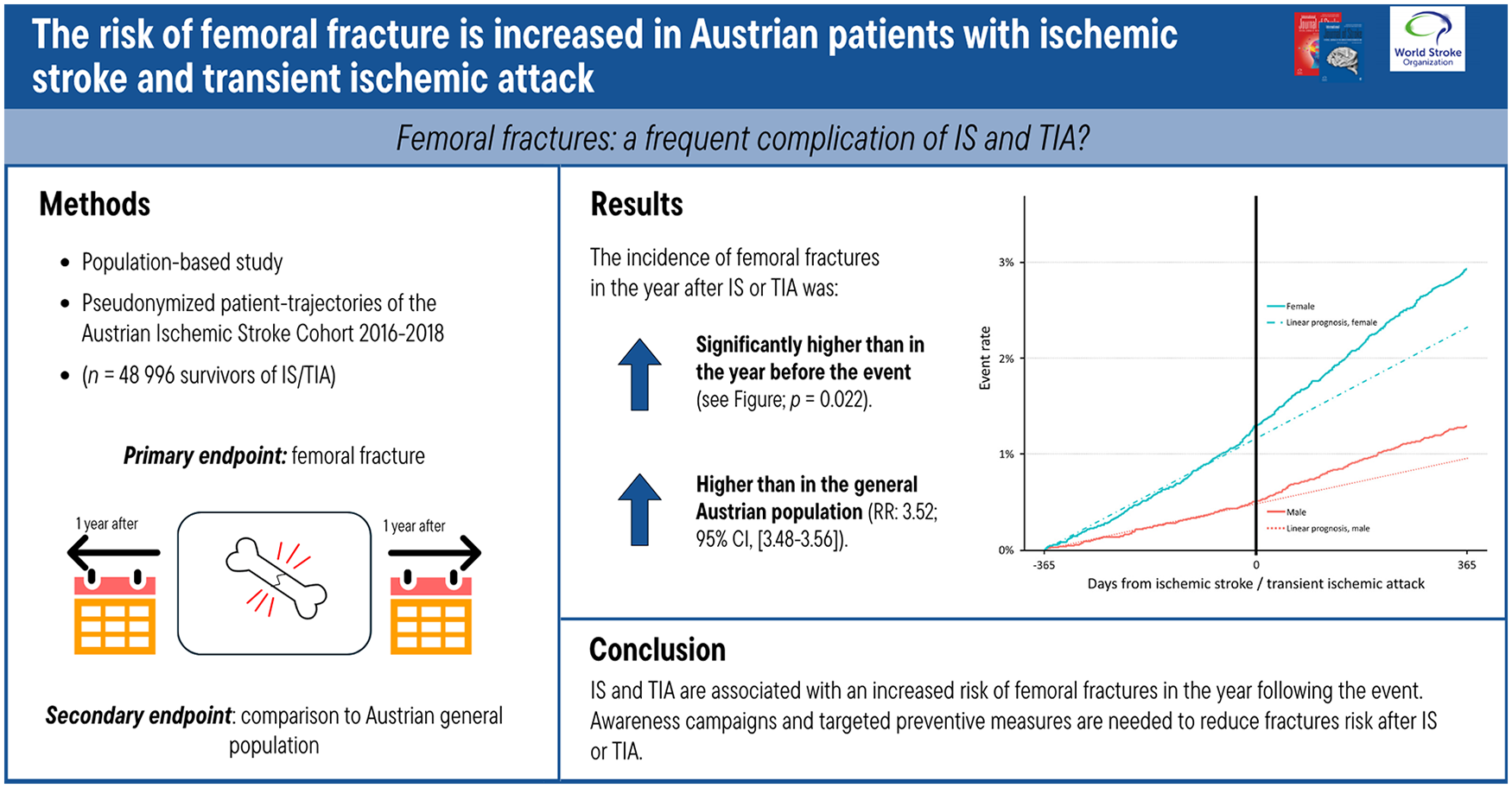
Population-based observational secondary analysis of the Austrian Stroke Cohort to assess the incidence of femoral fractures in the year after IS/TIA compared with the year before, and both intervals compared with the Austrian general population. All patients ⩾20 years treated for IS/TIA in Austria between 1 January 2016 and 31 December 2018 were identified using medical record linkage. Patient trajectories were reconstructed from 1 January 2015 to 31 December 2019 to have a 1-year observational period before and after the event. Femoral fractures within 1 year after IS/TIA compared to 1 year before IS/TIA were analyzed using McNemar test and Cox regression analysis considering sex and age. The 1-year age- and sex-adjusted relative risk of femoral fractures was calculated for patients with IS/TIA and compared to the Austrian general population.
