
Abstract
Introduction:
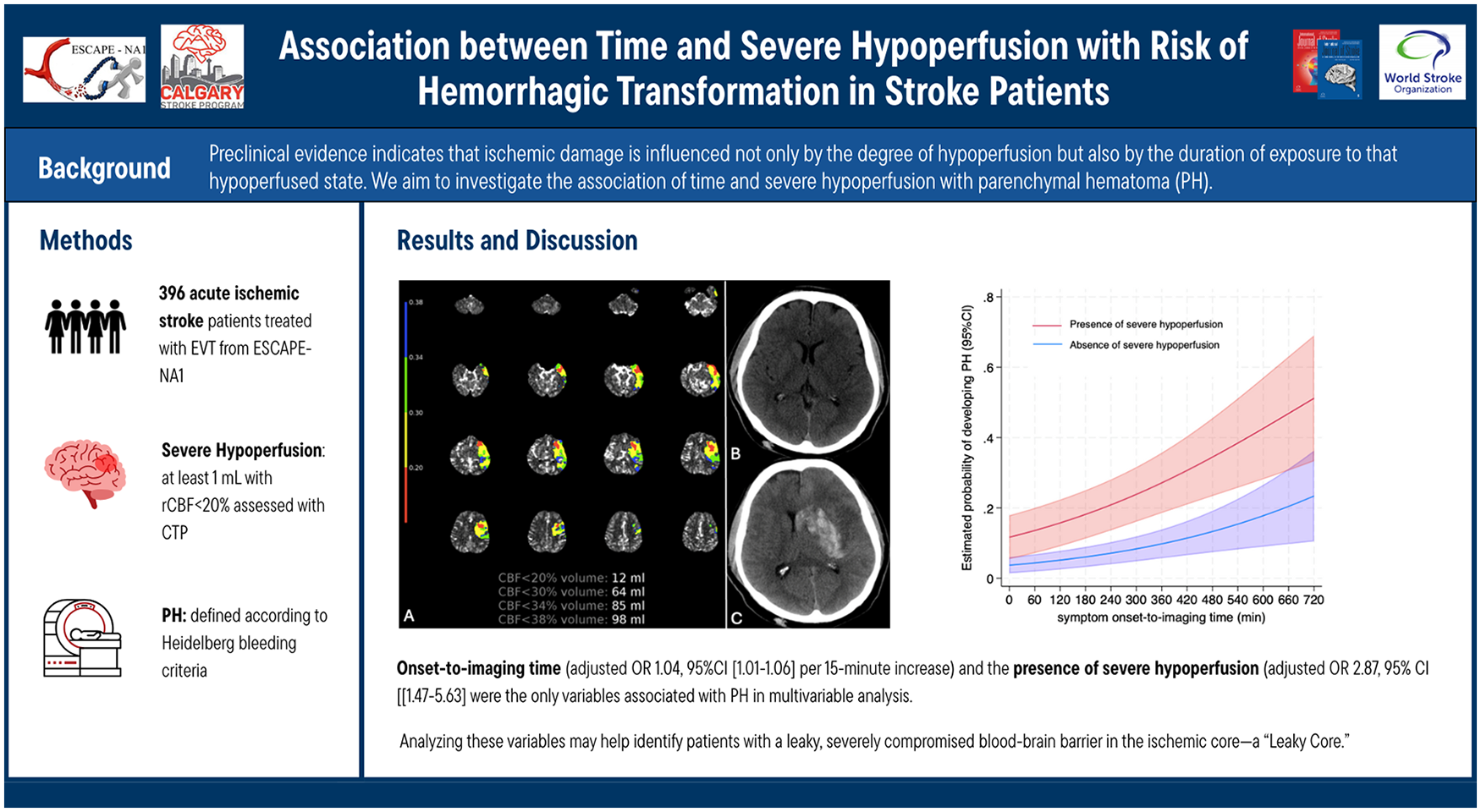
Perfusion imaging studies show a substantially increased risk of hemorrhagic transformation (HT) in severely hypoperfused tissue. Preclinical evidence indicates that ischemic damage is influenced not only by the degree of hypoperfusion but also by the duration of exposure to that hypoperfused state. We aim to investigate the association of time and severe hypoperfusion with parenchymal hematoma (PH) in ischemic stroke and explore whether there is a combined effect of the two variables on PH.
Methods:
Data are from the ESCAPE-NA1 trial, which evaluated the effect of nerinetide in large vessel occlusion patients treated with thrombectomy. This study included patients with some degree of recanalization (expanded Thrombolysis in Cerebral Infarct [eTICI] > 0) and available baseline CT perfusion. Severe hypoperfusion was defined as at least 1 mL volume of relative cerebral blood flow (rCBF) <20%. We assess 24-h imaging for the presence of PH, according to Heidelberg bleeding criteria. Univariable and multivariable logistic regression analyses, including interaction terms, were used to assess the effect of time and severe hypoperfusion on outcomes.
Results:
Out of 1105 patients from ESCAPE-NA1, 396 (35.8%) were included. The median age was 70 years (IQR = 59.8–79.2), 202 (51%) were females, and 50 (12.6%) experienced PH. Onset-to-imaging time (adjusted OR 1.04 [95% CI = 1.01–1.06] per 15-min increase) and the presence of severe hypoperfusion (adjusted OR 2.87 [95% CI = 1.47–5.63]) were the only variables associated with PH in multivariable analysis. No significant interaction effect of time and severe hypoperfusion on PH was found. The presence of severe hypoperfusion had a negative predictive value of 98% and a positive predictive value of 39.4% for predicting PH in patients presenting within 3 h and after 6 h from symptom onset, respectively.
Conclusion:
Both severe hypoperfusion and time affect the risk of hemorrhagic transformation. However, the interaction between these two variables was not statistically significant, indicating that their effects on hemorrhagic transformation risk are not dependent on each other. Analyzing these variables may help identify patients with a leaky, severely compromised blood-brain barrier in the ischemic core—a “leaky core.”
