
Abstract
Background:
Falls are common after stroke and can have serious consequences such as hip fracture. Prior research shows around half of individuals will fall within the 12 months post stroke, and these falls are more likely to cause serious injury compared to people without stroke. However, there is limited research on risk factors collected in the immediate post-stroke period that may relate to falls risk. Furthermore, the circumstances and consequences surrounding falls resulting in serious adverse events (serious falls) is underexplored.
Aims:
Using longitudinal cohort data from A Very Early Rehabilitation Trial (AVERT), we aimed to describe the occurrence, consequences, and circumstances of serious falls over 12 months post stroke and examine potential risk factors associated with these serious falls.
Methods:
Data from participants included in the AVERT trial (n = 2104; recruited from 56 stroke units across five countries) were analyzed. Serious falls were defined as those resulting in death, were life threatening, or required/prolonged hospitalization. Baseline variables included: demographics, pre-morbid function, stroke severity, hemi-neglect, functional independence, and mobility. Statistical analysis included Wilcoxon-Mann–Whitney tests, Fisher’s tests, and Firth’s logistic regressions (adjusting for age, stroke severity, and AVERT intervention group).
Results:
Of the 2104 participants, 85 (4%) experienced at least one serious fall (mean age 78.1 years, 45 male), with 91 individual falls. Fifty-five (60%) serious falls resulted in fracture, with 23 (42%) being hip fractures. Two (2%) falls resulted in death. Serious falls were most common during the day (26 of 38 reported), at home (30 of 63 reported) and while ambulating (22 of 42 reported). More serious falls were experienced by participants who were older, had worse pre-morbid mobility, were unable to walk 10 m independently in the first 24 hours post stroke, or required longer than 14 days to walk 50 m unassisted.
Conclusion:
This large international prospective study found 1 in 25 stroke survivors experienced serious falls in the first year after stroke. Fractures were a common outcome of these falls, but the true post-stroke fracture rate is likely to be underestimated due to our study methods, such as the exclusion of individuals with poor pre-morbid mobility and the absence of data on fractures not relating to falls or leading to an inpatient hospital admission. Clear associations between older age, impaired pre- and early post-stroke mobility and heightened risk of serious falls were found. Integrating these factors into post-stroke screening tools could improve identification of individuals at greater risk of serious falls and lead to more focused rehabilitation and injury prevention.
Introduction
Falls are common in people after stroke, with 37–73% of individuals falling within the first 6 months.1,2 Falls incidence in people with stroke is higher compared to the general older adult population, 3 and these falls are more likely to have serious consequences.1–4 People with stroke have an incidence of fractures from falls ranging from 1% to 9%,5–8 a two- to seven-fold increase compared to the general older adult population.9–11 Furthermore, people with stroke have a two- to four-fold increase in the proportion of hip fractures.3,12,13 This may be due to decreased weight bearing on the stroke-affected side 13 leading to hemiosteoporosis,1,8 coupled with increased falls toward the paretic side.2,10,14 Hip fractures are a serious complication associated with higher medical costs, greater disability, and more deaths than all other fractures combined. 10 Concerningly, individuals with stroke who sustain hip fractures are less likely to return to pre-morbid independence and have a higher mortality than their non-stroke counterparts.10,11 Thus, it is imperative to identify factors contributing to these injurious falls.
Limited evidence details the timing and circumstances of falls post stroke, particularly for injurious falls. Falls are more common early after stroke, with around half of the falls in the initial 6 months happening within 2 months post-hospital discharge. 15 In addition, half of stroke patients have been shown to experience falls within the first 3 weeks of inpatient rehabilitation. 7 Although the incidence of falls after stroke decreases over time, 16 existing literature mostly examines falls incidence at an average of 2–7 years post stroke4,5,17 and focusses more on higher-functioning populations (e.g. those able to independently ambulate). 4 There is a paucity of research related to individuals with greater impairment who have fallen in the early post-stroke period. Evidence suggests most post-stroke falls occur during the day in the home environment,4,5,12 but little is known about the specific circumstances of injurious falls, particularly serious injuries.