Results:
A total of 48,996 survivors of IS (n = 34,997) and TIA (n = 13,999) were included. The incidence of femoral fractures increased significantly from the year before the IS/TIA (8.9 per 1000 person-years, 95% CI 7.7–10.2) to the year after the event (11.8 per 1000 person-years, 95% CI 10.1–13.5; p = 0.022). Compared to the Austrian general population including 21.1 million patient-years at risk and 37,436 femoral fractures, the risk of femoral fractures was increased both in the year before (RR 2.08, 95% CI 2.06–2.11) and after (RR 3.52, 95% CI 3.48–3.56) the IS/TIA.
Conclusion:
The risk of femoral fractures was found to be increased in the year following an IS/TIA, indicating a direct association with the IS/TIA event.
Data access statement:
Reconstruction of medical record linkage and individual patient trajectory reconstruction were reported previously. Data from individual patient trajectories was used for this analysis.
Keywords
Introduction
Stroke, osteoporosis, and fragility fractures are highly prevalent conditions that have a significant impact on mortality, morbidity, and disability, and cluster together.1–3 Prospective case series reported a risk of any fracture between 2.0% and 4.6% in the year after transient ischemic attacks (TIA) or ischemic stroke (IS).4,5 In the Austrian STROKE-Card trial including 2149 patients, the risk of any fractures in the year after an ischemic stroke and transient ischemic attack (IS/TIA) was 4.6%, which was similar to the risk of stroke recurrence (4.4%). 6 These findings are in line with previous data, showing a 2-year risk of low-trauma fractures between 4.8% (TIA) to 5.7% (IS), with femoral fractures being the most common.7,8
Population-based registries suggested an up to 7-fold risk of fractures including femoral fractures within the first year after stroke compared to the general population.9,10 However, increased fracture risk after stroke does not necessarily imply an effect of the cerebrovascular event itself. Multiple potentially confounding factors such as genetic aspects, lifestyle risk factors, comorbidities or medication may influence this risk. Therefore, the question of whether femoral fractures are associated with IS/TIA remains unclear. A significant increase of femoral fractures in the year after an IS/TIA as compared to the year before the event in the same patient may reveal the impact of the cerebrovascular event itself on the risk of femoral fractures.
Aims
The aims of the present population-based observational secondary analysis of the Austrian stroke cohort were (1) to assess the association between the incidence of femoral fractures in patients with IS/TIA using patient-trajectories and (2) to compare the risk of femoral fractures between patients with IS/TIA and the Austrian general population.
Methods
The Austrian cohort of patients with IS/TIA was reconstructed between 1 January 2016 and 31 December 2018 using pseudonymized health-related patient data. A mandatory standardized national minimum basic data set (MBDS) is available for each in-patient admission in Austria as described earlier.11,12 Inclusion criteria comprised patients aged 20 years or older with acute IS (I63) or TIA (G45) according to the primary ICD-10 discharge diagnosis. We did not consider patients with a primary diagnosis of transient global amnesia (G45.4). In case of multiple events within the study period the earliest event was considered.
Femoral fractures within 1 year before and/or after IS/TIA
An observational period covering 1 year before and after the IS/TIA for each patient was accomplished by extending the respective patient-trajectory study period to 1 January 2015–31 December 2019. This included all in-patient treatment episodes irrespective of the primary discharge diagnosis of each patient. Data from a federal state of Austria indicated that more than 97.4% of stroke patients were treated in an in-patient setting and there are no TIA clinics in Austria. 13 Patients with femoral fractures were defined as acute in-patient admissions or transfers from another hospital with a primary discharge diagnosis of “S72—Fracture of femur.” Patients having passed away throughout the in-patient treatment period for IS/TIA were excluded. We included the first femoral fracture of each patient within the study period.
Femoral fractures in the Austrian general population
This included patients without IS/TIA as defined above and an acute in-patient admissions or transfers from another hospital with a primary discharge diagnosis of “S72—Fracture of femur” between 1 January 2016 and 31 December 2018.
Patient trajectory reconstruction
Data transmission of the MBDS is encrypted using Secure Copy with public key authentication, using Secure Shell for data transfer and data authentication. Patient pseudonymization is available since 2015, which is ensured using (1) a non-recalculable pseudonym, (2) a non-recalculable record-ID, and (3) age groups of 5 years. 11 Individual patient-trajectories can therefore be reconstructed and analyzed while respecting the patients’ privacy. Data quality and completeness is ensured through periodic data audits. Data extraction was conducted after data cleaning on 2 March 2021. This study followed the Strengthening the Reporting of Observational Studies in Epidemiology reporting guidelines. 14
Ethical considerations
This study was conducted according to federal Austrian laws and regulations and in accordance with the Helsinki Declaration as revised in 2013. The analyses were approved by the Austrian Inpatient Quality Indicators scientific and steering committee with the approval number 2021-2024-0.711.401 (Austrian Federal Ministry of Social Affairs, Health, Care and Consumer Protection). Given to the pseudonymized nature of the data, the requirement for written informed consent was waived.