Keywords
Introduction
Hemorrhagic transformation (HT) is a common and potentially devastating complication of acute ischemic stroke. 1 According to some studies, HT can be observed in up to one-half of ischemic stroke patients, however, functional outcomes are primarily affected only by the development of parenchymal hematoma (PH), which occurs in 5%–30% of cases.2–5 Reperfusion-mediated injury in the ischemic core is presumably the main underlying pathogenic mechanism of HT.6,7 When the blood flow is dramatically reduced and for an extended period, not only does neuronal tissue die, but the blood–brain barrier (BBB) becomes progressively compromised and more leaky. 6 While the entire ischemic core ultimately shares the fate of irreversible infarction, the degree of BBB disruption and the associated risk of HT can vary significantly across different patients and regions of the core.8–10 Accordingly, perfusion studies in ischemic stroke patients have demonstrated that even a small volume of severely hypoperfused tissue in the ischemic core can increase the risk of PH by up to 50%.3,8,10–16 Indeed, there is a robust correlation between severe hypoperfusion and heightened permeability of the BBB. 17 Perfusion imaging is the preferred imaging modality to assess severely hypoperfused tissue, and even superior to diffusion-weighted magnetic resonance imaging (MRI) in predicting PH development, as it can more accurately identify the damaged blood vessel rather than merely indicating neuronal tissue death. 10
Pathophysiological evidence indicates that ischemic damage is influenced not only by the degree of hypoperfusion (as previously shown in human studies) but also by the duration of exposure to that hypoperfused state.1,7 Moreover, both animal and clinical studies suggest that although the ischemic core gradually expands, perfusion parameters usually remain stable, failing to capture the time-dependency of cerebral ischemic damage accurately.18–25 The impact of time on severely hypoperfused tissue for the risk of hemorrhagic complications remains poorly explored.
Aims and hypothesis
We aim to investigate whether time modifies the association between severely hypoperfused tissue and the risk of PH in acute stroke patients with large vessel occlusion treated with endovascular thrombectomy. We hypothesize that severe hypoperfusion is an independent risk factor for PH/HT and their association is modified by time from onset to imaging acquisition in such a way that longer times increase the risk of PH/HT at a given level of hypoperfusion.
Methods
Standard protocol approvals, registrations, and patient consents
Ethics approval was obtained from the relevant ethics committees at all participating centers and regulatory approval was obtained as necessary. Patients or their authorized representatives provided written informed consent.
Patient sample and study design
Data used in this study derived from the ESCAPE-NA1 trial, a randomized, multicenter, double-blinded clinical trial that examined the efficacy and safety of nerinetide in the treatment of ischemic stroke patients who underwent endovascular thrombectomy (EVT). The inclusion criteria and design of the trial have been previously published. 26 In summary, the trial enrolled adult patients with acute ischemic stroke caused by a large vessel occlusion in the anterior circulation who presented within 12 h from symptoms onset. In addition, patients with poor collateral status (defined as ⩽ 50% pial collateral filling of the middle cerebral artery territory on multiphase CT angiography [mCTA]), or large ischemic core (defined as Alberta Stroke Program Early CT Score [ASPECTS] < 5) were excluded.
For this secondary analysis, we included only patients with available baseline CT perfusion (CTP) and 24-h follow-up non-contrast CT (NCCT) or MRI to evaluate the presence of hemorrhagic transformation. Based on robust pathophysiological and clinical evidence indicating that reperfusion of ischemic tissue is essential for the formation of a parenchymal hematoma,3,8,10–16 we excluded patients who did not achieve any degree of recanalization (expanded Thrombolysis in Cerebral Infarction [eTICI] scale = 0). For patients with unknown onset of symptoms, we used the last time they were seen well as the reference point for the onset of stroke symptoms. Patients were subdivided based on the time from symptom onset to imaging acquisition into three categories (<3 h, 3–6 h, and >6 h).
Imaging acquisition and analysis
An independent imaging core laboratory, blinded to patient information and outcomes, analyzed the neuroimaging scans of the patients. CTP images were acquired at specific sites following local imaging protocols using RApid processing of Perfusion and Diffusion (RAPID) software version 5.2.2 (iSchemaView, Inc., Menlo Park, CA). Severe hypoperfusion was defined as at least 1 mL volume of relative cerebral blood flow (rCBF) <20%, CTP-estimated ischemic core volume was defined as the volume with rCBF) < 30%, the hypoperfused tissue was defined as time-to-maximum (Tmax) > 6 s volume, and CTP mismatch ratio was defined as the ratio between hypoperfused tissue and CTP-estimated ischemic core (Tmax > 6 s volume/rCBF < 30% volume). Recanalization status was assessed on the final intracranial catheter angiography runs using the eTICI scale. 27 Each patient underwent an NCCT or MRI at 24 h after receiving acute treatment. Hemorrhagic transformation of infarcted tissue was defined according to Heidelberg bleeding classification as scattered small petechiae with no mass effect (hemorrhagic infarction [HI]-1), confluent petechiae with no mass effect (HI-2), hematoma within infarcted tissue occupying < 30% of infarction volume with no substantial mass effect (PH-1), and hematoma within infarcted tissue occupying > 30% of infarction volume with obvious mass effect (PH-2). 1 Remote PH, that is, parenchymal hematomas occurring remote from the infarct, were ignored for the purpose of this analysis since they are unrelated to impaired BBB in the infarcted tissue and rather occur as a complication of intravenous thrombolysis. HT was visually assessed on 24-h follow-up imaging by two expert neuroradiologists (M.G. and J.M.O) with 25 and 5 years of experience, respectively, blinded to whether severe hypoperfusion was present at baseline. 5 An exemplary case of severe hypoperfusion and PH is illustrated in Figure 1.
