
Abstract
Background:
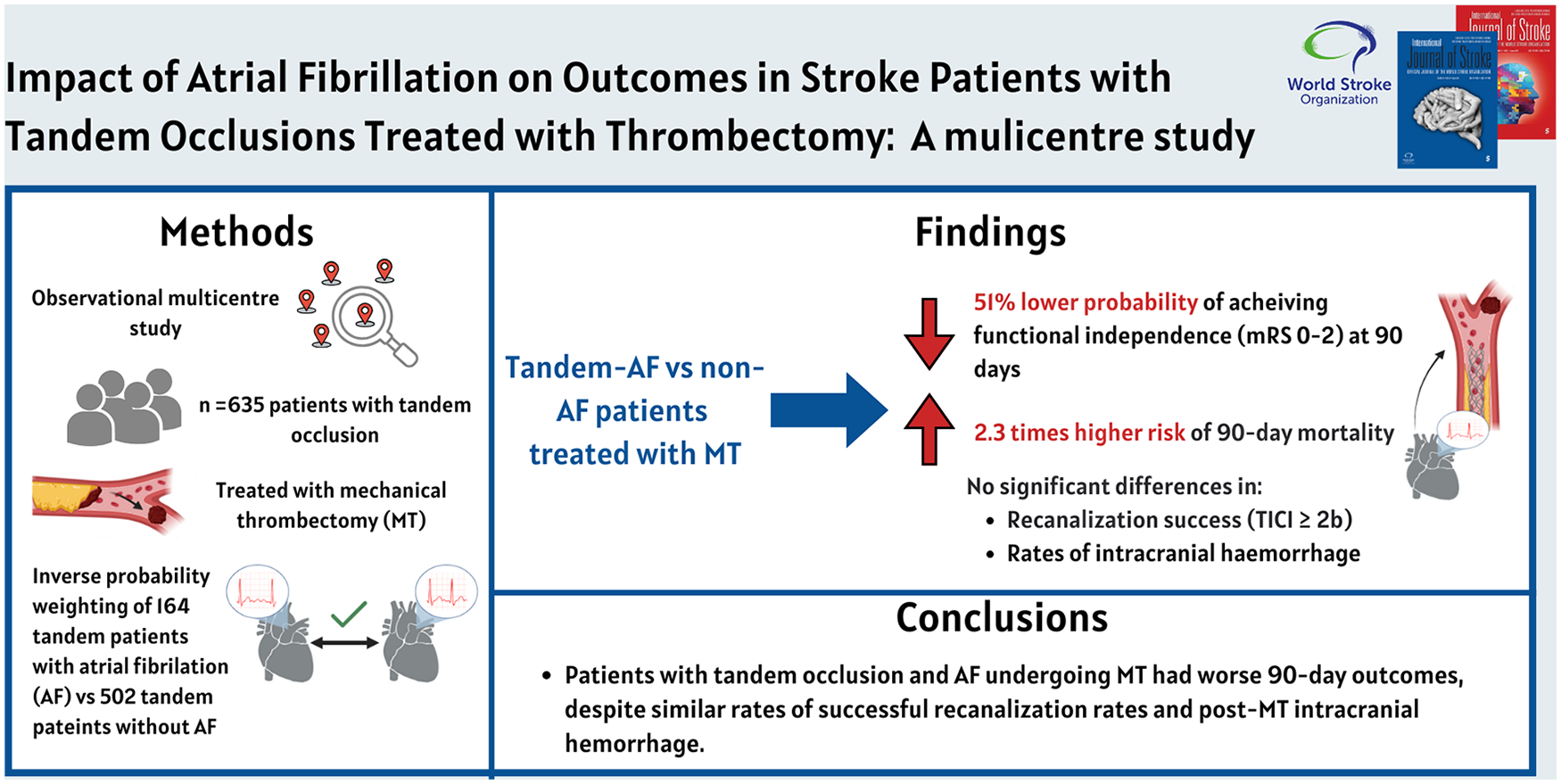
Tandem occlusions, involving simultaneous extracranial and intracranial artery blockages, represent a complex subtype of acute ischemic stroke treated with mechanical thrombectomy (MT). However, to date, the impact of atrial fibrillation (AF) on outcomes in this population remains unclear. This study aimed to evaluate the safety and efficacy of MT in patients with tandem occlusions, comparing those with AF to their counterparts without AF.
Methods:
We performed a multicentre, retrospective study using inverse probability weighting (IPW) to evaluate the effect of AF on outcomes in tandem occlusion patients treated with MT across three comprehensive stroke centers. The primary outcome was functional independence at 90 days (modified Rankin Scale [mRS] 0–2). Secondary outcomes included recanalization success (Treatment in Cerebral Infarction (TICI) ⩾ 2b), intracranial hemorrhage (ICH), symptomatic ICH (sICH), and 90-day mortality. Subgroup analyses assessed the interaction between AF and clinical or procedural factors.
Results:
Among 635 patients, 164 (25.8%) had AF (TandemAF). TandemAF patients had significantly lower rates of favorable 90-day functional outcomes (adjusted risk ratio [aRR] = 0.49; 95% confidence interval (CI): 0.31–0.76; p = 0.001) and higher 90-day mortality (aRR 2.29; 95% CI: 1.47–3.55; p < 0.001) compared to non-AF patients. Rates of successful recanalization, ICH, and sICH were similar between groups. Subgroup analysis revealed worse outcomes for TandemAF patients aged ⩾65 years, with National Institute of Health Stroke Scale (NIHSS) 11–42, and those treated with general anesthesia or intravenous thrombolysis.