Evidence regarding factors associated with post-stroke falls is equivocal. A systematic review identified impaired mobility, use of sedative or psychotropic medications, lower mood, and impaired cognition as significant predictors. 18 In addition, pre-stroke decreased functional status has been reported as a prominent risk factor 19 along with increased age.20–24 There is little consensus around the impact of hemi-neglect11,23,24 as a risk factor. Factors related to serious falls are relatively underexplored, with some evidence suggesting female sex and falls history being associated with greater risk of post-stroke fracture.8,20,22 Being aware of factors predisposing to injurious falls may allow more focussed rehabilitation and care for individuals who are at risk.
Aims and hypotheses
Our study used data collected from AVERT, 25 a large (n = 2104) multicentre stroke trial. Prior AVERT trial publications have only reported on falls resulting in death within the first 3 months (n = 2) and falls resulting in a serious adverse event (SAE; hereafter referred to as “serious falls”) within the first 14 days (n = 6). 26 We aimed to investigate the occurrence, consequences, and circumstances of serious falls from stroke onset to 12 months after stroke. In addition, we aimed to examine the association between serious falls and baseline variables related to participant demographics, pre-morbid independence, stroke details and post-stroke impairment, and physical function. We hypothesized that individuals who were older and had worse pre- and post-stroke physical function would have greater risk of serious falls.
Methods
Participants
Participants in this study were enrolled in the AVERT trial. 25 This was a large parallel-group, single-blind randomized controlled trial conducted across 56 stroke units in five countries (Australia, New Zealand, Malaysia, Singapore, and the United Kingdom) between July 2006 and October 2014. Ethics approval for AVERT was obtained from institutional review boards at all participating sites. Additional ethics approval for this analysis was received from The University of Melbourne Human Research Ethics Committee (2022-23716-27936-3).
Participants aged 18 years or older, who presented to a stroke unit within 24 hours of a first or recurrent stroke were eligible. Management with thrombolysis was allowed. Exclusion criteria were: clinically significant pre-morbid (i.e. pre-stroke) levels of disability (Modified Rankin Scale score (mRS) > 2), rapid deterioration requiring direct admission to an intensive care unit, palliation treatment or immediate surgery, concurrent diagnosis of rapidly deteriorating disease, subarachnoid hemorrhage, unstable coronary condition, lower limb fracture at time of stroke preventing participation in the early mobilization intervention, no response to voice, systolic blood pressure <110 mmHg or >220 mmHg, oxygen saturation <92% with supplementation, resting heart rate <40 bpm or >110 bpm, temperature >38.5, or enrolment in another intervention trial. The AVERT intervention focussed on early mobilization, implementing rehabilitation strategies to encourage early out of bed activity within 24 hours of stroke onset. The intervention lasted for 14 days or until the participant was discharged from the unit, whichever was sooner. Specifics of the intervention have been described elsewhere. 25
Primary outcome of interest: falls resulting in serious adverse events
Falls reported as SAEs were collected over 12 months following stroke. The AVERT trial used the standard definition for reporting of SAEs in a clinical trial: events that resulted in death, were life threatening (i.e. an immediate risk of death at the time of the event such as head trauma); required inpatient hospitalization (i.e. admission for any cause, excluding emergency room visits or outpatient facility admission), or prolongation of hospitalization (i.e. any event that occurs while patient is already in hospital which in itself prolongs the hospital stay in the opinion of the investigator); or an event that resulted in persistent or significant disability (considered significant by the investigator but does not meet any above recording criteria—e.g. diagnosis of significant cancer or permanent loss of mobility/cognitive function without a hospital admission). Non-serious falls were classified as important medical events (IMEs) and also recorded until 3 months post stroke.
All events were identified and evaluated by the AVERT medical, physiotherapy, and nursing staff if they occurred during the intervention period. Outside of the AVERT trial intervention period, blinded assessors arranged in-person assessments at 3 and 12 months (±7 days) by contacting the participant, their relatives, or their rehabilitation or accommodation units. At these assessments, review of medical records and detailed patient interview were performed to assess for SAEs. All events were reported in case report forms and documented in the participant’s medical record. If a participant was unable to attend an assessment due to illness, death or other reasons, the blinded assessor still made every effort to collect relevant data by contacting family members or care facilities and reviewing medical records. Serious adverse events, including falls, were reported to the AVERT office following each assessment.