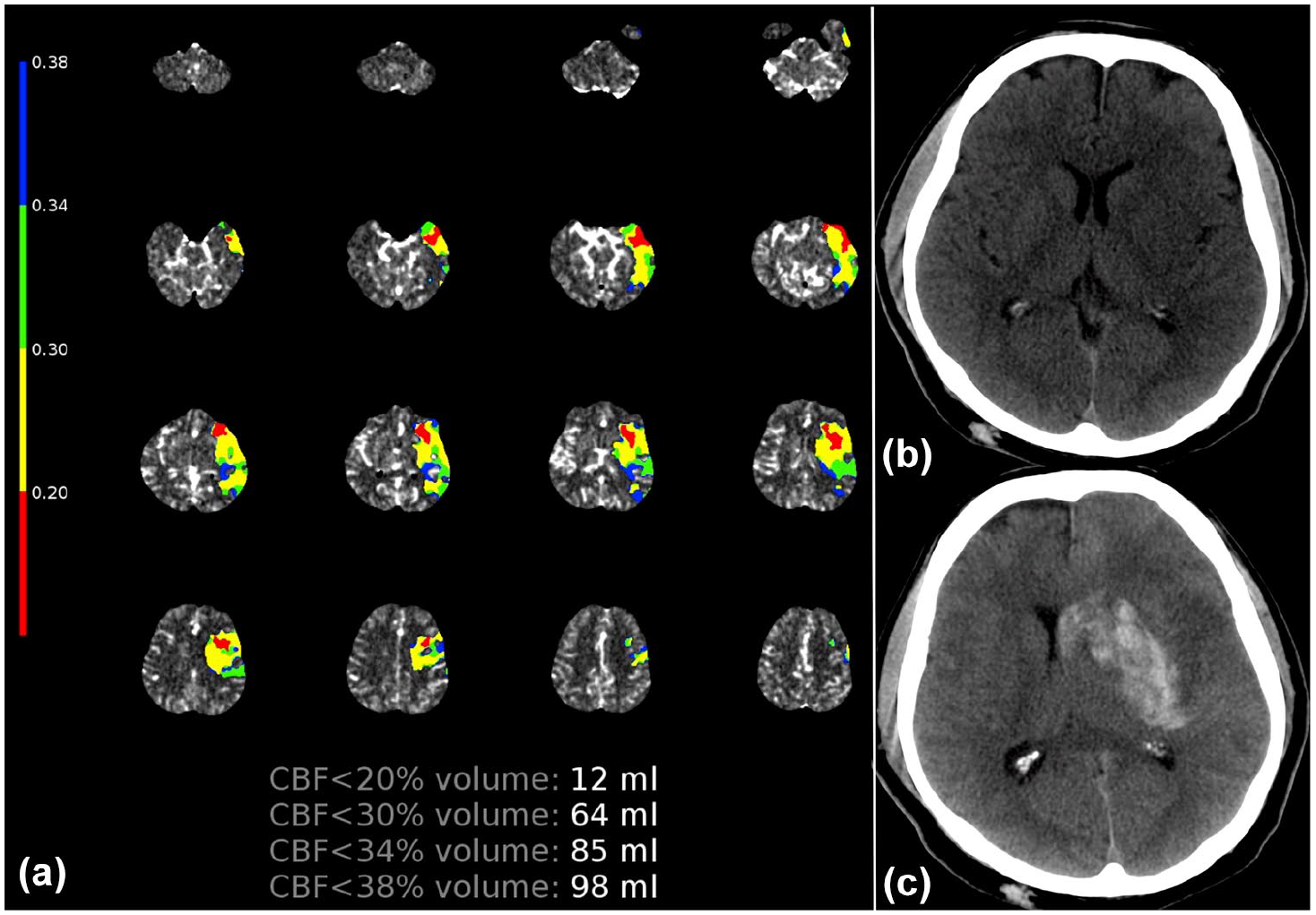
Exemplary case of severe hypoperfusion and hemorrhagic transformation.
Outcomes
The primary outcome was the presence of any parenchymal hematoma (PH-1 or PH-2). The secondary outcome was the presence of any hemorrhagic transformation of infarcted tissue (HI-1, HI-2, PH-1, or PH-2).
Statistical analysis
Quantitative and ordinal variables were expressed as medians and interquartile ranges, while nominal variables were reported as counts and percentages. Baseline clinical, radiological, and therapy workflow characteristics were reported with descriptive statistics and compared between patients with and without outcomes (any PH or any HT) using Fisher’s exact test for categorical variables and the Wilcoxon rank-sum test for continuous variables.
A multivariable binary logistic regression analysis investigated baseline variables significantly associated with outcomes in univariable analyses. Effect size estimates from logistic regression analyses were reported as odds ratios (ORs) with 95% confidence intervals (95% CI). The analyses were repeated with a two-by-two interaction term between time from onset to imaging and severe hypoperfusion (time*severe hypoperfusion) to determine a possible interaction between time and severe hypoperfusion on outcomes. In case the interaction term was not significant, all subgroup analyses that followed were considered exploratory.
The predictive performance of severe hypoperfusion (binary variable) for predicting outcomes was assessed over pre-specified time intervals from onset (<3 h, 3–6 h, >6 h) comprehensively, using sensitivity, specificity, positive predictive value (PPV), negative predictive value (NPV), and overall accuracy.
As a sensitivity analysis, we investigated the association between severe hypoperfusion, time from onset to imaging acquisition, and outcomes with regression analyses adjusted for predefined confounders, namely age, sex, baseline NIHSS, recanalization status (eTICI), intravenous thrombolysis, and time from imaging acquisition to recanalization. Furthermore, the main analyses were also conducted adjusted for potential confounders in patients with known symptom onset only (since the estimated time from symptom onset to imaging is naturally less accurate in patients with unknown symptom onset), and in patients who underwent MRI as follow-up imaging modality only (since hemorrhage sensitive MRI sequences have higher sensitivity for hemorrhagic changes compared to NCCT).
As a sensitivity analysis, we also investigated the predictive performance for outcome of severe hypoperfusion defined as at least 5 mL of rCBF < 20% volume and the Youden Index to assess the additional value of using severe hypoperfusion (rCBF < 20% volume) as a continuous variable rather than a binary variable (at least 1 mL of rCBF < 20%)
All calculated p-values were two-tailed. Statistical significance was assumed at p < 0.05. The statistical analysis was performed with Stata (Version 18.0).
Data availability
The corresponding author will grant access to the study data upon reasonable request and after approval by the ESCAPE-NA1 executive committee.
Results
Patient characteristics
Of 1105 patients recruited in the ESCAPE-NA1 study, 684 were excluded because they were not investigated with CTP at baseline, and 25 because they did not achieve any recanalization after thrombectomy (eTICI = 0) (Figure 2). Collectively, 396 (35.8%) patients were included in the study sample, and their characteristics are summarized in Table 1. The median age was 70 years (IQR = 59.8–79.2) and 202 (51%) patients were female. Overall, 50 (12.6%) patients developed a PH (PH-1 = 31 and PH-2 = 19). Patients who developed a PH, compared to patients who did not, had less chronic hypertension (56% vs 73.4%, p = 0.018), more rarely witnessed stroke onset (30% vs 57.1%, p < 0.001), lower baseline ASPECTS (7 [IQR = 6–8] vs8 [IQR = 7–9], p = 0.029), more frequent severe hypoperfusion (58% vs 28.3%, p < 0.001), larger rCBF < 20% volume (5.4 mL [IQR = 0–11.2] vs 0 mL [IQR = 0.-4.6], p < 0.001), larger CTP-estimated core volume (20.8 mL [IQR = 8.5–34.4] vs 9.1 mL [IQR = 0–29.8], p = 0.008), and longer onset-to-imaging time (320 min [IQR = 193–538] vs 141 min [IQR = 80–276], p < 0.001). None of the 25 patients who were excluded because of the absence of any recanalization (eTICI = 0) developed PH.