Endpoints
The main outcome of this study was the comparison of the incidence rate of femoral fractures within 1 year after versus 1 year before an IS/TIA, as assessed by matched-pairs analysis. Secondary analyses included the relative risk of femoral fractures in the year before and after the IS/TIA compared to the Austrian general population.
Statistical analysis
Demographic information was summarized using frequency counts and percentages. Information of the Austrian population was obtained from the federal statistical office. Incident events are reported per 1000 person-years. Age- and sex-standardization was carried out using the combined Austrian census population of the investigated time period (2016–2018) with the direct method and 95% confidence intervals (CIs) modeled assuming Poisson distribution. Censoring for intrahospital death after an IS/TIA was conducted but no information about death after discharge was available. To assess differences in frequency of femoral fractures between patients with IS/TIA and the general Austrian population excluding those with an IS/TIA, we calculated relative risks (RR) with 95% CIs. To assess differences in frequency of femoral fractures before and after the IS/TIA we used McNemar test (matched chi-square test). The McNemar test is a frequently used test for binary matched-pairs data as present in the manuscript comparing the same individuals in the preceding and subsequent year of the IS/TIA. To assess the association of sex and age group with femoral fractures before and after the IS/TIA a Cox regression analysis including interaction analysis was conducted. An alpha level of 5% was used. Analyses were performed using Microsoft Excel (Version 2308) and R (v4.2.2).
Results
We included 48,996 patients with ischemic stroke (n = 34,997) and TIA (n = 13,999) between January 2016 and December 2018. Of these, 47.6% (23,324/48,996) were female and 52.5% (25,704/48,996) were ⩾75 years of age (Table 1). The Austrian census population between 2016 and 2018, covered 21.1 million person-years at risk, with 37,436 recorded femoral fractures.
Patient characteristics for patients with ischemic stroke, transient ischemic attack and femoral fractures in Austria and characteristics of persons with femoral fractures in the Austrian general population.
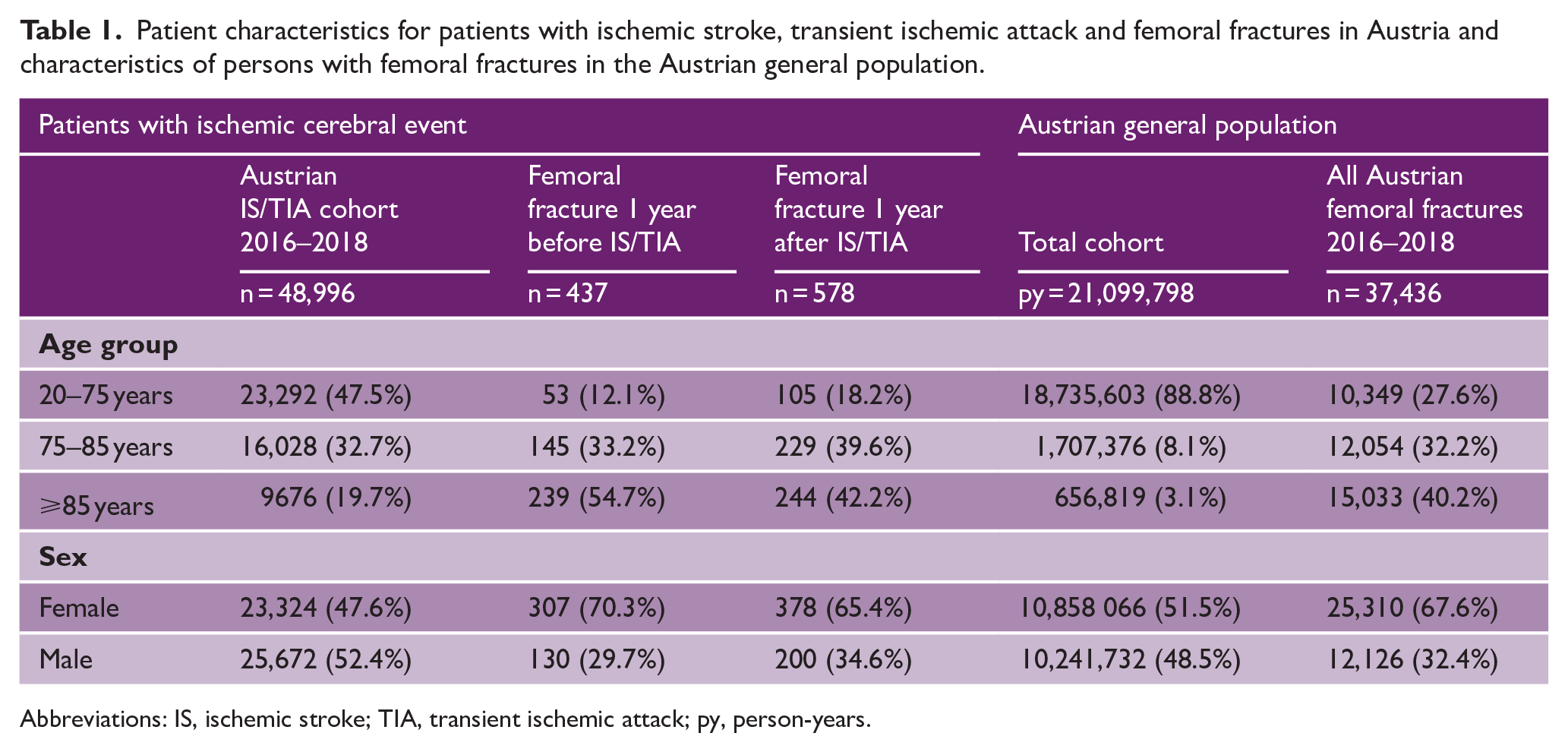
Abbreviations: IS, ischemic stroke; TIA, transient ischemic attack; py, person-years.
