
Abstract
Background:
Technical improvements in devices, changes in angiographic grading scales and various confounding factors have made difficult the detection of the temporal evolution of angiographic and clinical results after endovascular treatment (EVT) for acute ischemic Stroke (AIS). We analyzed this evolution in time using the Endovascular Treatment in Ischemic Stroke (ETIS) registry.
Materials and Methods:
We analyzed the efficacy outcomes of EVT performed from January 2015 to January 2022, and modelized the temporal trends using mixed logistic regression models, further adjusted for age, intravenous thrombolysis prior to EVT, general anesthesia, occlusion site, balloon catheter use and the type of first-line EVT strategy. We assessed heterogeneity in temporal trends according to occlusion site, balloon catheter use, cardio embolic etiology, age (<80 years vs ⩾80 years) and first-line EVT strategy.
Results:
Among 6104 patients treated from 2015 to 2021, the rates of successful reperfusion (71.1%–89.6%) and of complete first pass effect (FPE) (4.6%–28.9%) increase, whereas the rates of patients with >3 EVT device passes (43.1%–17.5%) and favorable outcome (35.8%–28.9%) decrease significantly over time. A significant heterogeneity in temporal trends in successful reperfusion according to the first-line EVT strategy was found (p-het = 0.018). The temporal trend of increasing successful reperfusion rate was only significant in patients treated with contact aspiration in first-line (adjusted overall effect p = 0.010).
Conclusion:
In this 7-year-old large registry of ischemic stroke cases treated with EVT, we observed a significant increase with time in the rate of recanalization whereas there was a tendency toward a decrease in the rate of favorable outcome over the same period.
Keywords
Background
The goal of endovascular treatment (EVT) for stroke due to Large Vessel Occlusion is to achieve recanalization of the occluded vessel as quickly and completely as possible. 1 The first studies that proved the efficacy of EVT in 2015 considered a partial recanalization (TICI 2b) at the end of the procedure, whatever the number of passes,2–6 as a technical success. Then, many mono- or multicentric studies, performed with different sample sizes and according to either an external core lab or self-adjudication grading of recanalization, reported almost complete final recanalization rates (TICI 2b/3 > 90%) at the end of procedure.7–10 More recently, a new standard of treatment efficiency has emerged: achievement of complete recanalization in one pass (first pass effect, FPE), that is clearly associated with increased rates of good patient outcomes at 3 months. 11 However, this more ambitious recanalization endpoint is only reached in less than half of the cases. 12
Along with this improvement in angiographic results, there has also been a refinement and increased precision in the grading of reperfusion evaluated during EVT. Thus, we moved from TIMI, TICI, mTICI to eTICI, with these reperfusion graduations providing a consistently better correlation with good patient outcomes.13–16 Furthermore, several factors still influence recanalization rates and the number of passes necessary such as occlusion location, age, anesthetic regimen and prior intravenous thrombolysis.8,17,18
Taken together, these elements associated with the expanding of EVT indications, have made it difficult to detect the temporal evolution of angiographic outcomes and clinical results after EVT for stroke.
Since 2015, the ETIS registry has exhaustively recorded all procedures performed in France in a network of expert centers. In this 7-year-old, nationwide registry of ischemic stroke treated with EVT, we analyzed the temporal evolution of angiographic recanalization results, clinical outcomes and the disparities in terms of subgroups.
Material and methods
Data availability statement
The data that support the findings of this study are available from the corresponding author upon reasonable request.
Study population
From January 2015 to January 2022, we collected clinical and imaging data from 26 different comprehensive stroke centers taking part in the ETIS registry (Endovascular Treatment in Ischemic Stroke). Prospectively gathered data were then retrospectively analyzed.
Patients included in our study presented with acute ischemic stroke caused by an anterior circulation occlusion proven on cerebral imaging (magnetic resonance imaging or computed tomography with angiographic sequences) and treated by EVT. Only patients harboring proximal middle cerebral artery occlusion (M1), with or without intracranial carotid occlusions (ICA), were included. However, we only considered the more proximal location. Hence, M1 with ICA are ICA, M1 without ICA are M1 occlusions.
Prior administration of intravenous thrombolysis was decided according to usual international guidelines. 19
Absence of LVO during the first run of Angio DSA as initial TICI > 2a, patients with (M2) occlusions, posterior circulation, isolated extracranial and tandem occlusions were excluded because of technical specificities that preclude reliable comparisons with other locations of occlusion. Age, baseline modified Rankin Scale (mRS), admission National Institutes of Health Stroke Scale and infarct core volume were not considered as exclusion criteria per se.
EVT was performed by neurointerventionalists in comprehensive stroke centers according to the guidelines prevailing at the time.19,20 All endovascular procedures were performed under a dedicated anesthesiological protocol that encompassed conscious sedation or general anesthesia. First-line EVT was chosen at the operator’s discretion using either an aspiration catheter, a stent retriever or both, and a balloon guide catheter (BGC) or not.
Outcomes
The primary outcomes were successful reperfusion at the end of procedure (mTICI 2b/3), complete FPE (mTICI three in one pass), total number of passes >3 and favorable outcome defined as an mRS score of 0–2 or equal to pre-stroke Rankin score. Since the TICI grade 2c only appeared in 2017 we did not consider this grade as a relevant endpoint to analyze in our inclusion period. 14 For safety outcomes we used both the radiological classification of intracranial hemorrhage (any ICH) 21 and the ECASS III criteria for symptomatic intracranial hemorrhage (sICH) defined as any new intracranial hemorrhage on follow-up imaging with a clinical deterioration within the first 7 days. 22
Statistical analysis
Categorical variables were expressed as frequencies and percentages. Quantitative variables were expressed as means (standard deviation), or medians (interquartile range) for non-normal distribution. Normality of distributions was assessed graphically and by using the Shapiro-Wilk test.
To assess the temporal trends from January 2015 to January 2022 in patient outcomes, we categorized the study period (time) into trimesters. We examined the shape of temporal trends for each outcome by using smooth curves fitted by a generalized additive model (binomial distribution with a logit link function) with a cubic smoothing spline term. Since we observed J-shaped temporal trends for mTICI ⩾ 2B at the end of EVT, FPE, favorable outcomes, and 90-day mortality, we modelized the temporal trends using mixed logistic regression models with center as random effect, and by including linear and quadratic time terms (a second-order polynomial regression model). The overall temporal effects were examined using linear contrast. For the rate of patients treated with more than three device passes, a linear temporal trend was found and we modelized the temporal trends with a mixed logistic regression including center as random effect and a linear time term only. Temporal trends were further adjusted for main patient characteristics known to impact angiographic outcomes (age, cardio embolic etiology, prior intravenous thrombolysis, general anesthesia, occlusion site, BGC use, and the type of first-line EVT strategy) or to impact favorable outcome and 90-day mortality (age, cardio embolic etiology, admission NIHSS score, admission ASPECT score, onset to groin puncture time, prior intravenous thrombolysis, and occlusion site). After adjustment on pre-specified covariates, favorable outcome, and 90-day mortality showed a linear temporal trend and were then modelized with a mixed logistic regression including center as random effect and a linear time term only.