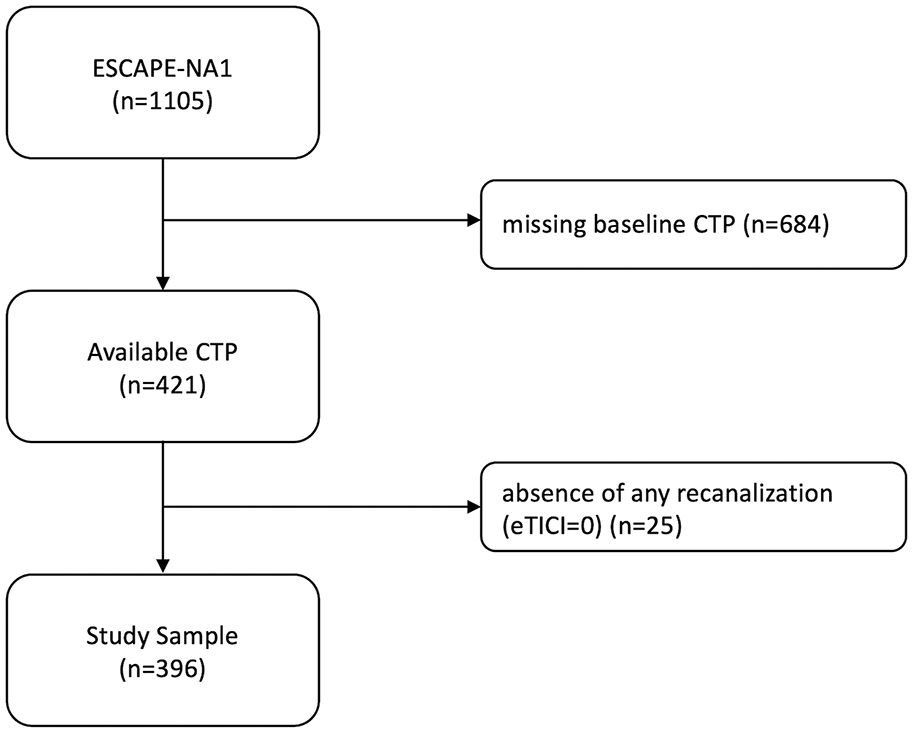
Flowchart of included patients.
Patient characteristics with and without parenchymal hematoma
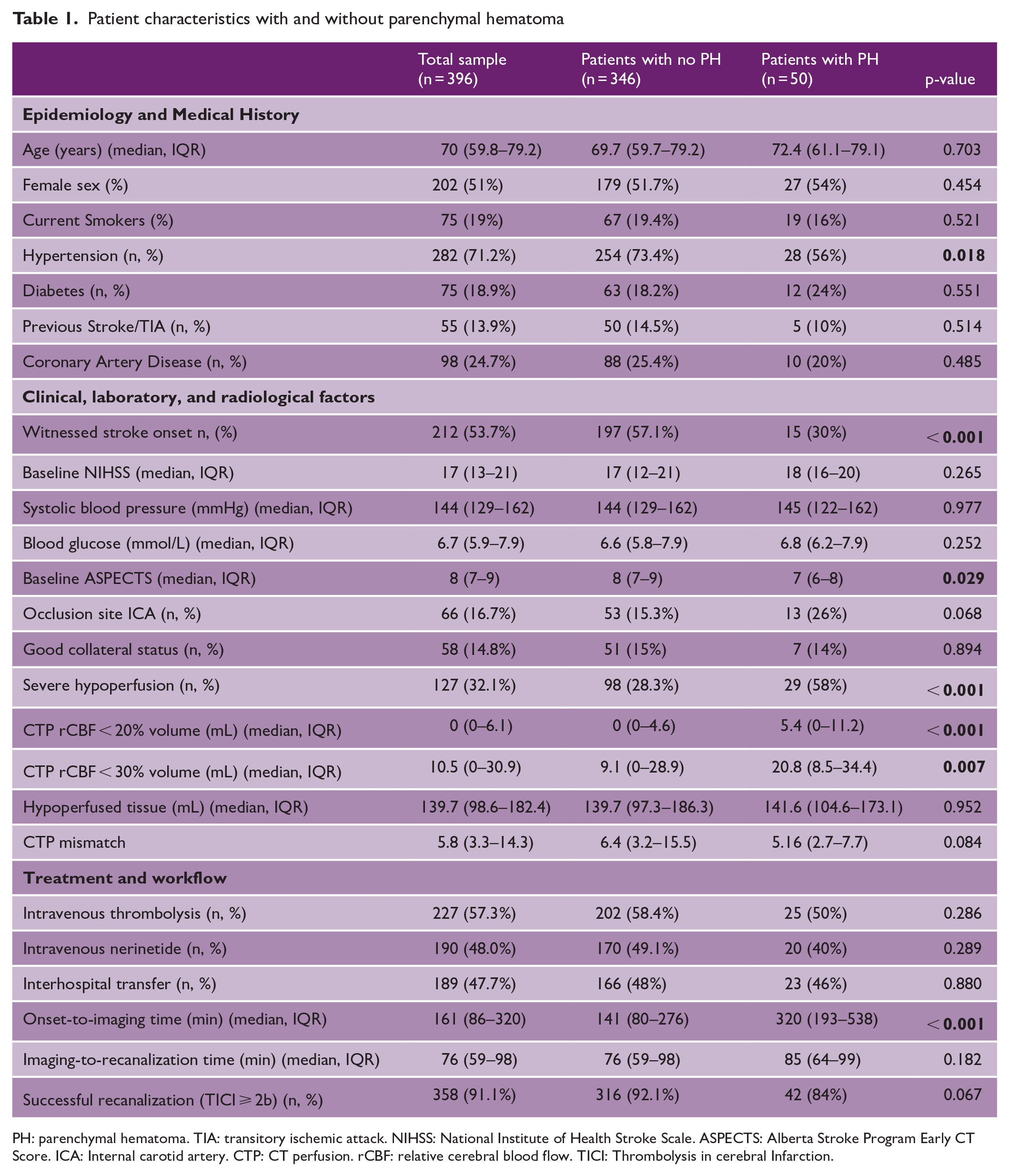
PH: parenchymal hematoma. TIA: transitory ischemic attack. NIHSS: National Institute of Health Stroke Scale. ASPECTS: Alberta Stroke Program Early CT Score. ICA: Internal carotid artery. CTP: CT perfusion. rCBF: relative cerebral blood flow. TICI: Thrombolysis in cerebral Infarction.