In total, 1,015 femoral fractures in 1,004 individuals were recorded in the year preceding and following the IS/TIA. Eleven patients experienced a femoral fracture both in the year before and after the event (Table 2). Femoral fractures were recorded in 437 patients in the year before the IS/TIA, representing an incidence of 8.9 per 1000 person-years (95% CI 7.7–10.2, Table 3). In the year after the IS/TIA femoral fractures were recorded in 578 patients. The incidence of femoral fractures was 11.8 per 1000 person-years (95% CI 10.1–13.5). Women and patients in the highest age-group represented the majority of patients with femoral fractures, both in the year before and after the IS/TIA. Femoral fractures were significantly more often observed in the year after the IS/TIA, compared to the year before (p = 0.022). Results by sex and age group are shown in Figure 1. This finding was not modified by age and sex (p-value for interaction > 0.05). A sensitivity analysis, excluding the eleven patients who experienced a femoral fracture both in the year before and after the IS/TIA confirmed these results (age- and sex-adjusted incidences of femoral fractures per 1000 person-years years in the year preceding the IS/TIA 8.7, 95% CI 7.4–9.9; in the year following the IS/TIA 11.6, 95% CI 9.9–13.3; RR 1.71, 95% CI 1.56–1.87, p < 0.001).
2×2 table of patients with and without femoral fractures in the year before and after the IS/TIA.
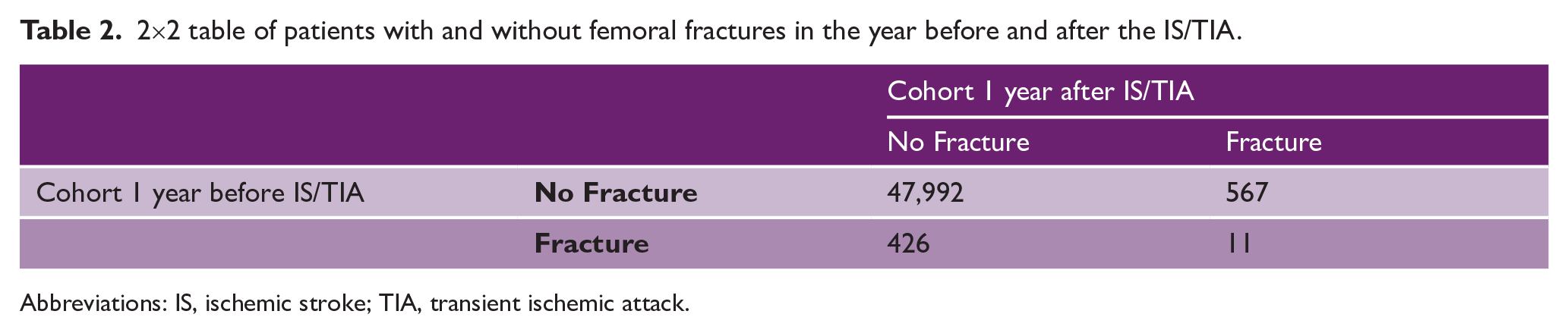
Abbreviations: IS, ischemic stroke; TIA, transient ischemic attack.
Incidence of femoral fractures in patients with ischemic stroke and transient ischemic attack in Austria and in the Austrian general population.
