
Abstract
Background:
There is conflicting evidence as to whether intra-arterial thrombolysis (IAT) adds benefit in patients with acute stroke who undergo mechanical thrombectomy (MT).
Methods:
We conducted a systematic review to identify studies that evaluate IAT in patients with acute stroke who undergo MT. Data were extracted from relevant studies found through a search of PubMed, Scopus, and Web of Science until February 2023. Statistical pooling with random effects meta-analysis was undertaken to evaluate odds of functional independence, mortality, and near-complete or complete angiographic recanalization with IAT compared to no IAT.
Results:
A total of 18 studies were included (3 matched, 14 unmatched, and 1 randomized). The odds ratio (OR) for functional independence (modified Rankin Scale: 0–2) at 90 days was 1.14 (95% confidence interval (CI): 0.95–1.37, p = 0.17, 16 studies involving 7572 patients) with IAT with moderate between-study heterogeneity (I2 = 38.1%). The OR for functional independence with IAT was 1.28 (95% CI: 0.92–1.78, p = 0.15) in studies that were either matched or randomized and 1.24 (95% CI: 0.97–1.58, p = 0.08) in studies with the highest quality score. IAT was associated with higher odds of near-complete or complete angiographic recanalization (OR: 1.65, 95% CI: 1.03–2.65, p = 0.04) in studies that were either matched or of randomized comparisons.
Conclusion:
Although the odds of functional independence appeared to be higher with IAT and MT compared with MT alone, none of the results were statistically significant. A prominent effect of the design and quality of the studies was observed on the association between IAT and functional independence at 90 days.
Keywords
Introduction
In patients with acute ischemic stroke (AIS) who undergo endovascular treatment, intra-arterial thrombolysis (IAT) is recommended in the American Stroke Association/American Heart Association (ASA/AHA) guidelines since 2013, 1 with a preference for mechanical thrombectomy (MT) over IAT alone according to the ASA/AHA 2019 guidelines. 2 However, there is conflicting evidence as to whether concurrent IAT adds any additional benefit if MT is already being performed. Recent trials3,4 have used MT alone without intra-arterial (IA) thrombolytics to reduce the occurrence of post-procedure intracranial hemorrhage (ICH). Although such trials3,4 demonstrated that MT increased (compared with no MT) the rates of functional independence in AIS patients, almost one-third of patients did not achieve adequate tissue perfusion on magnetic resonance imaging (MRI) and/or functional independence despite recanalization following MT. Therefore, IAT is used concurrently with MT with considerable variation in practice between sites5,6 to improve both the rates and time to achieve angiographic recanalization and distal arterial perfusion by acting on sites not amenable to MT.7–9 There are two previous systematic reviews and meta-analyses by Chen et al. 10 and Kaesmacher et al., 11 which have provided conflicting results. A more conclusive analysis may be possible with the availability of additional studies5,12–17 including results from the randomized Chemical Optimization of Cerebral Embolectomy (CHOICE) 17 clinical trial. We performed an updated systematic review of the literature to evaluate the effect of IAT as an adjunct to MT.
Methods
Literature search strategy
This systematic review and meta-analysis were conducted and reported according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines. 18 Three reviewers (A.L., I.N.A., and D.K.) searched the online databases of PubMed, Scopus, and Web of Science (from January 2012 until February 2023) to find all relevant observational studies, clinical trials, clinical studies, comparative studies, and multicenter studies. We also searched clinicaltrials.gov to identify any additional articles. We started the search from January 2012 to focus on contemporary MT devices that were initially approved in 201219 (see Supplemental Material for detailed search strategy). Relevant studies identified during the screening process then entered full-text review, in which full-text manuscripts were evaluated independently by reviewers (A.L., I.N.A., and D.K.) for eligibility, as well as reference lists from these studies to identify additional eligible studies. Any uncertainties about the inclusion of a study in the review were discussed with the study’s supervisor (A.I.Q.) for resolution.
Eligibility criteria
Included studies involved AIS patients (>18 years) with large-vessel occlusion in the anterior or posterior circulation, with data available for two treatment arms: (1) IAT given as an adjunct to MT treatment and (2) MT treatment alone without IAT. MT included aspiration techniques, stent-retrievers, stenting, and balloon angioplasty. IA thrombolytics considered were plasminogen activators. We excluded studies that reported on IA use of other medications such as glycoprotein IIb/IIIa inhibitors. A recent meta-analysis by Kaesmacher et al. 11 included observational data derived from randomized controlled trials in the HERMES (Highly Effective Reperfusion Using Multiple Endovascular Devices) collaboration that had IAT in the MT arm. Randomized-controlled trials that had relevant data included the MR CLEAN (Multicenter Randomized Clinical trial of Endovascular treatment for Acute ischemic stroke in the Netherlands), 20 ESCAPE (Endovascular Treatment for Small Core and Anterior Circulation Proximal Occlusion with Emphasis on Minimizing CT to Recanalization Times), 21 and THRACE (Trial and Cost Effectiveness Evaluation of Intra-arterial Thrombectomy in Acute Ischemic Stroke) 22 trials. Outcome data from the IAT with MT versus MT alone groups were extracted from this meta-analysis. 11 We excluded studies with duplicate data or no specific data regarding patients receiving adjunct IAT. We also excluded studies with less than 10 patients undergoing endovascular treatment. 23 In addition, included studies had to report at least one of the primary or secondary outcomes. The primary outcome in our study was functional independence at 90 days (modified Rankin Scale: 0–2). Secondary outcomes were all-cause mortality within 90 days, occurrence of post-MT symptomatic intracranial hemorrhage (sICH) as defined by each study, and successful reperfusion on angiogram (Thrombolysis in Cerebral Infarction [TICI]/ Thrombolysis in Myocardial Infarction [TIMI] score of ⩾2b). If the sICH definition was not available, then other surrogates (i.e. parenchymal hematoma type 2 (PH2) according to ECASS (European Cooperative Acute Stroke Study) criteria) were considered, as was also done in the meta-analysis by Kaesmacher et al., 11 as PH2 has been associated with a higher risk of early neurological deterioration. 24
Data extraction
Three reviewers (A.L., I.N.A., and D.K.) independently extracted study ID, author, year, characteristics, and quality data from included studies. The study characteristics that were extracted included (1) the proportion of the patient population receiving IAT, (2) the location of large-vessel occlusion in treated patients (anterior circulation (internal carotid artery (ICA), middle cerebral artery (MCA)) and/or basilar artery), (3) time to treatment (within 8 or 24 h of symptom onset), (4) type of comparison (matched, unmatched, or randomized), (5) type(s) of IAT used, (6) dosage of IAT given (if provided), and (7) timing of IAT (before or after MT). Primary and secondary outcome data and the sICH definitions applied in each study were also extracted.