Interaction between time and severe hypoperfusion on outcomes
No significant interaction between time from onset to imaging and severe hypoperfusion was observed on PH (pinteraction = 0.462) or any HT (pinteraction = 0.744).
Variables associated with parenchymal hematoma
In the multivariable binary logistic regression analysis, the only baseline variables associated with PH were the presence of severe hypoperfusion (adjusted OR 2.87 [95% CI = 1.47–5.63]) and onset-to-imaging time (adjusted OR 1.04 [95% CI = 1.01–1.06] per 15-min increase) (Table 2) (Figure 3). No association was observed for baseline ASPECTS, chronic hypertension, or witnessed stroke onset.
Predictors of parenchymal hematoma in univariable and multivariable analyses.
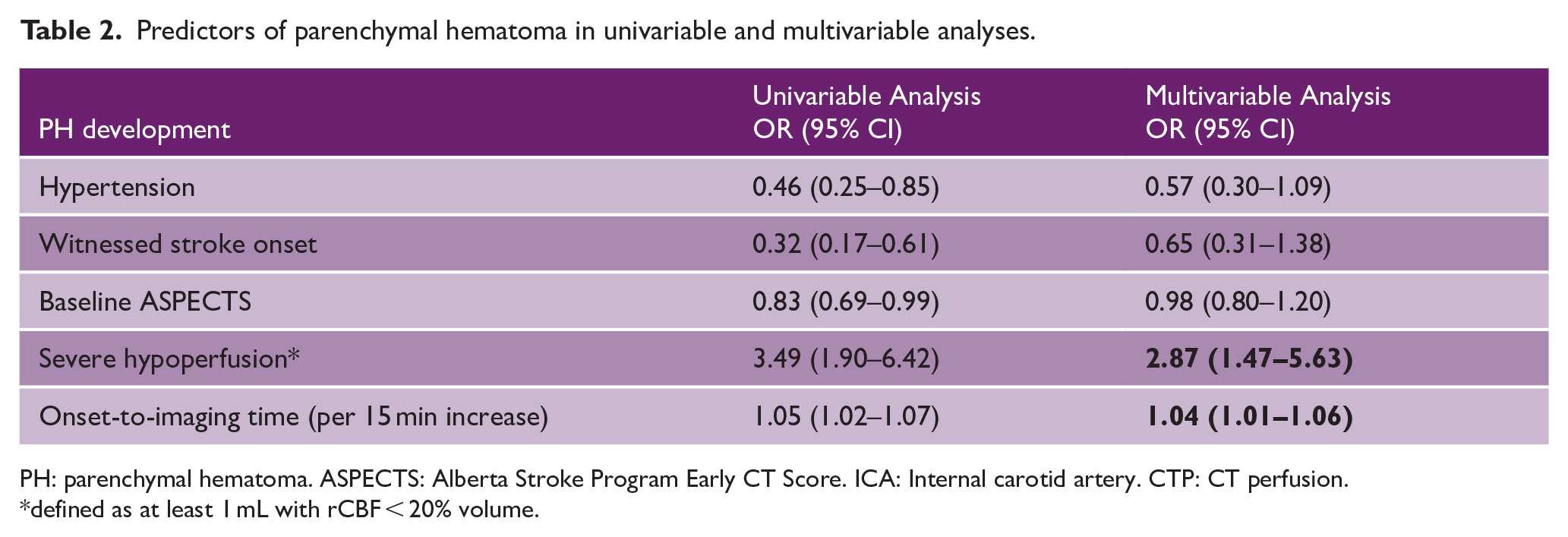
PH: parenchymal hematoma. ASPECTS: Alberta Stroke Program Early CT Score. ICA: Internal carotid artery. CTP: CT perfusion.
defined as at least 1 mL with rCBF < 20% volume.