Independent variables of interest
A list of variables with potential relationships to falls risk based on prior literature were examined.2,4,11 Demographic factors included: age at stroke onset; sex; pre-morbid disability assessed using the mRS (mRS 0–2 only, as per AVERT inclusion criteria); 25 and pre-morbid gait aid use. Stroke-related factors collected within 24 h of onset were stroke type (ischaemic, haemorrhagic); lesion side; Oxfordshire Community Stroke Project (OCSP) 27 classification, stroke severity (National Institutes of Health Stroke Scale, NIHSS); 28 mobility (Mobility Scale for Acute Stroke, MSAS); 29 hemi-neglect (NIHSS score 1-2), 30 and the use of thrombolysis.31,32 The other variable of interest was the AVERT trial group allocation (intervention or control).
Statistical analysis
Descriptive statistical analysis was conducted for the occurrence, consequences, and circumstances of serious falls. This included injury type, location, time, and activity surrounding the fall. Time of fall was categorized into three periods (day: 6 am–5:59 pm, evening 6 pm–10:59 pm and overnight 11 pm–5:59 am) as we believe this best captures falls after waking from sleep in comparison to evening falls.
As records of serious falls were derived from SAE records and a total of 67 participants in the trial were lost to follow-up at 12 months (with unknown time of loss of follow-up), exposure time could not be reliably estimated for participants that did not have any adverse events. We therefore considered the presence or absence of serious falls, and did not consider frequency of falls. Independent characteristics of interest for participants who did and did not sustain serious falls (the latter group included participants who sustained non-serious falls and those without any falls) were compared using Fischer exact and Wilcoxon-Mann–Whitney tests. Due to the relatively low incidence of serious falls, Firth’s logistic regression was used to estimate the associations between each independent variable and serious falls. 33 All regression analyses were adjusted for age and stroke severity (NIHSS), as per the original trial, 25 as well as AVERT trial group allocation. 33 Where one of these three variables was investigated, it was not adjusted for itself (i.e. estimated associations of age and serious falls do not adjust for age).