We assessed heterogeneity in temporal trends for the rate of successful reperfusion, complete FPE and favorable outcome according to the key patient and procedural characteristics (occlusion site, balloon catheter use, cardioembolic etiology, age (<80 years vs ⩾80 years) and first-line EVT strategy) by including the corresponding interaction terms with time (and quadratic time terms for successful reperfusion and complete FPE) in the multivariable mixed logistic regression models.
Missing values in pre-specified covariates and outcomes were handled in multivariate analyses by multiple imputation using a regression switching approach (chained equations with m = 10). 23 Imputation procedure was performed under the missing at random assumption using all baseline characteristics variables and outcomes with a predictive mean matching method for quantitative variables and multinomial or binary logistic regression models for categorical variables. Estimates obtained in the different imputed data sets were combined using Rubin’s rules. 24
Statistical testing was performed at the two-tailed α level of 0.05. Data were analyzed using the SAS software package, release 9.4 (SAS Institute, Cary, NC).
Results
From January 2015 to January 2022, 6104 patients with an occlusion in M1-MCA or intracranial ICA were consecutively treated by EVT in the 26 centers participating in the prospective ETIS registry (Supplemental Table 1). The ETIS registry includes 26 centers of EVT of Stroke among the 38 centers in France. Supplemental Table 2 shows characteristics of the patient population according to calendar year and shows changes in patient or treatment characteristics over time, with patients being older, rate of wake-up strokes higher, rate of prior IVT lower, and rate of balloon guide catheter use higher.
Baseline characteristics are presented in Table 1. Briefly, mean age was 71.5 ± 14.8 years old and 35.0% (n = 2132) of patients were over 80. Seventy-eight percent (78%) of the patients were treated for M1-MCA occlusion and 22% for ICA intracranial occlusion. 52% (n = 2709) had a cardio embolic etiology and 48% had other causes of stroke. First line EVT strategy was stent-retriever alone for 9% of patients (n = 500), contact aspiration alone for 43% (n = 2432) and a combination of stent-retriever and contact aspiration for the remaining 48% (n = 2726). Regarding study outcomes, 87.3% (95% CI 86.5–88.2, n = 5167) of patients had a successful reperfusion (mTICI ⩾ 2B) at the end of the procedure and 25.6% (95% CI 24.3–16.9, n = 1116) had a complete FPE. More than three EVT device passes were required in 21.0% (95% CI 19.8–22.2, n = 930) of cases and 27.9% (95% CI 36.7–29.2, n = 1380) of patients achieved a favorable outcome at 3 months.
Baseline characteristics and outcomes of study population (N = 6104).
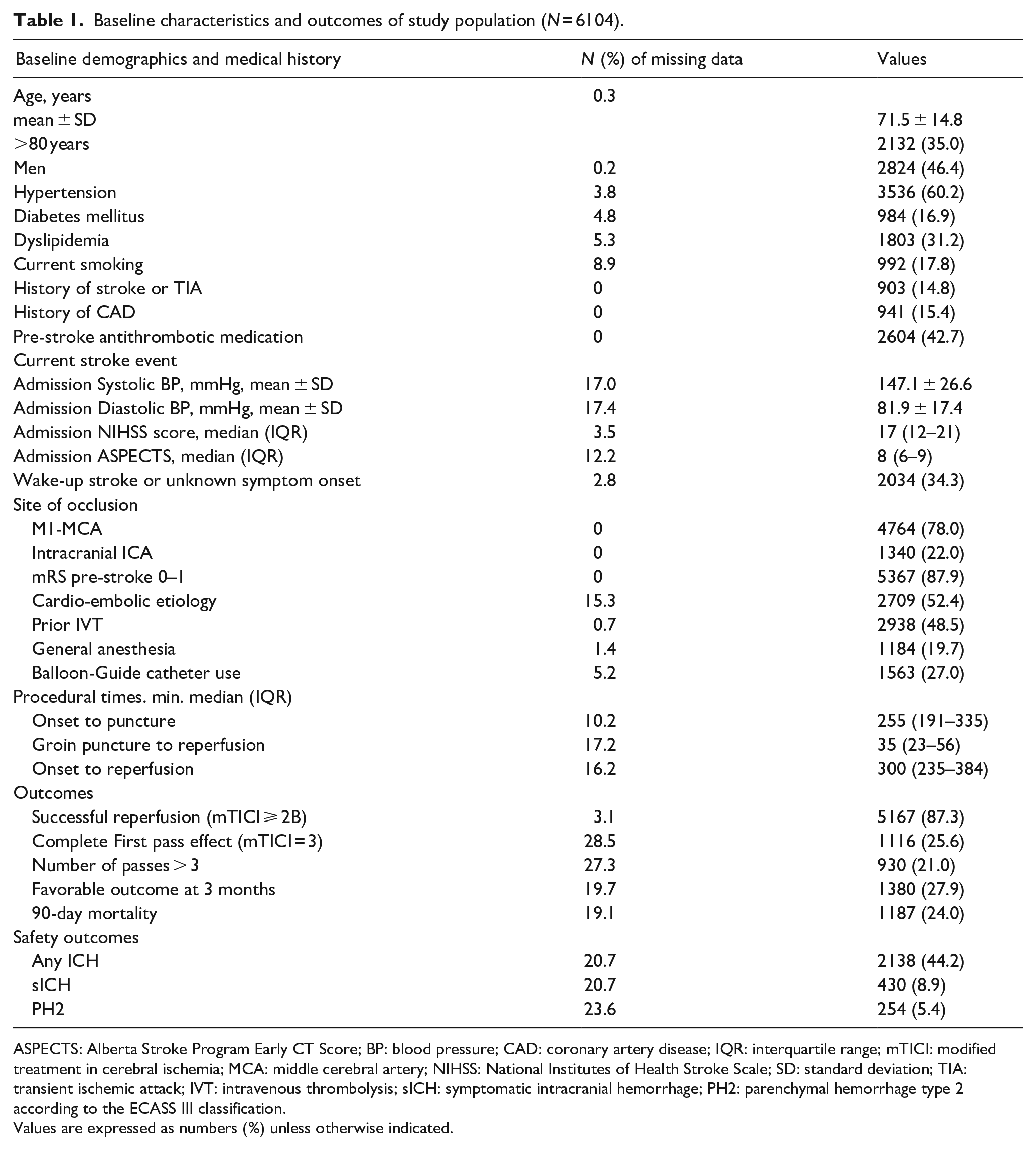
ASPECTS: Alberta Stroke Program Early CT Score; BP: blood pressure; CAD: coronary artery disease; IQR: interquartile range; mTICI: modified treatment in cerebral ischemia; MCA: middle cerebral artery; NIHSS: National Institutes of Health Stroke Scale; SD: standard deviation; TIA: transient ischemic attack; IVT: intravenous thrombolysis; sICH: symptomatic intracranial hemorrhage; PH2: parenchymal hemorrhage type 2 according to the ECASS III classification.
