
Abstract
Introduction
Falls are common post-stroke events but their relationship with healthcare costs is unclear. The aim of this study was to examine the relationship between healthcare costs in the first year after stroke and falls among survivors discharged to the community.
Patients and methods
Survivors of acute stroke with planned home discharges from five large hospitals in Ireland were recruited. Falls and healthcare utilisation data were recorded using inpatient records, monthly calendars and post-discharge interviews. Cost of stroke was estimated for each participant from hospital admission for one year. The association of fall-status with overall cost was tested with multivariable linear regression analysis adjusting for pre-stroke function, stroke severity, age and living situation.
Results
A total of 109 stroke survivors with complete follow-up data (mean age = 68.5 years (SD = 13.5 years)) were included. Fifty-three participants (49%) fell following stroke, of whom 28 (26%) had recurrent falls. Estimated mean total healthcare cost was €20,244 (SD=€23,456). The experience of one fall and recurrent falls was independently associated with higher costs of care (p = 0.02 and p < 0.01, respectively).
Discussion
The observed relationship between falls and cost is likely to be underestimated as aids and adaptions, productivity losses, and nursing home care were not included.
Conclusion
This study points at differences across fall-status in several healthcare costs categories, namely the index admission, secondary/tertiary care (including inpatient re-admissions) and allied healthcare. Future research could compare the cost-effectiveness of inpatient versus community-based fall-prevention after stroke. Further studies are also required to inform post-stroke bone-health management and fracture-risk reduction.
Introduction
Stroke is a major cause of death and acquired disability that imposes a considerable burden on society. 1 Care for people with stroke accounts for approximately 3% of annual healthcare expenditure in several countries including Ireland.1–3 Recent European studies have estimated healthcare costs of between €12,000 and €18,000 in the first year after stroke with the majority of these costs occurring in the first few months after the event.2–6 Approximately 7000 people are admitted to hospital with a stroke annually in Ireland, and based on anticipated changes in the country’s population demographics, cost of stroke in Ireland is estimated to increase by over 50% between 2007 and 2021.7,8 It is therefore important to consider options for reducing costs and increasing the efficiency of post-stroke service provision.
Falls are common adverse events after stroke and may contribute to increased costs. Stroke survivors fall at almost twice the rate and have four times the risk of hip fracture compared with healthy aged-matched adults.9,10 It is estimated that approximately 50% of those discharged home fall in the first year with up to 40% falling repeatedly and 5% experiencing fractures.11–13 In older adults, falls have been found to be associated with increased healthcare utilisation, independent of age and comorbidities. 14 Irish estimates for 2004 show fracture-related admissions for older adults cost an average of €8331 per inpatient stay. 15 To our knowledge, little is known about the relationship between post-stroke falls and costs. The aim of this study was to estimate cost of stroke care in Ireland in the first year among survivors discharged to the community and to examine the relationship between falls and cost.
Methodology
Study design
From a multicentre, prospective cohort study (the Falls Related EvEnts after StrokE Study), 16 we obtained patient-level healthcare cost relating to Medical treatment, rehabilitation, regular care costs and informal care provision.
Healthcare context
Although Irish residents are entitled to receive care through the public healthcare system, delays and limited availability of post-discharge rehabilitation services lead some stroke survivors to pay for services in addition to those provided by the national health service.7,17 Unfortunately, unlike some other European countries, Ireland does not have centralised or linkable utilisation databases.4,7 Therefore, the current study collected patient-reported healthcare utilisation data about all services provided, independent of funding.
Participants
We recruited adults with a diagnosis of acute ischaemic or haemorrhagic stroke from five large teaching hospitals in the city of Dublin between November 2013 and August 2014. Those with a planned discharge home to the community were recruited consecutively. We excluded stroke survivors discharged to a nursing home and those unable to provide consent due to severe cognitive deficits (Mini Mental State Exam <18) 18 or severe receptive language deficits (as judged by treating speech and language therapists). Ethical approval was received from each hospital’s Research Ethics Committee and all participants provided written informed consent.