Risk of bias assessment in studies
The quality of included observational studies5,6,12–16,20–22,25–31 was assessed by three independent reviewers (A.L., I.N.A., and D.K.) for risk of bias using the Newcastle–Ottawa Quality Scale (NOS) for Cohort Studies. 32 The NOS evaluates three quality parameters (selection, comparability, and outcome), with a maximum of 4 points for selection, 2 points for comparability, and 3 points for outcomes, with a maximum total score of 9 for each study, representing a good quality study. 32 Studies having a total score of less than five are identified as studies with a high risk of bias.33,34 For assessing the quality of the single randomized trial in our study, 17 we used a revised risk of bias (RoB-2) tool. 35 It evaluates the risk of bias as low, moderate, or high risk across different parameters (such as random sequence generation, allocation concealment, degree of blinding, attrition bias, or selective reporting) for an overall grading of low, moderate, or high risk of bias.
Statistical analysis
We calculated the odds ratio (OR) as effect size for each comparison for functional independence at 90 days, all-cause mortality within 90 days, post-MT sICH, and near-complete or complete recanalization. For each outcome, comparisons were analyzed using random effects models to account for heterogeneity, with a Mantel–Haenszel (MH) estimator for between-study heterogeneity statistic Q, and results displayed in forest plots. Heterogeneity was described using I² (the percentage of the residual variation that is attributable to between-study). We used meta-regression to identify any heterogeneity in effect due to study-level covariates including the location of occlusion in treated patients (middle cerebral artery only, middle cerebral or internal carotid arteries, any intracranial artery, or basilar artery only), time to treatment (⩽8 h and >8 h), comparator group (matched, unmatched, or randomized), and quality grade on the association between IAT and study outcomes. We tested for the presence and extent of publication bias using funnel plots. Adjusted effect sizes were then estimated by incorporating theoretically missing studies using the trim-and-fill approach. 