Values are expressed as numbers (%) unless otherwise indicated.
Temporal trends in main outcomes from January 2015 to January 2022
The rate of successful recanalization was 71.1% (95% CI 64.2–77.4) in 2015 by comparison to 89.6% (95% CI 84.4–93.5) in January 2022. As shown in Table 2, the rate of successful recanalization varied significantly over time, with a non-linear temporal trend. As shown in Figure 1(a), a decelerating slope increase was observed, with a linear increase from 2015 to 2017 and a plateau effect after 2018. (Supplemental Figure 1 and Supplemental Table 2).
Temporal trends in primary angiographic and clinical outcomes from January 2015 to January 2022 in patients treated by EVT for M1-MCA or intracranial ICA occlusions.
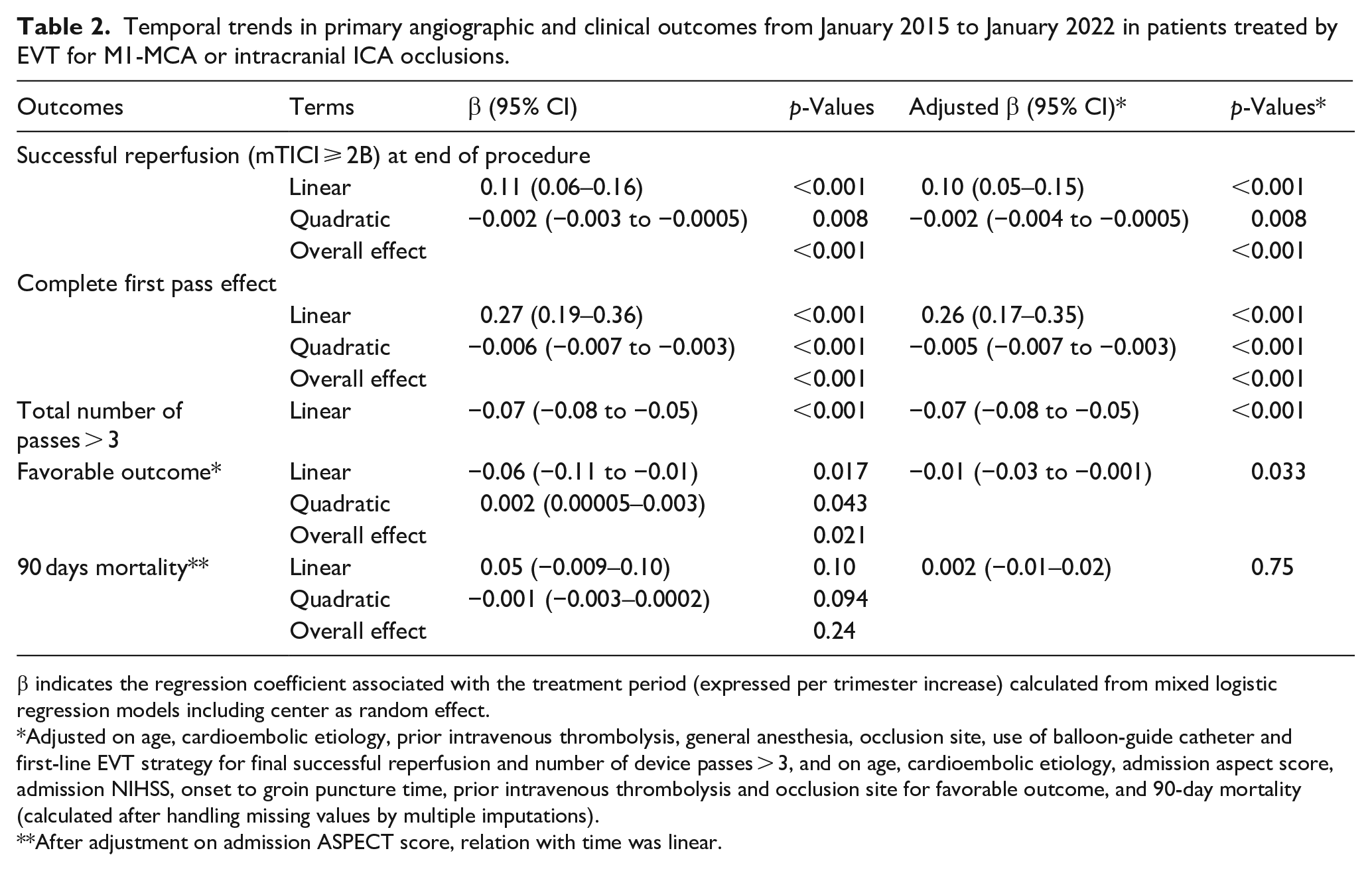
β indicates the regression coefficient associated with the treatment period (expressed per trimester increase) calculated from mixed logistic regression models including center as random effect.
Adjusted on age, cardioembolic etiology, prior intravenous thrombolysis, general anesthesia, occlusion site, use of balloon-guide catheter and first-line EVT strategy for final successful reperfusion and number of device passes > 3, and on age, cardioembolic etiology, admission aspect score, admission NIHSS, onset to groin puncture time, prior intravenous thrombolysis and occlusion site for favorable outcome, and 90-day mortality (calculated after handling missing values by multiple imputations).
After adjustment on admission ASPECT score, relation with time was linear.