Conclusions:
Patients with tandem occlusion and AF undergoing MT showed significantly worse functional and survival outcomes relative to their non-AF counterparts, despite comparable procedural success rates. These findings highlight the critical need for tailored management strategies to mitigate the unique risks associated with AF in this population. Further research is essential to refine therapeutic approaches and improve outcomes for this high-risk group.
Introduction
Tandem occlusions are defined as intracranial vessel occlusion with concomitant high-grade stenosis or occlusion of the ipsilateral cervical internal carotid artery (ICA) and occur in up to a third of all patients with stroke undergoing mechanical thrombectomy (MT) in the anterior circulation.1–3 Although MT is the standard of care for acute ischemic stroke resulting from anterior circulation tandem occlusions, this approach presents greater procedural complexity compared to isolated intracranial occlusions, as it involves the management of two distinct lesions, 4 the potential use of stent placement, and the consequent requirement for early initiation of antiplatelet therapy. 5 Furthermore, the absence of randomized controlled trials and the inconsistent findings from observational studies have left several critical questions unanswered regarding the optimal management of tandem occlusions. These gaps in evidence also contribute to the limited understanding of the predictive factors underlying poorer clinical outcomes in this population. 6
Atrial fibrillation (AF) is a major cause of acute ischemic stroke, accounting for approximately 20%–30% of all cases.7,8 While some data remain conflicting, evidence generally indicates that MT achieves similar 90-day functional outcomes and mortality rates in patients with and without AF. 9 In particular, AF detected after stroke demonstrated a positive association with functional independence in patients with stroke who underwent MT. 10 However, patients with AF undergoing MT frequently have higher rates of comorbidities compared to their non-AF counterparts, which may play a significant role in shaping long-term functional outcomes after the procedure. 11
To date, previous studies on post-MT outcomes in patients with acute LVO and AF have either excluded individuals with tandem occlusions or included them only in minimal proportions.11–13 Therefore, this has led to a significant paucity of robust data pertaining to this specific subgroup and to a considerable uncertainty regarding the implications of AF on outcome of acute ischemic stroke due to tandem occlusion. In this study, we investigated the impact of AF on outcomes of patients with anterior circulation tandem occlusions undergoing MT across three comprehensive stroke centers.
Methods
This is a multicentre, observational, investigator-initiated, post hoc analysis from prospective collected data from local registries, which included all acute stroke patients aged 18 years or older with anterior circulation tandem occlusion due to atherosclerosis or dissection consecutively treated with MT in three thrombectomy capable centers: Charing Cross Hospital, Imperial College Healthcare NHS Trust, London (UK); St George’s University of London, London (UK); Udine University Hospital, Udine (Italy) between 1 January 2021 and 30 March 2023 with local stroke registries available.14–16 These registries adhere to stringent data collection protocols, ensuring a high degree of completeness. As a result, the overall proportion of missing data in our dataset was minimal. To address missing data, we performed a complete case analysis, excluding cases with unavailable baseline characteristics or missing primary outcome information. Specifically, 17 patients were excluded due to missing baseline data, while 46 patients were excluded because the primary effectiveness outcome was not recorded or the patients were lost to follow-up, as reported in Figure 1 (study flow chart).

Study flow chart. ASPECTS: Alberta Stroke Program Early CT score; mRS: modified Rankin score.
Tandem lesion was defined as a proximal intracranial occlusion (intracranial occlusion of internal carotid artery (ICA) or of M1-M2 segments of the middle cerebral artery (MCA) and a cervical occlusion or stenosis ⩾ 50%). All patients underwent computed tomography (CT) of brain including CT angiography or magnetic resonance imaging (MRI) including MRI angiography. Intravenous thrombolysis (IVT) with intravenous tissue plasminogen activator (tPA) was administered in all patients who presented within 4.5 h of stroke symptom onset and without contraindications according to current guidelines. 17 All patients received MT of the intracranial occlusion with and without cervical ICA lesion intervention. The cervical ICA treatment approach was based on the operator’s preference based on patient vessel anatomy, clinical status, and operator experience. The decision regarding periprocedural antithrombotic management was made according to the protocol of each center. Both intracranial and extracranial occlusions were treated emergently at the same MT session. There was no standardized selection protocol for MT treatment, and patients were selected for MT based on the participating center protocol. Patients with tandem occlusion and AF (TandemAF) included those with previously known AF as well as those with newly detected AF identified in close temporal proximity to the index stroke during the hospital admission. Additional outpatient follow-up and monitoring were not included in this study. While additional outpatient monitoring might enhance detection rates, it was beyond the scope of this analysis. Ethical approval for this study was obtained from the institutional review boards of all participating centers. Given the retrospective nature of the study and the use of fully anonymized data collected as part of routine clinical care, informed consent was waived in accordance with local regulations. All data were handled in compliance with data privacy and protection standards, ensuring confidentiality and adherence to ethical guidelines. For the purpose of this analysis, the criteria for patients selection were: (1) age ⩾ 18 years; (2) Alberta Stroke Program Early CT score (ASPECTS) 5 or more; 18 (3) Intracranial occlusion of ICA or occlusion of M1-M2 segments of the MCA and a cervical occlusion or stenosis ⩾ 50%; and (4) pre-event modified Rankin Scale (mRS) score of 0 to 2.