36 We performed the following sensitivity analyses: (1) due to the presence of both funnel plot and between-study heterogeneity, we compared the fixed and random effects estimates of the intervention effect as recommended by Sterne et al. 37 ; (2) repeated the analysis after only including studies that used matched or randomized comparators; and (3) repeated the analysis after only including studies with the highest quality score (greater than 8). Statistical analyses were performed using R (version 4.2.0), R package dplyr (version 1.0.9), and meta (version 5.2-0). All estimates included a 95% confidence interval (CI) and p values <0.05 were considered statistically significant.
Results
Literature search and study characteristics
A flow diagram depicting the study selection for IAT in adjunct to MT is shown in Figure 1. A total of 1587 potentially relevant studies were found in the search. A total of 18 studies (17 nonrandomized observational studies and 1 randomized controlled trial) met the inclusion criteria. It is notable that two studies were excluded one of which had too small a sample size, 23 and the other study presented results that were not in a format that could be pooled along with the other studies. 38 A summary of study characteristics of included studies is shown in Table 1. Primary and secondary outcome data and definitions of sICH and successful reperfusion of included studies are shown in Supplemental Tables 1 and 2.
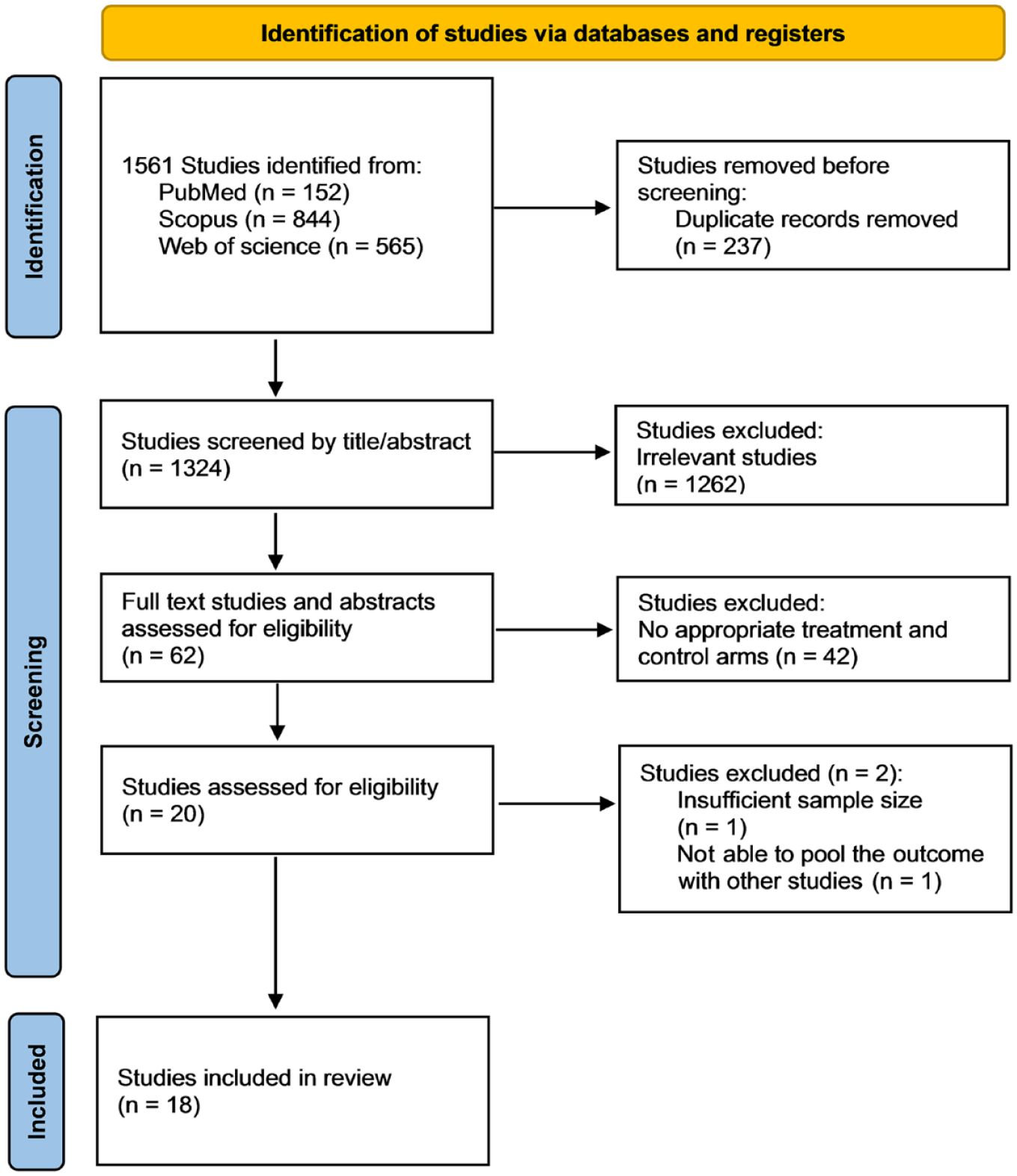
Flow chart depicting identification of studies through literature search.
Study characteristics of the included studies.
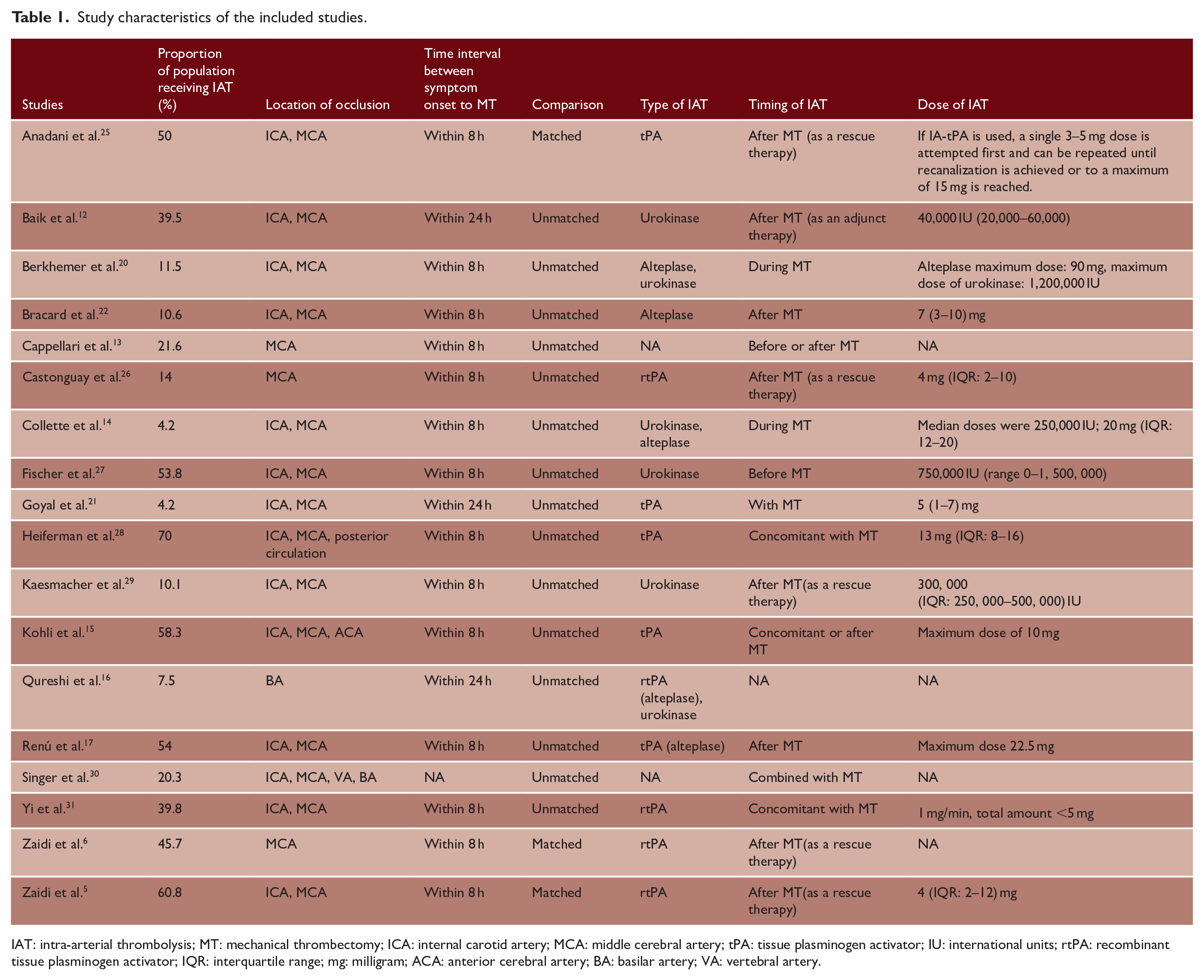
IAT: intra-arterial thrombolysis; MT: mechanical thrombectomy; ICA: internal carotid artery; MCA: middle cerebral artery; tPA: tissue plasminogen activator; IU: international units; rtPA: recombinant tissue plasminogen activator; IQR: interquartile range; mg: milligram; ACA: anterior cerebral artery; BA: basilar artery; VA: vertebral artery.