Baseline data collection
Demographic and clinical data were collected from medical records. Stroke severity on admission was rated using the National Institutes of Health Stroke Scale (NIHSS). 19 If not recorded in the notes, as occurred with 50% of participants, this was conducted retrospectively using an established method 20 and strokes were classified as mild (NIHSS 1–4), moderate (NIHSS 5–15) or severe (NIHSS >15). 21 The number of comorbid conditions recorded in the hospital admission notes were recorded if included in the Functional Comorbidity Index. 22 Participants reported their pre-stroke function based on the Nottingham Extended Activity of Daily Living (NEADL) scale and a score between 0 and 22 (low-to-high function) was calculated. 23
Falls data collection
In accordance with international recommendations, a fall was defined as ‘an unexpected event in which participants came to rest on the ground, floor or lower level’. 24 Inpatient fall-status was established through a post-discharge phone call with participants. Falls that occurred after discharge from hospital were recorded both prospectively using participant-completed calendars and retrospectively through face-to-face interviews at six months and phone interviews at one year. A ‘faller’ was defined as a participant who experienced at least one fall over the follow-up period. Participants who experienced at least two falls were designated as ‘recurrent fallers’.
Healthcare utilisation data collection
Healthcare utilisation was recorded from hospital admission to one year after discharge in all participants. Length of inpatient stay (including in a rehabilitation hospital) was recorded from medical records. Participants’ self-reported post-discharge healthcare utilisation was recorded both prospectively using participant-completed calendars and retrospectively through structured interviews at six months and one year after discharge. The number of visits to the following services was recorded: general practitioner (GP), outpatient services, emergency department, public health nurse, physiotherapist, occupational therapist, speech and language therapist, dietician, psychologist, optician, dentist, chiropodist, hearing services, alternative therapist, day care and respite care. Participants also reported their number of re-admissions as an inpatient and nights spent in hospital. The source and frequency of any regular help received was recorded. It was classified as informal (from friends and family) or formal care. At the final interview, participants reported their pre-stroke and current employment status.
Cost estimation
Total cost of stroke was calculated for each participant based on healthcare utilisation and unit costs. Sub-categories of cost were calculated as follows: cost of index admission, post-discharge primary care, secondary/tertiary care (including inpatient re-admissions), post-discharge allied health services, other post-discharge services, regular formal care and regular informal care.
Unit costs were extracted from existing Irish sources and adjusted to 2014-price levels using the national Consumer Price Index for Health.7,25–27 Unit costs and sources for each service are presented in online Supplemental Table 1. Costs are expressed in Euro (€). The cost of informal care was estimated based on an assumption that it replaces approximately 50% of formal care. The cost of informal care is not included in the total cost of stroke but is presented separately. Total cost did not include productivity losses, but the number of individuals affected by a change in employment status was estimated. The number of hours of formal and informal care received by participants over the first and second six-month periods post-discharge was estimated as detailed in Table 1.
Estimation of care hours during six-month period.
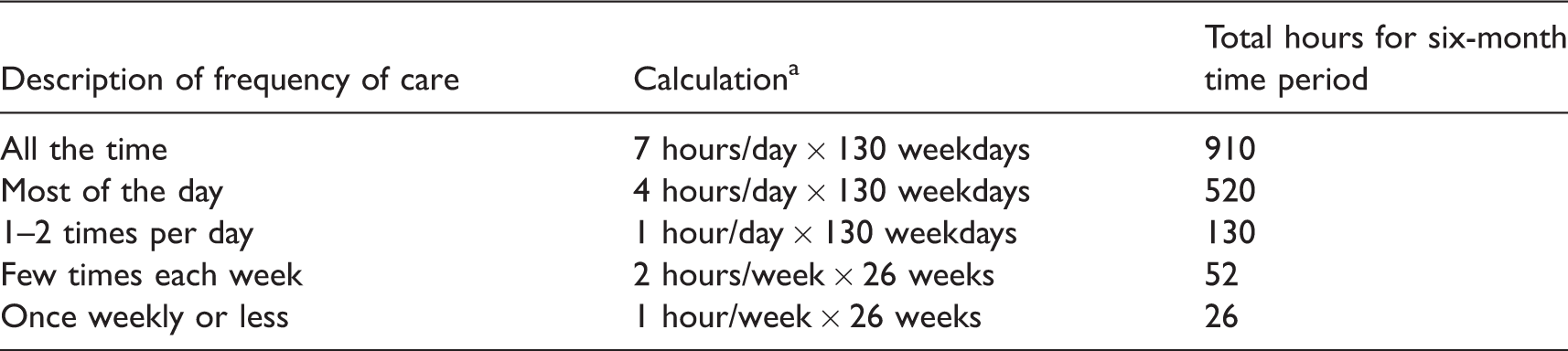
aAssumption of weekday service during ‘office hours’ 7 and equal distribution of service use across each six-month time period.