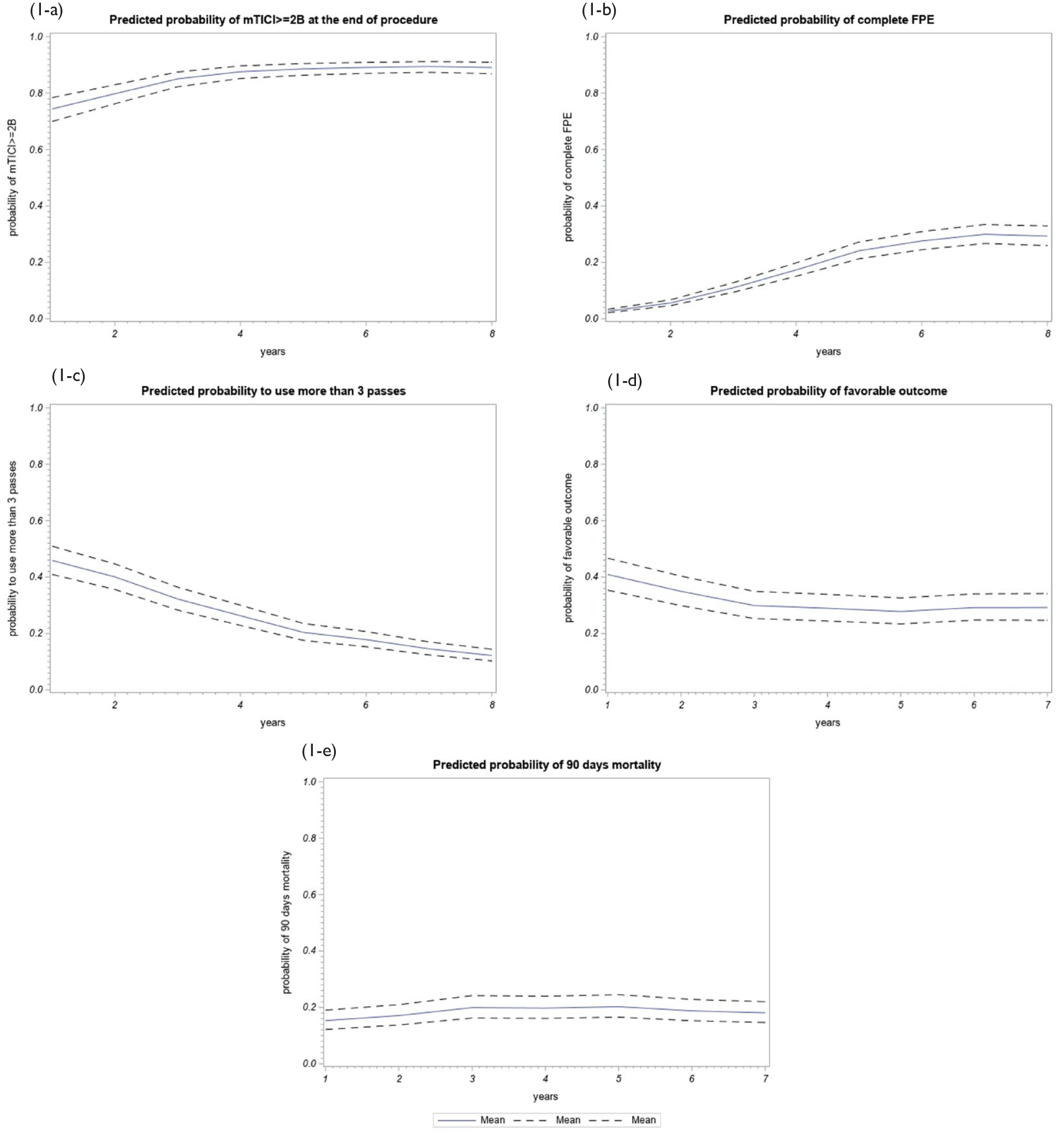
Predicted probabilities of outcomes over time from January 2015 to January 2022. Dashed line represent 95% CI.
In the same way, the rate of complete FPE significantly increased over time, with 4.6% (1.0–12.9) in 2015 by comparison to 28.9% (22.3–36.3) in January 2022. As shown in Figure 1(b), a decelerating slope increase was found, with a linear increase from 2015 to 2020 and a plateau after January 2020.
The percentage of patients having undergone >3 EVT device passes decreased over the years from 43.1% in 2015 to 17.5% in 2021, with a significant linear time effect (regression coefficient = −0.06; 95% CI −0.08 to −0.05, p < 0.001; Table 2 and Figure 1). Concerning the favorable outcome, after adjustment on pre-specified covariates, we found a significant decrease in rate over time (regression coefficient = −0.01; 95% CI −0.03 to −0.001, p = 0.033; Table 2 and Figure 1). No change was found for 90-day mortality over time in univariate and multivariate analyses (Table 2 and Figure 1).
Similar results were found in sensitivity analyses performed in the population with pre-stroke MRS 0–1 (sensitivity analyses 1, Supplemental Table 6) and in the population included in a center which recruited patients since 2015 (sensitivity analyses 2, Supplemental Table 7), except that the rate of favorable outcome did not increase over time in sensitivity analyses 1 (p = 0.12).
Temporal trends in successful reperfusion, complete FPE and favorable outcome according to key subgroups
Temporal trends from January 2015 to January 2022 in successful reperfusion at the end of procedure, complete FPE and in favorable outcomes according to key subgroups are presented in Supplemental Tables 3–5. A significant heterogeneity of temporal trends in successful reperfusion according to first-line EVT strategy was found (p-het = 0.018). The increasing temporal trend observed in successful reperfusion rates was only significant in patients treated with contact aspiration as first-line (adjusted overall effect p = 0.010) (Supplemental Table 3 and Figure 2). No heterogeneity was found according to occlusion site, use or not of BGC, cardioembolic etiology and age subgroups (p for heterogeneity all >0.26, Supplemental Table 3). Regarding the complete FPE and favorable outcome, we found no evidence of temporal trends whatever the subgroups (Supplemental Tables 4 and 5).