Study quality
The median quality grade was 8, with 11 studies having a quality grade of 8 or greater for risk of bias using the NOS scoring system5,6,12–16,20,25,29,31 (see Supplemental Tables 3 and 4). There was an overall low risk of bias using Rob-2 assessment tool for the randomized controlled trial. 17 The only potential of bias that was classified as moderate risk was due to pre-mature terminated early during the corona virus disease 2019 pandemic due to difficulty in recruitment.
Effect of IAT on functional independence at 90 days
The OR for functional independence at 90 days was 1.14 (95% CI: 0.95–1.37, p = 0.17, 16 studies involving 7572 patients) with IAT with moderate between-study heterogeneity (I2 = 38.1%; Figure 2(a)). A sizable asymmetry was detected in the funnel plot. After applying the trim and fill approach, the resulting adjusted OR for functional independence at 90 days slightly increased (OR: 1.16, 95% CI: 0.96–1.40, p = 0.13; Figure 2(b)). Similar results were observed in a fixed effect model (OR: 1.12, 95% CI: 0.97–1.30, p = 0.13). In the meta-regression, no relationship was identified between study-level covariates and effect size (p > 0.05). The OR for functional independence at 90 days with IAT was 1.28 (95% CI: 0.92–1.78, p = 0.15) in studies that were either matched or randomized comparisons, 1.24 (95% CI: 0.97–1.58, p = 0.08) in studies with the highest quality score, and 1.14 (95% CI: 0.94–1.38, p = 0.20) in observational studies.
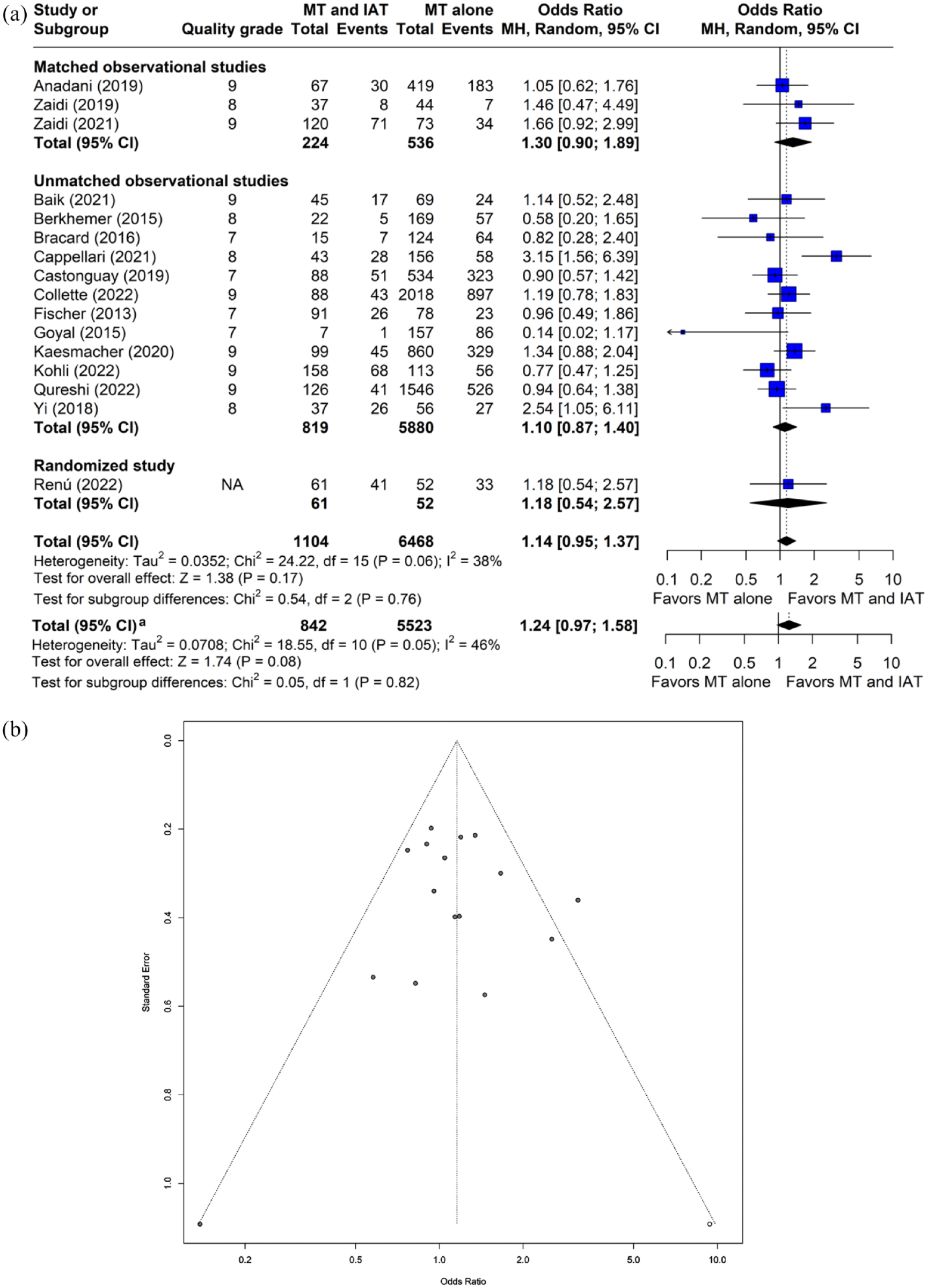
Plots of odds ratio for functional independence at 90 days (modified Rankin Scale score: 0–2) in patients undergoing MT with and without IAT. (a) Forest plot and hypothesis testing for heterogeneity, overall effect, and subgroup differences (b) Funnel plot for adjusting publication bias with published studies (filled circles) and trim-and-fill assigned studies (open circles). MT: mechanical thrombectomy; IAT: intra-arterial thrombolysis; MH: Mantel–Haenszel Test; CI: confidence interval.