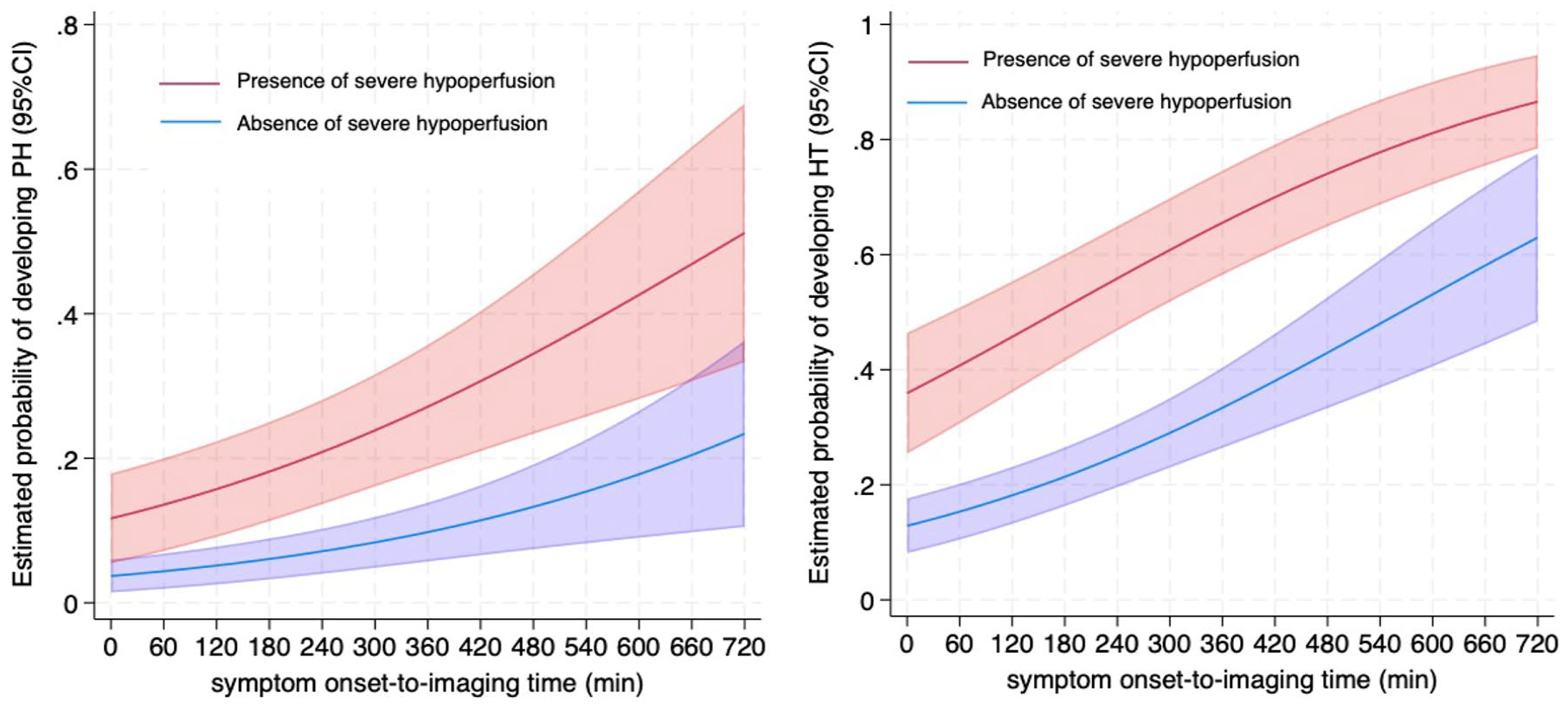
Association of time and the estimated probability of parenchymal hematoma (left) and any hemorrhagic transformation (right) in patients with and without severe hypoperfusion.
Predictive performance for parenchymal hematoma
Among 396 patients, 210 (53%) presented within 3 h from symptom onset, 104 (26.3%) between 3 and 6 h, and 82 (20.7%) beyond 6 h. The prevalence of PH in the three groups was 4.8% (<3 h), 18.3% (3–6 h), and 25.6% (>6 h). The PPV of severe hypoperfusion increased progressively over time: 11.5% (95% CI = 7.5–17.1), 27.3% (95% CI = 17.3–40.2), and 39.4% (95% CI = 28.5–51.5). The NPV of severe hypoperfusion decreased progressively over time: 98% (95% CI = 94.6–99.2), 85.9% (95% CI = 79.6–90.5), and 83.7% (95% CI = 74.3–90.1). Table 3 summarizes the predictive performances stratified by time windows.
Predictive performance of severe hypoperfusion, defined as at least 1 mL volume with rCBF < 20%, for predicting PH according to time from onset-to-imaging acquisition.
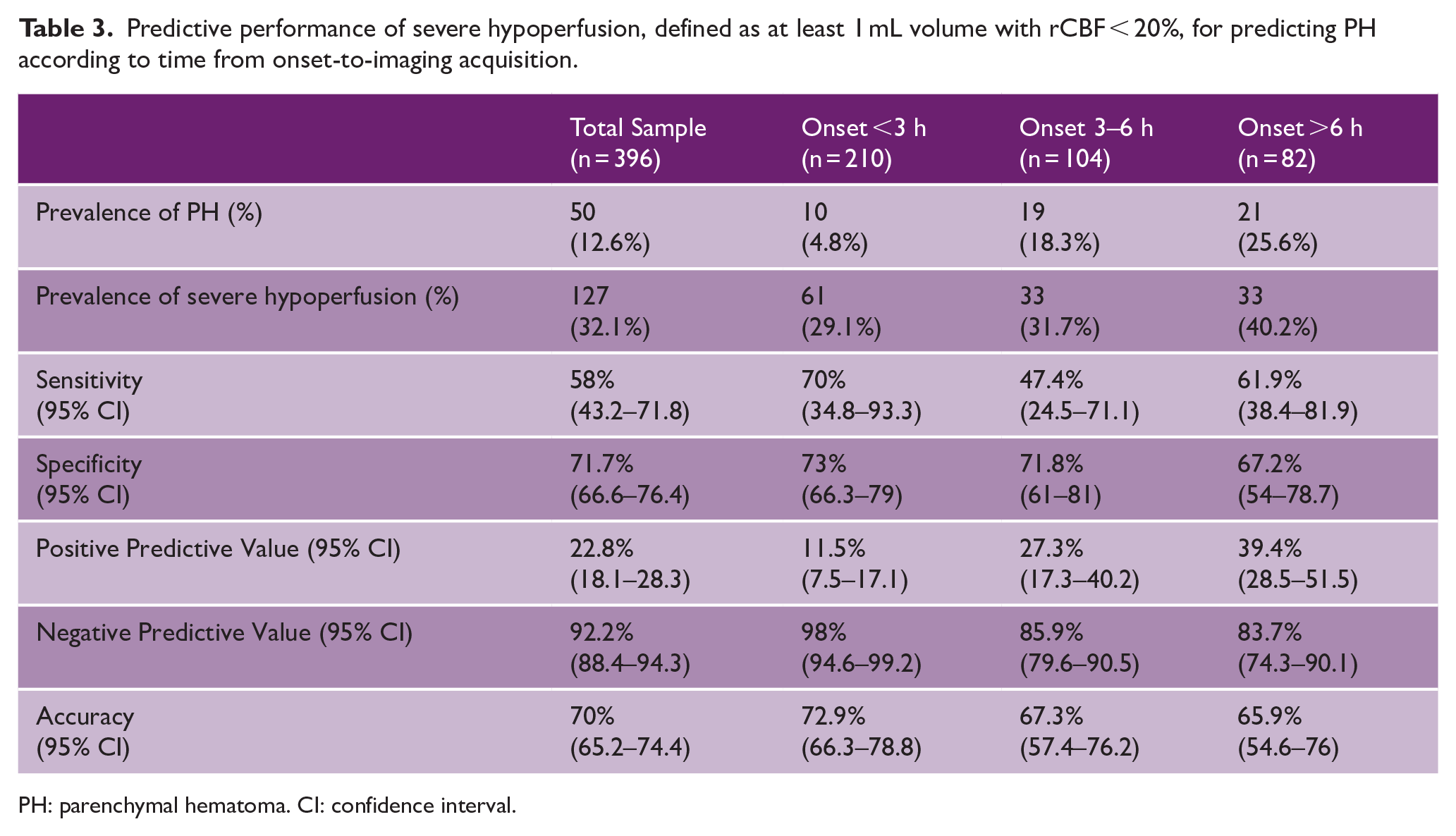
PH: parenchymal hematoma. CI: confidence interval.