Statistical analysis
Data were analysed using Stata Version 13.1 for Mac (StataCorp). Cost for non-fallers was compared with that of ‘one-time fallers’ and ‘recurrent fallers’ using univariable linear regression for each cost category. Univariable linear regression analysis was conducted to explore the association between several factors (fall-status, pre-stroke status (NEADL), stroke severity (NIHSS), age and living situation) and total cost. Explanatory variables were chosen to account for factors that may influence baseline pre-stroke healthcare utilisation and the cost of the stroke itself. 28 Fall-status as a variable represented the stroke-recovery phase in the analysis. Age was categorised as conducted in a large prospective study of community-dwelling older adults in Ireland that has shown a relationship between healthcare utilisation and age. 28 An a priori decision was made to dichotomise NIHSS as <5 points or 5+ points as this cut-off is used to clinically distinguish mild from moderate/severe stroke. A multivariable linear regression model was used to test the association of fall-status with overall cost with adjustment for the other factors. A significance level of p < 0.05 was used for all analyses.
Sensitivity analysis
Five sensitivity analyses were conducted:
Participants with costs above the 95th and below the 5th percentiles of cost were excluded. Higher unit costs for allied healthcare services were assigned by applying costs to estimated patient contact hours rather than total hours worked by therapists.
7
A lower cost was applied to time spent in an offsite rehabilitation facility compared with the acute hospital. Costs calculated from estimated hours of regular formal care were excluded. Cost was weighted to a one-year time period for all participants to account for the variable follow-up time due to different lengths of acute stay in hospital.
Results
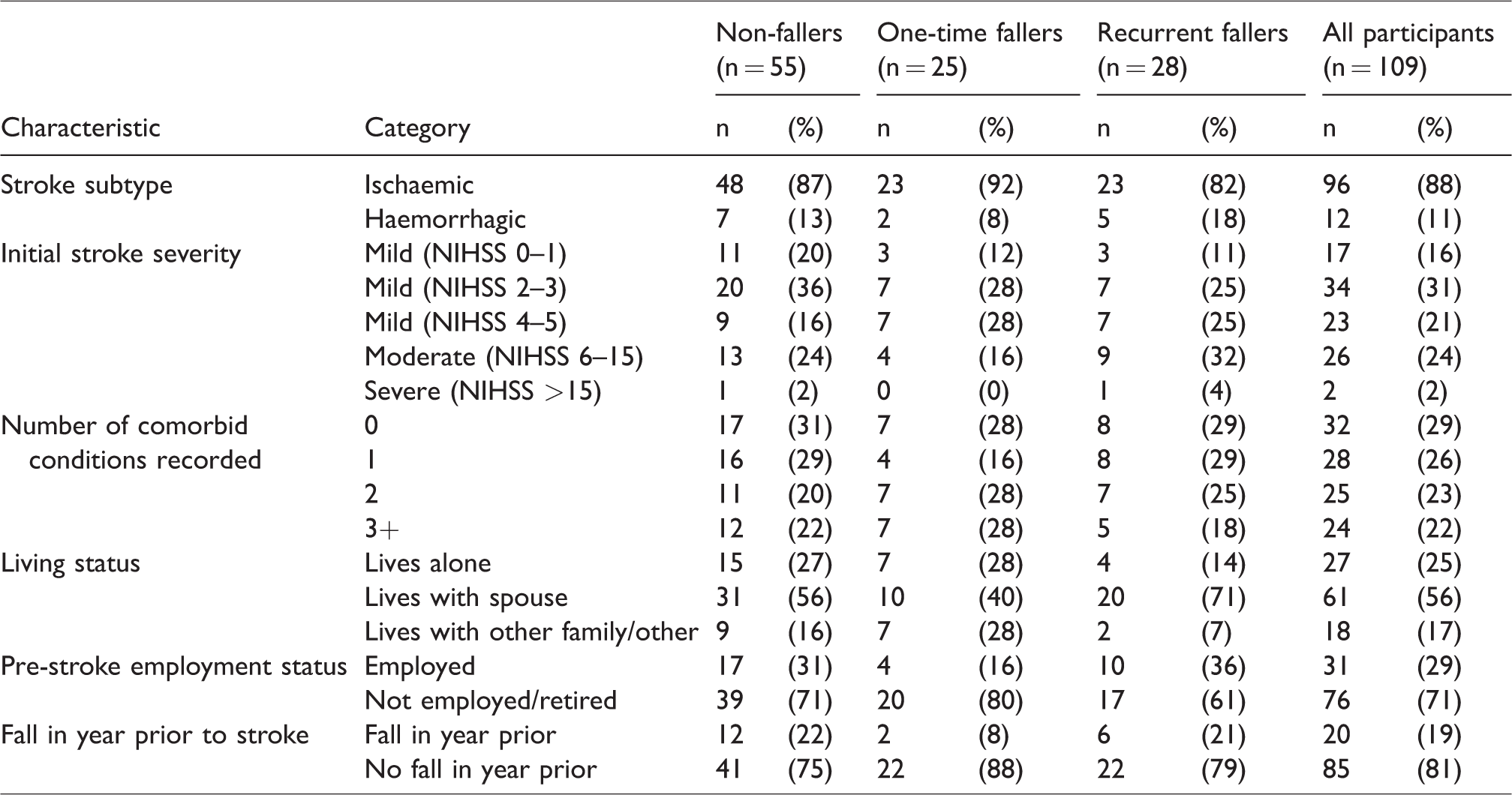
In total, 322 stroke survivors were referred, 270 were potentially eligible, 128 were recruited and 109 (67 men and 42 women) completed all follow-up interviews. Figure 1 shows the flow of participants through recruitment and follow-up. Participants had a mean age of 68.5 years (SD = 13.5) at baseline. Their median pre-stroke NEADL score was 18 (Interquartile Range = 16–21), signifying good function, and the median NIHSS score was 3 (Interquartile Range = 2–7), indicating mild–moderate stroke. The mean total follow-up time period was 395 days (SD = 32 days). Initial median length of inpatient stay was 14 days (range 2–163 days). For 16% of participants (n = 17), this included days at a rehabilitation facility. A further 13% received Early Supported Discharge (ESD). Seventeen participants (16%) had a previous stroke and 20 (19%) had a fall in the prior year. Table 2 shows further participant characteristics at baseline by post-stroke fall-status.
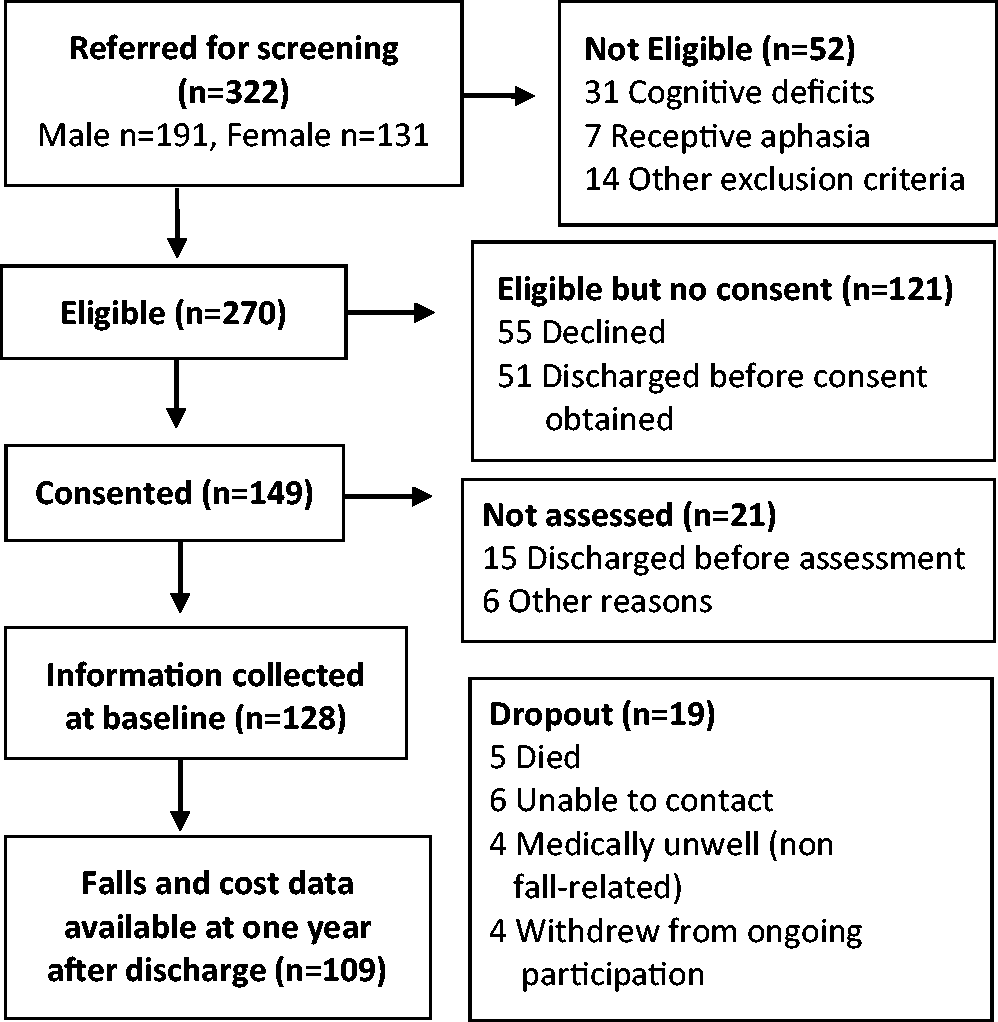
Flow diagram of recruitment and follow-up of participants.