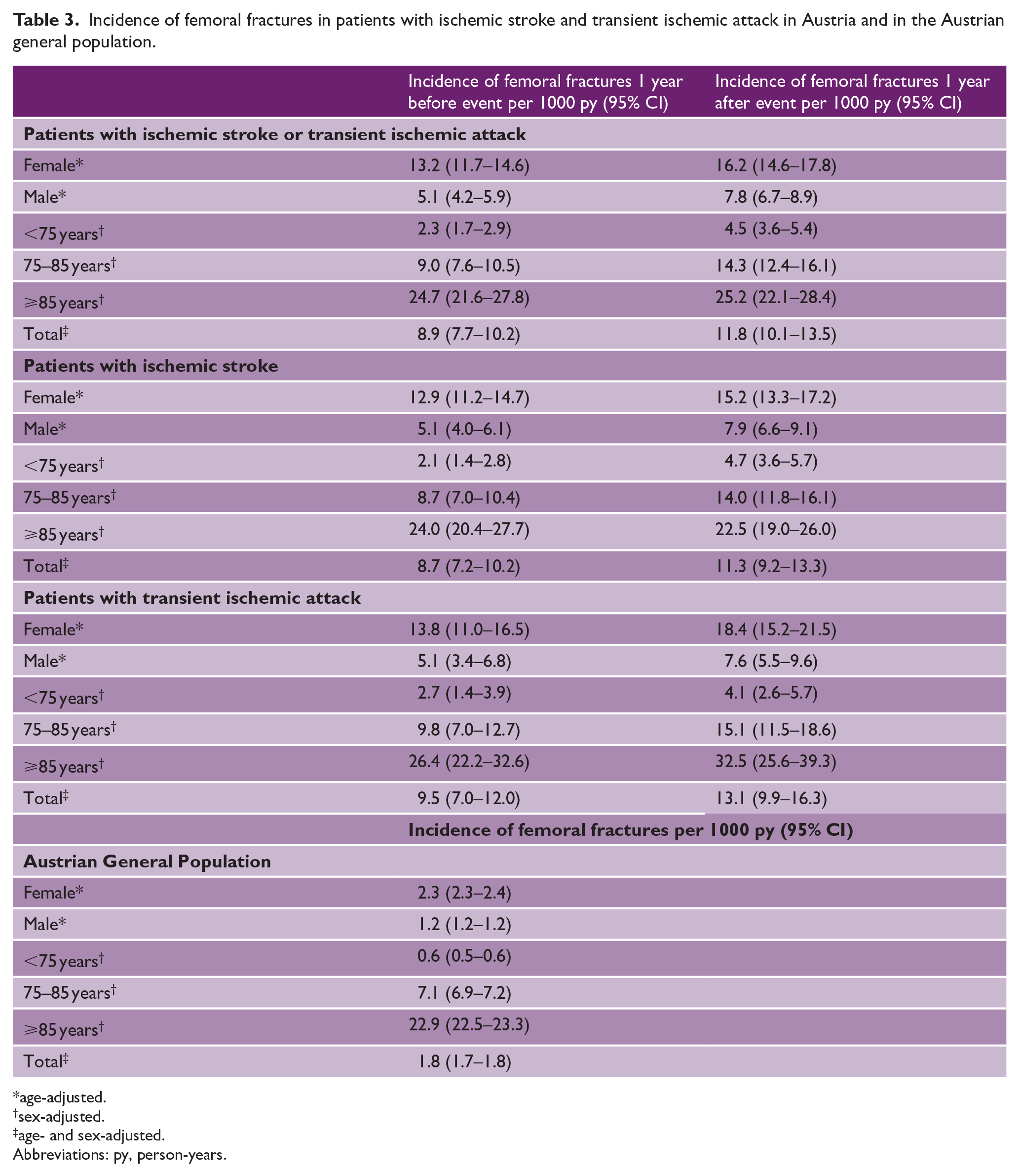
age-adjusted.
sex-adjusted.
age- and sex-adjusted.
Abbreviations: py, person-years.
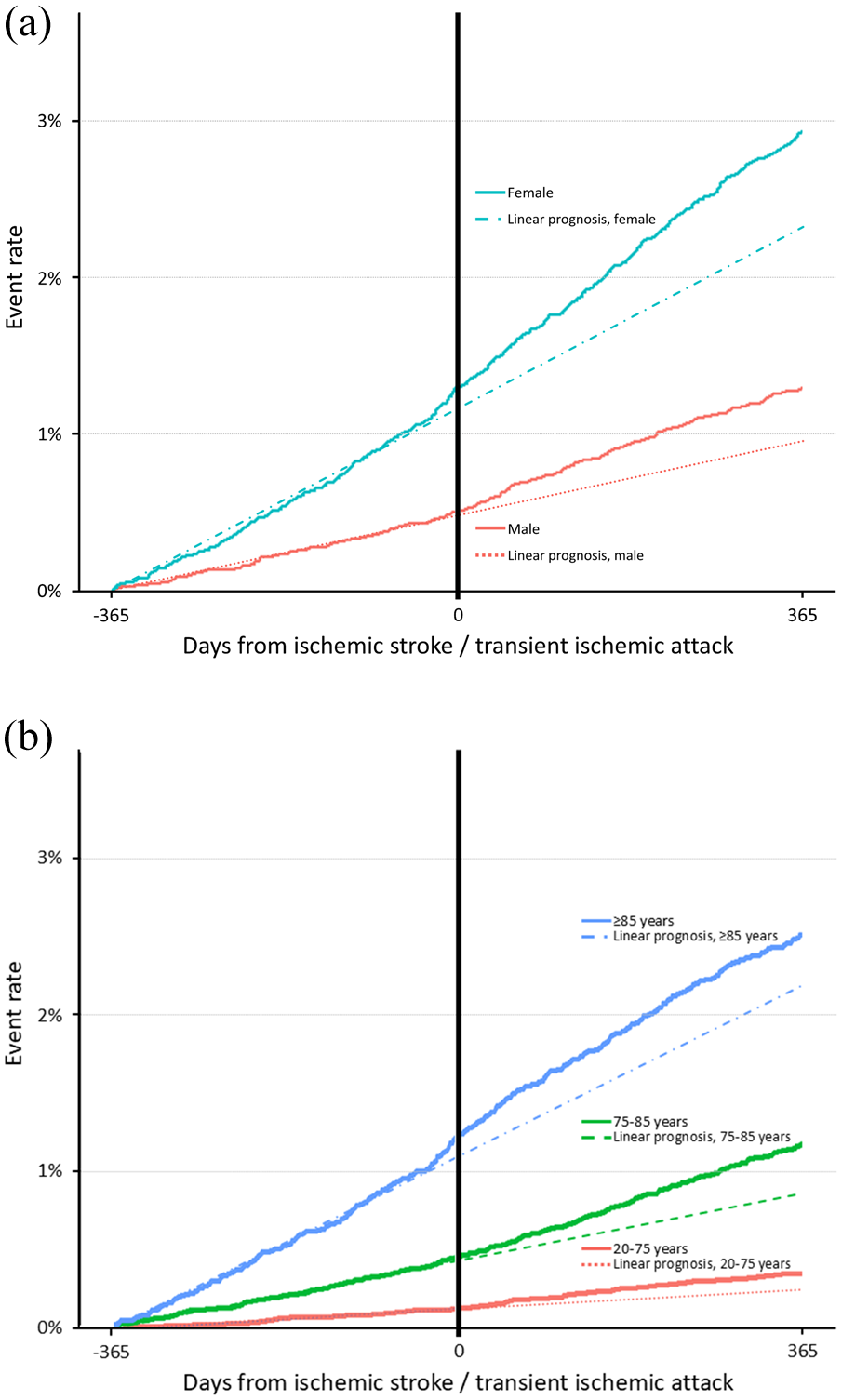
Femur fractures within 1 year before and after an ischemic cerebral event in Austria (a) by sex and (b) by age group.
The incidence of femoral fractures in the Austrian general population was 1.8 per 1000 person-years (95% CI 1.7–1.8). The 1-year age- and sex-adjusted relative risk of femoral fractures was elevated in patients with IS/TIA compared to the Austrian general population, both in the year before (RR 2.08, 95% CI 2.06–2.11) and after (RR 3.52, 95% CI 3.48–3.56) the event. Similar results were seen for the subgroups of IS and TIA patients, as well as in female and male patients as depicted in Table 4.
Relative risk of femoral fractures in patients with ischemic stroke and transient ischemic attack in Austria compared to the Austrian general population.
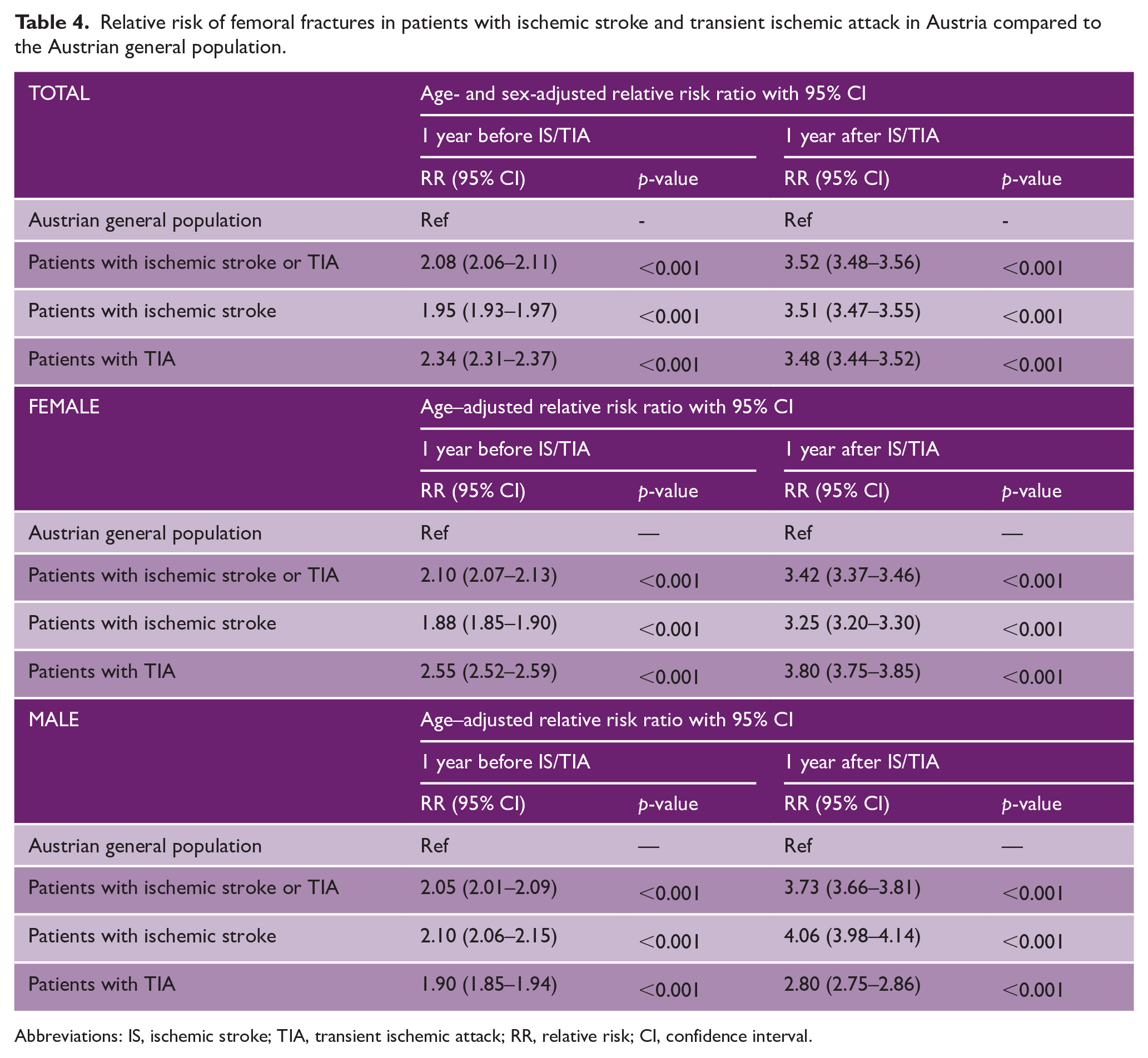
Abbreviations: IS, ischemic stroke; TIA, transient ischemic attack; RR, relative risk; CI, confidence interval.
Discussion
In this study, pseudonymized patient-trajectories were used to assess the association between the incidence of femoral fractures and IS/TIA in a national population-based observational secondary before-after analysis. The main finding of the present analysis was that femoral fractures occur more frequently in the year after an IS/TIA compared to the year before, suggesting a role of the cerebrovascular event on the risk of femoral fractures. There is a constant increase of femoral fractures after the IS/TIA in the first year and findings were consistent in women and men and across age groups.
Notably, patients with an IS/TIA have an approximately 2-fold higher risk of femoral fractures in the year before the cerebrovascular event compared to the Austrian general population. This may indicate that existing co-morbidities and risk factors leading to IS/TIA already predispose to femoral fractures.
Remarkably, patients with IS and TIA had a comparable risk of femoral fractures. Thus, neurological deficits do not seem to account for the increased risk of femoral fractures. This finding aligns with previous data.7,15,16 Based on the Ontario Stroke Registry, the additive effect of disability-associated falls to the risk of femoral fractures appears to be small.7,15 The 2-year risk of any fragility fracture after TIA was reported to be 4.8% and 5.7% after IS respectively. 7 A scoring system (FRAC-Stroke score) has been developed based on the aforementioned data, with a range from −9 to +36 points and a predicted risk of nontraumatic fractures between 0.5% and 34.1%. 