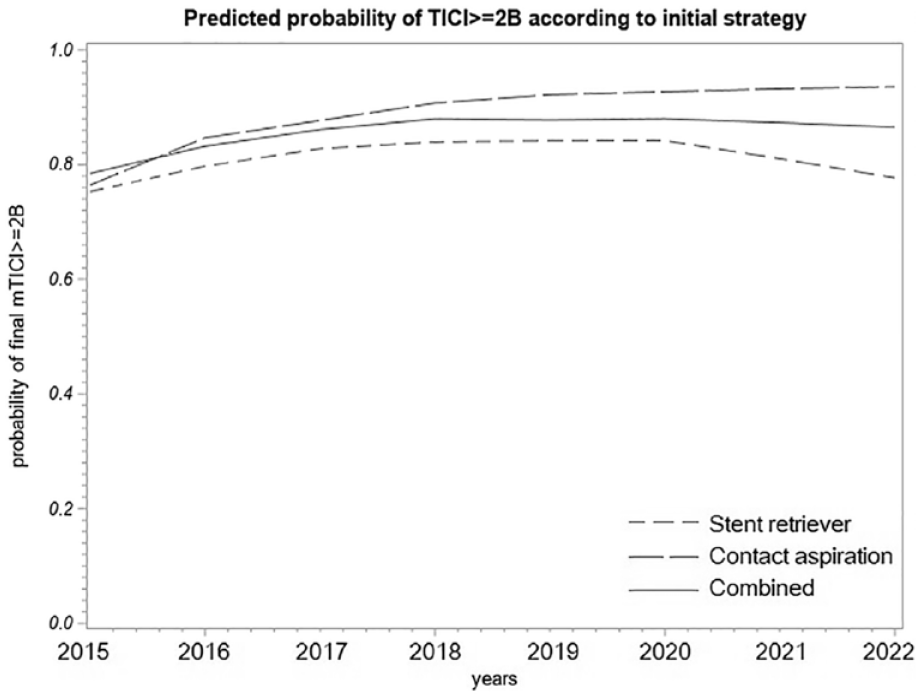
Predicted probabilities of successful final reperfusion (mTICI ⩾ 2B) over time from January 2015 to January 2022 according to the first-line EVT strategy.
Discussion
In this 7-year-old large multicenter registry of ischemic stroke patients treated with EVT, we analyzed the temporal evolution of angiographic recanalization results. We found a significant increase over time in the rate of successful recanalization and complete FPE as well as a significant decrease in the rate of >3 device passes. Furthermore, we highlight disparities of temporal trends only in successful reperfusion rates at the end of the procedure regarding the first-line strategy chosen. We found no such heterogeneities comparing different ages, location of occlusion, use of BGC, or stroke etiology for the rate of successful reperfusion rates at the end of the procedure, the FPE or the rate of >3 device passes.
Considering the rate of mTICI2b at the end of the procedure, we observed in our study a decelerating slope increase, with a linear increase up to 2017 and a plateau effect after 2018. Indeed, a significant subset of clots still remain recalcitrant to current strategies that is, typically fibrin rich or calcified thrombi.25–27 This failure is because, during retrieval, devices remain compressed by the organized clot and slide between it and the vessel wall without any removal effect. Novel stent retrievers designed to improve the incorporation and removal of organized thrombi appear to be promising strategies to improve FPE, number of passes, and final TICI.28,29
The rate of complete FPE significantly increased over time until January 2020 and the rate of patients requiring >3 EVT device passes decreased with a significant linear time effect until the last period considered in the study (January 2022). These observations point to the relevance of more ambitious endpoints than the final (at the end of the procedure) « substantial perfusion with distal branch filling of ⩾50% of territory visualized » (TICI 2b) previously considered as technically successful EVT. 30 Indeed, although since 2020 the rate of complete perfusion with normal filling of all distal branches in one pass (true FPE TICI 3) stagnates, there may still be room for improvement to avoid exceeding three passes. Indeed, previous studies have suggested that occurrence of hemorrhagic transformation increases when the degree of revascularization decreases and when the number of device passes increases beyond 3.17,31
Our study, based on a real-life registry, is the first to investigate longitudinally and over several years the evolution of angiographic and clinical results after EVT in such a large population. Recently, an analysis of the MR CLEAN registry found better recanalization rates since July 2016 compared to the slot between 2014 and June 2016. 32 However, in this study, there were no continuous or longitudinal assessments of the temporal evolution of angiographic recanalization results. Furthermore, we have been able to adjust our longitudinal analysis on different potential confounding factors that may have influenced the recanalization rates, such as occlusion location, age, anesthetic regimen, and prior intravenous thrombolysis. Hence, operators’ learning curves and improvement of medical devices are reliably and clearly highlighted as independent explanations for observed temporal trends in outcomes after EVT in this population. This is the main finding of our study because such an analysis has never been performed in this way.
Of note, at the individual level, the operator’s learning curve has also been emphasized. In the ETIS registry and two additional high-volume stroke centers, authors recently found that among 36 operators having performed a median of 97.5 EVT procedures, increasing experience in EVT is associated with significantly shorter procedural duration and better recanalization rates during the operator’s first 100 EVT procedures. 33 However, this latter study did not consider the potential evolution of « macroscopic » results of EVT over the study period as we have highlighted in this study.
Regarding the favorable outcome, one can assume that the improvement in recanalization rates would translate into better clinical outcomes. Despite this assumption, we observed a tendency toward a decrease in the rate of favorable outcome from January 2015 to January 2017 and thereafter no significant change over time. We attempted to adjust our analysis for age, admission NIHSS score, onset to groin puncture time, prior intravenous thrombolysis and occlusion site. However, it is important to integrate the expanding indications since 2015, with EVT progressively being considered for increasingly older patients, more extensive ischemic cores and later time-windows.34–36 The evidence of a preserved therapeutic benefit in these subgroups, usually associated with an a priori poorer prognosis, is likely to have influenced the clinical outcome over the study period. Furthermore, IVT rates have decreased markedly over the years in the observed population of EVT treated patients. Contraindications to IVT, apart from being a marker for the proportion of patients arriving >4.5 h, is also a marker of general comorbidity, which supports the fact that the population has changed (see Supplemental Table 2).