Statistical analysis
Inverse probability weighting
To achieve balanced baseline characteristics between stroke tandem patients with (TandemAF) and without AF (Tandem), we applied Inverse Probability Weighting (IPW) to create a pseudo-matched cohort. Propensity scores were generated using a logistic regression model incorporating pre-defined baseline variables: age, sex, pre-stroke mRS, risk factors (hypertension, diabetes, hyperlipidemia, smoking status, prior TIA/ischemic stroke), pre-thrombectomy Alberta Stroke Scale Early CT Score (ASPECTS), previous use of antiplatelet treatment, large vessel occlusion characteristics (degree of extracranial carotid stenosis, site of distal occlusion), stroke severity (NIHSS at admission), and procedural features (onset to groin time, administration of intravenous thrombolysis, type of anesthesia, type of technique for distal thrombus thrombectomy, type of emergent carotid treatment, intraprocedural use of heparin, number of passes, periprocedural use of antithrombotic). Propensity scores were then used to assign inverse probability weights to each patient. To assess balance between groups, standardized mean differences (SMD) were calculated for each covariate. We also checked the overlap of propensity score distributions between groups to ensure sufficient comparability and applied stabilized weights to reduce the impact of extreme values and improve the reliability of the model.
Outcomes
The primary effectiveness outcomes were the 90-day favorable functional outcome, as defined by a modified Rankin Scale (mRS) score of 0 to 2, and the 90-day shift in patient mRS scores between patients with TandemAF and Tandem occlusion. The secondary effectiveness outcomes included favorable recanalization (post-procedural Treatment in Cerebral Infarction [TICI] score of 2b, 2c or 3), post-MT ordinal distribution of TICI scores, 24-h early neurological improvement and deterioration (⩾2 points decrease or increase in the NIHSS score from baseline, respectively), and 24-h median change in the NIHSS score from baseline. The safety outcomes were post-MT any intracerebral hemorrhage (ICH), as defined by any category of the Heidelberg bleeding classification system, 19 post-MT symptomatic hemorrhage (sICH) (any ICH causing ⩾ 4 points worsening on the NIHSS score), 90-day all-cause mortality. The occurrence of all outcomes was adjudicated by local investigators and validated by an expert neuroradiologist (for outcomes involving neuroimaging exam).
Statistical analysis
Categorical variables were reported as number and percentage, continuous variables as mean and SD or median and interquartile range (IQR), according to their distribution. For the primary effectiveness outcomes, we calculated the risk ratio and risk difference with 95% confidence intervals (CIs) for the 90-day occurrence of favorable mRS score between patients with TandemAF and Tandem occlusion. The 90-day shift of mRS scores was compared using an ordinal generalized linear model (GLM) and results were presented as odds ratio (OR) with 95% CIs. We applied a proportional odds model (cumulative logit), which is appropriate for the ordinal nature of the mRS categories. For the secondary effectiveness outcomes, risk ratios and differences between the two groups of patients were calculated for the occurrence of post-procedural favorable TICI score, 24-h early neurological improvement and deterioration. Changes in the 24-h NIHSS scores from baseline between patients with TandemAF and Tandem occlusion were compared using linear regression, and results were presented as OR and 95% CIs. The ordinal distribution of post-procedural TICI score was compared using chi-square test. For all the safety outcomes, we also calculated risk differences (RD) and risk ratios (RR) with 95% CIs between the sex groups, while the 90-day ordinal distribution of ICH categories was compared with chi-square test. All outcome analyses were performed separately in the unadjusted and adjusted cohorts for previous use of oral anticoagulant therapy.
Subgroup analysis of the primary effectiveness outcome in the weighted cohort was performed calculating differences between patients with TandemAF and Tandem occlusion in 12 prespecified subgroups (age [<65 years or ⩾65 years], NIHSS score at onset [0 to 5, 6 to 10, 11 to 42], ASPECTS [< 6 or ⩾ 6], hypertension, diabetes, sex, site of distal occlusion [carotid T, ICA + M1, ICA + M2], intravenous thrombolysis, onset to groin time [⩽ 360 min, > 360 min], type of anesthesia [general or local], thrombectomy technique for distal thrombus [stenting, aspiration, combined], treatment of emergent carotid [none, balloon angioplasty plus stenting, balloon angioplasty alone]). Finally, we used a GLM model with AF, subgroup variable, and their interaction term as independent variables to assess the homogeneity in the effect of sex by each subgroup variable. The p value was presented for the interaction term. As the outcomes of the present study were exploratory and there were no assumptions regarding the IPW analysis, a sample size was not prespecified for this analysis. All statistical analyses were performed using R software, version 4.2. Statistical significance was set at a p value < 0.05.
Results
Overall, a total of 635 patients were included in the analysis, of whom 164 (25.8%) were TandemAF while 471 (74.2%) were Tandem. Among the TandemAF group of patients, 131 (79.8%) had known AF while 33 (20.2%) had AF newly detected in close temporal proximity after the index stroke. The number of excluded patients with reasons is reported in the study flow chart (Figure 1). Weighted and unweighted baseline characteristics are summarized in Table 1. Overall, a satisfactory balance was achieved for all baseline variables which showed a standardized difference (SD) of propensity scores below 0.20. 20 Graphical representations of propensity scores and covariate balance distributions confirmed the overall quality of the matching process (Supplemental Figure 1 and 2). After applying IPW, a significant difference was observed between the two groups regarding the use of oral anticoagulant therapy prior to the index event (p < 0.001). Among the TandemAF group, 61 patients (37.2%) were receiving oral anticoagulation at the time of the index event, compared to only 16 patients (3.4%) in the Tandem group that were previously on treatment with oral anticoagulant because of previous deep venous thrombosis.
Baseline characteristics of the unmatched and matched cohorts.