Results
Participant characteristics and occurrence of serious falls
The mean age of the 2104 AVERT trial participants was 70.6 (12.8) years and 1286 (61%) were male. Over 12 months post-stroke, there were 91 individual serious falls reported. Eighty-five participants (4%) experienced one or more serious falls. The mean age of participants who experienced serious fallers was 78.1 (9.7) years, and 45 (53%) were male. Participant characteristics are summarized in Table 1. Serious falls in the first 12 months occurred at a median (interquartile range [IQR]) 175 (82, 279) days post stroke (range 3–359 days) and most commonly within the community setting (Figure 1).
Participant demographics, stroke-related characteristics, and trial group allocation.
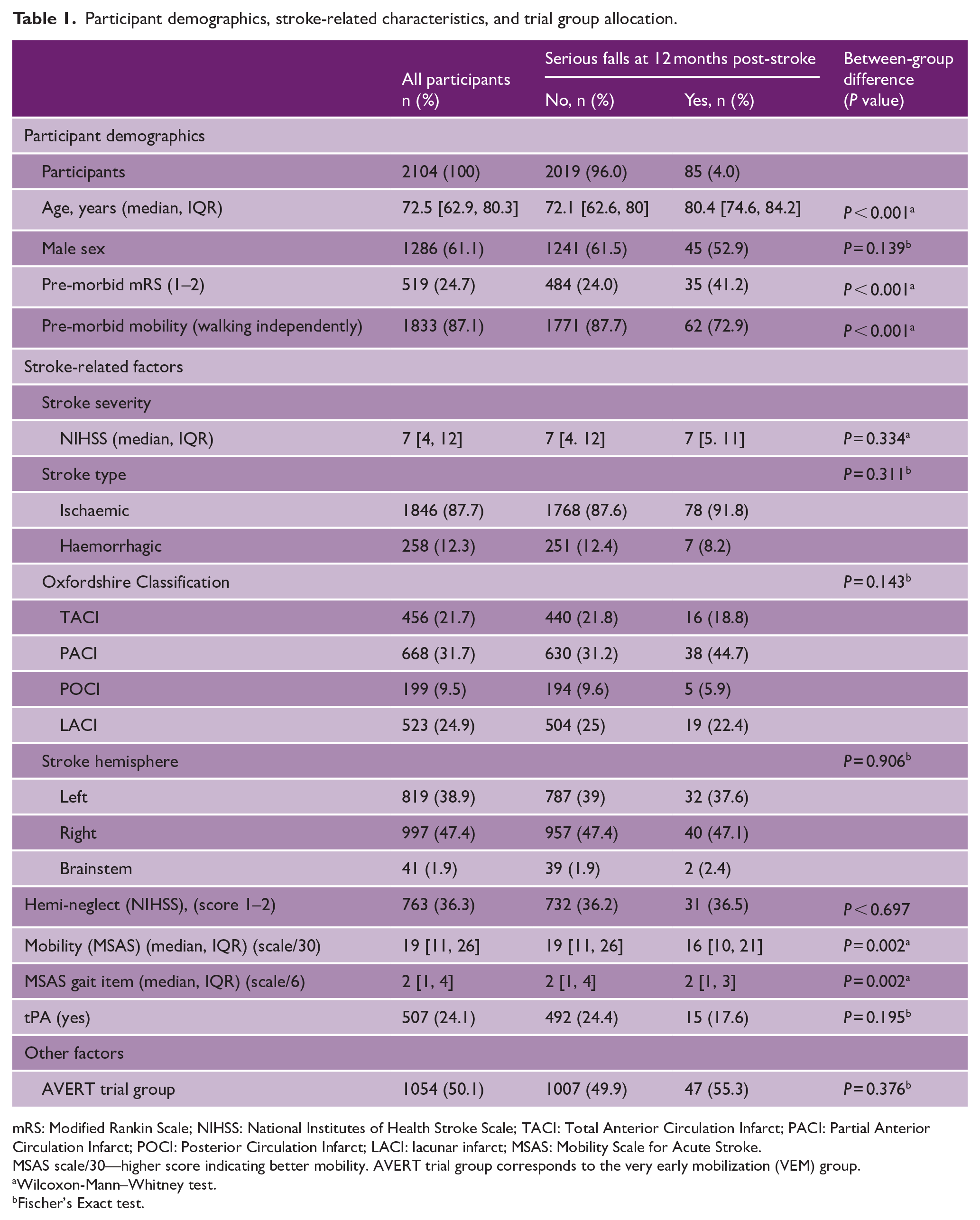
mRS: Modified Rankin Scale; NIHSS: National Institutes of Health Stroke Scale; TACI: Total Anterior Circulation Infarct; PACI: Partial Anterior Circulation Infarct; POCI: Posterior Circulation Infarct; LACI: lacunar infarct; MSAS: Mobility Scale for Acute Stroke.
MSAS scale/30—higher score indicating better mobility. AVERT trial group corresponds to the very early mobilization (VEM) group.
Wilcoxon-Mann–Whitney test.
Fischer’s Exact test.
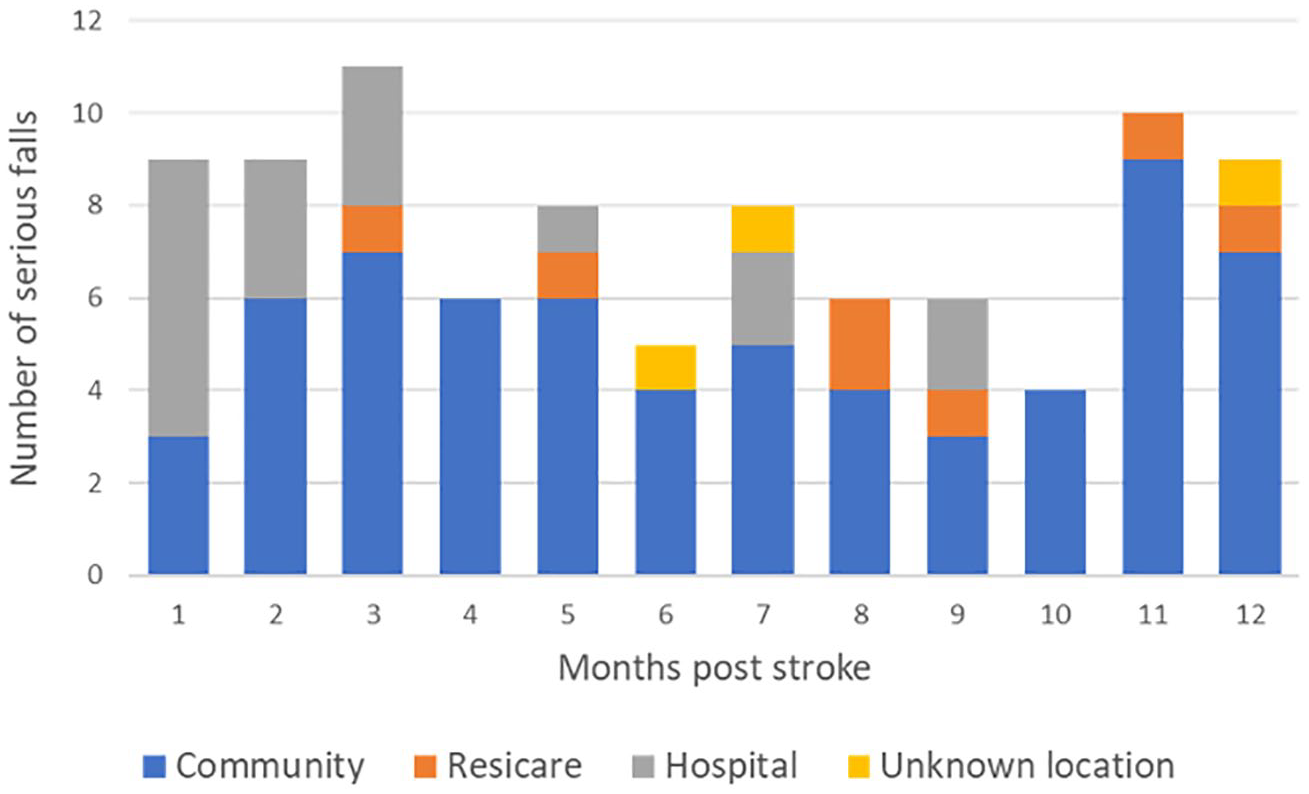
Distribution of serious falls over time.
Consequences of serious falls
The most common serious adverse event category of the 91 serious falls was “required hospitalisation” (n = 76, 84%). This was followed by “prolonged hospitalisation” (n = 9, 10%), “resulted in significant disability” (n = 4, 4%), and “resulted in death” (n = 2, 2%). Of the 91 serious falls, 55 (60%) resulted in fracture (n = 23, 42% hip fractures; n = 6, 11% being rib fractures), 17 (19%) resulted in head injury (ranging