Effect of IAT on all-cause mortality within 90 days
The OR for all-cause mortality within 90 days with IAT was 0.86 (95% CI: 0.71–1.05, p = 0.14, I2 = 0%, 14 studies, 5197 subjects, Figure 3(a)). A sizable asymmetry was detected in the funnel plot. After applying the trim and fill approach, the resulting adjusted OR for all-cause mortality at 90 days was 0.88 (95% CI: 0.72–1.07, p = 0.18; Figure 3(b)). Similar results were observed in a fixed effect model (OR: 0.86, 95% CI: 0.70–1.04, p = 0.12). In the meta-regression, the location of occlusion (category of middle cerebral or internal carotid arteries) had a significant effect on the association between IAT and all-cause mortality within 90 days (p = 0.04). The ORs for all-cause mortality within 90 days with IAT were 0.76 (95% CI: 0.50–1.14, p = 0.18) in studies that were either matched or randomized comparisons, 0.85 (95% CI: 0.67–1.08, p = 0.19) in studies of highest quality grade, and 0.88 (95% CI: 0.72–1.07, p = 0.20) in observational studies.
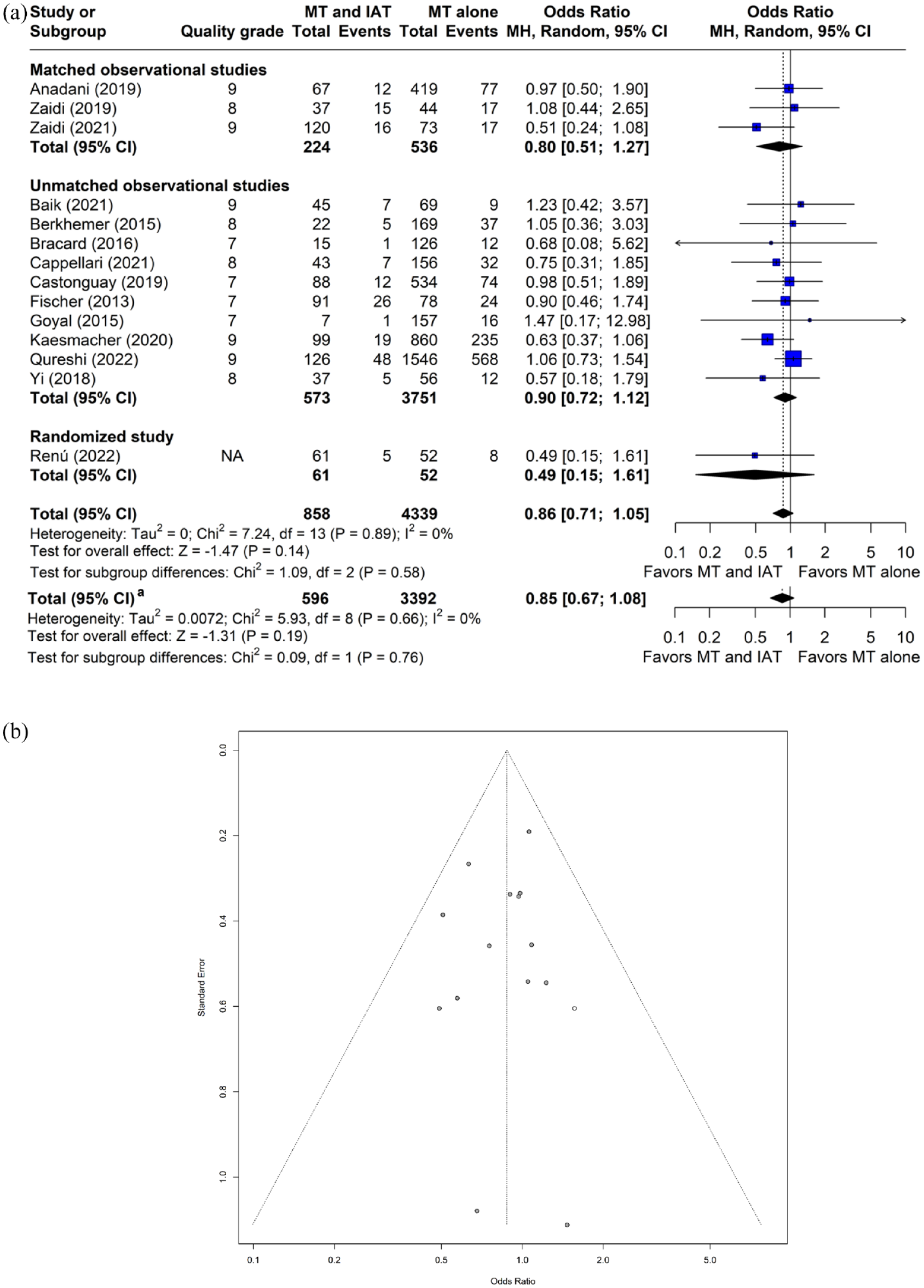
Plots of odds ratio for all-cause mortality within 90 days in patients undergoing MT with and without IAT. (a) Forest plot and hypothesis testing for heterogeneity, overall effect, and subgroup differences (b) Funnel plot for adjusting publication bias with published studies (filled circles) and trim-and-fill assigned studies (open circles). MT: mechanical thrombectomy; IAT: intra-arterial thrombolysis; MH: Mantel–Haenszel test; CI: confidence interval.