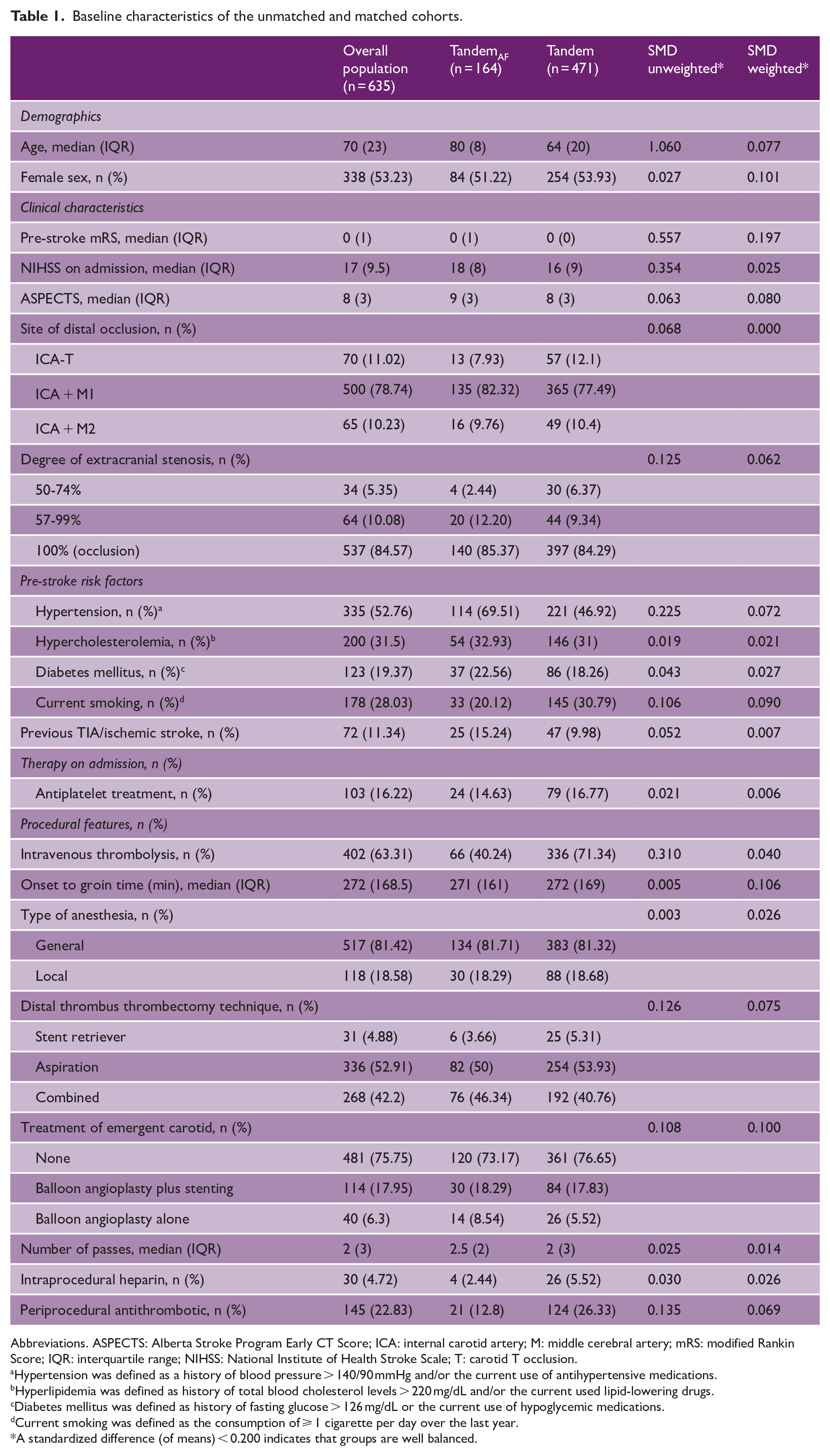
Abbreviations. ASPECTS: Alberta Stroke Program Early CT Score; ICA: internal carotid artery; M: middle cerebral artery; mRS: modified Rankin Score; IQR: interquartile range; NIHSS: National Institute of Health Stroke Scale; T: carotid T occlusion.
Hypertension was defined as a history of blood pressure > 140/90 mmHg and/or the current use of antihypertensive medications.
Hyperlipidemia was defined as history of total blood cholesterol levels > 220 mg/dL and/or the current used lipid-lowering drugs.
Diabetes mellitus was defined as history of fasting glucose > 126 mg/dL or the current use of hypoglycemic medications.
Current smoking was defined as the consumption of ⩾ 1 cigarette per day over the last year.
A standardized difference (of means) < 0.200 indicates that groups are well balanced.
Primary effectiveness outcome
The absolute rate of favorable functional outcome at 90 days (mRS, 0–2) was 25.6% in the TandemAF group and 40.6% in the Tandem group. This corresponded to an absolute risk difference of −14.94% (95% CI: −22.96 to −6.92, p < 0.001) in the unadjusted analysis and −16.21% (95% CI: −25.1 to −7.3, p < 0.001) in the adjusted analysis. There was a significant difference in the rate of favorable 90-day mRS score (0–2) (aRR = 0.49; 95% CI: 0.31 to 0.76; p = 0.001) and 90-day mRS distribution (aOR = 2.17; 95% CI: 1.54 to 3.13; p < 0.001) between TandemAF and Tandem groups of patients in the weighted cohort (Table 2) (Figure 2).
Outcomes comparison in the unmatched and matched cohorts.