Variables associated with any hemorrhagic transformation and predictive performance for any hemorrhagic transformation
Overall, 139 (35.1%) patients developed HT (HI-1 = 50, HI-2 = 39, PH-1 = 31, and PH-2 = 19). HT occurred in 71 (51.1%) patients with severe hypoperfusion compared to 56 (21.8%) patients without it (p < 0.001) (Supplementary Table 1). In multivariable binary logistic regression analysis, the variables associated with the development of HT were blood glucose levels (adjusted OR 1.34 [95% CI = 1.15–1.56] per 1 mmol/L increase), intravenous thrombolysis (adjusted OR 2.78 [95% CI = 1.24–6.22], severe hypoperfusion (adjusted OR 2.10 [95% CI = 1.03–4.04]), and symptom onset-to-imaging time (adjusted OR 1.08 [95% CI = 1.05–1.12] per 15-min increase) (Supplementary Table 2) (Figure 3). The PPV of severe hypoperfusion for predicting HT in patients presenting >6 h from symptom was 72.7% (95% CI = 58.6–83.4). The NPV of severe hypoperfusion for predicting HT in patients presenting <3 h from symptom onset was 86.6% (95% CI = 81.3–90.6) (Supplementary Table 3).
Sensitivity analysis in patients with known symptom onset
Two-hundred-thirteen (53.8%) patients had a known symptom onset. Among them, 15 (5.1%) developed PH. The association between PH and severe hypoperfusion (aOR 5.47 [95% CI = 1.50–20.00]) and onset-to-imaging time (aOR 1.13 [95% CI = 1.06–1.20] per 15-min increase) was statistically significant. The association between HT and severe hypoperfusion (aOR 2.56 [95% CI = 1.22–5.37]) and onset-to-imaging time (aOR 1.09 [95% CI = 1.05–1.14] per 15-min increase) was statistically significant.
Other sensitivity analyses
The main analyses yielded similar results in the patients investigated with MRI as follow-up imaging and when severe hypoperfusion was defined as at least 5 mL of rCBF < 20% ( Supplementary Materials and Supplementary Table 4 ). Moreover, multiple additional analyses showed that when severe hypoperfusion volume as a continuous variable was included in the multivariable and predictive models, there was no independent association of severe hypoperfusion volume with PH and no increase in performance of the predictive model. ( Supplementary Materials )
Discussion
Severe hypoperfusion, defined as at least 1 mL of rCBF < 20% on CTP maps, is a strong predictor for hemorrhagic complications after stroke thrombectomy. There is an association between PH and time from onset to imaging, whereby the odds of PH and HT increase by 4% and 8%, respectively, with every 15-min increment. Severe hypoperfusion yields high NPV and moderate PPV for predicting PH in the early and late window.
Our findings are consistent with the pathophysiology of ischemic infarction,8–10 suggesting that the disruption of the BBB within the ischemic core regions—and consequently the likelihood of HT—is influenced not only by the degree of hypoperfusion but also by the duration of exposure to that hypoperfused state. Similarly to using CTP maps to assess the baseline ischemic core, the risk of HT in severely hypoperfused tissue regions might be enhanced by considering the time elapsed from symptom onset, for instance, within defined time windows.18–23 However, we did not find a significant interaction effect of time from onset to imaging and severe hypoperfusion on outcomes, that is, there is no evidence to suggest that the effect of severe hypoperfusion at different onset-to-imaging time subgroups differs from the main effect.
Previous clinical studies reported a PPV of up to 50% for severely hypoperfused tissue in predicting PH, which is higher than what we observed. These studies adopted a stringent definition of severely hypoperfused tissue, specifying thresholds of either relative cerebral blood volume (rCBV) < 2.5% or absolute CBV < 1.8 mL/100 g.9–11,14,15,28 These definitions are collectively referred to as “very low CBV (vlCBV).” In our study, we used a less stringent definition of severe hypoperfusion, defining it as a rCBF < 20%, for pragmatic and pathophysiological reasons. The pragmatic choice of our definition was informed by the fact that rCBF < 20% maps are automatically provided by the widely available CTP RAPID software. 29 Moreover, considering the time-dependent nature of cerebral ischemic injury across varying perfusion levels,24,30,31 it is likely that in cases of extremely severe hypoperfusion (i.e. vlCBV), the damage occurs almost immediately, so it is nearly independent of the duration of ischemia. Conversely, as perfusion levels gradually rise (i.e. rCBF < 20–30–34%), the impact of time on injury becomes increasingly more critical.24,30,31
Notably, our results also included patients with unknown onset, arguably leading to overestimating the time elapsed since symptom onset. Indeed, in cases of unwitnessed onset, a conservative approach typically assumes the worst-case scenario, considering that the onset could have occurred at any point between when the patient was last seen normal and when they were discovered in a symptomatic state.32,33 Accordingly, our findings were even more robust when including only patients with known onset, with an increased risk of PH of 13% for every additional 15 min from onset to qualifying imaging acquisition.
In our analyses, we found that the volume of severe hypoperfusion (continuous variable) improved the predictive performance for PH minimally compared to the simple presence of severe hypoperfusion (binary variable). This finding is in line with previous studies that have highlighted the significance of the presence of any vlCBV, rather than the volume of tissue with vlCBV, in predicting HT risk.3,8,10–16 In other words, an ischemic core with a 1 ml volume of severely hypoperfused tissue seems to yield a similar risk of PH compared to an ischemic core with 20, 30, or 50 mL of severely hypoperfused tissue. Moreover, trials in large ischemic core thrombectomy patients have not found an increased risk of hemorrhagic complications compared to non-large core stroke trials,34–37 supporting the hypothesis that the presence of any volume of severe hypoperfusion is what determines the risk of HT and the volume of severely hypoperfused tissue plays a less critical role.