from soft tissue injury to subdural hemorrhage), and 12 (13%) resulted in soft tissue injury (necessitating hospitalization). Two participants died after falling due to subdural hemorrhage. One fatal fall occurred at 8 days post-stroke (85 year-old male, fall in hospital, not thrombolysed), and the other at 41 days post-stroke (84 year-old male, fall in hospital 11 days after a prior serious fall at home, not thrombolysed). Of 46 serious falls with injury side reported, 34 (74%) sustained injuries on their stroke-affected side. Of the 20 hip fractures with injury side reported, 13 (65%) occurred on the stroke-affected side.
Circumstances surrounding serious falls
Complete information about the time, location, and mechanism of serious falls was not available for all participants. Of the 63 serious falls with location reported, 30 (48%) occurred at home, 17 (27%) in the hospital, 8 (13%) outdoors, and 7 (11%) in a residential care setting. Of the 38 serious falls with time of fall reported, 26 (68%) occurred during the day (6 am–5:59 pm), 11 (18%) in the evening (6–10:59 pm), and 8 (13%) overnight (11 pm–5:59 am). Of the 42 serious falls with circumstances surrounding fall reported, 22 (52%) occurred while ambulating or standing, 14 (33%) while transferring, 11 (26%) while toileting, and 6 (14%) under other circumstances (e.g. fall from lying or seated position). It is important to note that eight of the serious falls relating to toileting occurred while ambulating and three occurred while transferring, and these were also included in their respective categories.
Factors associated with serious falls
When comparing those individuals who experienced at least one serious fall to all other individuals, older age (serious falls median 80.4 versus 72.1, P < 0.001), lower MSAS (median 16 versus 19, P = 0.002), worse pre-morbid mRS (P < 0.001), worse pre-morbid mobility (P < 0.001), and inability to independently walk 10 m within 24 hours of stroke (P = 0.009) were significantly associated with increased risk of serious falls (Table 1).