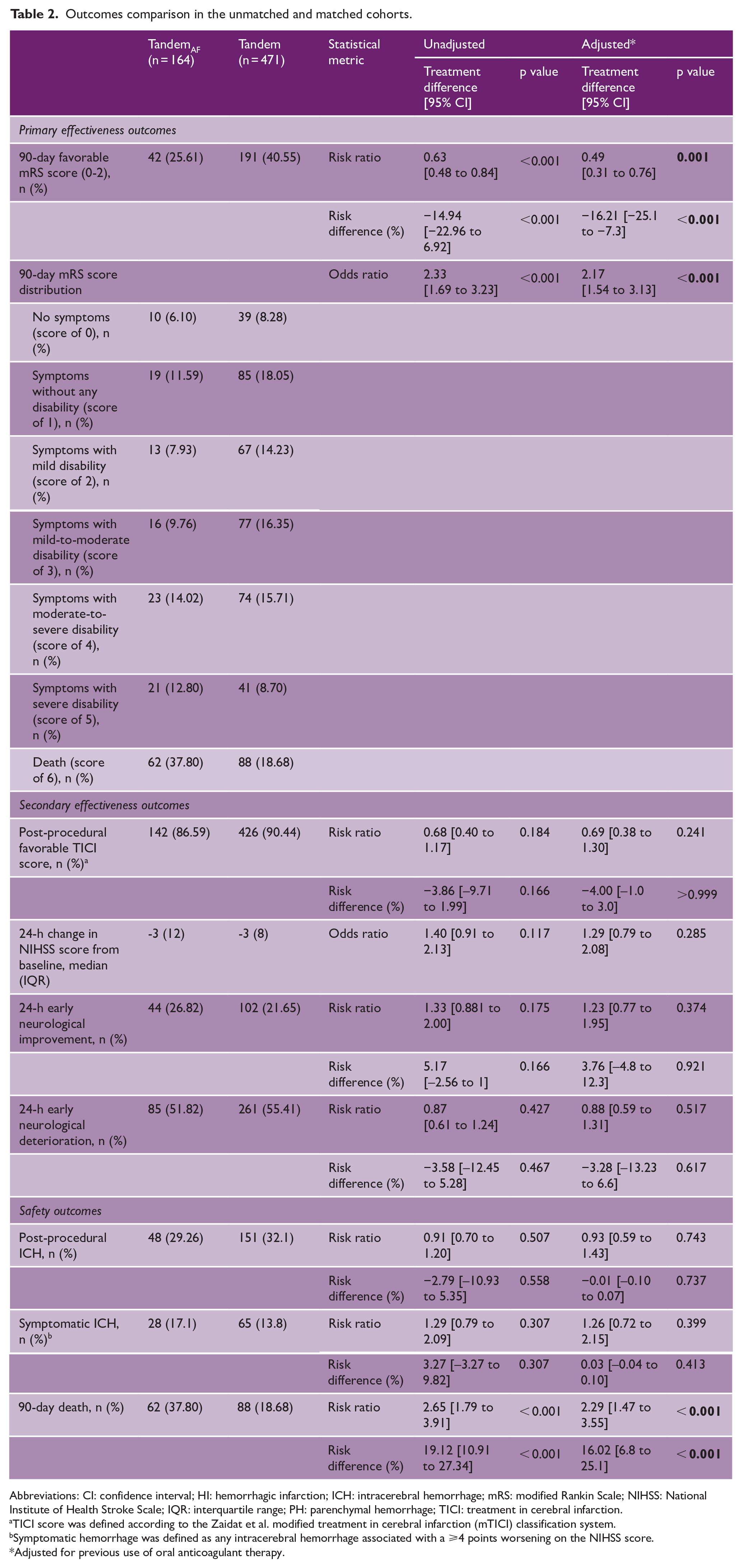
Abbreviations: CI: confidence interval; HI: hemorrhagic infarction; ICH: intracerebral hemorrhage; mRS: modified Rankin Scale; NIHSS: National Institute of Health Stroke Scale; IQR: interquartile range; PH: parenchymal hemorrhage; TICI: treatment in cerebral infarction.
TICI score was defined according to the Zaidat et al. modified treatment in cerebral infarction (mTICI) classification system.
Symptomatic hemorrhage was defined as any intracerebral hemorrhage associated with a ⩾4 points worsening on the NIHSS score.
Adjusted for previous use of oral anticoagulant therapy.