It is noteworthy that our timeline of inclusion covered the COVID epidemic in France that induced a significant decrease in the number of patients treated with EVT during the first stages and alarming indicators of lengthened care delays. 37 However, there was no difference in the rate of successful reperfusion (82.3% vs 82%; p = 0.932) or in-hospital mortality (12.9% vs 17.3%; p = 0.124) before compared to during the epidemic period. The evolution of EVT devices, including the use of BGC and more complex SR designs, certainly led to improved recanalization rates, but it appears that it was principally the use of larger diameter aspiration catheters that drove the improvement of recanalization results during the study period. 38
Based on a description of EVT outcomes in a large multicenter national registry, our study provides reliable and detailed endpoints for EVT result assessments over time. Indeed, efforts should focus on the rate of FPE for which there is still room for improvement. To a larger extent, our work reveals another aspect of the temporal trends for results of Endovascular treatment of large cerebral vessel occlusion. The use of SR alone dramatically decreased over time due to the seducing good results when SR is associated with CA (i.e. CAPTIVE, ARTS, SOLUMBRA, or SAVE).39–42 However, we may question whether, in the absence of this association, the strategy of the simple SR alone would still have benefited from the improvement of complex stent retriever designs along the period of our study. The curves of recanalization improvements for each different device are censored due to the increasing utilization of new devices. It appears that technical innovation progresses faster than the interventionists’ learning curves with a given device (e.g. SR and CA). It is noteworthy that a recent Chinese study found, among 1069 LVO patients treated by SR as first-line in EVT and assessed by an external core-lab, rates of successful recanalization after all procedures of 91.2%, complete recanalization after all procedures of 70.2%, and first-pass complete recanalization of 34.8%. The aspiration catheter was not widely used throughout China between 2017 and 2019; interventionists preferred to use the SR alone for the first-line EVT procedure during this study period. 43
Limitations of our study include the lack of core lab evaluation for TICI grade scaling after EVT. Moreover, precise information concerning the CA and SR devices (manufacturer, length, diameters) were not included in our analysis. Finally, there was neither imaging data nor thrombus histology available to demonstrate the previously suggested relationship of recanalization results with thrombus type.44,45 In our study, we focused on the temporal evolution of angiographic recanalization results. Besides, it would also be very interesting to use the same longitudinal methodology applied to the intra-hospital delay with milestones at the arrival in CSC, imaging, entrance to the angiosuite, and groin puncture. Furthermore, data from years 2015 to 2021 are complete but for 2022, only January data were used. Last, our analysis focused only on the first-line strategy of EVT. We did not account for second line strategies after one or more passes.
Conclusion
In this 7-year-old large registry of ischemic stroke patients treated with EVT, we analyzed the temporal evolution of angiographic outcomes and found a significant decrease over time in the rate of >3 device passes as well as a significant increase in complete FPE and in final successful reperfusion. The improvement of CA devices appears to have played an important part in this latter temporal trend.
Supplemental Material
sj-pdf-1-eso-10.1177_23969873231180338 – Supplemental material for Temporal trends in results of endovascular treatment of anterior intracranial large cerebral vessel occlusion: A 7-year study
Supplemental material, sj-pdf-1-eso-10.1177_23969873231180338 for Temporal trends in results of endovascular treatment of anterior intracranial large cerebral vessel occlusion: A 7-year study by Romain Bourcier, Arturo Consoli, Jean-Philippe Desilles, Julien Labreuche, Maeva Kyheng, Hubert Desal, Quentin Alias, Benjamin Gory, Cyril Dargazanli, Kévin Janot, François Zhu, Bertrand Lapergue and Gaultier Marnat in European Stroke Journal
Footnotes
Appendix

| Centres | Intervenants |
|---|---|
| 001-Foch | Bertrand LAPERGUE |
| 001-Foch | Adrien WANG |
| 001-Foch | Arturo CONSOLI |
| 001-Foch | Oguzhan COSKUN |
| 001-Foch | Federico DI MARIA |
| 001-Foch | Silvia PIZZUTO |
| 001-Foch | Alessandro SGRECCIA |
| 001-Foch | Charline BENOIT |
| 001-Foch | Lucas GORZA |
| 001-Foch | David WEISENBURGER-LILE |
| 001-Foch | Waliyde JABEUR |
| 001-Foch | TCHIKVILADZE Maia |
| 001-Foch | Serge EVRARD |
| 001-Foch | Georges RODESCH |
| 002-FOR | Raphaël BLANC |
| 002-FOR | Jean-Philippe DESILLES |
| 002-FOR | Michel PIOTIN |
| 002-FOR | Stanislas SMAJDA |
| 002-FOR | Simon ESCALARD |
| 002-FOR | Benjamin MAIER |
| 002-FOR | Hocine REDJEM |
| 002-FOR | Mikael MAZHIGI |
| 002-FOR | François DELVOYE |
| 002-FOR | Amira AL RAAISI |