Detailed participant characteristics at baseline by post-stroke fall-status (n = 109).
Over 95% of participants visited their GP, 57% attended a physiotherapist and 59% received informal care during follow-up. The proportion of participants who used each service and their number of visits is presented in online Supplemental Table 2. Table 3 shows the proportion of each fall-category that used each category of care. Notably, 100% of recurrent fallers, 72% of one-time fallers and 57% of non-fallers received community allied healthcare. At the end of the follow-up period, 18 of the 31 (58%) individuals who were employed pre-stroke had ceased working.
Sub-categories of cost by fall-status (2014 costs in €).
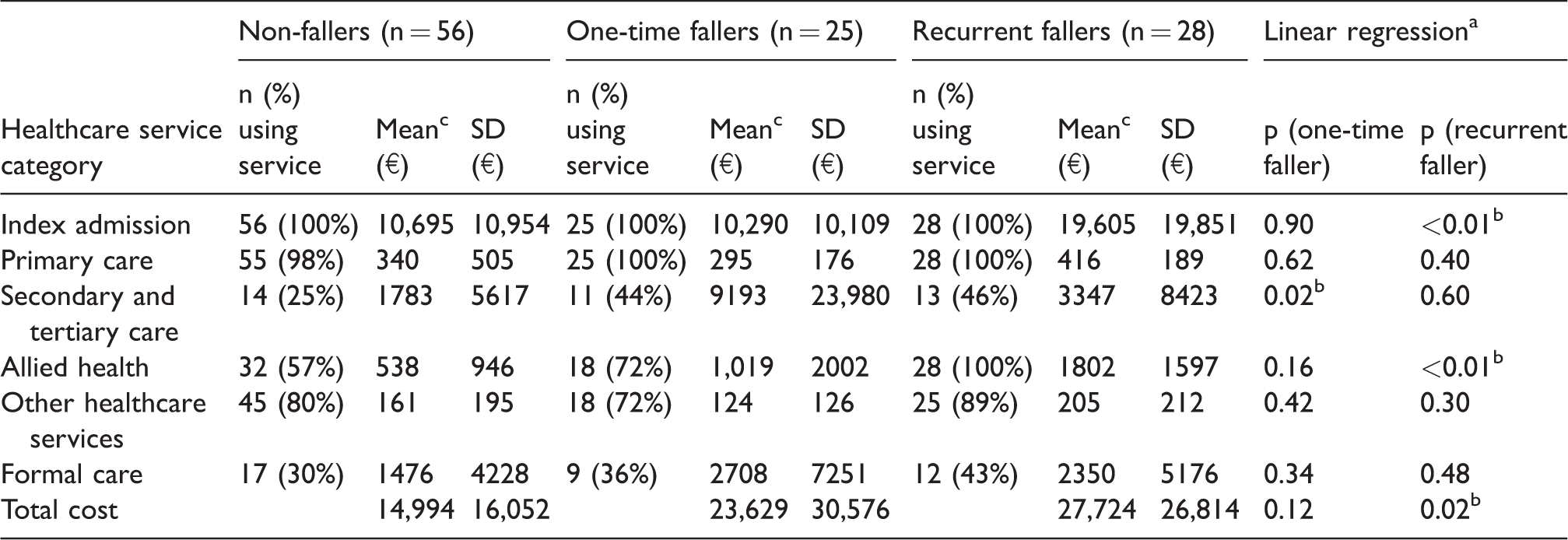
aNon-faller = reference category.
bStatistically significant at 95% confidence level.
cCalculated based on all participants in fall-category, not just those using service
During the follow-up period, almost half of participants fell (n = 53), 26% repeatedly (n = 28). Six ‘one-time’ and five ‘recurrent fallers’ experienced falls in hospital. After at least one of their falls, 21 fallers (40% of fallers) reported seeking healthcare advice, while 10% of fallers (n = 5) reported sustaining fractures.