15 Disability only had a minor contribution to this score.7,15 Similarly, the scoring system derived from a secondary analysis of the IRIS trial demonstrated its capacity to differentiate between patients at high- and low-risk for fractures. 16 Dalli et al. 17 recently reported results from a retrospective analysis of the Australian stroke registry with a similar higher fracture risk in patients with stroke and TIA. A prospective, population-based cohort study demonstrated that 23.5% of patients with stroke had fallen at least once within two years after the event. 18 Patients with an impaired mobility and an mRS score of 2–3 exhibited the highest risk of falling when compared to independently mobile patients. 18
It is not reasonable to assume that changes in medication for the prevention of stroke may explain the higher risk of femur fractures following an IS/TIA.19–22 It has been demonstrated that vitamin K-dependent oral anticoagulants, which have been associated with an increased risk of osteoporosis, have already been replaced by direct anticoagulants in Austria that do not pose an increased risk for osteoporosis. 19 Statins, which are frequently prescribed following an IS/TIA, have been suggested to possess protective properties against osteoporosis. 20 Antihypertensive treatment has been demonstrated to increase the risk of falls and syncope, yet not the risk of fractures. 21 Conversely, depression and antidepressant medications are associated with an increased risk of femur fractures.22,23 A Danish registry-based cohort study found that 25.4% of patients with IS received a diagnosis of depression and antidepressant medication within two years of the IS, with over half of them receiving the diagnosis and starting treatment within the first three months. 24 In a nationwide matched cohort study of elderly individuals in Sweden, Brännström et al. 22 observed that those receiving antidepressants had more than twice the incidence of femur fractures than those without antidepressant medication. However, the increased incidence was almost identical before and after the start of the antidepressive treatment. 22 The highest risk of femur fractures occurred 16 to 30 days before the prescription of medication. 22 This result may indicate a parallel increase in the risk of femur fractures and the emerging need for a treatment of depression. IS/TIA can be conceived as life-changing events causing elevated levels of stress, which, in turn, may result in negative coping responses and various mental health disorders, including insomnia, anxiety, and depression. 25