| 002-FOR | William BOISSEAU |
| 003-Lyon | Omer EKER |
| 003-Lyon | Tae-Hee CHO |
| 003-Lyon | Laurent DEREX |
| 003-Lyon | Julia FONTAINE |
| 003-Lyon | Laura MECHTOUFF |
| 003-Lyon | Norbert NIGHOGHOSSIAN |
| 003-Lyon | Elodie ONG |
| 003-Lyon | Lucie RASCLE |
| 003-Lyon | Roberto RIVA |
| 003-Lyon | Françis TURJMAN |
| 003-Lyon | Morgane LAUBACHER |
| 003-Lyon | Mehdi BEYRAGUED |
| 003-Lyon | Yves BERTHEZENE |
| 003-Lyon | Marc HERMIER |
| 003-Lyon | Ameli ROXANNA |
| 003-Lyon | Alexandre BANI-SADR |
| 003-Lyon | Andrea FILIP |
| 003-Lyon | Matteo CAPPUCCI |
| 004-Nantes | Romain BOURCIER |
| 004-Nantes | Benjamin DAUMAS DUPORT |
| 004-Nantes | Pierre Louis ALEXANDRE |
| 004-Nantes | Cédric LENOBLE |
| 004-Nantes | Hubert DESAL |
| 004-Nantes | Solene DE GAALON |
| 004-Nantes | Benoît GUILLON |
| 004-Nantes | Cécile PRETERRE |
| 004-Nantes | Guillaume TESSIER |
| 004-Nantes | Arthur LIONNET |
| 005-Nancy | Benjamin GORY |
| 005-Nancy | Lisa HUMBERTJEAN-SELTON |
| 005-Nancy | René ANXIONNAT |
| 005-Nancy | Anne-Laure DERELLE |
| 005-Nancy | Liang LIAO |
| 005-Nancy | Emmanuelle SCHMITT |
| 005-Nancy | Sophie PLANEL |
| 005-Nancy | Sébastien RICHARD |
| 005-Nancy | Gioia MIONE |
| 005-Nancy | Jean-Christophe LACOUR |
| 005-Nancy | Marian DOUARINOU |
| 005-Nancy | Gabriela HOSSU |
| 005-Nancy | Bailiang CHEN |
| 005-Nancy | Gérard AUDIBERT |
| 005-Nancy | Agnès MASSON |
| 005-Nancy | Lionel ALB |
| 005-Nancy | Marine BEAUMONT |
| 005-Nancy | Adriana TABARNA |
| 005-Nancy | Marcela VOICU |
| 005-Nancy | Grégoire BARTHEL |
| 005-Nancy | Iona PODAR |
| 005-Nancy | Madalina BREZEANU |
| 005-Nancy | Marie REITTER |
| 005-Nancy | François ZHU |
| 006-Bordeaux | Gaultier MARNAT |
| 006-Bordeaux | Jean-Sébastien LIEGEY |
| 006-Bordeaux | Pierre BRIAU |
| 006-Bordeaux | Lisa PAPILLON |
| 006-Bordeaux | Igor SIBON |
| 006-Bordeaux | Xavier BARREAU |
| 006-Bordeaux | Jean PAPAXANTHOS |
| 006-Bordeaux | Jérome BERGE |
| 006-Bordeaux | Sabrina DEBRUXELLES |
| 006-Bordeaux | Stephane OLINDO |
| 006-Bordeaux | Mathilde POLI |
| 006-Bordeaux | Pauline RENOU |
| 006-Bordeaux | Sharmila SAGNIER |
| 006-Bordeaux | Thomas TOURDIAS |
| 006-Bordeaux | Thomas COURRET |
| 006-Bordeaux | Ludovic LUCAS |
| 007-Montpellier | Cyril DARGAZANLI |
| 007-Montpellier | Vincent COSTALAT |
| 007-Montpellier | Isabelle MOURAND |
| 007-Montpellier | Caroline ARQUIZAN |
| 007-Montpellier | Lucas CORTI |
| 007-Montpellier | Adrien TER SCHIPHORST |
| 007-Montpellier | CAGNAZZO Federico |
| 008-Kremlin Bicêtre | Laurent SPELLE |
| 008-Kremlin Bicêtre | Jildaz CAROFF |
| 008-Kremlin Bicêtre | Christian DENIER |
| 008-Kremlin Bicêtre | Vanessa CHALUMEAU |
| 008-Kremlin Bicêtre | Cristian MIHALEA |
| 008-Kremlin Bicêtre | Nicolas LEGRIS |
| 008-Kremlin Bicêtre | Augustin OZANNE |
| 008-Kremlin Bicêtre | Leon IKKA |
| 008-Kremlin Bicêtre | Olivier CHASSIN |
| 008-Kremlin Bicêtre | Sophie GALLAS |
| 008-Kremlin Bicêtre | Laura VENDITTI |
| 008-Kremlin Bicêtre | Mariana SAROV |
| 008-Kremlin Bicêtre | Jonathan CORTESE |
| 009-Rennes | Jean-Christophe FERRE |
| 009-Rennes | Stephane VANNIER |
| 009-Rennes | Thomas RONZIERE |
| 009-Rennes | Maria Veronica LASSALLE |
| 009-Rennes | Jean-Yves GAUVRIT |
| 009-Rennes | Clément TRACOL |
| 009-Rennes | Abdelghani Fakhreddine BOUSTIA |
| 009-Rennes | Cécile MALRAIN |
| 009-Rennes | Edouard BEAUFRETON |
| 009-Rennes | Thibault LAPOTRE |
| 009-Rennes | Quentin ALIAS |
| 009-Rennes | Julien HISSIER |
| 009-Rennes | Maud GUILLEN |
| 010-Amiens | Cyril CHIVOT |
| 010-Amiens | Audrey COURSELLE |
| 010-Amiens | Elisa OUIN |
| 010-Amiens | Chantal LAMY |
| 010-Amiens | Kevin DELAFORGE |
| 010-Amiens | Manuel FERNANDEZ |
| 010-Amiens | Jérémie VIAL |
| 010-Amiens | Quentin LAFARTE |
| 010-Amiens | Xavier DESDOIT |
| 011-Brest | Serge TIMSIT |
| 011-Brest | Aurore JOURDAIN |
| 011-Brest | Jean-Christophe GENTRIC |
| 011-Brest | Julien OGNARD |
| 011-Brest | Irina VIAKHIREVA |
| 011-Brest | Jordan CORIS |
| 011-Brest | Sabine PRUD’HON |
| 011-Brest | François-Mathias MERRIEN |
| 011-Brest | Denis MARECHAL |
| 011-Brest | Marie BRUGUET |
| 011-Brest | Pierre Yves ROUSSEAU |
| 011-Brest | Philippe GOAS |
| 012-Caen | Marion BOULANGER |
| 012-Caen | Emmanuel TOUZE |
| 012-Caen | Denis VIVIEN |
| 012-Caen | Charlotte BARBIER |
| 012-Caen | Romain SCHNECKENBURGER |
| 012-Caen | Fabrizio SALARIS |
| 012-Caen | Julien COGEZ |
| 012-Caen | Sophie GUETTIER |
| 012-Caen | Estelle LA PORTE |
| 012-Caen | Jean BOUCHART |
| 013-Limoges | Charbel MOUNAYER |
| 013-Limoges | Aymeric ROUCHAUD |
| 013-Limoges | Suzana SALEME |
| 013-Limoges | Géraud FORESTIER |
| 014-Pitié-Salpêtrière | Frédéric CLARENCON |
| 014-Pitié-Salpêtrière | Charlotte ROSSO |
| 014-Pitié-Salpêtrière | Sara LEDER |
| 014-Pitié-Salpêtrière | Flore BARONNET |
| 014-Pitié-Salpêtrière | Sophie CROZIER |
| 014-Pitié-Salpêtrière | Anne LEGER |
| 014-Pitié-Salpêtrière | Kevin PREMAT |
| 014-Pitié-Salpêtrière | Shotar EIMAD |
| 014-Pitié-Salpêtrière | Stéphanie LENCK |
| 014-Pitié-Salpêtrière | Nader SOUROUR |
| 014-Pitié-Salpêtrière | Laure BOTTIN |
| 014-Pitié-Salpêtrière | Sam GHAZANFARI |
| 014-Pitié-Salpêtrière | Marion YGER |