Effect of IAT on post-MT symptomatic intracerebral hemorrhage
The OR for post-MT sICH with IAT was 1.19 (95% CI: 0.89–1.58, p = 0.25, I2 = 0%, 17 studies, 8231 subjects, Figure 4(a)). A sizable asymmetry was detected in the funnel plot. After applying the trim and fill approach, the adjusted OR for sICH was 1.25 (95% CI: 0.94–1.66, p = 0.12; see Figure 4(b)). The OR for post-MT sICH with IAT was 1.12 (95% CI: 0.84–1.49, p = 0.43) in a fixed effect model. In the meta-regression, no relationship was identified between study-level covariates and effect size (p > 0.05). The ORs for post-MT sICH with IAT were 1.39 (95% CI: 0.61–3.18, p = 0.43) in studies that were either matched or randomized comparisons, 1.04 (95% CI: 0.72–1.49, p = 0.85) in studies of highest quality grade, and 1.21 (95% CI: 0.90–1.61, p = 0.20) in observational studies.
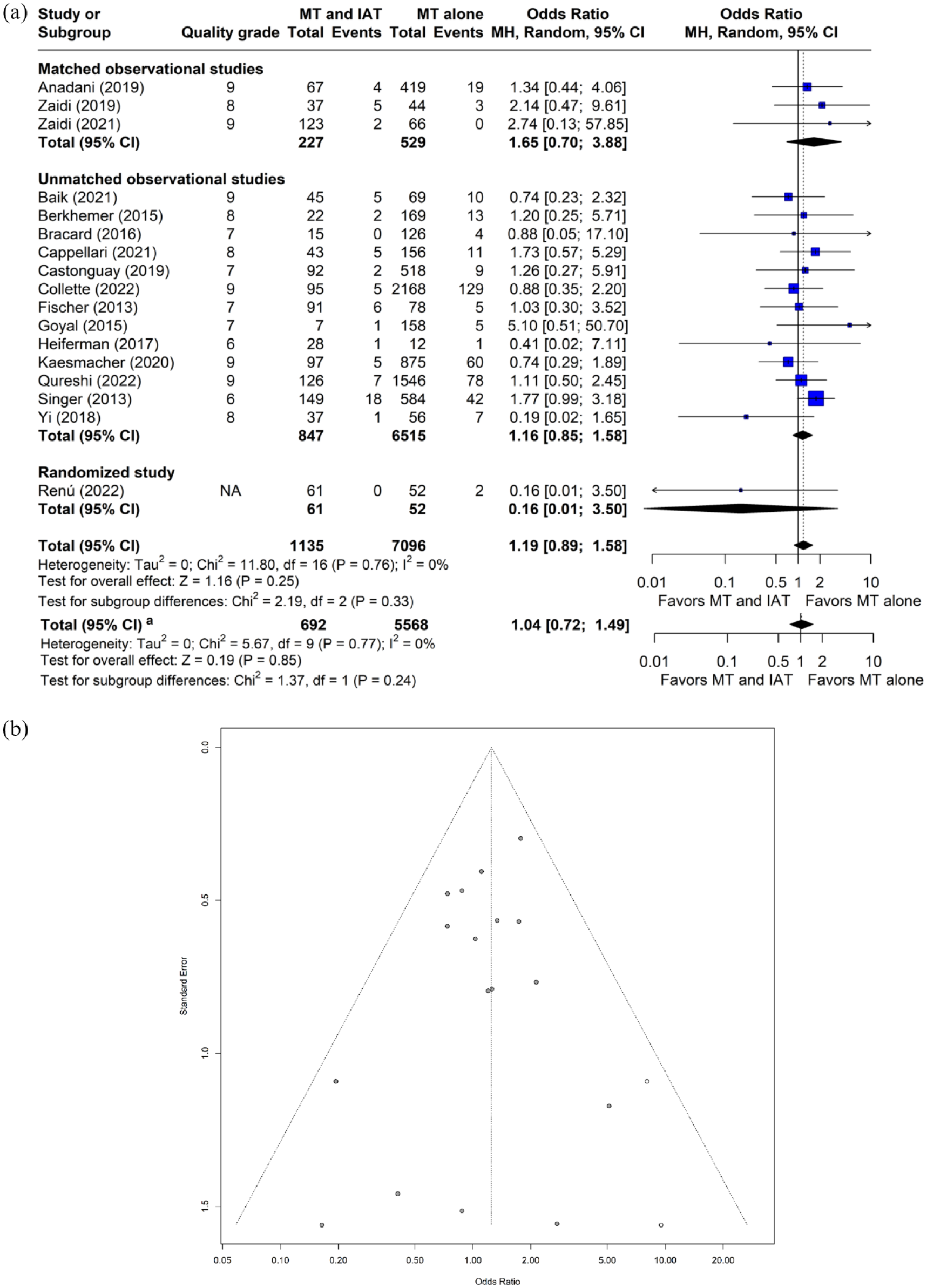
Plots of odds ratio for symptomatic intracranial hemorrhage in patients undergoing MT with and without IAT. (a) Forest plot and hypothesis testing for heterogeneity, overall effect, and subgroup differences (b) Funnel plot for adjusting publication bias with published studies (filled circles) and trim-and-fill assigned studies (open circles). MT: mechanical thrombectomy; IAT: intra-arterial thrombolysis; MH: Mantel–Haenszel test; CI: confidence interval.
Effect of IAT on near-complete or complete angiographic recanalization
The OR for near-complete or complete angiographic recanalization with IAT was 0.88 (95% CI: 0.63–1.23, p = 0.46, I2 = 69.9%, 18 studies, 8403 subjects, Figure 5(a)). A sizable asymmetry was detected in the funnel plot. After applying the trim and fill approach, the adjusted OR for near-complete or complete angiographic recanalization was significantly lower with IAT (OR: 0.59, 95% CI: 0.39–0.88, p = 0.01; Figure 5(b)). IAT was associated with significantly lower odds of near-complete or complete angiographic recanalization in a fixed effect model (OR: 0.73, 95% CI: 0.62–0.85, p < 0.001). In the meta-regression, no relationship was identified between study-level covariates and effect size (p > 0.05). IAT was associated with higher odds (OR: 1.65, 95% CI: 1.03–2.65, p = 0.04) of near-complete or complete angiographic recanalization in studies that were either matched or randomized comparisons. The ORs for near-complete or complete angiographic recanalization with IAT were 0.85 (95% CI: 0.55–1.33, p = 0.48) in studies with the highest quality grade and 0.83 (95% CI: 0.59–1.15, p = 0.26) in observational studies.