From a public health perspective, these data reinforce the need for primary prevention of cerebrovascular events and bone health. Screening for fractures using the Fracture Risk Assessment (FRAX) score is recommended for individuals aged 50 years and above in Austria. 26 The FRAX score has been demonstrated to be predictive of femoral fractures in patients who have experienced a stroke. 27 Patients with a ⩾5% 10-year risk of a hip fracture, or a ⩾20% risk of a major osteoporotic fracture within the next ten years should undergo further investigations, including dual-energy X-ray absorptiometry and blood tests of bone metabolism. 26 Reduced mobility and the mRS should be included in the calculation of risks of falls and fractures.15,18 A meta-analysis suggests a beneficial effect of physical exercise on bone mineral density of the paretic extremity. 28
A nationwide program of post-stroke disease management has been implemented in Austria, based on the findings of the Stroke Card trial. 6 In the future, the effect of this program on the secondary consequences of ischemic cerebral events may be evaluated in a real-world setting by using the pseudonymized reconstruction of patient trajectories in Austria.
Limitations
Limitations of the presented work clearly concern the limited amount of stroke-specific patient information, including the severity of stroke, comorbidities and medication. This information would be necessary to identify the cohort at the highest risk of femoral fractures. However, the accompanying prospective cohort study which assessed all relevant patients’ characteristics, and all fractures yielded highly consistent findings.
The presented data represent renumeration information within the Austrian health system, posing the potential for coding bias. However, rigorous and regular reviews and controlling measures ensure correctly coded, high-quality data. 11 Further limitations include a known data completeness of 92%, and the current advice to forego analyses with routine out-patient documentation due to lower data-cohesiveness. 11 We deliberately did not broaden the study period in order to abstain from potential bias due to the SARS-CoV2 pandemic.
Censoring for intrahospital death due to any cause was possible. However, information on deaths occurring after discharge throughout the follow-up period was not available, which resulted in a conservative statistical approach. Consequently, the incidence of femoral fractures after IS/TIA estimated in the study is likely to be lower than the actual incidence. In the accompanying paper, the person-years were reduced by 2.2% once considering deaths after discharge.