| 014-Pitié-Salpêtrière | Sonia ALAMOWITCH |
| 014-Pitié-Salpêtrière | Stephen DELORME |
| 014-Pitié-Salpêtrière | Aymeric WITTWER |
| 014-Pitié-Salpêtrière | Christine VASSILEV |
| 016-Ste Anne | Olivier NAGGARA |
| 016-Ste Anne | Guillaume TURC |
| 016-Ste Anne | Wagih BEN HASSEN |
| 016-Ste Anne | Basile KERLEROUX |
| 016-Ste Anne | Denis TRYSTRAM |
| 016-Ste Anne | Christine RODRIGUEZ-REGENT |
| 017-Rouen | Ozlem OZKUL-WERMESTER |
| 017-Rouen | Chrysanthi PAPAGIANNAKI |
| 017-Rouen | Evelyne MASSARDIER |
| 017-Rouen | Aude TRIQUENOT |
| 017-Rouen | Margaux LEFEBVRE |
| 017-Rouen | Julien BUREL |
| 018-Toulouse | Alain VIGUIER |
| 018-Toulouse | Christophe COGNARD |
| 018-Toulouse | Anne Christine JANUEL |
| 018-Toulouse | Jean-François ALBUCHER |
| 018-Toulouse | Lionel CALVIERE |
| 018-Toulouse | Jean-Marc OLIVOT |
| 018-Toulouse | Jean DARCOURT |
| 018-Toulouse | Nicolas RAPOSO |
| 018-Toulouse | Fabrice BONNEVILLE |
| 018-Toulouse | Guillaume BELLANGER |
| 018-Toulouse | Louis FONTAINE |
| 018-Toulouse | Philippe TALL |
| 019-Bayonne | Frédéric BOURDAIN |
| 019-Bayonne | Patricia BERNADY |
| 019-Bayonne | Guillaume BALLAN |
| 019-Bayonne | Stephanie BANNIER |
| 019-Bayonne | Emmanuel ELLIE |
| 019-Bayonne | Olivier FLABEAU |
| 019-Bayonne | Julia POTENZA |
| 019-Bayonne | Antoine SOULAGES |
| 019-Bayonne | Laurent LAGOARDE-SEGOT |
| 019-Bayonne | Hélène CAILLIEZ |
| 019-Bayonne | Louis VEUNAC |
| 019-Bayonne | David HIGUE |
| 020-Vannes | Anthony LEBRAS |
| 020-Vannes | Sarah EVAIN |
| 020-Vannes | Benoit PEGAT |
| 020-Vannes | Arnaud LE GUEN |
| 020-Vannes | François CHEDEVILLE |
| 020-Vannes | Jérémy JOUAN |
| 021-Pau | Stéphanie DEMASLES |
| 021-Pau | Johann Sebastian RICHTER |
| 021-Pau | Bruno Thierry BARROSO |
| 021-Pau | Camille DAHAN |
| 021-Pau | Alexis GONNET |
| 021-Pau | Régis HUBRECHT |
| 021-Pau | Zoé LEPINE |
| 021-Pau | Hélène CASTAGNET |
| 021-Pau | Raluca MARASESCU |
| 022-Grenoble | Olivier HECK |
| 022-Grenoble | Pauline CUISENIER |
| 022-Grenoble | Olivier DETANTE |
| 022-Grenoble | Isabelle FAVRE WIKI |
| 022-Grenoble | Clémentine BONAZ |
| 022-Grenoble | GARAMBOIS Katia |
| 022-Grenoble | Loic LEGRIS |
| 022-Grenoble | Adrian KASTLER |
| 022-Grenoble | Kamel BOUBAGRA |
| 022-Grenoble | Corentin BERTHET |
| 022-Grenoble | Stephane Charara |
| 024-Strasbourg | Valérie WOLFF |
| 024-Strasbourg | Raoul POP |
| 024-Strasbourg | Véronique QUENARDELLE |
| 024-Strasbourg | Valérie LAUER |
| 024-Strasbourg | Raoul POP |
| 024-Strasbourg | Irène PIERRE-PAUL |
| 024-Strasbourg | Roxana GHEOCA |
| 024-Strasbourg | Malwina TRZECIAK |
| 026-Reims | Solène MOULIN |
| 026-Reims | HUA Vi Tuan |
| 026-Reims | Paolo PAGANO |
| 026-Reims | Alexandre DOUCET |
| 026-Reims | Christophe GELMINI |
| 026-Reims | Pierre-François MANCEAU |
| 026-Reims | Laurentiu PAIUSAN |
| 026-Reims | Isabelle SERRE |
| 026-Reims | Sébastien SOIZE |
| 026-Reims | Thi Ngoc Phuong NGUYEN |
| 026-Reims | Maher SAHNOUN |
| 026-Reims | Nathalie CAUCHETEUX |
| 028-Clermont-Ferrand | Anna FERRIER |
| 028-Clermont-Ferrand | Abderrahim ZERROUG |
| 028-Clermont-Ferrand | Ricardo MORENO |
| 028-Clermont-Ferrand | Emmanuel CHABERT |
| 028-Clermont-Ferrand | Elie LTEIF |
| 028-Clermont-Ferrand | Pauline PARIS |
| 028-Clermont-Ferrand | Nathalie BOURGOIS |
| 028-Clermont-Ferrand | Marie RAQUIN |
| 029-Angers | Anne PASCO-PAPON |
| 029-Angers | Jean Baptiste GIROT |
| 029-Angers | Alderic LECLUSE |
| 029-Angers | Sophie GODARD |
| 029-Angers | Vincent L’ALLINEC |
| 030-Tours | Kevin JANOT |
| 030-Tours | Richard BIBI |
| 030-Tours | Marie GAUDRON |
| 030-Tours | Arnaud BRETONNIERE |
| 030-Tours | Mariam ANNAN |
| 030-Tours | Héloïse IFERGAN |
| 030-Tours | Grégoire BOULOUIS |
| 030-Tours | Marco PASI |
| 030-Tours | Séverine DEBIAIS |
| 030-Tours | Elisabeth MOLINIER |
| 032-Bar le Duc | Anthony WIETRICH |
| 032-Bar le Duc | Valérie RUCHE |
| 032-Bar le Duc | Karine LAVANDIER |
| 033-Dijon | Yannick BEJOT |
| 033-Dijon | Brivale LEMOGNE |
| 033-Dijon | Fédéric RICOLFI |
| 033-Dijon | Laura BAPTISTE |
| 033-Dijon | Pierre THOUANT |
| 033-Dijon | Gaulthier DULOQUIN |
| 033-Dijon | Pierre olivier COMBY |
| 034-Besançon | Guillaume CHARBONNIER |
| 034-Besançon | Louise BONNET |
| 034-Besançon | Nicolas RAYBAUD |
| 034-Besançon | Benjamin BOUAMRA |
| 034-Besançon | Thierry MOULIN |
| 034-Besançon | Alessandra BIONDI |
Acknowledgements
We thank Mary Pellegrin for help in editing the final version of the manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
Local ethical committees approved data collection and analysis.
Informed consent
Verbal informed consent was obtained from legally authorized representatives before the study.
Guarantor
RB is the guarantor.
Contributorship
All authors have made substantial contributions and have approved the final submitted version.
Trial registration
Endovascular Treatment in Ischemic Stroke; ClinicalTrials.gov Identifier: NCT03776877.
Data availability statement
The data that support the findings of this study are available from the corresponding author upon reasonable request.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.