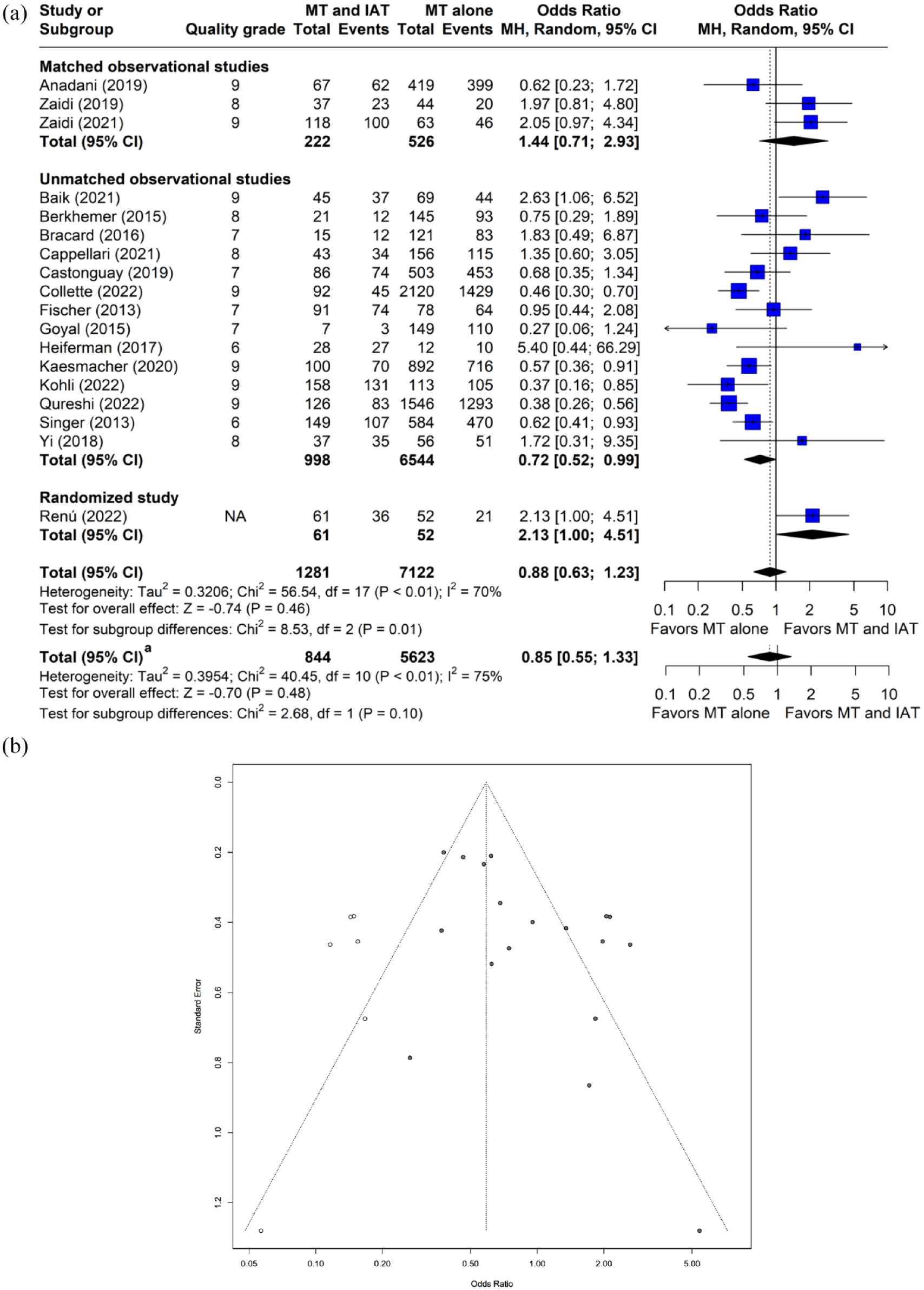
Plots of odds ratio for near-complete or complete recanalization in patients undergoing MT with and without IAT. (a) Forest plot and hypothesis testing for heterogeneity, overall effect, and subgroup differences (b) Funnel plot for adjusting publication bias with published studies (filled circles) and trim-and-fill assigned studies (open circles). MT: mechanical thrombectomy; IAT: intra-arterial thrombolysis; MH: Mantel–Haenszel test; CI: confidence interval.
Discussion
Salient findings
In the current systematic review and meta-analysis, we did not identify any significant association between IAT as an adjunct to MT and functional independence at 90 days, all-cause mortality within 90 days, or sICH. However, the direction of association suggested a possible increase in functional independence at 90 days (14% higher odds) and a reduction in all-cause mortality within 90 days with IAT. There was a trend toward higher odds of functional independence at 90 days among patients who received IAT in studies of the highest quality grade (24% higher odds) and in studies that were matched or randomized comparisons (28% higher odds). The direction of association suggested a possible increase in the odds of post-MT sICH with IAT although the increase was not detected when the analysis was restricted to studies of the highest quality grade. However, the odds increased from 19% higher (all studies) to 39% higher in studies that were matched or randomized comparisons. The association between IAT and near-complete or complete angiographic recanalization demonstrated inconsistent results. Overall, IAT was associated with lower rates of near-complete or complete angiographic recanalization in the fixed effect model but not in the random effects model. IAT was associated with higher odds of near-complete or complete angiographic recanalization in studies that were matched or randomized comparisons. A previous meta-analysis including 4581 patients by Chen et al. 10 reported that IA treatment (thrombolytics or glycoprotein IIb/IIIa inhibitors) was associated with a higher rate of functional independence and another meta-analysis including 2797 patients by Kaesmacher et al. 11 reported that IAT was not associated with higher rates of functional independence as an adjunct to MT. Inclusion of additional studies5,12–17 such as results from the randomized CHOICE 17 trial in our analysis increased the sample size (7572 patients) by almost 2–4 folds compared with the previous analyses by Chen et al. 10 and Kaesmacher et al. 11 Therefore, the precision of estimates of various outcomes was higher, and type 2 errors in comparisons were reduced. By increasing the design diversity among included studies, we also identified the prominent effect of design and quality of the studies on the association between IAT and functional independence at 90 days.