Age was significantly associated with serious falls with the odds of a serious fall increasing by 6.46% (odds ratio [OR] 95% confidence interval [CI]: 1.04–1.09) for every additional year. NIHSS and AVERT trial group were not associated with serious falls (OR 1.00, 95% CI: 0.97–1.04 and OR 1.24, 95% CI: 0.80–1.92, respectively). An increased risk of serious falls was associated with decreased mobility within 24 hours post stroke as assessed with the MSAS total scale (OR 0.94, 95% CI 0.90–0.97), with the gait item of the MSAS indicating those requiring assistance or supervision to walk 10 m (OR 4.51, 95% CI: 1.19–40.30) and those unable to walk (OR 6.39, 95% CI: 1.59–58.35) being more prone to serious falls compared to those able to walk independently. In addition, individuals who took more than 14 days to gain the ability to walk 50 m without physical assistance were also shown to be at greater risk of serious falls compared to those able to independently walk within the first 2 days. These results are summarized in Figure 2.
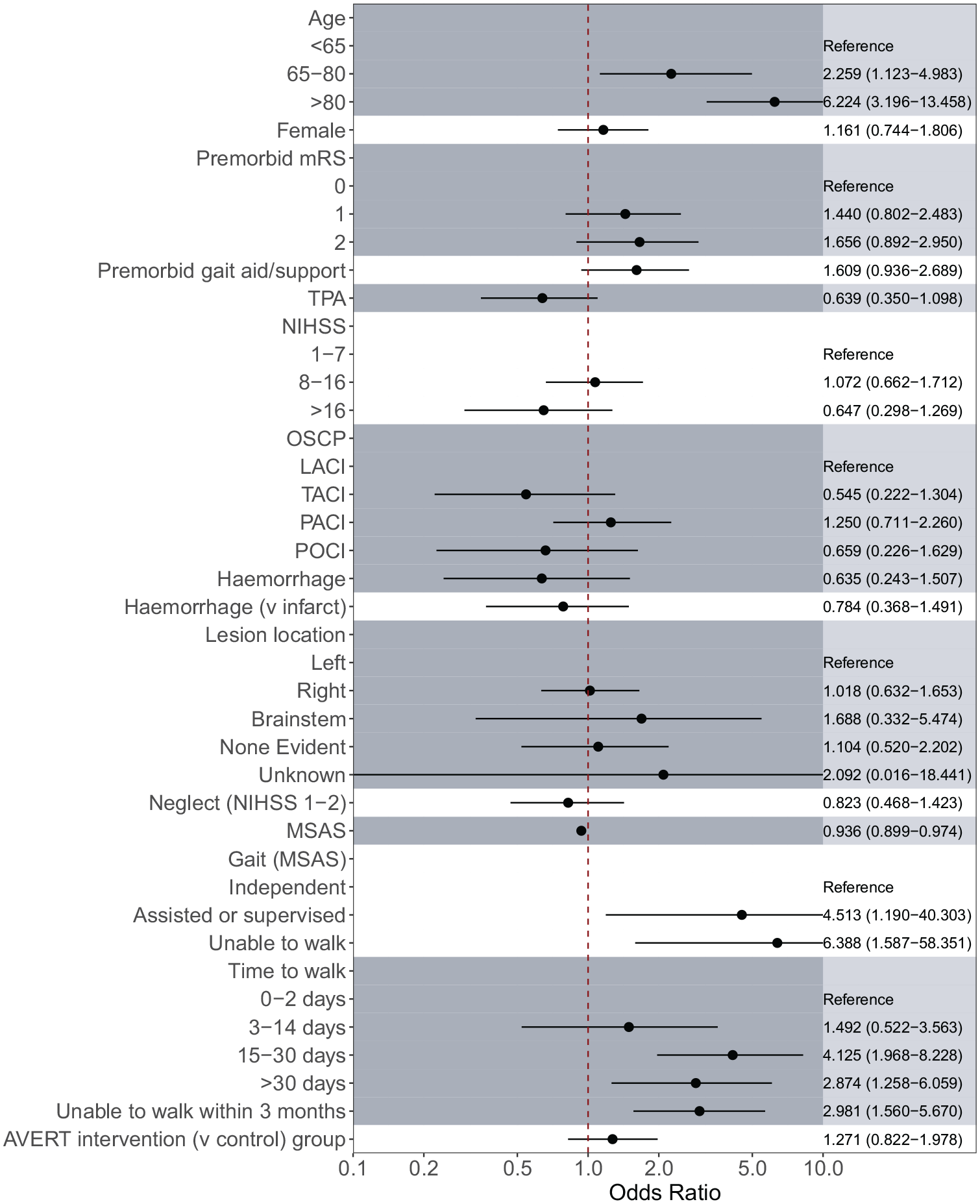
Associations between independent variables and serious falls, adjusted for age, NIHSS, and AVERT treatment arm using Firth’s logistic regression.
