
Abstract
Background:
Stroke is a leading cause of global mortality and disability, with a disproportionately high burden in low- and middle-income countries. Access to intravenous thrombolysis (IVT) and endovascular treatment (EVT) remains extremely limited.
Aims:
We evaluated the spatial distribution and geographic accessibility of stroke centers in India.
Methods:
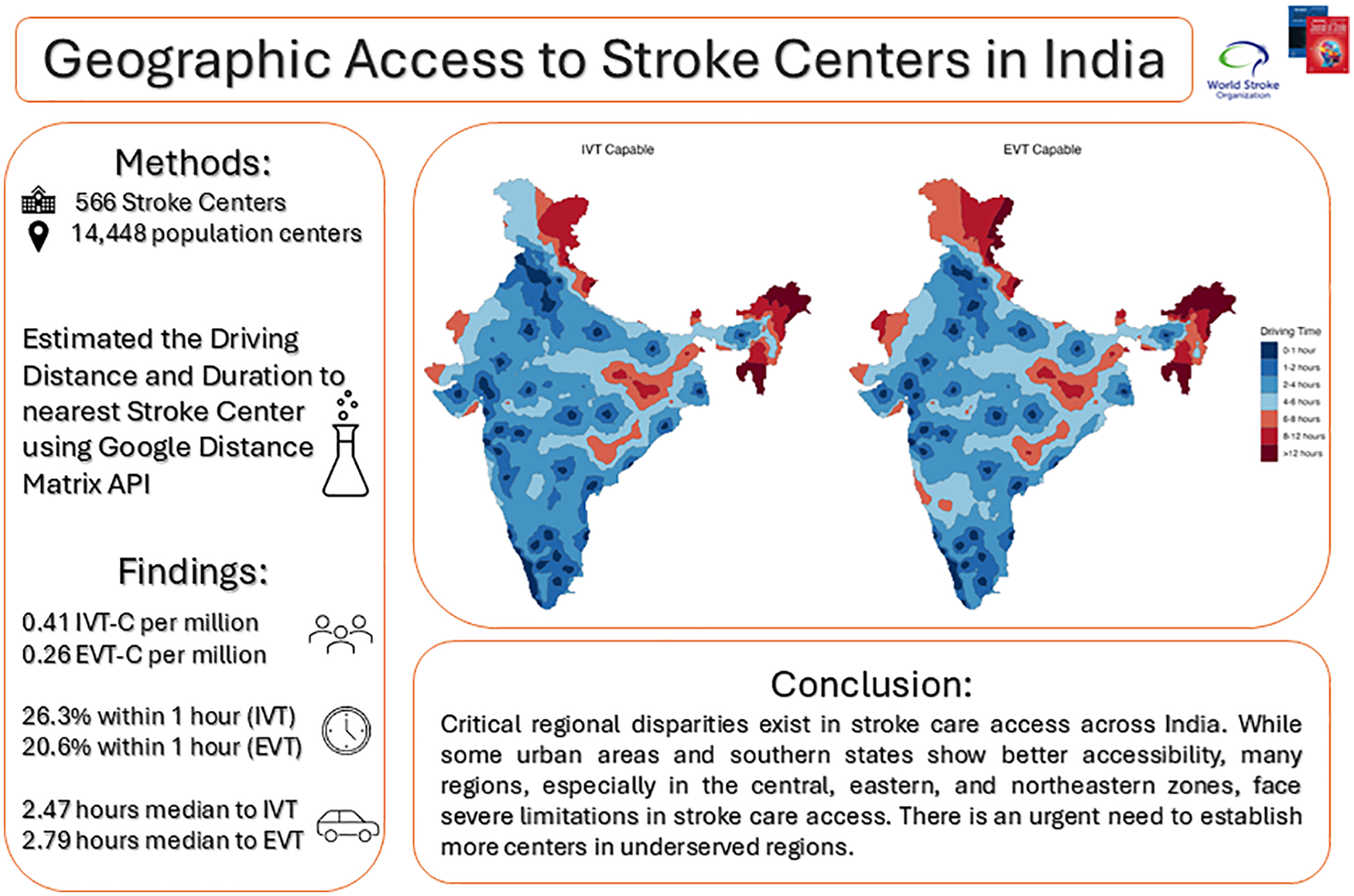
Data on IVT capable (IVT-C) and EVT capable (EVT-C) stroke centers were collected in March 2021 from thrombectomy devices and pharmaceutical industry providers, respectively. Data were collated and geocoded to compare and calculate zonal statistics and state/union territory (UT) summaries using descriptive statistics. Data on population centers were obtained from the Survey of India website. For estimating driving times, we used the Google Distance Matrix API to find the driving distance between each population center and its nearest stroke facility. Subsequently, population coverages were estimated as a proportion of the population having access to stroke centers for each time interval and based on the population projection for the year 2020 and compared across states.
Results:
A total of 566 IVT-C stroke centers were spread across 26 states and UTs, of which 361 (63%) were EVT-C. Ten UTs lacked stroke centers. The average stroke centers per million (SCPM) population was 0.41 and 0.26 for IVT-C and EVT-C, respectively. Median distances to the nearest IVT-C and EVT-C centers were 115 km (interquartile range (IQR): 66–175) and 131 km (IQR: 79–198), respectively. Access within 1 h to an IVT-C and an EVT-C center was available to 26.3% and 20.6% of the Indian population, respectively.
Conclusions:
Access to stroke care in India is poor, with critical regional disparities as reflected by the low SCPM population, long driving times, and a small population with access within the golden hour. There is an urgent need to establish IVT-C and EVT-C stroke centers in the existing poorly served regions of India to increase access and improve outcomes for stroke patients.
Get full access to this article
View all access options for this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.