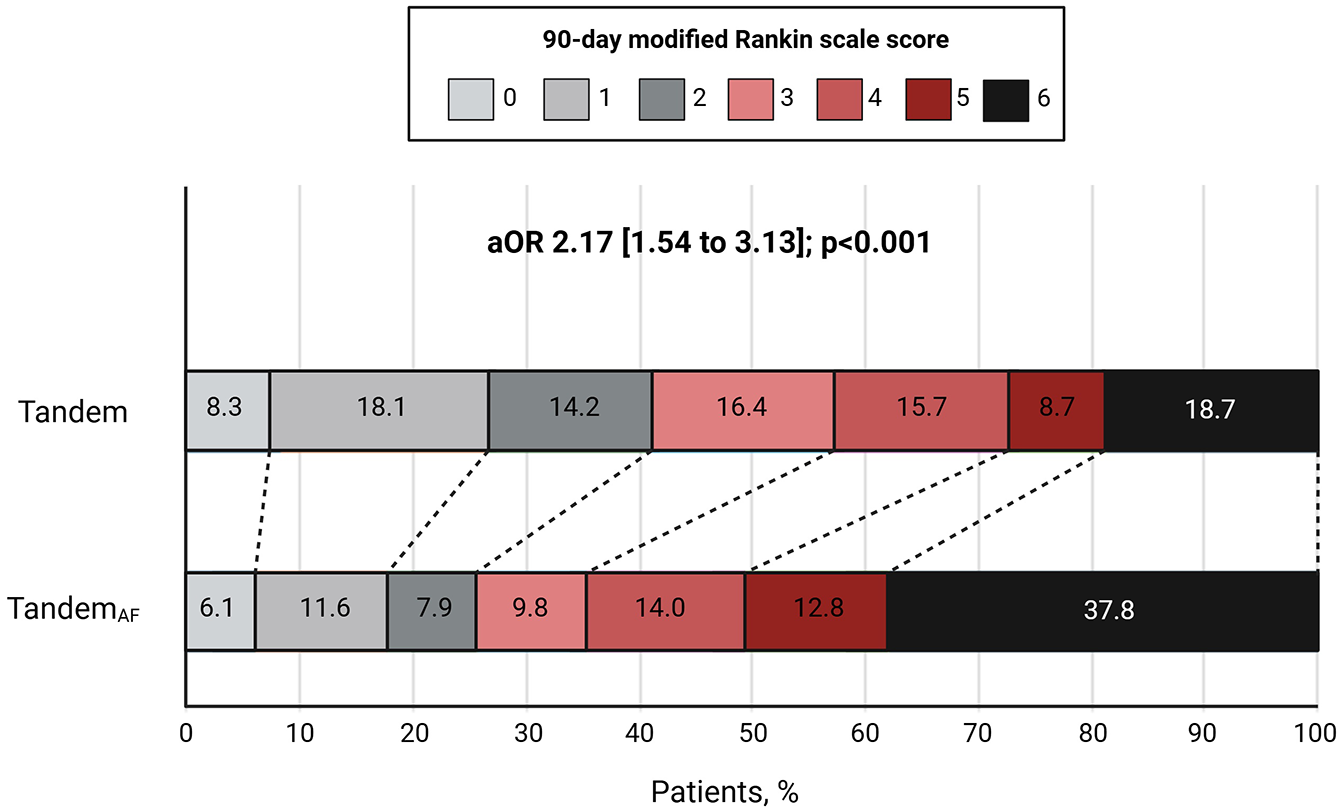
Ordinal mRS distribution between the two groups in the weighted cohort.
Secondary effectiveness outcomes
Our analysis did not show significant differences in the rate of post-procedural favorable TICI, 24-h change in NIHSS score from baseline, 24-h early neurological improvement and 24-h early neurological deterioration between TandemAF and Tandem groups of patients in the weighted cohorts (Table 2).
Safety outcomes
There were no significant differences in the risk of post-procedural ICH and sICH between the two groups of patients. However, we observed a significant difference in the rate of 90-day death (aRR = 2.29; 95% CI = 1.47 to 3.55; p < 0.001) between TandemAF and Tandem groups of patients in the weighted cohort (Table 2).
Subgroup analysis for the primary effectiveness outcome in the weighted cohort
Results of subgroup analysis for the primary effectiveness outcome in the weighted cohort are presented in Supplemental Table 1 and Figure 3. We observed a significantly lower rate of favorable 90-day mRS score (0–2) in TandemAF patients with age ⩾ 65 years (aRD = −10%; 95% CI = −19 to −1; p < 0.027), pre-stroke mRS score of 1 (aRD = −18%; 95% CI = −33 to −2; p = 0.044), NIHSS score on admission 11–42 (aRD = −13%; 95% CI = −21 to −5; p < 0.027), ASPECTS ⩾ 6 (aRD = −13%; 95% CI = −19 to −1; p < 0.027), with no history of diabetes (aRD = −14%; 95% CI = −23 to −5; p = 0.005), intracranial occlusion of M1 segment of the MCA (aRD = −14%; 95% CI = −22 to −5; p = 0.003), use of general anesthesia (aRD = −18%; 95% CI = −26 to −9; p < 0.001), treatment with intravenous thrombolysis (aRD = −22%; 95% CI = −33 to −11; p = 0.001), aspiration as distal thrombus thrombectomy technique (aRD = −16%; 95% CI = −27 to −6; p = 0.011), and balloon angioplasty plus stenting (aRD = −29%; 95% CI = −47 to −10; p = 0.004).