Discussion
This large international study provided a unique opportunity to identify serious falls risk. We demonstrated that in the first 12 months after stroke 4% of individuals experienced serious falls. Based on an exposure of 12 months per participant, the incidence of serious falls is 43 per 1000 person-years, and 26 fractures per 1000 person-years. This was lower than recent Australian-based findings for 12 month post-stroke fracture incidence (i.e. 74 fractures per 1000 person-years) 22 ; however, this study included fractures due to other mechanisms such as overexertion and repetitive stress, in addition to falls. Our findings only related to fractures classified as an SAE (e.g. requiring inpatient hospitalization, not including general practitioner or emergency department-only care) and did not include participants with poor pre-morbid function or those who were medically unwell or unstable in the first 24 h post stroke. Nevertheless, our incidence was similar to other research on post-stroke fracture rates. 34 The high rate of hip fracture (42% of fractures) is consistent with prior research suggesting that hip fractures represented a large proportion (30%–45%) of post-stroke fractures.2,11,22 Our finding that fractures were more common on the stroke-affected side may be due increased bone loss secondary to reduced weight bearing on the paretic side,35,36 compounded by increased falls toward the paretic side.2,10,14 Our findings on time of serious falls post stroke also aligns strongly with prior research in a large Australian cohort, with a similar median time to fracture of 170 days within the first year. 22
Prior research reporting location of falls has similarly found they commonly occur within the home environment (61%–77%).4,12 Our study found a relatively large proportion occurred within the hospital environment, likely due to the data collection occurring immediately after stroke. Nonetheless, location data should be interpreted cautiously as this was not analyzed relative to the time spent in different settings, and data in the post-discharge period may be less accurate. Similarly, our findings indicated that most falls occurred during the day (6 am–5:59 pm), which is consistent with prior research.5,12 In regard to circumstances surrounding falls, a toileting category was added which overlapped with some results from the ambulating and transferring categories. Falls that occurred while going to the bathroom were common (26% of those reporting on activity), and this has been previously highlighted in the literature.4,5 Presence of continence issues may lead to greater urgency and frequency of bathroom mobility. 37 Furthermore, post-stroke functional deficits may make it more difficult for individuals to steady themselves while adjusting clothing when toileting, and privacy requirements may also contribute to a reluctance to seek assistance.
We found increased age to be strongly associated with a greater risk of serious falls. This is in line with prior stroke research suggesting older adults are at higher risk of falls.20–22 This may be related to an age-related decline in physical function which is well documented. 38 Prior literature has suggested that an accumulation of multiple comorbidities increases risk for falls (⩾three comorbidities).3,12 Recent research has also highlighted malnutrition, depression, and osteoarthritis as associated with post-stroke fracture risk. 22 However, our study did not have aggregate data on comorbidities (e.g. a comorbidity index), and we did not include individual comorbidity data in our current analysis (e.g. hypertension, diabetes, arthritis, and prior stroke). Furthermore, we did not have specific individual data on some potentially relevant comorbid conditions, including osteoporosis or baseline cognitive impairment, or medications.
Regarding stroke-related factors, our study found better early post-stroke mobility was significantly associated with reduced risk for serious falls. Previous literature has similarly indicated that reduced mobility after stroke is associated with increased fracture incidence.6,10 However, the strength of this association is likely attenuated by the non-linear relationship between mobility and falls, resembling an inverted “U” shape. 39 This suggests that individuals on both extremes (i.e. those with significantly reduced mobility and highly mobile individuals) experience fewer falls, whereas those with moderate mobility deficits may have increased risk. 39 These individuals between the two extremes are likely more active than those with significantly reduced mobility and thus more frequently find themselves in situations that may lead to falls. Nonetheless, our inferences are based on mobility assessments around the time of stroke and are not an accurate reflection of mobility at time of fall.