This concept of a severely hypoperfused core that cannot benefit from reperfusion and at the same time is at increased risk of hemorrhage suggests that advanced neuroimaging in acute ischemic stroke could potentially help decision-making by estimating not only the salvageable tissue but also delineating areas of the core at risk of bleeding, and perhaps even quantifying the risk of hemorrhage. The latter may be particularly relevant in light of the recently published large core thrombectomy trials that demonstrated clinical benefits of thrombectomy in this patient subgroup.34–37 Furthermore, patients with an ischemic core with a leaky, severely compromised BBB integrity (“leaky core”) would be ideal candidates for neuroprotective agents that mitigate the ischemia-reperfusion damage, and the presence of a “leaky core” could also inform bridging thrombolysis decision-making.38,39
Notably, while advanced techniques such as dynamic contrast-enhanced imaging can reliably assess BBB integrity, 40 it remains uncertain whether CTP-derived parameters accurately reflect BBB disruption. 41 Yet, this is in line with our hypothesis that hypoperfusion can serve as a surrogate for BBB status only when appropriately adjusted for the time of symptom onset. Future research should prioritize pragmatic, CT-derived imaging approaches that more directly assess the BBB integrity.
Our study has several limitations that should be acknowledged. First, the ESCAPE-NA1 trial excluded patients with low ASPECTS and poor collateral status, which likely resulted in a selection bias excluding most fast progressors and patients with “very” severe hypoperfusion. Second, most patients in our study presented relatively early after symptom onset, partly owing to the inclusion criteria of the trial, which only allowed enrollment within 12 h from last known well. Third, we did not explore the relationship between time elapsed from symptom onset and more stringent definitions of severely reduced perfusion because only standardized thresholded CT perfusion maps were available due to central, uniform CT perfusion post-processing workflow. Fourth, we did not assess the spatial overlap between baseline perfusion imaging and 24-h hemorrhagic transformation. Future studies incorporating high-resolution voxel-level imaging data are needed to investigate this relationship and strengthen the argument for a direct causal link. Fifth, several potential technical and clinical pitfalls are inherent in CTP imaging. 42 Moreover, the exclusion of 684 patients due to missing baseline CTP might have introduced a selection bias. Although most sites followed uniform, site-specific acute stroke imaging protocols and thus, whether or not a patient underwent CTP was mainly a factor of which site they were admitted to, some centers might reserve CTP imaging for specific clinical scenarios, such as uncertain time of onset or the absence of early ischemic changes on non-contrast CT—which could lead to a less representative study population. Sixth, the Heidelberg bleeding classification has a few limitations: (1) its detailed nature may limit its use in routine clinical practice where time or imaging quality may not be sufficient, (2) some hemorrhage may not always be clearly attributable to HT, especially in patients with trauma, and (3) its sensitivity depends on the imaging technique (e.g. MRI vs CT). Finally, similar analyses should be conducted using the other aspect of BBB disruption in ischemic stroke, namely, cerebral edema, as an outcome.
The CBF threshold for ischemic core has been shown to be time-dependent,19,20,43 and the same may be true for a “leaky core” threshold that predicts a high likelihood of hemorrhagic transformation. However, the very low CBV threshold previously investigated might be so severe that it may be a marker of hemorrhagic transformation across all time points, regardless of the time elapsed from symptom onset to imaging.
Conclusion
Both severe hypoperfusion and time have an effect on the risk of hemorrhagic transformation in ischemic stroke patients. The risk of developing PH and HT increased by 4% and 8%, respectively, with every 15-min time from onset-to-imaging increment in our study. However, the interaction between these two variables was not statistically significant, indicating that their effects on hemorrhagic transformation risk are not dependent on each other. In other words, each factor contributes to risk independently, but there is no evidence that the effect of one modifies the impact of the other. Perfusion imaging, combined with time information, may help discriminate regions within the ischemic core with a leaky, severely compromised BBB integrity (“leaky core”), and thus may help select candidates for neuroprotective agents that mitigate the ischemia-reperfusion damage, and inform thrombolysis bridging decisions. Future research should aim to establish perfusion parameters associated with a “leaky core,” and assess a possible time-dependency of these parameters.
Supplemental Material
sj-docx-1-wso-10.1177_17474930251360519 – Supplemental material for Association between time and severe hypoperfusion with risk of hemorrhagic transformation in stroke patients
Supplemental material, sj-docx-1-wso-10.1177_17474930251360519 for Association between time and severe hypoperfusion with risk of hemorrhagic transformation in stroke patients by Umberto Pensato, Nathaniel Rex, Nima Kashani, Amy YX Yu, Ashutosh P Jadhav, Joung-Ho Rha, Ajit S Puri, Paul Burns, Andrew M Demchuk, Michael D Hill, Mayank Goyal and Johanna M Ospel in International Journal of Stroke
Footnotes
Acknowledgements
None.
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: AY holds a Canada Research Chair (Tier 2) in Data-driven design of stroke systems; MG reports personal fees from Medtronic, Stryker, Microvention, and Mentice, during the conduct of the study, unrestricted research grants to University of Calgary from NoNO, Stryker, and Medtronic, patents for a system of acute stroke diagnosis, with royalties paid to GE Healthcare, and a system of simulation for acute neurointervention, with royalties paid to Mentice, and ownership interest in Circle Neurovascular; MDH reports grants from Canadian Institutes for Health Research, Alberta Innovates, and NoNO, for the conduct of the study, reports personal fees from Merck, reports non-financial support from Hoffmann-La Roche Canada; reports grants from Covidien (Medtronic), Boehringer-Ingleheim, Stryker, and Medtronic, outside the submitted work; reports a patent for systems and methods for assisting in decision-making and triaging for acute stroke patients, issued to US Patent office Number 62/086,077, owns stock in Calgary Scientific, is a director of the Canadian Federation of Neurological Sciences and Circle NeuroVascular, and has received grant support from Alberta Innovates Health Solutions, CIHR, Heart & Stroke Foundation of Canada, and the National Institutes of Neurological Disorders and Stroke; JMO is a consultant for Abbvie and Nicolab. All other authors declare no competing interests.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The ESCAPE-NA1 trial was supported by a grant from the Canadian Institutes of Health Research, by Alberta Innovates and NoNO.
Ethical approval
Ethics approval was obtained from the relevant ethics committees at all participating centers and regulatory approval was obtained as necessary.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.