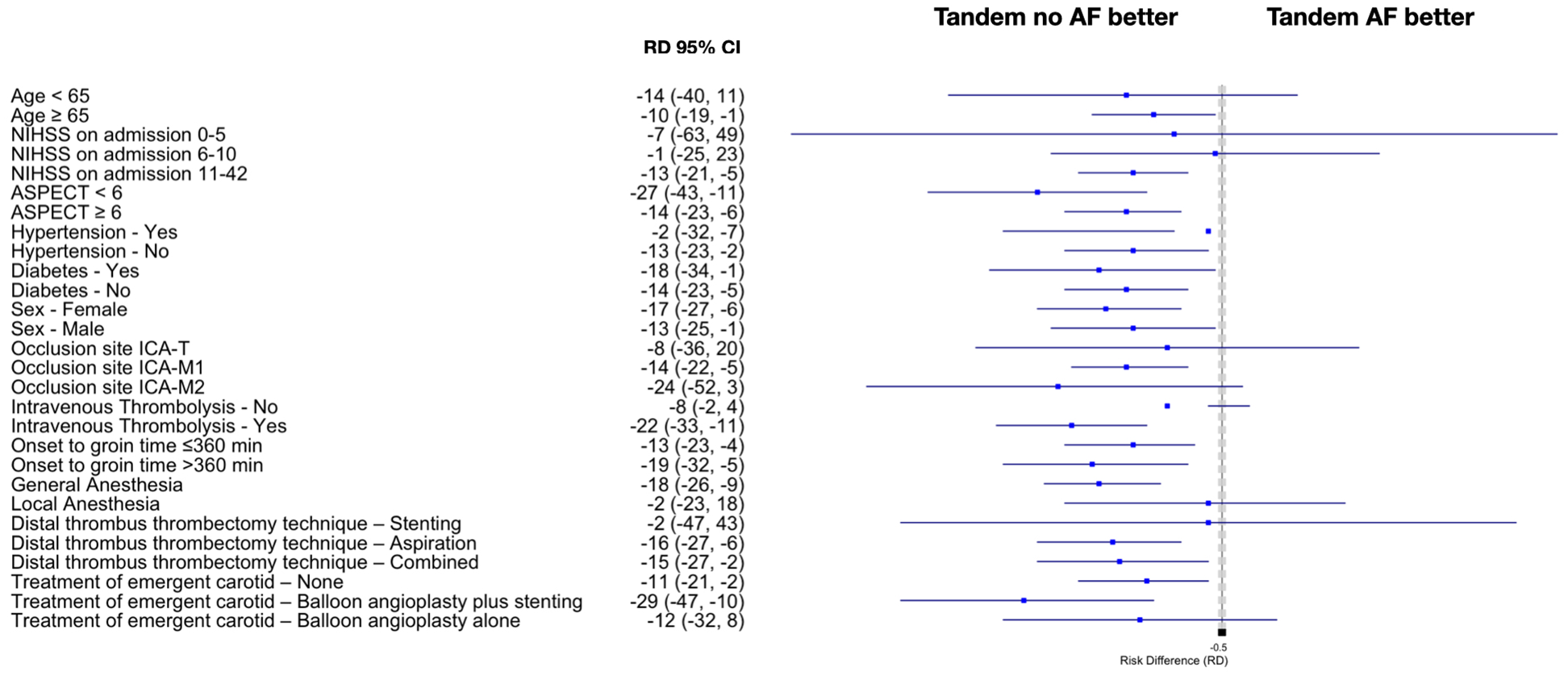
Subgroup analysis for the primary effectiveness outcome in the weighted cohort. ASPECTS: Alberta Stroke Program Early CT Score; CI: confidence interval; NIHSS: National Institute of Health Stroke Scale; RD: risk difference.
Discussion
Our multicenter study based on an IPW analysis showed significant difference in terms of functional independence at 90 days when we compared patients with TandemAF to their counterparts without AF. Moreover, TandemAF patients exhibited significantly increased risk of 90-day death relative to their non-AF counterparts. Interestingly, we did not observe a significant difference in terms of rate of successful recanalization and rate of post-procedural ICH, sICH between the two groups of patients before and after adjustment for previous use of oral anticoagulation. Furthermore, the subgroup analysis highlighted the significant impact of AF on 90-day functional outcomes. TandemAF patients showed consistently lower rates of functional independence, with notable disparities across specific demographic, clinical, and procedural subgroups. Overall, our findings underscore that, while procedural success and immediate complications appear comparable between groups, AF emerges as a predictor of long-term functional and survival outcomes in patients undergoing MT for tandem occlusion.
Previous studies have produced conflicting results on the post-MT outcomes in acute LVO stroke patients with AF and their counterparts without AF. 9 An individual patient data analysis of six randomized clinical trials21–26 involving 1351 patients of which 447 (33.1%) with AF showed no significant correlation between the presence of AF and outcome of MT. 12 Kobeissi et al. 11 performed a systematic review and meta-analysis including 10 studies with 6543 patients. After sensitivity analysis the rate of mRS scores of 0 to 2 was significantly lower among patients with AF. Furthermore, the authors documented that mortality was significantly higher in the AF group with no significant heterogeneity observed. However, it is noteworthy that these prior studies either excluded patients with tandem occlusions entirely or included them only in minimal proportions.
Few studies have previously investigated predictors of good functional outcomes in patients with tandem occlusion, primarily through analyses of demographics, clinical, and radiological data.27–33 Notably, AF has not been identified as a predictor of outcomes in these studies, highlighting the need for further investigation in this specific population. However, these studies often employed different design limiting their generalizability compared to the approach used in our study. In our analysis we obtained that TandemAF patients had significantly lower rates of favorable 90-day functional outcomes and increased rate of 90-day death compared to patients without AF. Although we use an IPW analysis to match for baseline characteristics between the two groups, our findings highlight the detrimental effect of AF on recovery and long-term disability following MT, which may be attributed to a combination of factors, including greater comorbidity burden. Moreover, patients with AF also tend to be older11,34 and this trend held true in our analysis, with TandemAF patients had a median age of 80 years compared to 64 of their counterparts without AF. Furthermore, our subgroup analysis indicated that patients with a pre-stroke mRS of 1 had significantly lower rates of favorable 90-day functional outcomes in the atrial fibrillation group. This finding suggests that even in patients with minimal pre-stroke disability, AF may negatively influence post-thrombectomy recovery. As a population, patients with AF tend to have higher rates of comorbidities, including hypertension, dyslipidemia, heart failure, diabetes, asthma, chronic obstructive pulmonary disease, history of myocardial infarction, arrythmia (other than AF), and valvular heart disease that could impact on the worse outcome observed. We hypothesize that the combination of advanced age, greater comorbidity burden likely contributed to the poorer recovery and increased mortality observed in TandemAF patients, instead of AF itself contributing to the worse outcomes. These results highlight the need for tailored management strategies to address the unique risks associated with AF in this high-risk population.