The total mean cost of care over the first year was estimated at €20,244 (SD=€23,456). The median cost was €10,425 (IQR=€5937–€28,429). Table 3 shows sub-categories of cost by fall-status. Recurrent fallers had a statistically higher cost of their index admission (p < 0.01) and post-discharge allied healthcare services (p < 0.01) than non-fallers. Recurrent fallers also had significantly higher overall cost (mean €12,730 higher, 95% CI €2,181–€23,280). As shown in Table 3, the only category of cost that was significantly higher for one-time fallers than non-fallers was the cost of secondary/tertiary care. One-time fallers spent a mean of 13.4 nights in hospital during re-admissions (SD = 35.1), in comparison to a mean of 2.6 nights (SD = 8.2) for non-fallers. The mean cost of informal care was estimated at €2512 (SD=€4682), €1361 (SD=€2213) and €3422 (SD=€4851) for non-fallers, one-time fallers and recurrent fallers, respectively. No significant association was found between the cost of informal care and single falls (p = 0.27) or recurrent falls (p = 0.36).
Table 4 shows the results of univariable and multivariable linear regression analyses. Higher cost of stroke care was associated with both the experience of one fall or recurrent falls (p < 0.01) when compared to not falling, independent of pre-stroke reported functional status, age, stroke severity and living status. Table 5 shows the results of the sensitivity analyses. Excluding participants outside the top and bottom fifth percentile of cost had the largest effect on the overall cost of stroke care. In all analyses, the experience of recurrent falls remained statistically associated with total cost when compared with the experience of no falls, adjusting for factors outlined in Table 4.
Linear regression analysis with total cost as outcome.
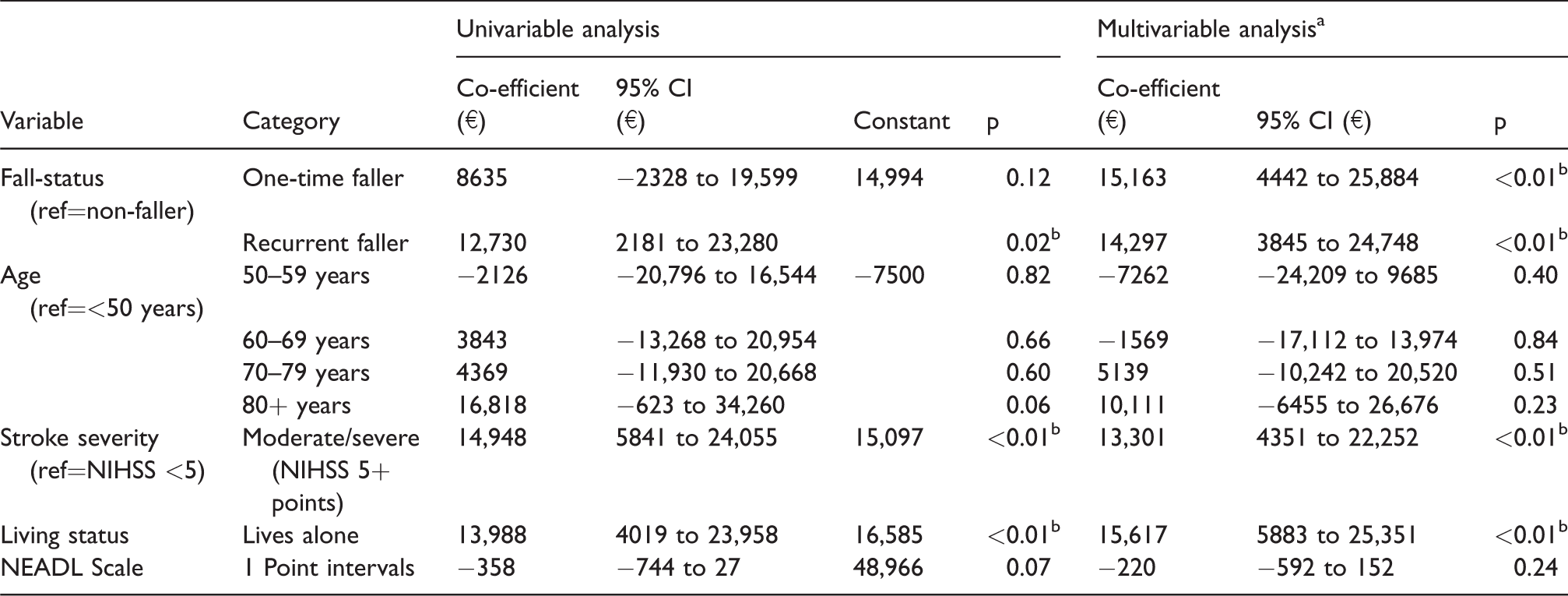
NIHSS: National Institutes of Health Stroke Scale; NEADL: Nottingham Extended Activities of Daily Living.
aConstant= −5812, adjusted R2=0.27 (with all five variables included in model).
bStatistically significant at 95% confidence level.
Sensitivity analyses.