Strengths include the large national cohort of consecutive patients providing a robust foundation for a population-based analysis. The capacity to reconstruct patient-trajectories provides the unique opportunity to examine femoral fractures before and after the IS/TIA of each individual patient.
In conclusion, the risk of femoral fractures is elevated in the year following an IS/TIA compared to the year preceding it, indicating that IS/TIA are associated with an increased risk of femoral fractures. Further studies are necessary to identify those at highest risk of stroke-associated femoral fractures. Overall, these data call for increased awareness and the implementation of measures for fracture prevention, which should be integrated into post-stroke care.
Footnotes
Acknowledgements
We want to thank Dr Silvia Tuerk for her support to the Austrian stroke care. We want to thank Dr Mehdi Mousavi and Dr Thomas Hausner for their expertise.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The authors received no financial support for the research, authorship, and/or publication of this article. This study is supported by VASCage-Research Center on Clinical Stroke Research. VASCage is a Competence Centers for Excellent Technologies (COMET) Center within the COMET program and funded by the Federal Ministry for Climate Action, Environment, Energy, Mobility, Innovation, and Technology, the Federal Ministry of Labor and Economy, and the federal states of Tyrol, Salzburg, and Vienna. COMET is managed by the Austrian Research Promotion Agency (Österreichische Forschungsförderungsgesellschaft).
Ethical considerations
This study was conducted according to federal Austrian laws and regulations and in accordance with the Helsinki Declaration as revised in 2013. The analyses were approved by the Austrian Inpatient Quality Indicators scientific and steering committee with the approval number 2021-2024-0.711.401 (Austrian Federal Ministry of Social Affairs, Health, Care and Consumer Protection). Given to the pseudonymized nature of the data, the requirement for written informed consent was waived.
Consent to participate
Given to the pseudonymized nature of the data, the requirement for written informed consent was waived.
Data availability statement
Due to ethical and legal restrictions, pseudonymized patient-level data from this study cannot be shared. However, aggregated data are available from the corresponding author on reasonable request.