Current perception of IAT as adjunct to MT
IAT continues to be used frequently in an inconsistent manner as an adjunct to MT in AIS patients. Over 60% of respondents used IAT with MT without any clear consensus on its indications or therapeutic value in a survey of 104 neurointerventionalists. 39 Of those who used IAT, 60.4% indicated that they used IAT for: (1) treating a primary distal occlusion, (2) as rescue therapy, and/or (3) adjunctive therapy. Almost half (49.4%) of those surveyed believed that IAT may have a role with MT, but more evidence is needed, while 37.6% agreed that IAT has a role in MT. Only 12.9% felt there was no role for IAT in modern endovascular practice. A survey of 99 neurologists and neurointerventionalists from all German University hospitals, all participants of the German Stroke Registry—Endovascular Treatment (GSR), found that IAT was used in select cases by 39% and as a standard of care by 3% of the respondents. 40 We surveyed individuals who were part of the ACTION CVT (Direct Oral Anticoagulants Versus Warfarin in the Treatment of Cerebral Venous Thrombosis) group, Life journal authors of stroke-related publications, ASPIRE (Anticoagulation in ICH Survivors for Stroke Prevention and Recovery) clinical trial, COVID-19 stroke project, SVIN (Society of Vascular and Interventional Neurology) task force on trainee education, and Endovascular Stroke Treatment Optimization (ESTO)-2 investigators (unpublished data). A total of 92 (63%) of 146 respondents reported they followed no specific protocol on who received IAT, but 79% reported using IAT with MT. A total of 82 (56.1%) respondents stated that they would classify the importance of determining the therapeutic value of IAT during MT as very important or important. A total of 135 (92.5%) stated that they would definitely, very probably, or probably modify their practice if a randomized clinical trial demonstrated that IAT with MT reduced death or disability, and 121 (82.8%) respondents stated that they would be able to include IAT very easily or easily with MT in their practice.
Limitations of our analysis
The analysis is predominantly based on observational studies. Observational studies comprise approximately 80–90% of published clinical research41,42 and 64% of systematic reviews include observational studies. 43 However, assessing the causal relationship between IAT and various outcomes is limited by both bias and confounding. 44 Particularly, IAT is preferentially used in patients who have incomplete or no recanalization after MT (rescue treatment). The inverse relationship between IAT and odds of near-complete or complete angiographic recanalization was probably reflective of the pattern of use rather than the lack of effect on recanalization. We think that methodological heterogeneity may also account for the lack of a significant association seen between IAT and various outcomes. We used the recommendations by Metelli and Chaimani 44 by using the random effects model accounts for heterogeneity, performing subgroup analysis or meta-regression by study design and characteristics, and performing a sensitivity analysis excluding studies of lower credibility. We used the NOS for cohort studies, 45 which is a commonly utilized method of grading the quality of observational studies. 33 We evaluated the effect of the quality of the study in the meta-regression and sensitivity analyses. Our analysis identified a prominent effect of the quality of the study and whether comparisons were made between groups that were either matched or assigned with random allocation. We also noticed funnel plot asymmetry in all the endpoints ascertained,37,46 which can be a result of publication or other reporting biases, heterogeneity, and chance. 37 We acknowledge the limitations posed by performing meta-regression using a relatively small number of studies since a large ratio of studies to a covariate is required for a meaningful analysis. Usually, a ratio of 10 studies to 1 covariate is recommended in meta-regression. 47
Implications of our analysis
Our analysis points to the relative lack of evidence in existing reports that supports the relatively prevalent practice of administering IAT as an adjunct to MT in AIS patients. IAT was associated with higher rates of recanalization and functional independence when IAT was used as an adjunct to MT in some observational studies.29,48 IAT may ameliorate microcirculatory compromise caused by a combination of capillary constriction followed by filling with entrapped erythrocytes, leukocytes, and fibrin-platelet deposits which prevents tissue perfusion after recanalization with MT.49–51 Perfusion abnormalities can be seen in almost 80% of patients after near-complete or complete recanalization following MT. 52 Our analysis suggested that the odds of functional independence at 90 days may be higher with IAT as an adjunct to MT (compared with MT alone) in studies of the highest quality grade, or in studies that were either matched or randomized comparisons. However, the odds of post-MT sICH may be higher with IAT, particularly in studies that were either matched or randomized comparisons. As none of the results were statistically significant and thus remain inconclusive, the risk–benefit ratio is not well known, and assuming a positive or null effect of IAT as an adjunct to MT may overlook a potentially negative effect of IAT. Randomized clinical trials are required to assess the risk–benefit ratio and identify AIS patient populations most likely to benefit from IAT as an adjunct to MT.
Supplemental Material
sj-docx-1-wso-10.1177_17474930231184369 – Supplemental material for Mechanical thrombectomy with intra-arterial thrombolysis versus mechanical thrombectomy alone in patients with acute ischemic stroke: A systematic review and meta-analysis
Supplemental material, sj-docx-1-wso-10.1177_17474930231184369 for Mechanical thrombectomy with intra-arterial thrombolysis versus mechanical thrombectomy alone in patients with acute ischemic stroke: A systematic review and meta-analysis by Adnan I Qureshi, Abdullah Lodhi, Iqra N Akhtar, Xiaoyu Ma, Danish Kherani, Chun Shing Kwok, Daniel E Ford, Daniel F Hanley, Ameer E Hassan, Thanh N Nguyen, Alejandro M Spiotta and Syed F Zaidi in International Journal of Stroke
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
ORCID iDs
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.