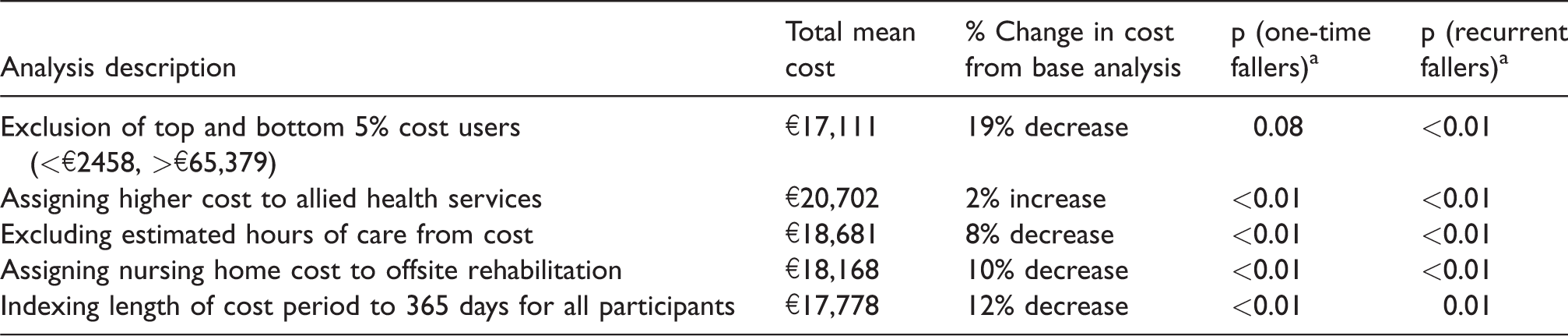
aMultivariable linear regression, controlling for factors as in Table 4. Reference category= ‘non-fallers’.
Discussion
This study examined the relationship between fall-status and the healthcare costs of community-dwelling individuals following stroke. The experience of recurrent falls during the follow-up period was found to be associated with higher costs of stroke care overall, a higher cost of the index admission and a higher cost of post-discharge allied healthcare services. Furthermore, when controlling for age, pre-stroke reported function, stroke severity and living status, the experience of both a single fall and recurrent falls were independently associated with higher costs. In this cohort, the estimated average cost of care was €20,244. This is in line with previous international studies using similar methodologies.4,5 It is also similar to an Irish 2007 prevalence-based estimate cost of €18,751 per stroke in the first year. 29 In addition, the post-stroke falls incidence in this cohort is in keeping with similar prospective studies.9,13 Despite the majority of participants (93%) having mild–moderate strokes, half of participants still experienced a fall.
In this study, we present the categories of healthcare costs that drive the statistical association between overall cost and the experience of falls in this population, namely inpatient care initially after the stroke or due to a re-admission. Those who fall recurrently over the first year are also the individuals who received the highest level of allied healthcare after discharge. Community-based services, however, as seen in prior studies, do not contribute significantly to the overall cost of care as they are relatively inexpensive.1,6 This study does not claim to attribute healthcare costs purely to the fall events themselves. We do know that after at least one of their falls, 40% of fallers sought healthcare advice and 10% sustained fractures that required medical care. Falls experienced during stroke recovery have an important relationship with perceived falls-risk, fear of falling and implementation of falls-prevention interventions 30 that could contribute to overall cost both before and after the fall event itself. Fallers post-stroke in this and previous studies were found to have a longer initial inpatient stay. 13 Those deemed to be at risk of falls are likely kept longer in hospital for rehabilitation. 13 ESD is a service that accelerates hospital discharge by providing rehabilitation at home. 7 It is considered to be the best international practice post-stroke, but only 5% of stroke survivors in Ireland currently access it.31–33 Wren et al. estimated that developing ESD in Ireland could save €2–7 million. 7 As community-based interventions have not been shown to reduce falls after stroke thus far, 34 further research should explore whether ESD could reduce healthcare costs after stroke while providing adequate falls-prevention rehabilitation.
Re-admissions to hospital are another important contributor to average costs in each fall category. Interestingly, fall-status in this study was statistically associated with the category of secondary/tertiary care for one-time fallers only. Large standard deviations suggest that this cost was driven by a small number of individuals. Sensitivity analysis also revealed that excluding very high-cost users resulted in the experience of one-time falls no longer being independently associated with overall healthcare costs. Fractures and other injuries requiring inpatient admission are potentially expensive and can occur even with a single fall. 15 Bone density assessment to facilitate targeted introduction of treatments to reduce the likelihood of post-stroke fractures may have the potential to reduce overall costs of care following stroke, 33 but this requires further research.