Hemi-neglect, a post-stroke factor whose contributions to falls are controversial,11,23,38 was not found to be significantly associated with serious falls. However, hemi-neglect was captured within the very early post-stroke period, which may not be the most appropriate timing, and was not assessed with a comprehensive testing battery. Assessment of hemi-neglect on admission to inpatient rehabilitation or prior to hospital discharge may be more appropriate. It has been hypothesized that a presence of hemi-neglect is associated with increased postural instability, 40 and this may be one mechanism leading to increased falls. 24
Attempts to create screening models to predict post-stroke falls have assessed factors such as age, falls history, and hemi-neglect, but have shown limited clinical applicability. 41 A recent Australian study utilized the Fracture Risk After Ischaemic Stroke (FRAC-stroke), which identifies people who should be screened for osteoporosis and includes factors such as age, female sex, mRS, rheumatoid arthritis, osteoporosis, and previous falls and fractures. 8 They found higher FRAC-stroke scores in individuals with post-stroke fractures. Our study confirmed an association between age and serious falls risk and additionally highlighted pre- and post-stroke mobility as significant factors. Incorporating these factors into screening models could improve targeted support for high-risk individuals, though further research is needed to validate their clinical utility.
Limitations
Our study had several limitations. First, individuals with mRS > 2 pre-stroke were excluded from the study (22% of those screened) 25 and may be a group who are at higher risk of serious falls. Those who were medically unstable or unwell early post stroke were also excluded (28% of those screened) 25 and may have influenced the findings. In addition, generalizability of our findings may be impacted by other factors related to trial eligibility or consent. While nominated representatives were also able to provide consent, others were not enrolled due to participation in other trials, refusal, or other reasons. Baseline factors such as mobility and hemi-neglect were collected within 24 h of stroke. This may not be the most appropriate time to assess risk as individuals can change quickly in the first days to weeks following stroke. Nevertheless, impaired mobility was associated with increased falls risk, and early assessment may allow for timely identification of people at risk and influence decision-making. It is important to note stroke survivors may experience multiple serious falls, and we were not able to reliably calculate serious falls rates from our data. Another limitation was the lack of information pertaining to the circumstances and consequences surrounding falls, as this was not the focus of the SAE data collection for the AVERT trial. Complete information about the time, location, and mechanism of serious falls would have provided a more robust analysis.
Conclusion
Although it is well-recognized that falls after stroke have adverse outcomes, accurate information on the occurrence of serious falls and their contribution factors is unclear. By identifying these factors, early recognition of individuals susceptible to serious falls may aid in both falls and injury prevention. These individuals should be targeted for comprehensive falls risk assessment and management. In terms of injury prevention, screening for other comorbidities such as osteoporosis may be beneficial in these populations who are already at higher risk of fracture. Similarly, the use of anticoagulation in these high-risk populations may be an important question for future research, where the benefit may not outweigh the risk. Our study indicated that increased age, poor early post-stroke mobility, and pre-morbid function are associated with higher risk of serious falls. These individuals may therefore require specific attention for falls and injury prevention.
Footnotes
Acknowledgements
The authors thank the AVERT Collaboration investigators for their hard work and for allowing access to their dataset used in this study (see Supplementary appendix by Bernhardt et al.) 25 . They thank all participants and their families without whom this trial would not be possible and to the 56 stroke units across the globe and their staff involved in this trial.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The AVERT trial was supported by the National Health and Medical Research Council (NHMRC) of Australia (grant nos. 386201 and 1041401); Chest Heart and Stroke Scotland (grant no. Res08/A114); Northern Ireland Chest Heart and Stroke (grant no. AVERT-NI 2008); Singapore Health (grant no. SHF/FG401P/2008); The Stroke Association, UK (grant no. TSA2009/09), and the National Institute of Health Research, UK (grant no. HTA Project 12/01/16). JB also received fellowship funding from the NHMRC (grant nos. 1058635 and 1154904), Australian Research Council (grant no. 0991086), and the National Heart Foundation. KB received funding from the University of Melbourne (grant no. 2021ECR172).
Data availability
The data that support the findings of this study are available upon reasonable request.