Interestingly, our analysis revealed comparable rates of successful reperfusion, post-procedural ICH and sICH between the two groups of patients before and after adjustment for previous use of oral anticoagulation. To the best of our knowledge, no previous studies have evaluated the effectiveness and safety of MT in this patient population. These findings are important because they provide context for the worse outcomes observed in patients with TandemAF compared with patients without AF. As the immediate procedural outcomes were comparable between groups, the 90-day worse outcomes in patients with AF cannot be attributed to rates of technical success or post-procedural bleeding. Thus, there are several possible explanations for the differences in functional outcomes. Instead, there are likely to be driven by the broader clinical context, including baseline characteristics and peri-procedural management, that plays a more substantial role in influencing long-term outcomes among patients with AF.
Finally, our subgroup analyses revealed that the negative association between AF and favorable outcomes was particularly pronounced in specific patient groups. Older patients (⩾65 years), those with higher admission NIHSS scores (11–42) had significantly worse outcomes in the TandemAF cohort. In addition, procedural characteristics, such as the use of general anesthesia, intravenous thrombolysis, aspiration thrombectomy, or balloon angioplasty with stenting, were associated with significantly lower rates of favorable outcomes in patients with AF. These findings underscore the need to consider both patient- and procedure-specific factors when managing tandem occlusions in the context of AF.
Several limitations of this study warrant consideration. First, as a retrospective analysis, our findings are subject to inherent biases, including unmeasured confounding, despite the use of IPW. Second, heterogeneity in procedural techniques and peri-procedural care across participating centers may have influenced the observed outcomes and limited the generalizability of the results. Finally, while IPW improved baseline balance, it did not account for all comorbidities, such as respiratory conditions and other factors that are typically more prevalent in AF patients, potentially contributing to the observed outcome disparities.
In conclusion, this study demonstrates TandemAF patients exhibiting worse functional and survival outcomes compared to their counterparts without AF. These findings highlight the need for individualized management strategies to optimize outcomes in this high-risk population. A key consideration is the optimal antithrombotic regimen after MT. While oral anticoagulation is the standard for stroke prevention in stroke patients with AF, the role of dual therapy with anticoagulation plus antiplatelets remains uncertain, particularly in the early post-thrombectomy phase. Balancing the risk of recurrent thromboembolism with the potential for hemorrhagic complications is critical, and future studies should clarify whether combination therapy offers additional protection without increasing bleeding risk and further exploring the mechanisms underlying the observed outcome disparities.
Supplemental Material
sj-docx-3-wso-10.1177_17474930251330139 – Supplemental material for Impact of atrial fibrillation on outcomes in stroke patients with tandem occlusions treated with thrombectomy: A multicentre study
Supplemental material, sj-docx-3-wso-10.1177_17474930251330139 for Impact of atrial fibrillation on outcomes in stroke patients with tandem occlusions treated with thrombectomy: A multicentre study by Lucio D’Anna, Matteo Foschi, Mariarosaria Valente, Liqun Zhang, Nina Mansoor, Matthew Fallon, Adelaida Gartner Jaramillo, Fedra Kuris, Antonio Taglialatela, Francesco Toraldo, Filippo Komauli, Massimo Sponza, Vladimir Gavrilovic, Kyriakos Lobotesis, Gian Luigi Gigli, Soma Banerjee and Giovanni Merlino in International Journal of Stroke
Supplemental Material
sj-jpeg-1-wso-10.1177_17474930251330139 – Supplemental material for Impact of atrial fibrillation on outcomes in stroke patients with tandem occlusions treated with thrombectomy: A multicentre study
Supplemental material, sj-jpeg-1-wso-10.1177_17474930251330139 for Impact of atrial fibrillation on outcomes in stroke patients with tandem occlusions treated with thrombectomy: A multicentre study by Lucio D’Anna, Matteo Foschi, Mariarosaria Valente, Liqun Zhang, Nina Mansoor, Matthew Fallon, Adelaida Gartner Jaramillo, Fedra Kuris, Antonio Taglialatela, Francesco Toraldo, Filippo Komauli, Massimo Sponza, Vladimir Gavrilovic, Kyriakos Lobotesis, Gian Luigi Gigli, Soma Banerjee and Giovanni Merlino in International Journal of Stroke
Supplemental Material
sj-jpeg-2-wso-10.1177_17474930251330139 – Supplemental material for Impact of atrial fibrillation on outcomes in stroke patients with tandem occlusions treated with thrombectomy: A multicentre study
Supplemental material, sj-jpeg-2-wso-10.1177_17474930251330139 for Impact of atrial fibrillation on outcomes in stroke patients with tandem occlusions treated with thrombectomy: A multicentre study by Lucio D’Anna, Matteo Foschi, Mariarosaria Valente, Liqun Zhang, Nina Mansoor, Matthew Fallon, Adelaida Gartner Jaramillo, Fedra Kuris, Antonio Taglialatela, Francesco Toraldo, Filippo Komauli, Massimo Sponza, Vladimir Gavrilovic, Kyriakos Lobotesis, Gian Luigi Gigli, Soma Banerjee and Giovanni Merlino in International Journal of Stroke
Footnotes
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: S.B. is a key opinion leader for RAPIDAI. All other authors have no conflicts of interests.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was partially funded by the Graham-Dixon charity.
Ethical approval
This study has obtained approval from the UK Health Regulator Authority (HRA) (HRA Reference No.: 275260). The study has also received confirmation of capacity and capability from the Imperial College Healthcare NHS Trust.
Informed consent
Informed consent was not a legal requirement as the research was carried out using data collected as part of routine care and any researchers outside the direct care team only had access to anonymized data.
Data availability
Data available upon reasonable request.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.