Strengths and limitations
While self-report of healthcare utilisation in the post-discharge period may have been affected by compliance and recall bias, it has been shown to be comparable to administrative databases in previous research, particularly for high-cost care. 35 Within the Irish system, the lack of a centralised utilisation database and the high rate of privately accessed care makes self-report necessary. 2 Ideally, self-report of inpatient falls would be verified using both incident report systems and medical records but this was not considered feasible in the current multi-site study due to limited resources. 36 A major strength of this study is that we collected post-discharge falls and healthcare utilisation data using a combination of prospective diaries and retrospective interviews. 24 While this resulted in collection of detailed information about falls and healthcare utilisation, it must be acknowledged that sample size is relatively small, resulting in wide 95% confidence intervals in regression analyses.
While the study had a low attrition rate in the follow-up phase (<15%) and included stroke survivors across five large university teaching hospitals,9,12,31 it must be noted that of the 270 individuals originally determined to be potentially eligible, only 41% were recruited and completed follow-up. This may affect the external validity of the study. The majority of those who were not recruited or followed-up in the current study had either short lengths of stay in hospital (i.e. <3 days) or did not participate due to perceived burden of the study. This could include both the lowest and highest users of healthcare. It is therefore unclear to what extent this could have influenced the observed association between falls and cost.
We have tested assumptions of our methodology by performing several sensitivity analyses. This has increased our confidence in the observed statistical relationship between healthcare cost and falls in this population. It is likely that the strength of this association has been underestimated. Total cost of stroke care did not include the cost of aids or home adaptions, which are recommended falls-prevention interventions in current stroke care guidelines. 33 Informal care was not found to be associated with fall-status in the current study. Previous research has found, however, that carers may be reluctant to leave stroke survivors at home alone due to perceived falls-risk even in the absence of falls. 37 We acknowledge that care provided by friends and family can reduce the burden of stroke on society but may also result in carers being unable to continue in paid employment, thus contributing to the ‘indirect’ financial cost of stroke. 2 However, we opted to exclude the cost of informal care from ‘total cost’ in our study design to facilitate comparisons with data from the vast majority of related studies.1,7
The current study focused on survivors discharged to the community who account for 66% of those who experience a stroke in Ireland. 31 This study does not purport to estimate the cost of care for all persons with stroke as it excludes those discharged to nursing homes or those who died as inpatients. Productivity losses amongst stroke survivors themselves were not accounted for in the current study either and this may also have underestimated costs. Between 17% and 28% of participants in the current study were affected by changes in employment. In a recent Dutch study, 6 29% of stroke survivors experienced productively losses, accounting for 10% of overall costs.
Conclusion
This study points at differences across fall-status in several healthcare costs categories, namely the index admission, secondary/tertiary care (including inpatient re-admissions) and allied healthcare. The relationship between increased overall cost of care and fall-status exists independently of pre-stroke factors and stroke severity. Future research could compare both the effectiveness and cost of inpatient versus community-based fall-prevention interventions. Further studies are also required to inform post-stroke bone-health management and fracture-risk reduction.
Supplemental Material
Supplemental material for First year post-stroke healthcare costs and fall-status among those discharged to the community
Supplemental material for First year post-stroke healthcare costs and fall-status among those discharged to the community by Mary E Walsh, Jan Sorensen, Rose Galvin, David JP Williams, Joseph A Harbison, Sean Murphy, Ronan Collins, Dominick JH McCabe, Morgan Crowe and N Frances Horgan: Central Statistics Office in European Stroke Journal
Footnotes
Acknowledgements
We would like to thank all staff in stroke care at participating sites, in particular Imelda Noone and Joan Mc Cormack for assistance with identification of potential participants and Colm Brannigan for his assistance with data collection. We would also like to gratefully acknowledge the contribution of participants who gave generously of their time and energy.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Irish Research Council (Government of Ireland Postgraduate Scholarship Scheme 2013).
Informed consent
Written informed consent was obtained from all participants for their anonymised information to be published in this article.
Ethical approval
Four research ethics committees approved this study: Beaumont Hospital, Mater Misericordiae University Hospital, St Vincent’s Healthcare Group and Tallaght/St James’s Hospitals.
Guarantor
MEW.
Contributorship
MEW was involved in study design, performed data collection, data analysis and drafted the manuscript. JS advised on and assisted with data analysis and assisted in drafting of manuscript. RG and NFH were involved in study design and supervised data collection and analysis. DJPW, JAH, SM, RC, DJHM and MC were involved in study design and assisted with recruitment. All authors edited drafts of manuscript and approved the final version for submission.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.